Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
|
|
|
- Wesley Watts
- 5 years ago
- Views:
Transcription




1 Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018


2 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC FEATURED PRESENTER Karen Taubert RN, BSN, MBA, NCQA PCMH CCE Senior Consultant Qualis Health
3 Your lines are currently muted HOUSEKEEPING We ll address questions at the end of the presentation You can ask a question in the following ways: RAISE YOUR HAND FUNCTION - your line will be unmuted and you can ask the question verbally QUESTIONS FUNCTION type your question in the box and the facilitator will read it aloud This webinar is being recorded. A recording will be sent to you in a follow-up .
4 Care Coordination & Care Transitions (CC) Pre-Work Questions 1. What metrics are you monitoring to ensure care coordination systems for test and referral tracking are functioning in a manner that delivers results and reports to the provider in a timely manner? 2. What member or members of the care team is responsible for tracking and follow-up of patients recently discharged from the hospital or ED?
 Advancing Healthcare Improving")
5 2017 NCQA PCMH Standard 5: Care Coordination and Care Transitions (CC) Advancing Healthcare Improving Health

6 1. Resources for patient readiness assessment? 2. Our renewal date is 2/21/2020. Is there any problem with submitting our application for renewal early, for example October or November of 2019? NCQA said: Begin enrollment in the QPass system at the beginning of November; this will ensure that the 2020 annual reporting evaluation is loaded in the system. Just be mindful that you will be losing several months of recognition. Also be sure that to have the correct annual reporting document which can be obtained from the NCQA store. 3. How many months ahead of the chosen completion date would you suggest that we have everything submitted? 4. Did you notice any big changes with the new standards and guidelines that came out in July of 2018? 6

7 Change Concepts for Practice Transformation 7
8 Objectives Identify opportunities to improve your organization s process for closed-loop tracking of lab results, imaging tests, and referrals. Consider your organization s current methods of connectivity with health care facilities that support safe care transitions. 8 8
9 High Intensity of Care Needs Patient Support Aligned with Need Logistical Support includes appointments, reports, patient follow-up, providing information and support for patients as they navigate the system Care Coordination Logistical Clinical Care Management Medication mgmt Logistical Clinical Monitoring Clinical Follow-up Care Logistical Clinical Monitoring High % Percent of Patients Low % Low MacColl Institute for Healthcare Innovation, Group Health Research Institute
10 Care Coordination Metrics Examples. What are you measuring? Community Resources, Self-Management Support, etc. Patient satisfaction ratings for community resources Percent community resources for which loop was closed (i.e., patient received or evaluated the resource) Patient health confidence pre- and post-provision of self-management support Referrals Number of open referrals or percentage of referrals open > 60 days Percent referral results acknowledged by ordering clinician Test Orders Percentage lab orders open > 30 days Percentage of lab results pushed to portal and accessed by patient Percent lab results with documentation of patient notification Percent lab results acknowledged by ordering clinician Post-Discharge Follow-Up Percent patients called within 72 hours of discharge from hospital Percent patients scheduled for follow-up within seven days of discharge from hospital (and/or that showed for appt) Percent patients with discharge summary in chart by day of follow-up visit Percent high-risk ED discharges called within one business day Percent patients discharged from the hospital with med reconciliation performed within five business days 10
11 Key Design Elements for Care Coordination System 1. Assume accountability 2. Provide patient support 3. Build relationships and agreements 4. Develop connectivity 11


12 Care Coordination System: Better by Design The Space That Separates Us.. Dangerous Territory for Patients SNMHI, Care Coordination Implementation Guide, 12
13 Care Coordination and Care Transitions (CC) The practice systematically tracks tests, referrals and care transitions to achieve high quality care coordination, lower costs, improve patient safety and ensure effective communication with specialists and other providers in the medical neighborhood. 3 Competencies 21 Criteria 15 required documented processes 13
14 Competency A The practice effectively tracks and manages laboratory and imaging tests important for patient care and informs patients of the result. 1 Core criteria 2 Elective criteria 14
15 Competency A Criteria CC 01 Lab and Imaging Test Management (Core) CC 02 Newborn Screenings (1 Credit) CC 03 Appropriate Use for Labs and Imaging (2 Credits) - New 15

16 Competency A Required Documented Processes CC 01 Core - tracks and manages lab and imaging tests important for care and informs patients of the result CC 02 Elective follows up with inpatient facilities about newborn hearing and blood-spot 16
17 Competency A - CC 01 (Core) Manages Lab and Imaging Tests Aligns with PCMH A A. and B. Tracking lab and imaging tests until results are available, flagging and following up on overdue results. C. and D. Flagging abnormal lab and imaging results, bringing them to the attention of the clinician. E. and F. Notifying patients/families/caregivers of normal and abnormal lab and imaging test results. Evidence = Documented process AND Evidence of implementation 17

18 Consider Virtual Review 18

19 Consider Virtual Review 19


20 Competency A - CC 02 (1 Credit) Newborn Hearing and Blood-Spot Screening Follows up with the hospital or state health department if it does not receive screening results. Aligns with PCMH A Evidence = Documented process AND evidence of implementation 20

21 Consider Virtual Review 21
. Evidence = Evidence of implementation 22")
22 Competency A - CC 03 (2 Credits) Appropriate Use for Imaging and Lab Tests are Indicated - New Determines when imaging and lab tests are necessary based on established protocols and evidencebased guidelines. May implement clinical decision supports to ensure that protocols are used (e.g., embedded in order entry system). Evidence = Evidence of implementation 22

23 Competency E Example 23

24 Competency B The practice provides important information in referrals to specialists and tracks referrals until the report is received. Competency B The practice provides important information in referrals to specialists and tracks referrals until the report is received. 3 Core criteria 10 Elective criteria 1 Core criteria 9 Elective criteria 24
25 Competency B Criteria CC 04 Referral Management (Core) CC 05 Appropriate Referrals (2 Credits) CC 06 Commonly Used Specialists Identification (1 Credit) CC 07 Performance Information for Specialist Referrals (2 Credits) CC 08 Specialist Referral Expectations (1 Credit) 25
26 Competency B Criteria CC 09 Behavioral Health Referral Expectations (2 Credits) CC 10 Behavioral Health Integration (2 Credits) CC 11 Referral Monitoring (1 Credit) CC 12 Co-Management Arrangements (1 Credit) CC 13 Treatment Options and Costs (2 Credits) 26
27 Competency B Required Documented Processes CC 04 Core provides important information in referrals to specialists and tracks referrals until report is received CC 08 Elective works with specialists to set expectations for information sharing and patient care CC 09 Elective - works with behavioral health specialists to set expectations for information sharing and patient care (may use agreement in lieu of documented process) CC 10 Elective integrates behavioral health providers into the care delivery system CC 11 Elective monitors timeliness of referral responses CC 13 Elective engages with patients regarding cost implications of treatment option 27
28 Competency B Criteria CC 04 (Core) Referral Management Aligns with PCMH B Provides the clinical question, the required timing and the type of referral. Provides pertinent demographic and clinical data, including test results and the current care plan. Tracking referrals until the report is available, flagging and following up on overdue reports. Evidence = Documented process AND evidence of implementation 28

29 Competency B Elective Criteria CC05 through CC13 = 14 Possible Credits 29

30 Competency B - CC 05 (2 Credits) Appropriate Referrals - New Uses clinical protocols or decision support tools to determine if a patient needs to be seen by a specialist or if care can be addressed or managed by the primary care clinician. Evidence = Evidence of implementation 30


31 Competency B - CC 06 (1 Credit) Commonly Used Specialists - New Monitors patient referrals to gain information about the referral specialists and frequently used specialty types. Evidence = Evidence of implementation 31
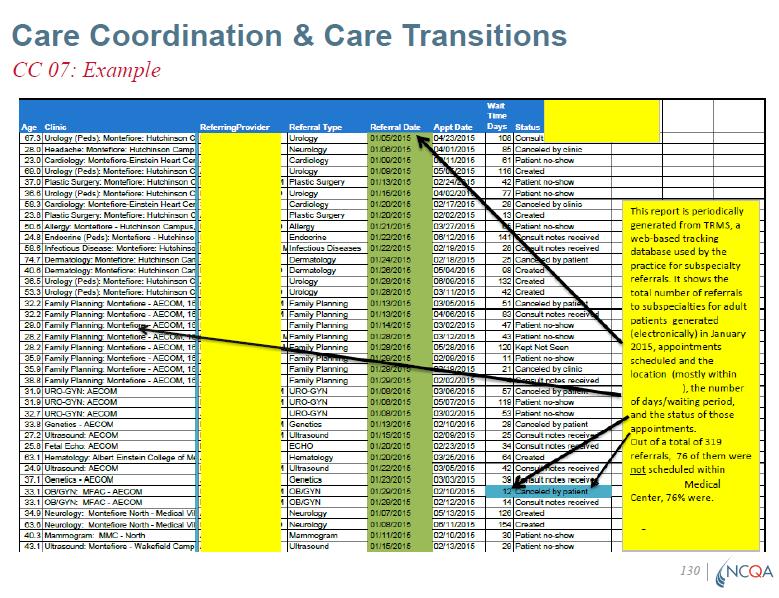
32 Competency B - CC 07 (2 Credits) Performance Information on Consultants/Specialists Consults available information about the performance of clinicians or practices to which it refers patients, and makes such information available to the practice team. Information gathered in CC 11 regarding timely and appropriate referral response may be useful here. Aligns with PCMH B Evidence = Data source AND examples 32

33 Consider Virtual Review 33
34 34
35 Competency B CC 08 (1 Credit) Specialist Referral Expectations Has established relationships with healthcare specialists through formal or informal agreements that establish expectations for exchange of information (e.g., frequency, timeliness, content). Aligns with PCMH B Evidence = Documented process OR Agreement 35
36 Competency B - CC 09 (2 Credits) Behavioral Health Referral Expectations Aligns with PCMH B Has established relationships with behavioral healthcare providers through formal or informal agreements that establish expectations for exchange of information (e.g., frequency, timeliness, content). A practice needs an agreement if it shares the same facility or campus as behavioral health professionals, but has separate systems. 36
37 Competency B - CC 09 (2 Credits) Behavioral Health Referral Expectations Aligns with PCMH B Evidence = Agreement OR Documented process AND evidence of implementation A notification demonstrating legal inability to receive a report or confirmation that a behavioral health visit occurred is sufficient. 37
38 38
39 Competency B - CC 10 (2 Credits) Behavioral Health Providers Integration Aligns with PCMH B Behavioral health integration includes care settings that have merged to provide behavioral health services and care coordination at a single practice setting. Providers work together to integrate patients primary care and behavioral health needs. Evidence = Documented process AND evidence of implementation 39
40 CC10 Additional Detail from NCQA Question: The criteria guidance states - behavioral health integration includes care settings that have merged to provide behavioral health services and care coordination at a single practice setting. "This is more involved than co-location of practices, because all providers work together to integrate patients primary care and behavioral health needs, have shared accountability and collaborative treatment and workflow strategies." Does this indicate a practice must have co-location of BH services to meet the criteria? Answer: No, co-location of BH services is not required to meet elective criterion CC 10; however, the practice must be able to demonstrate that it (at least partially) shares systems with a BH provider and that both providers work together to manage patient physical and behavioral healthcare needs to facilitate warm hand-offs and improved access to BH care. Please let us know if you have any further questions, and we are more than happy to assist! 40

41 Competency B - CC 11 (1 Credit) Monitors Timeliness and Quality of the Referral Response - New Assesses the response received from the consulting/specialty provider, evaluates whether the response was timely and provided appropriate information about the diagnosis and treatment plan. 41


42 Competency B - CC 11 (1 Credit) Monitors Timeliness and Quality of the Referral Response - New The practice bases its definition of timely on patient need On-going assessment and referral monitoring may be helpful in CC 07 Evidence = Documented process AND report. Aligns with PCMH B 42
 43")
43 CC 11 (1 Credit) may be used to meet CC 07 (2 Credits) 43
44 Competency B - CC 12 (1 Credit) Co-management Arrangements When a particular specialist regularly treats a patient, the primary care clinician and the specialist enter into an agreement that enables safe and efficient co-management of the patient s care. Aligns with PCMH B Evidence = 3 examples of implementation 44

45 Competency B - CC 13 (2 Credits) Treatment Options and Cost - New Makes patients aware of treatment costs as indicated. Evidence = Documented process AND evidence of implementation 45
46 Examples of CC 13 Implementation Add a financial question to the clinical intake screening Directs patients to copay and prescription assistance programs Use shared decisionmaking tools Ask about prescription drug coverage Tell patients which services are critical and should not be skipped Recommend less expensive treatment options, if appropriate 46

47 Shared Decision Making Tool with Reference to Cost 47

48 Competency C Connects with health care facilities to support patient safety throughout care transitions. The practice receives and shares necessary patient treatment information to coordinate comprehensive patient care. 3 Core criteria 5 Elective criteria 48

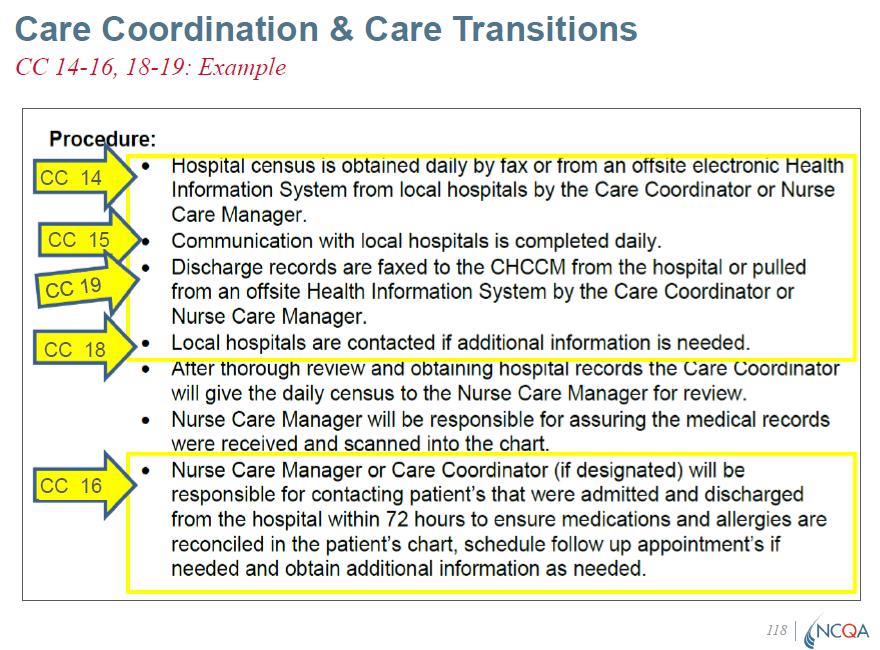
49 Competency C Core Criteria = 3 CC 14 Identifying Unplanned Hospital and ED Visits CC 15 Sharing Clinical Information CC 16 Post- Hospital/ED Visit Follow-up 49
50 Competency C Elective Criteria = 5 CC 17 Acute Care After Hours Coordination (1 Credit) CC 18 Information Exchange During Hospitalization (1 Credit) CC 19 Patient Discharge Summaries (1 Credit) CC 20 Care Plan Collaboration for Practice Transitions (1 Credit) CC 21 External Electronic Exchange of Information (Max 3 Credits) 50
51 Competency C Criteria Requiring Documented Processes CC 14 Core Systematically identifies patients with unplanned hospital admissions and ED visits CC 15 Core - Shares clinical information with admitting hospitals and emergency departments CC 16 Core - Contacts patients/families/caregivers for follow-up care, if needed, within an appropriate period following a hospital admission or emergency department visit CC 17 Elective - Systematic ability to coordinate with acute care settings after office hours through access to current patient information. CC 18 Elective - Exchanges patient information with the hospital during a patient s hospitalization CC 19 Elective - Implements a process to consistently obtain patient discharge summaries from the hospital and other facilities 51
52 Competency C Criteria - CC 14 (Core) Identifies Unplanned Hospital and ED Visits Works with local hospitals, EDs and health plans to identify patients with recent unplanned visits Aligns with PCMH C Evidence = Documented process and evidence of implementation 52

53 Consider Virtual Review 53
54 CC14 Additional Detail from NCQA Question: The criteria guidance states - "The practice should develop a process for monitoring unplanned admissions and emergency department visits and states how often monitoring takes place. The practice works with local hospitals, EDs and health plans to identify patients with recent unplanned visits. The practice provides a report with the proportion of local admissions and ED visits (reported separately) to facilities where practices have an established notification exchange mechanism." Can the "notification exchange mechanism" be a manual process such as faxing the ADT record to the practice daily for review, or does this imply an electronic exchange of data or shared system? Answer: Yes, the practice may use a manual process to identify and monitor any unplanned admissions to hospitals or emergency departments to meet core criterion CC 14. NCQA is not prescriptive regarding whether the process is manual vs. electronic, but the practice must provide both a documented process and evidence of implementation such as monitoring these admissions at facilities with which it works with regularly and has a relationship. 54
55 55
56 Competency C - CC 15 (Core) Sharing Clinical Information Demonstrates timely sharing of information with admitting hospitals and emergency departments. Shared information supports continuity in patient care across settings. Aligns with PCMH C Evidence = Documented process AND evidence of implementation. The practice provides three examples to meet the criteria. 56
57 Competency C - CC 16 (Core) Post Hospital/ED Visit Follow-Up Contacts patients to evaluate their status after discharge from an ED or hospital, and to make a follow-up appointment, if appropriate. The practice s policies define the appropriate contact period in addition to a log documenting systematic follow-up was completed. Aligns with PCMH C Evidence = Documented process AND evidence of implementation 57
58 Consider Virtual Review 58
59 Competency C Elective Criteria CC 17 CC 21 7 Credits Total CC 17 Acute Care After Hours Coordination (1 Credit) CC 18 Information Exchange During Hospitalization (1 Credit) CC 19 Patient Discharge Summaries (1 Credit) CC 20 Care Plan Collaboration for Practice Transitions (1 Credit) CC 21 External Electronic Exchange of Information (Maximum 3 Credits) 59


60 Competency C - CC 17 (1 Credit) Acute Care After Hours Coordination - New Communicates with acute care facilities when a patient is seen after the office is closed. Sharing patient information allows the facility to coordinate patient care based on current health needs and engage with practice staff. Evidence = Documented process AND at least one example of coordination with a facility 60
61 CC 17 Additional Detail Question: We have providers on call after-hours who are responsible for coordinating the exchange of current information with acute care settings. Our process is a manual one, however, it is across our practice sites. Is this acceptable? Answer: Yes, a practice can meet CC 17 using a manual process. As long as the practice has an arrangement with one or more acute care settings that specifies how they can contact someone to access relevant patient information needed for care coordination, then it would meet the intent of the criterion. If you have any additional questions, please don't hesitate to contact us. 61
62 Competency C - CC 18 (1 Credit) Information Exchange During Hospitalization The practice demonstrates that it can send and receive patient information during the patient s hospitalization. Note: CC 15 assesses the practice s ability to share information, but the focus of CC 18 is two-way exchange of information. Aligns with PCMH C Evidence = Documented process AND evidence of implementation 62

63 Competency C - CC 19 (1 Credit) Patient Discharge Summaries Proactively attempts to obtain discharge summaries. The process may include a local database or active outreach to ensure that the practice is notified when a patient is discharged from a hospital or other care facility. Aligns with PCMH C Evidence = Documented process AND evidence of implementation 63
64 Consider Virtual Review 64

65 Competency C - CC 20 (1 Credit) Transitional Care Plans The practice involves the patient/family/caregiver in the development or implementation of a written care plan for young adults and adolescent patients with complex needs transitioning to adult care. Aligns with PCMH A 65
66 The Plan May Include A summary of medical information A list of providers, medical equipment and medications for patients with special health care needs Patient response to the transition Obstacles to transitioning to an adult care clinician Special care needs Information provided to the patient about the transition of care Arrangements for release and transfer of medical records 66

67 Competency C - CC 20 Transitional Care Plans Family Medicine For family medicine practices that do not transition patients from pediatric to adult care, they should still educate patients and families about ways in which their care experience may change as the patient moves into adulthood. Evidence = Evidence of implementation 67
68 68
69 Competency C - CC 20 Transitional Care Plans Internal Medicine Internal medicine practices receiving patients from pediatricians are expected to request/review the transition plan provided by pediatric practices or develop a plan if one is not provided to support a smooth and safe transition. Evidence = Evidence of implementation 69

70 Competency C - CC 21 (Up to 3 Credits) Electronic Information Exchange - New Utilizes an electronic system to exchange patient health record data and other clinical information with external organizations The practice demonstrates the capability for two-way data exchange 70
 B.")
71 Competency C - CC 21 (Up to 3 Credits) Electronic Information Exchange - New A. Regional health information organization or other health information exchange source that enhances the practice s ability to manage complex patients. (1 Credit) B. Immunization registries or immunization information systems. (1 Credit) C. Summary of care record to another provider or care facility for care transitions. (1 Credit) Evidence = Evidence of implementation 71
72 Competency C - CC 21 (Up to 3 Credits) Electronic Information Exchange - New Practices can demonstrate this by: A. Exchanging patient medical record information to facilitate care management of patients with complex conditions or care needs. Aligns with PCMH G B. Submitting electronic data to immunization registries to share immunization services provided to patients. Aligns with PCMH G C. Making the summary of care record accessible to another provider or care facility for care transitions. Aligns with PCMH G 72

73 Questions? 73

74 COMPLEX CARE All of the below, and Provide enhanced services & tracking CHRONIC CONDITIONS All of the below, and Monitor, according to guidelines Identify and address chronic care gaps WELL Provide screenings, immunizations, and follow-up Administer at-risk assessments Track referrals and test orders Connect with between-visit support Support during transitions, including Follow-up after ED visits and hospital admissions 74
75 Join us for the Final PCMH Webinar in the series! Performance Measurement & Quality Improvement (QI) Wednesday, October 10, 12-1 PM REGISTER HERE Learning Objectives: Name the model for quality improvement used by your organization. Identify the metrics (measures) used to evaluate improvement efforts and outcomes at your organization. Specify how patients, families, providers, and care team members are involved in quality improvement activities.
76 Upcoming WACMHC Training Events Social Determinants of Health: A Washington Roundtable for FQHCs Wednesday, September 26 Seattle, WA REGISTER HERE Managers, directors, and key positions in Social Determinants of Health work are encouraged to join us for a day dedicated to discussions about statewide efforts in collecting and using Social Determinants of Health. Hear from partners in the healthcare safety net, and connect with peers to discuss challenges, successes, and experiences in implementing a screening program. SAVE THE DATE Quality Improvement Roundtable Change Management November 5 Please complete the evaluation after the end of the session. Your feedback is appreciated! Questions? Contact the WACMHC Practice Transformation Team at QualityImprove@wacmhc.org
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
QI ROUNDTABLE. NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA
 QI ROUNDTABLE NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA WELCOME HOUSEKEEPING Please sign in Folders Restrooms Electronic devices
QI ROUNDTABLE NCQA PCMH 2017 Understanding the New Standards and Re-designed Recognition Process TUESDAY, NOVEMBER 7, 2017 YAKIMA, WA WELCOME HOUSEKEEPING Please sign in Folders Restrooms Electronic devices
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
NCQA PCMH 2017 Standard Two 4/11/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Introduction to PCMH 2017
 Introduction to PCMH 2017 PCMH 2017 Eligibility Requirements Eligibility Requirements Outpatient primary care practices Practice defined: a clinician or clinicians practicing together at a single geographic
Introduction to PCMH 2017 PCMH 2017 Eligibility Requirements Eligibility Requirements Outpatient primary care practices Practice defined: a clinician or clinicians practicing together at a single geographic
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
The New York State Health Center Controlled Network (NYS-HCCN)
") The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
NCQA PCMH 2017 Standards Intro 3/29/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017
 Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A)
") SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
College-wide Patient-Centered Medical Home Program Meharry Medical College
 + The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
+ The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Presbyterian Healthcare Services Care Management
 Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
HEALTH CARE HOME ASSESSMENT (HCH-A)
") HEALTH CARE HOME ASSESSMENT (HCH-A) To be used by Health Care Homes involved in stage one implementation To asses practice readiness, monitor progress, and for evaluation purposes. Practice name Your name
HEALTH CARE HOME ASSESSMENT (HCH-A) To be used by Health Care Homes involved in stage one implementation To asses practice readiness, monitor progress, and for evaluation purposes. Practice name Your name
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Patient-Centered Medical Home (PCMH) All materials 2015, National Committee for Quality Assurance
 All materials 2015, National Committee for Quality Assurance") Patient-Centered Medical Home (PCMH) 2014 1 All materials 2015, National Committee for Quality Assurance Learning Objectives Introduction to PCMH and Eligibility Overview of the 6 PCMH Standards Highlight
Patient-Centered Medical Home (PCMH) 2014 1 All materials 2015, National Committee for Quality Assurance Learning Objectives Introduction to PCMH and Eligibility Overview of the 6 PCMH Standards Highlight
Patient Centred Medical Home Self-assessment (PCMH-A)
") Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
QUALITY IMPROVEMENT ROUNDTABLE
 QUALITY IMPROVEMENT ROUNDTABLE 2014 NCQA PCMH STANDARDS TRAINING FOLLOW UP SEPTEMBER 29, 2015 OLYMPIA, WA Advancing Healthcare Improving Health HOUSEKEEPING Asking Questions To ask questions aloud, click
QUALITY IMPROVEMENT ROUNDTABLE 2014 NCQA PCMH STANDARDS TRAINING FOLLOW UP SEPTEMBER 29, 2015 OLYMPIA, WA Advancing Healthcare Improving Health HOUSEKEEPING Asking Questions To ask questions aloud, click
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Appendix 4. PCMH Distinction in Behavioral Health Integration
 Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Care Coordination Overview. Janet Tennison, PhD UPV Standards October 8, 2013
 Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
Deeper Dive on Team Roles: Part I
 Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs
 Transformation and Recognition/Certification Programs") Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
Instructions for Completing the BHICCI Case Rate Readiness Assessment (CRRA) and Workplan
 and Workplan") Instructions for Completing the BHICCI Case Rate Readiness Assessment (CRRA) and Workplan IEHP intends to sustain integrated complex care through case rate funding to health care organizations/clinics
Instructions for Completing the BHICCI Case Rate Readiness Assessment (CRRA) and Workplan IEHP intends to sustain integrated complex care through case rate funding to health care organizations/clinics
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Agenda. NE CAH Region Discussion
 NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
Primary Care Transformation in Academic Medical Centers. Objectives of Session
 Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Community Health Centers: Medical Homes in the Safety Net. Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health
 Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
NCQA Recognition Programs Redesign Work in Progress
 NCQA Recognition Programs Redesign Work in Progress March 2016 Mina Harkins, MBA, BSMT, PCMH CCE NCQA Assistant Vice President Recognition Programs Policy and Resources Re-use without permission is prohibited
NCQA Recognition Programs Redesign Work in Progress March 2016 Mina Harkins, MBA, BSMT, PCMH CCE NCQA Assistant Vice President Recognition Programs Policy and Resources Re-use without permission is prohibited
2014 Patient Centered Medical Home (PCMH) Recognition
 Recognition") Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
PCMH 2011 Standard 1: Elements D, E, F & G. Slide 1
 PCMH 2011 Standard 1: Elements D, E, F & G Slide 1 PCMH Learning Community Project Structure Assessment, Gap Analysis, Workplan Webinar Series Group Technical Assistance Learning Sessions (Face to Face)
PCMH 2011 Standard 1: Elements D, E, F & G Slide 1 PCMH Learning Community Project Structure Assessment, Gap Analysis, Workplan Webinar Series Group Technical Assistance Learning Sessions (Face to Face)
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2017-2018 V12.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2017-2018 V12.0 Blue Cross Blue Shield of Michigan is a nonprofit
Hudson Headwaters Journey to Patient Centered Medical Home Recognition
 Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
NCQA s Patient-Centered Medical Home (PCMH) 2011
 2011") NCQA s Patient-Centered Medical Home (PCMH) 2011 Johann Chanin, Director, Product Development Mina Harkins, Assistant Vice President, Recognition Programs All materials 2011, National Committee for Quality
NCQA s Patient-Centered Medical Home (PCMH) 2011 Johann Chanin, Director, Product Development Mina Harkins, Assistant Vice President, Recognition Programs All materials 2011, National Committee for Quality
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F
 Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home Domains of Function. Interpretive Guidelines
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers
: Strategies to Overcome Implementation Barriers") Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers March 23, 2017 A Department of Social Services PCMH Presentation Hosted by Community Health Network of CT,
Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers March 23, 2017 A Department of Social Services PCMH Presentation Hosted by Community Health Network of CT,
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Improving Systems of Care for Children and Youth with Special Health Care Needs
 Improving Systems of Care for Children and Youth with Special Health Care Needs L E A R N I N G C O L L A B O R A T I V E O N I M P R O V I N G Q U A L I T Y A N D A C C E S S T O C A R E I N M A T E R
Improving Systems of Care for Children and Youth with Special Health Care Needs L E A R N I N G C O L L A B O R A T I V E O N I M P R O V I N G Q U A L I T Y A N D A C C E S S T O C A R E I N M A T E R
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
PCMH 2014 Record Review Workbook (RRWB)
") PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Risk Stratification for Population Health Management
 STEPS FOR SUCCESS IN Risk Stratification for Population Health Management EVERY DOCTOR HAS EXPERIENCED THE 80/20 RULE WHEN IT COMES TO TREATING THEIR SICKEST PATIENTS, says Leonard Fromer, MD, FAAFP, Executive
STEPS FOR SUCCESS IN Risk Stratification for Population Health Management EVERY DOCTOR HAS EXPERIENCED THE 80/20 RULE WHEN IT COMES TO TREATING THEIR SICKEST PATIENTS, says Leonard Fromer, MD, FAAFP, Executive
Clinical Medical Standing Orders (PCMH 1G) Delegation of Duties (NM Medical & Nurse Practice Acts, FTCA) CLIA Waived Testing (CLIA)
 Delegation of Duties (NM Medical & Nurse Practice Acts, FTCA) CLIA Waived Testing (CLIA)") Rev. 2/26/2013 REQUIRED POLICY Administration Governance (HRSA, BPHC, NM Licensure) Conflict of Interest (BPHC) Scope of Services/Locations (HRSA, BPHC) Hours of Operations & After Hours Coverage (BPHC,
Rev. 2/26/2013 REQUIRED POLICY Administration Governance (HRSA, BPHC, NM Licensure) Conflict of Interest (BPHC) Scope of Services/Locations (HRSA, BPHC) Hours of Operations & After Hours Coverage (BPHC,
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates