New Models of Health Care: The Patient Centered Medical Home. Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
|
|
|
- Sophia Norton
- 5 years ago
- Views:
Transcription


1 New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
2 Objectives of this session: What s the burning platform for change? What are key components of new models of care? What are the core concepts of the PCMH? Does the PCMH work? How is it paid for? What does it mean to be Patient Centered and what does a PCMH look like? 2

3 Institute of Medicine
4 IOM: Crossing The Quality Chasm About 50% of the time, interventions that we all agree should happen don t, no matter what the problem or setting and it is much worse for patients who are poor or of color Quality of Chronic Illness Care» 15-24% adequate control of HTN» 42% of DM have appropriate lipid control» 38% A-fib on appropriate anticoagulation» 25% of Depression adequately treated» 40% CHF readmitted within 120 days 30-40% of US health care spending is waste (IOM 2005, CBO 2008) 4
5 IOM: Crossing The Quality Chasm Improvement in 6 domains 1) Safety 2) Effectiveness 3) Patient Centeredness 4) Timeliness 5) Efficiency 6) Equity Outline change at 4 levels: 1) Patient experience 2) Function of Microsystems 3) Function of organizations that have microsystems 4) Policy and Payment environment to support change 5

6 Future of Family Medicine 6
7 Traditional Model» Physician centered» Unnecessary barriers to access for patients» Reactive, fragmented care» Individual physician-patient visits» Experienced based» Haphazard chronic disease management New Model Patient centered Advanced access for patients Responsive, proactive and integrated Planned visits Evidence based Purposeful, organized chronic disease management
8




9 9 Joint Principles of the Patient Centered Medical Home Principles Personal Physician Physician directed medical practice Whole Person Orientation Care Coordination/ Integrated Care Quality and Safety Enhanced Access Payment

10 Joint Principles of the Patient Centered Medical Home Joint Principles of PCMH Personal Physician Physician directed medical practice Whole Person Orientation Care Coordination/ Integrated Care Quality and Safety Enhanced Access Payment Pillars of Primary Care First-contact care Continuity of care over time Comprehensiveness, or concern for the entire patient rather than one organ system Coordination with other parts of the health system. * Physicians can t do this alone: The PCMH brings together several systems interventions 10
 +74 % preventa)ve care -18% all cause -50% readmission -7% total PMPM Genesis (MI) -50% -15% 26.")
11 Outcomes of PCMH Trials Site ED Visits Quality Hospitalizations Cost Group Health -29% +36% sta)n -16% all cause $17 PMPM use CCNC -16% + asthma assessment + influenza vaccine -40% (asthma) - 20% reduction readmissions at 1 year -$380M in 2010 Geisenger (PA) +74 % preventa)ve care -18% all cause -50% readmission -7% total PMPM Genesis (MI) -50% -15% 26.6% fewer days Intermountain - 10% reduction $640/pt/year Hopkins Guided Care NCBCBS % reduction in visits -15% 24% 37% Nursing Home Days Savings $1364/Pt $75K/RN $9-$13 PM/PM HealthPartners (MN) -39% +129% optimal DM score -24% hospitalization -40% readmissions - 8% 11
12 NCQA PCMH Standards 2011 Standard Changes from 2008 Standard 1 Access redefined After hours Same day access/advanced Access Continuity Electronic access 2 Population Management Move from tools (point of care) to managing populations 3 Expanded Care Management Behavioral Health - 3 rd Important Condition as unhealthy behavior, mental health, substance abuse Identification of High Risk Patients 4 Expanded self-management support and community resources 5 Expanded Care Coordination Transitions, referral tracking, specialist agreements 6 Expanded Quality Improvement continuous quality improvement Disparities/vulnerable populations Patient experience Patient Advisory Council 12

13 UNC Family Medicine Center 17,200 empaneled patients with visits in the past 18 months 64 PCP s 56,000 visits PCMH level 3 (2011 standards)
14 Access is critical Access redefined: not just extended hours and overbooking.» Advanced access scheduling 60.0 UNC Family Medicine Center - Historical Appointment Access Data Days (Jun'13) Faculty Resident Overall Linear (Overall) PATIENT SATISFACTION - Overall Satisfaction (3-month running average) by Month Introduction of new Press Ganey sampling method


15 Access is critical Access redefined: not just extended hours and overbooking» Asynchronous communication Message response time: 10 hours less than phone calls Remote INR monitoring» After hours access: Good phone triage Management of symptoms new medications, new diagnoses» Access to the Team» MA, Pharmacist, RN, Care manager Minutes Total Pa8ent Wait Time: FMC Faculty YTD
16 Care Management A collaborative process of assessment, planning, facilitation, care coordination, evaluation, and advocacy for options and services to meet an individual s and family s comprehensive health needs through communication and available resources to promote quality costeffective outcomes. Case Management Society of America, Trends: ED Visits and Inpatient Admissions MSW Model High risk panel Inpatient Admission s trend_inp atient 8 ED visits/month 7.5 admissions per month 0 Year/Month (YYYYMM) 8/17/13 16
17 Team Based Care: Transitions Inpatient Service ACTion appointment (< 7 days post-discharge) Pharmacist PCP Care Manager (LCSW) % Discharges seen by ACTion team 25% No show rate 22.2% Overrall re-admission rate 25.0% Readmission rate of patients who attended ACTion appointment 16.7% Routine Care Co-management with Pharmacy Re-admission rate of no-show 27.3% Care Manager/PCP high risk panel

18 Continuous Quality Improvement: Engagement at All Levels Resident QIP project Screening rate = 58% 80% when visit was for DM, CHF, or CAD 18% when presented for different chief complaint Total patients 2578 Total screened 969 Positive PHQ-2 Positive PHQ-9 New Diagnosis
19 Continuous Quality Improvement: The Practice 60% 50% 40% 30% 20% 10% 0% % of Patients with Diabetes & BP > 140/90 Not an error 37% 31% 33% 36% 39% 33% 30% 30% 30% 28% 30% 31% 31% 33% 36% 35% 26% 27% 28% 27% 26% 29% 22% Overall Team 1 Team 2 Team 3 Team 4 Goal 5% 7% 7% 30.0% 20.0% Disparities in Care: % of Patients with Diabetes & A1C > % 0.0% Overall African American Caucasian Hispanic GOAL
 63.18 62.09 62.56 64.")

20 Continuous Quality Improvement: The Practice 100 Mammography Rate - Weekly Data Mammography Rate by Provider: 90 Mammo Rate % (National Average) /19/2013 5/26/2013 Date 6/2/2013 6/9/2012 Project: Family Medicine Mammo Data.MPJ; Worksheet: Mammo Weekly - 6 wks; 6/11/2013; Lindsay Stortz, LStortz@unch.unc.edu Goal: 74% (National Average) Mean: 62% (FMC Average) High Performer: Margaret Helton (82%) 20



21 Continuous Quality Improvement: The Staff Before After 21
22 UNC DFM Patient Advisory Council Council Work Committee Work Strategic goals: Patient satisfaction Operational groups: QI, Supervisors, Communications, Renovation, Epic Individual/Small Group Work Research, curriculum design, community outreach PAC Successes: Family Medicine Center Renovation and Re-design Help redesign pediatric triage process. Patient input on faculty research/grant proposals. Review and analyze patient satisfaction data direct interventions Review and provide feedback on patient surveys Help prepare monthly patient e-newsletter Provide on-call service for FMC patients in need of addiction counseling. Review current internal and external departmental signage. Make recommendations for change 22

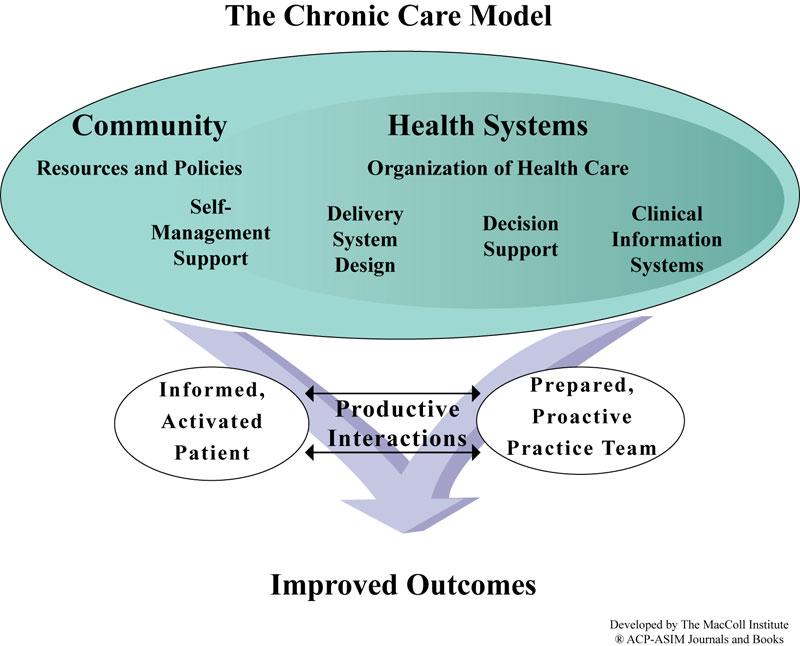
23 In a patient-centered medical home, it is hoped that the wheel would recognize the importance of treating each patient (the hub) as an individual in providing the best healthcare and clinic operations possible. This simply means a respect for the individual patient's health issues, socioeconomics, education and most important, an interactive treatment. In other words, the patient's welfare is a consideration from the check-in (or before) to the check-out. - HD,
24 Shared savings pilots: Paying for the PCMH» NY, MN, CO, MD, NC (CCNC)» PMPM (risk stratified), pay-for-performance, one-time payments BCBS: NC, CareFirst WellPoint: Indiana United Healthcare» Reimbursement tied to quality and cost-effectiveness, contracts linked to quality measurements will increase to $50 billion by 2017 CMS 2013 fee schedule» Transitional care Proposed CMS 2014 fee schedule» complex chronic care (CCC) conditions PQRS value based reimbursement Meaningful Use 24

25 Key Components of Practice Transformation to a PCMH Leadership and Change Management (culture change) Big Bang implementation Access Redefined A core interdisciplinary team celebrate success Care Management at the center of practice Risk Stratification resources where they are most impactful Team based care delivery large and small See our practice through our patients lens 25
 In North Carolina AHEC NC AHEC: 9 regional centers across the state, each center has a team of professionals to help primary care practices in the")
26 ACOFP.org» Medical Home Quality Markers» Links to resources AAFP.org» PCMH checklist» Many links to resources Resources IHI.org (Institute for healthcare Improvement) PCPCC.com (patient Centered Primary Care Collaborative) In North Carolina AHEC NC AHEC: 9 regional centers across the state, each center has a team of professionals to help primary care practices in the following areas: Achieving MU Improving clinical outcomes of patients Transforming into a patient centered medical home (many of the consulting staff are newly certified content experts by NCQA) If interested, contact your local AHEC or visit 26
27 UNC Family Medicine Top 12 Hurdles for Level 3 PCMH, 2011 Standards 1) Documenting Self-Management - provide self-care tools, self-mgmt. resources, set goals with date, etc. 2) Medication review document OTCs & herbals, assess understanding of meds and barriers to adherence, etc 3) Clinical summaries provide clinical summary at each relevant visit (med list, problem list, allergies, etc.) 4) Care transitions info transfer between PCP/hospital following discharge; not issue for FM due to integrated UNC EMR (WebCIS) 5) Defining an unhealthy behaviors/mental health condition as 1 of the 3 important conditions FM used tobacco use 6) Define high-risk population in a reasonable/low-impact way FM used those with diabetes +smoking (comorbidity) 7) Patient Experience - Are you going to use CAHPS to track patient experience? Can you get it up and running in time? FM did not. 8) Choose your preventive screening outreach wisely. FM: false positives on pneumovax and retinal photo outreach. 9) For re-application, look early at what elements require documentation; this saves a lot of work. 10) Patient experience feedback and patient advisory council 11) Documenting team based approach to care for element 1G need team-based care in job descriptions, training materials, etc. 12) Record review (shorter time period) vs Registry report (1 year) for data collection: Decide early 27
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
Improving Quality and Achieving Equity
 Improving Quality and Achieving Equity Measuring Performance and Taking Action A Case Study of Massachusetts General Hospital Joseph R. Betancourt, M.D., M.P.H. Director, The Disparities Solutions Center
Improving Quality and Achieving Equity Measuring Performance and Taking Action A Case Study of Massachusetts General Hospital Joseph R. Betancourt, M.D., M.P.H. Director, The Disparities Solutions Center
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care
 Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Building a Better Home: Transformation to a Patient Centered Health Home. Anna M. Gard, FNP-BC Association of Clinicians for the Underserved
 Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
The Future of Physician Reimbursement
 The Future of Physician Reimbursement EBG (PQRS-Quality Measures) yield Outcome Report Yield Increased Quality Yield Decreased Cost yield Increased Patient Satisfaction - CAHPS Consumer Assessment of Healthcare
The Future of Physician Reimbursement EBG (PQRS-Quality Measures) yield Outcome Report Yield Increased Quality Yield Decreased Cost yield Increased Patient Satisfaction - CAHPS Consumer Assessment of Healthcare
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Patient-Centered Primary Care
 Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
The Virtual Connection: Electronic Visits. Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009
 The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Outline 11/17/2014. Overview of the Issue Program Overview Program Components Program Implementation
 Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
Physical Health Integration in a Behavioral Health Setting Robin Reed, MD, MPH Rupal Yu, MD, MPH Acknowledgements The Duke Endowment Piedmont Health Services Carolina Advanced Health Community Care of
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
The Why and How. Carol L. Henwood, DO, FACOFP dist.
 Patient-Centered Medical Home: The Why and How Carol L. Henwood, DO, FACOFP dist. AODME January 14, 2012 The Triple Aim Improved Health Enhanced Patient Experience of Care Reduced Cost [+1: Improved Productivity]
Patient-Centered Medical Home: The Why and How Carol L. Henwood, DO, FACOFP dist. AODME January 14, 2012 The Triple Aim Improved Health Enhanced Patient Experience of Care Reduced Cost [+1: Improved Productivity]
MHS Care Management Program 1017.PR.P.PP.1 10/17
 MHS Care Management Program 1017.PR.P.PP.1 10/17 Sample Integrated Transitional Care Model Inpatient Admission Process Admission thru discharge and beyond Goals: Ensure safe and timely transitions of care
MHS Care Management Program 1017.PR.P.PP.1 10/17 Sample Integrated Transitional Care Model Inpatient Admission Process Admission thru discharge and beyond Goals: Ensure safe and timely transitions of care
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Transforming Primary Care in the Adirondack Region of New York State
 Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
The PCMH St Joseph s Experience
 The PCMH St Joseph s Experience Priya Radhakrishnan, MD Roshni Kundranda, MD, MSPH Binh Doung, DO Jenni Schroeder, RN, BSN ACP Regional Meeting Tucson, 2013 Disclosure No financial conflicts of interest
The PCMH St Joseph s Experience Priya Radhakrishnan, MD Roshni Kundranda, MD, MSPH Binh Doung, DO Jenni Schroeder, RN, BSN ACP Regional Meeting Tucson, 2013 Disclosure No financial conflicts of interest
Primary Care Redesign Updates to DFM
 Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
2019 Quality Improvement Program Description Overview
 2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
Improving Effectiveness in the PCMH. Shawn Stinson, MD FACP
 Improving Effectiveness in the PCMH Shawn Stinson, MD FACP 1 Overview Introduction to BCBSSC PCMH program Must haves for successful outcomes in a primary care practice Agreement on evidence based practices
Improving Effectiveness in the PCMH Shawn Stinson, MD FACP 1 Overview Introduction to BCBSSC PCMH program Must haves for successful outcomes in a primary care practice Agreement on evidence based practices
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014
 Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012
 Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Patient-centered care - from buzz word to meaningful reality. Current Health Care System
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
PCMH Standard 4. Deborah Johnson Ingram
 PCMH Standard 4 Deborah Johnson Ingram Patient Centered Medical Home 2011 Standards Recap of PCMH Standard 3 PCMH Standard 3: Plan and Manage Care Practice implements evidence-based guidelines System to
PCMH Standard 4 Deborah Johnson Ingram Patient Centered Medical Home 2011 Standards Recap of PCMH Standard 3 PCMH Standard 3: Plan and Manage Care Practice implements evidence-based guidelines System to
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Patient Centered Medical Home (PCMH)
") Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Improving Medicaid Chronic Disease Care and Controlling Costs. The Case for Medical Homes and Community Networks
 Improving Medicaid Chronic Disease Care and Controlling Costs The Case for Medical Homes and Community Networks L. Allen Dobson,Jr. MD FAAFP Chair -Board of Directors NC Community Care Networks, Inc HOME
Improving Medicaid Chronic Disease Care and Controlling Costs The Case for Medical Homes and Community Networks L. Allen Dobson,Jr. MD FAAFP Chair -Board of Directors NC Community Care Networks, Inc HOME
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
New Models of Care- Looking at PCMH & Telehealth
 New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Medical Home Best Practices: Case Study Examples
 Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
meaningful reality Katie Coleman, MSPH
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
University of Cincinnati Patient Centered Medical Home Leadership Decisions
 University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks
 Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
National Committee for Quality Assurance
 National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
Employer Breakout Session Payment Change in Ohio: What it Means for Employers
 Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is