Primary Care Transformation in Academic Medical Centers. Objectives of Session
|
|
|
- Wilfrid Fields
- 6 years ago
- Views:
Transcription

1 Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton, MD,MPH; Andrew Ellner MD, MSc; Jonathan Sugarman, MD, MPH and Cory Sevin, RN, MSN; Objectives of Session Describe an approach to launching a collaborative across academic primary care practices Describe early findings from the work at Harvard Medical School, including findings on leadership engagement, team structures, patient and provider satisfaction, and clinical process and outcome measures. Identify key lessons learned that others can apply in transforming primary care teaching practices in academic medical centers 2 1




2 Introductions 3 2

3 Overall Goal/Aims of AIC Create a learning community across Harvard clinical affiliates focused on continuously improving systems for primary care delivery and education Create a platform for combined educational and delivery innovation Trainees are integrated within high-functioning primary care teams that provide: proactive, population-oriented care focused on wellness, prevention and highly effective chronic disease management Achieve sustainable improvements in the experience of care for patients in our affiliated clinics Increase quality and start to reduce costs for patients at our affiliated clinics 5 Double Helix of Academic Primary Care Delivery Reform Practice Change Educational Change Building Blocks for Change Teams Leadership QI strategy Empanelment 6 3
4 Academic Innovations Collaborative (AIC) 7 The Academic Innovations Collaborative 19 AMC-affiliated primary care practices 6 hospital-based 13 community-based Community health center and private practices 11 Residency Programs 7 Internal Medicine, 1 Family Medicine, 1 Med-Peds, 2 Pediatrics 8 4
5 What We Aim to Accomplish Together 1. Establish team-based care 2. Manage populations prospectively 3. Find/manage high-risk populations 4. Improve physician/workforce satisfaction 5. Improve patient and trainee experience 9 The Power of Teams Effects of QI Strategies for Type 2 Diabetes on Glycemic Control 10 JAMA. 2006;296:


6 Key Components of the AIC Funding sources: HMS Center for Primary Care - $8 million Academic Health Centers - $6 million How we spend our funds: Full-time program manager at each large AHC Protected time for practice transformation Learning sessions, academies, coaching Design, operation, evaluation Time frame: 2 years, launched July Engaging Leadership 12 6
7 The Structure of the AIC At each clinic site: Transformation team 6-12 staff members including residents Aims statement Develop and test changes during Action Periods Learning sessions 3x per year, in person Monthly conference calls 13 The Structure of the AIC Practice coaching -from CPC/IHI/Qualis Health Leadership academy Educator and trainee academy Resident curriculum Learner-led quality improvement and care coordination activities Patient engagement patient/family advisory councils, regular patient surveys, patients on transformation teams 14 7
8 AIC I 3 Colorado Pennsylvania Participants Change Model Components 19 HMS affiliated teaching practices & community clinics Qualis Change Concepts & IHI Breakthrough 25 FM/IM/Peds teaching practices in NC, SC, VA 10 FM programs 25 FM programs 20 community health centers IHI Breakthrough Plan Do Study Act Chronic Care Model Multidisciplinary Teams x x x x Learning Sessions x x x x Webinars/Conference Calls x x x Shared Website x x x PCMH E learning Modules Consultants/ Practice Coaching Leadership Sessions Resident Participation on Teams Residency Curriculum Development x x x x x x x x x x x x x x NCQA PCMH Application x x x PCMH Monitor Assessment x x x x Monthly Update Reports x x x 15 Online Registry x x AIC Set-Up For Quality Improvement Using data to drive improvement At practice level Building capacity through a quality improvement strategy writing aims, connecting measures and testing/implementation The SNMHI Change Concepts provide a road map for guided transformation 16 8
9 How Do Practices Know if they are Making Progress? 17 Measurement for Improvement Regular Measurement monthly transformation updates, run charts Tiered, flexible measurement strategy PCMH-A tool External evaluation Stories of Improvement 18 9




10 The Work of the AIC Aim Statement #1: Assign Panels Team-based Care Teams Outreach to Patients by July 2013 Aim Statement #2: Balance Panels Team Huddles Self-Management Goals by January 2014 Aim Statement #3: Balance Panels Pre- and Post-visit Planned Care Visits by July Data: Site-Specific Measures 20 10





11 Looking Under the Hood The Change Concepts for Practice Transformation: What s different? Transformation in academic medical centers compared to other settings: What s different? Measuring progress using the PCMH-A: What s different? 21 Examples of Medical Home Frameworks 22 11

 describe how and where to begin PCMH transformation Executive Summaries provide a concise description of each Change Concept, its role in PCMH transformation, and key implementation activities")
 provide a full introduction, implementation strategies and tools, and case studies 38 webinars 3 policy briefs on medical home payment and health reform 23 tools that can be")
12 The SNMHI Framework: The Change Concepts for Practice Transformation Wagner EH, Coleman K, Reid RJ, Phillips K, Abrams MK, Sugarman JR. The Changes Involved in Patient-Centered Medical Home Transformation. Primary Care: Clinics in Office Practice. 2012; 39: PCMH Implementation Resources Patient-Centered Medical Home Assessment (PCMH-A) Introductory materials ( describe how and where to begin PCMH transformation Executive Summaries provide a concise description of each Change Concept, its role in PCMH transformation, and key implementation activities and actions 13 Implementation Guides ( ) provide a full introduction, implementation strategies and tools, and case studies 38 webinars 3 policy briefs on medical home payment and health reform 23 tools that can be used to test or apply the key changes A Crosswalk between the Change Concepts for Practice Transformation and 2011 NCQA PCMH Recognition Standards ( Crosswalk.pdf) A downloadable registry of tools and resources ( 12


13 Goal: To have effective, involved leaders help staff see a better future, and give them the tools, resources and time to achieve it. Goal: To have in place a sustainable, broadly inclusive approach to continuous quality improvement that includes trusted performance measurement and a strategy for changing practice. SNMHI 25 Laying the Foundation: Why is it Important? Leadership and QI strategy provide the foundation for redesign. Practices that succeed in quality improvement initiatives have adaptive reserve the ability to learn and change. Key feature is leadership that can: envision a future, facilitate staff involvement, and devote time and resources to make changes. Practices that don t routinely measure and review performance are unlikely to improve. SNMHI 26 13

14 Goal: To assign all patients to a provider/care team to facilitate continuous care and population management. Goal: To develop skilled and well organized care teams, and ensure that patients are able to see their care team consistently over time. Teams should be designed to meet the needs of patient panels (typically include provider, MA, RN, front desk staff) SNMHI 27 Building Relationships: Why is it Important? Empanelment is the platform for population health: Links patients to care teams Profoundly changes culture and sense of accountability Team involvement in the care of chronically ill is the single most powerful intervention. Patients who have a continuity relationship with a personal provider have better health process measures and outcomes: Continuity of care increases the likelihood that the provider is aware of psychosocial problems impacting health. SNMHI 28 14

15 Goal: To encourage patients to expand their role in decisionmaking, health-related behaviour change and self-management and to communicate with them in a language and at a level they understand. Goal: To use planned interactions and follow-up with patients according to patient need, and to identify high-risk patients and ensure they are receiving appropriate care management services. SNMHI 29 Changing Care Delivery: Why is it Important? Patient activation is tied to health improvement. Patient involvement in QI activities and health center boards helps maintain the focus on patient and family needs. It also makes change process more efficient by incorporating enduser feedback in real time, and potentially avoiding useless or even harmful tests of changes Well-organized care is patient-centered care. Well-organized care is good care: Practices that do pre-visit planning (huddle) have better measures of chronic disease control and preventive care. SNMHI 30 15
16 Goal: To track and support patients when they obtain services outside the practice, and ensure safe and timely referrals or transitions. Goal: To ensure that established patients have 24/7 continuous access to their care teams via phone, , or in-person visits. SNMHI 31 Reducing Barriers to Care: Why is it Important? Evidence of cost savings comes, primarily, from improvements in care coordination and access. Even a few hours of off-hours appointment access is associated with reduced ED use. SNMHI 32 16
17 Lots of PCMH Assessment Tools Already Exist, Such As NCQA PCMH Recognition Readiness Tool Medical Home Index MHIQ Safety Net Medical Home Scale However, none of these align directly with the Change Concepts for Practice Transformation 33 Background Developed for the SNMHI by the MacColl Center for Health Care Innovation (Group Health Research Institute) and Qualis Health Based on the ACIC (Assessing Chronic Illness Care) survey tool developed by the MacColl Center Developed to measure a site s progress towards achieving the 8 Change Concepts Self-administered assessment first tested by 65 SNMHI sites every six months and now being used in a number of improvement initiatives, including the AIC Health Services Research 48, no. 6pt1 (2013): SNMHI 34 17
18 The PCMH-A Has Dual Roles It serves as a tool to assist practices in having internal conversations that allow many voices to contribute to observations about strengths and opportunities for improvement It serves as a tool to assist practices in tracking incremental progress over reasonable time periods as they strive to transform into patientcentered medical homes SNMHI 35 Example: PCMH-A PCI Component Opportunities Components Level D Level C Assessing patient and family values and preferences Score is not done is done, but not used in planning and organizing care Significant Implementation Level B Level A is done and providers incorporate is systematically done and it in planning and organizing care on incorporated in planning and organizing an ad hoc basis. care


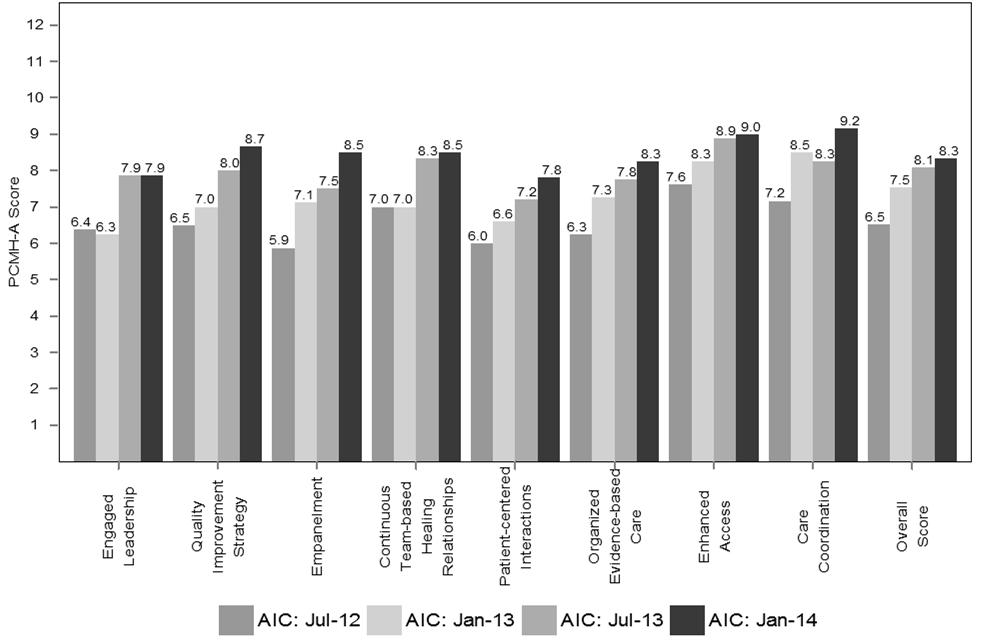
19 37 Data: PCMH-A Score 38 19
 c Enhanced Academic Primary Care Practices (NEW STRUCTURES & PROCESSES) d OUTCOMES OF INTEREST")
20 b Academic Innovations Collaborative Confounding Factors Patients Providers Predisposing Characteristics Age, Sex Size, Location Enabling Factors SES Case Mix, Payment Change Perceived Needs Medical Patient Mix Complexity a Traditional Academic Primary Care Practices (EXISTING STRUCTURES & PROCESSES) c Enhanced Academic Primary Care Practices (NEW STRUCTURES & PROCESSES) d OUTCOMES OF INTEREST Aim 1 Aim 2 Aim 3 Strategies/Tools for AMC Practices Provider Work Satisfaction Trainee Skills and Experience Care Quality and Health Plan Costs Courtesy of Alyna T. Chien, MD, MS 20
21 Key Lessons Learned Change in complex AMC affiliated clinics is possible Success is built on a foundation of engaged leadership Having a QI method is key The Qualis Change Concepts provide a useful roadmap that can be contextually adapted Regular and varied forms of measurement are KEY Building teams is both a process AND an outcome Engaging patients and trainees is critical We have just begun 41 21
Transforming Care for Vulnerable Populations:
 Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Where Do We Go From Here? The Value of Sustaining Practice Transformation
 Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
The New York State Health Center Controlled Network (NYS-HCCN)
") The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The Practice Transformation Support Hub. North Central ACH Regional Assessment and Technical Assistance
 The Practice Transformation Support Hub North Central ACH Regional Assessment and Technical Assistance The Healthier Washington Practice Transformation Support Hub An investment of Healthier Washington
The Practice Transformation Support Hub North Central ACH Regional Assessment and Technical Assistance The Healthier Washington Practice Transformation Support Hub An investment of Healthier Washington
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs
 Transformation and Recognition/Certification Programs") Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
M4: Primary Care Teams: Learning from Effective Ambulatory Practices
 M4: Primary Care Teams: Learning from Effective Ambulatory Practices Ed Wagner, MD, MPH, FACP, Director Emeritus, MacColl Center for Health Care Innovation Margaret Flinter, PhD, Senior Vice President
M4: Primary Care Teams: Learning from Effective Ambulatory Practices Ed Wagner, MD, MPH, FACP, Director Emeritus, MacColl Center for Health Care Innovation Margaret Flinter, PhD, Senior Vice President
Community Health Centers: Medical Homes in the Safety Net. Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health
 Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
Deeper Dive on Team Roles: Part I
 Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Part 1: NCQA PCMH 2014 Standards
 Part 1: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health Objectives Examine the requirements for NCQA PCMH 2014 Standards Review project
Part 1: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health Objectives Examine the requirements for NCQA PCMH 2014 Standards Review project
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A)
") SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
QUALITY IMPROVEMENT ROUNDTABLE
 QUALITY IMPROVEMENT ROUNDTABLE 2014 NCQA PCMH STANDARDS TRAINING FOLLOW UP SEPTEMBER 29, 2015 OLYMPIA, WA Advancing Healthcare Improving Health HOUSEKEEPING Asking Questions To ask questions aloud, click
QUALITY IMPROVEMENT ROUNDTABLE 2014 NCQA PCMH STANDARDS TRAINING FOLLOW UP SEPTEMBER 29, 2015 OLYMPIA, WA Advancing Healthcare Improving Health HOUSEKEEPING Asking Questions To ask questions aloud, click
Design Principles for Learning and Caring in Patient-Centered Primary Care Homes
 The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
QI ROUNDTABLE. NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA
 QI ROUNDTABLE NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA WELCOME HOUSEKEEPING Please sign in Folders Restrooms Electronic devices
QI ROUNDTABLE NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA WELCOME HOUSEKEEPING Please sign in Folders Restrooms Electronic devices
Improving Patient-Centered Medical Home (PCMH) Recognition: Board-Endorsed Recommendations of the PCPCC Accreditation Work Group
 Recognition: Board-Endorsed Recommendations of the PCPCC Accreditation Work Group") Improving Patient-Centered Medical Home (PCMH) Recognition: Board-Endorsed Recommendations of the PCPCC Accreditation Work Group BACKGROUND: Patient-Centered Primary Care Collaborative November 2015 The
Improving Patient-Centered Medical Home (PCMH) Recognition: Board-Endorsed Recommendations of the PCPCC Accreditation Work Group BACKGROUND: Patient-Centered Primary Care Collaborative November 2015 The
The medical home model of primary care delivery has
 ORIGINAL RESEARCH The Safety Net Medical Home Initiative Transforming Care for Vulnerable Populations Jonathan R. Sugarman, MD, MPH,* Kathryn E. Phillips, MPH,* Edward H. Wagner, MD, MPH,w Katie Coleman,
ORIGINAL RESEARCH The Safety Net Medical Home Initiative Transforming Care for Vulnerable Populations Jonathan R. Sugarman, MD, MPH,* Kathryn E. Phillips, MPH,* Edward H. Wagner, MD, MPH,w Katie Coleman,
College-wide Patient-Centered Medical Home Program Meharry Medical College
 + The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
+ The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
Experience from the Front Line*: Patient-Centered Medical Home
 Experience from the Front Line*: Patient-Centered Medical Home Mark W. Friedberg, MD, MPP Natural Scientist RAND Presentation to the Roundtable on Value and Science-Driven Health Care Institute of Medicine
Experience from the Front Line*: Patient-Centered Medical Home Mark W. Friedberg, MD, MPP Natural Scientist RAND Presentation to the Roundtable on Value and Science-Driven Health Care Institute of Medicine
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010
 Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Implementing Patient-Centered Medical Home Pilot Projects:
 Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
Patient Centered Medical Home
 Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
New Models of Care- Looking at PCMH & Telehealth
 New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017
 D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Olympic Community of Health
 Olympic Community of Health [cover page] North Central Accountable Community of Health Patient-Centered Medical Home Assessment (PCMH-A) Summary of Regional Results (Interim Report) Olympic Accountable
Olympic Community of Health [cover page] North Central Accountable Community of Health Patient-Centered Medical Home Assessment (PCMH-A) Summary of Regional Results (Interim Report) Olympic Accountable
Reducing Care Fragmentation Executive Summary
 Reducing Care Fragmentation Executive Summary A TOOLKIT FOR COORDINATING CARE Reducing Care Fragmentation 49 Executive Summary Reducing Care Fragmentation: A Toolkit for Coordinating Care is for clinics,
Reducing Care Fragmentation Executive Summary A TOOLKIT FOR COORDINATING CARE Reducing Care Fragmentation 49 Executive Summary Reducing Care Fragmentation: A Toolkit for Coordinating Care is for clinics,
Health Reform and The Patient-Centered Medical Home
 THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
Primary Care Meets Population Health: The Parable of Preventable Hospitalizations
 Department of Family & Community Medicine University of California, San Francisco Primary Care Meets Population Health: The Parable of Preventable Hospitalizations Kevin Grumbach, MD Duke Department of
Department of Family & Community Medicine University of California, San Francisco Primary Care Meets Population Health: The Parable of Preventable Hospitalizations Kevin Grumbach, MD Duke Department of
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Team-Based Care Initiative Interim Report
 F I N A L Team-Based Care Initiative Interim Report September 28, 2017 Jay Crosson Tricia Collins Higgins Lee-Lee Ellis Jasmine Little Alexander Bohn Geraldine Haile Ebo Dawson-Andoh Submitted to: The
F I N A L Team-Based Care Initiative Interim Report September 28, 2017 Jay Crosson Tricia Collins Higgins Lee-Lee Ellis Jasmine Little Alexander Bohn Geraldine Haile Ebo Dawson-Andoh Submitted to: The
CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities
 CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities MODERATOR: Jonathan Sugarman, MD, MPH, President and CEO of Qualis Health SPEAKERS:
CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities MODERATOR: Jonathan Sugarman, MD, MPH, President and CEO of Qualis Health SPEAKERS:
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
DIGEST. Safety Net Medical Home Initiative. From the Principal Investigator. Summer 2012
 Safety Net Medical Home Initiative M E D I C A L H O M E N E W S F R O M T H E S A F E T Y N E T M E D I C A L H O M E I N I T I AT I V E The Medical Home Digest is a newsletter devoted to keeping you
Safety Net Medical Home Initiative M E D I C A L H O M E N E W S F R O M T H E S A F E T Y N E T M E D I C A L H O M E I N I T I AT I V E The Medical Home Digest is a newsletter devoted to keeping you
PCMH and the Care of Complex High Cost Patients
 PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
Clinician Information Packet: Transition from Pediatric to Adult Care
 Clinician Information Packet: Transition from Pediatric to Adult Care 1 This packet contains information about: Processes for planning, transferring and integrating patients into adult care How to incorporate
Clinician Information Packet: Transition from Pediatric to Adult Care 1 This packet contains information about: Processes for planning, transferring and integrating patients into adult care How to incorporate
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
SAFETY NET MEDICAL HOME INITIATIVE
 SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
HEALTH CARE HOME ASSESSMENT (HCH-A)
") HEALTH CARE HOME ASSESSMENT (HCH-A) To be used by Health Care Homes involved in stage one implementation To asses practice readiness, monitor progress, and for evaluation purposes. Practice name Your name
HEALTH CARE HOME ASSESSMENT (HCH-A) To be used by Health Care Homes involved in stage one implementation To asses practice readiness, monitor progress, and for evaluation purposes. Practice name Your name
Patient Centred Medical Home Self-assessment (PCMH-A)
") Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Patient Centered Medical Home (PCMH)
") Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards
 and the NCQA PCMH 2011 Standards") Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Oregon Health Authority Patient-Centered Primary Care Home Program. May 2013
 Oregon Health Authority Patient-Centered Primary Care Home Program May 2013 Presentation Objectives Provide a brief background on Oregon s Patient-Centered Primary Care Home Program and vision for practice
Oregon Health Authority Patient-Centered Primary Care Home Program May 2013 Presentation Objectives Provide a brief background on Oregon s Patient-Centered Primary Care Home Program and vision for practice
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs
 The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
DIGEST. Safety Net Medical Home Initiative FINAL ISSUE. From the Principal Investigator. Summer Lessons Learned
 Safety Net Medical Home Initiative FINAL ISSUE M E D I C A L H O M E N E W S F R O M T H E S A F E T Y N E T M E D I C A L H O M E I N I T I AT I V E - The Medical Home Digest is a newsletter devoted to
Safety Net Medical Home Initiative FINAL ISSUE M E D I C A L H O M E N E W S F R O M T H E S A F E T Y N E T M E D I C A L H O M E I N I T I AT I V E - The Medical Home Digest is a newsletter devoted to
Better Health and Lower Costs for Patients With Complex Needs
 Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
Better Health and Lower Costs for Patients With Complex Needs An IHI Triple Aim Collaborative Informational Call May 12, 2015 Faculty on Informational Call Today Cory Sevin IHI Director Catherine Craig
Using a team-based care approach to achieve Care Coordination
 Using a team-based care approach to achieve Care Coordination June 2015 Dawn Welling RN MSN Director of PCMH Care Initiatives Kimberly Wente RN BSN, Senior Care Coordinator Jen Kirstein RN BSN, Care Coordinator
Using a team-based care approach to achieve Care Coordination June 2015 Dawn Welling RN MSN Director of PCMH Care Initiatives Kimberly Wente RN BSN, Senior Care Coordinator Jen Kirstein RN BSN, Care Coordinator
Katie Coleman, MSPH EDUCATION AND TRAINING
 Katie Coleman, MSPH Address MacColl Center for Health Care Innovation Group Health Research Institute 1730 Minor Avenue, Suite 1600 Seattle, WA 98101 Phone (206) 287-2872 Email coleman.cf@ghc.org EDUCATION
Katie Coleman, MSPH Address MacColl Center for Health Care Innovation Group Health Research Institute 1730 Minor Avenue, Suite 1600 Seattle, WA 98101 Phone (206) 287-2872 Email coleman.cf@ghc.org EDUCATION
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient-Centered Medical Home
 2015 QUEST Integration HMSA QUEST Integration Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross and Blue Shield Association
2015 QUEST Integration HMSA QUEST Integration Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent Licensee of the Blue Cross and Blue Shield Association
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Patient-Centered Medical Home
 2014 Primary Care HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E HMSA, an Independent Licensee of the Blue Cross and Blue Shield Association Progressing
2014 Primary Care HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E HMSA, an Independent Licensee of the Blue Cross and Blue Shield Association Progressing
New Models of Health Care: The Patient Centered Medical Home. Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
 New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
Thank you for joining us! The webinar will begin shortly.
 i2i Systems Presents 2014 PCMH Standards A Whole New Ballgame Thank you for joining us! The webinar will begin shortly. 2014 PCMH Standards A Whole New Ballgame Shannon Nielson, MHSA, PCMH-CCE Objectives
i2i Systems Presents 2014 PCMH Standards A Whole New Ballgame Thank you for joining us! The webinar will begin shortly. 2014 PCMH Standards A Whole New Ballgame Shannon Nielson, MHSA, PCMH-CCE Objectives
America s Voice for Community Health Care
 America s Voice for Community Health Care The NACHC Mission To promote the provision of high quality, comprehensive and affordable health care that is coordinated, culturally and linguistically competent,
America s Voice for Community Health Care The NACHC Mission To promote the provision of high quality, comprehensive and affordable health care that is coordinated, culturally and linguistically competent,
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model
 Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model Robert Gabbay MD, PhD Director, Penn State Institute for Diabetes and Obesity Professor of Medicine Penn State College
Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model Robert Gabbay MD, PhD Director, Penn State Institute for Diabetes and Obesity Professor of Medicine Penn State College
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health
 PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
NCQA PCMH 2017 Standards Intro 3/29/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PRINCIPLES OF THE PATIENT CENTERED MEDICAL HOME
 Page 1 of 12 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 American Academy of Family Physicians (AAFP) American Academy
Page 1 of 12 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 American Academy of Family Physicians (AAFP) American Academy
Why Are We Doing This?
 ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
National Committee for Quality Assurance
 National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
Improving Quality and Achieving Equity
 Improving Quality and Achieving Equity Measuring Performance and Taking Action A Case Study of Massachusetts General Hospital Joseph R. Betancourt, M.D., M.P.H. Director, The Disparities Solutions Center
Improving Quality and Achieving Equity Measuring Performance and Taking Action A Case Study of Massachusetts General Hospital Joseph R. Betancourt, M.D., M.P.H. Director, The Disparities Solutions Center
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Patient-Centered Medical Home
 2017 Primary Care Federally Qualified Health Centers (FQHCs) January 2017 (released December 2016) HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent
2017 Primary Care Federally Qualified Health Centers (FQHCs) January 2017 (released December 2016) HMSA Patient-Centered Medical Home Getting Started and Ongoing Management P R O G R A M G U I D E An Independent
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Fast-Track NCQA-PCMH Recognition. Using i2i Systems NCQA Pre-Validated PCMH Solution
 Fast-Track NCQA-PCMH Recognition Using i2i Systems NCQA Pre-Validated PCMH Solution Goal of Today s Webinar Share Why NCQA-PCMH Pre-Validation Matters Learn How to Fast-Track to NCQA-PCMH Recognition Hear
Fast-Track NCQA-PCMH Recognition Using i2i Systems NCQA Pre-Validated PCMH Solution Goal of Today s Webinar Share Why NCQA-PCMH Pre-Validation Matters Learn How to Fast-Track to NCQA-PCMH Recognition Hear
Practice Facilitators - Catalyst for Medical Home Transformation
 March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
Patient Centred Medical Home Readiness Program
 Module/workshop title: Patient Centred Medical Home Readiness Program Facilitated by: Australian Practice Nurses Association (APNA) Current as at 29/03/2018 For more information, contact: Cairns p: (07)
Module/workshop title: Patient Centred Medical Home Readiness Program Facilitated by: Australian Practice Nurses Association (APNA) Current as at 29/03/2018 For more information, contact: Cairns p: (07)
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees