update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
|
|
|
- Terence Stafford
- 5 years ago
- Views:
Transcription
 Care Model May")
1 update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
2 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards: 2014, Projected 2017 and beyond o Montana PCMH Program Intersection of PCMH & EHR o Key functionalities needed o Care management Clinical quality platform o Multidisciplinary care teams o Integrating care across continuums Advancing your Medical Home o Metric & Transmission Consolidation Reporting Examples o Continuous Quality Improvement
 Recognition is the most widely adopted model for transforming primary care practices into medical homes.")
3 Background: What is a PCMH? The patient-centered medical home is a model of care that emphasizes care coordination and communication to transform primary care into what patients want it to be. NCQA Patient-Centered Medical Home (PCMH) Recognition is the most widely adopted model for transforming primary care practices into medical homes. Patients in medical homes receive the right care, in the right amount, at the right time. This increasingly popular delivery system modernization leads to safer and better care, empowers patients and renews the patient-provider relationship.

4 Primary Care is not PCMH Slide from Daniel Duffy MD School of Community Medicine Tulsa Oklahoma

5 Another view -Group Health Innovates: Medical Home Model of Primary Care, August 2, 2012, Eric B. Larson

6 Changes over Time


7 Evidence-Based Results Source: The Patient-Centered Medical Home s Impact on Cost and Quality- Annual Review of Evidence Published February 2016 by Patient-Centered Primary Care Collaborative
8 Updated NCQA PCMH Standards

9 NCQA 2014 Standards
10 Significant growth of care model o NCQA 2017 Standards Anticipated Changes. Preparation for population health Annual check-ins Potential changes to PCMH Levels Medical homes are included in MACRA Sustained transformation In keeping with the goal of continuous improvement, practices show that they comply with NCQA standards over long periods.

11 PCMH Stakeholder Council
12 Intersection of PCMH & EHR

13 PCMH & EHR Intersection
14 Key Functionalities Access Appointment access and continuity Electronic access- patient portal Communication needs Patient Information Comprehensive assessments Clinical quality Demographic Vulnerabilities and special populations Tracking and Coordinating Care Lab, referral, test tracking- complete functionality Exporting and Reporting Data Applicable third parties MT CSI program Affiliated projects Continuous quality improvement 6 overall measures


15 Patient Self-Management Comprehensive health assessment Identify populations for care management- *TRUE POPULATION HEALTH* o Care planning- goals, barriers, treatment plans, inclusion of team members and resources o Medication management Proactive outreach to patients needing services o Builds relationship with provider and care team o Robust medical record- external results entry o Comprehensive resource- go to place for care Transitional care management o External o Internal

16 Patient Registry- Example
17 Multidisciplinary Care Teams Standardized care team & evolution of Providers, nursing, billing, coding, registration staff Enhanced care team design Diabetic health embedded in primary care setting Behavioral health is on the radar- 1 pilot site Care Manager/Specialist positions (LPN, RN) Lead role in care team care management Transitions of Care Advanced Care Planning Centralized Team Population Health/ Centralized Support Services Clinical quality driver- ERE Other underlying tasks Tele-health capacities

18 Integrating Care Across Continuums Transitions of Care & Chronic Care Coordination patients Agreements with other organizations- affiliated and external Agreements with specialty for result tracking- referral and lab/test tracking Emergency Departments Urgent Care Retail clinics Behavioral health- varying departments and providers Diabetic health- varying departments and providers
19 Advancing Your Medical Home
20 Metric & Transmission Consolidation Identify/Edit Metric List: State PCMH Program Metrics Regional & System Metrics NCQA Recognition Metrics Operationally Driven Metrics Payer Metrics NQF Metrics Develop transmission process- annual extraction, EHR sweep and send via secure portal, HIE, etc. Determine data extraction specifics How is the data derived? - structured data, free text, coding, etc. Patient level or aggregate level reporting? Provider level or per clinic? Develop clinical quality workflows to guide teams in inputting data in right area so can be pulled from back end

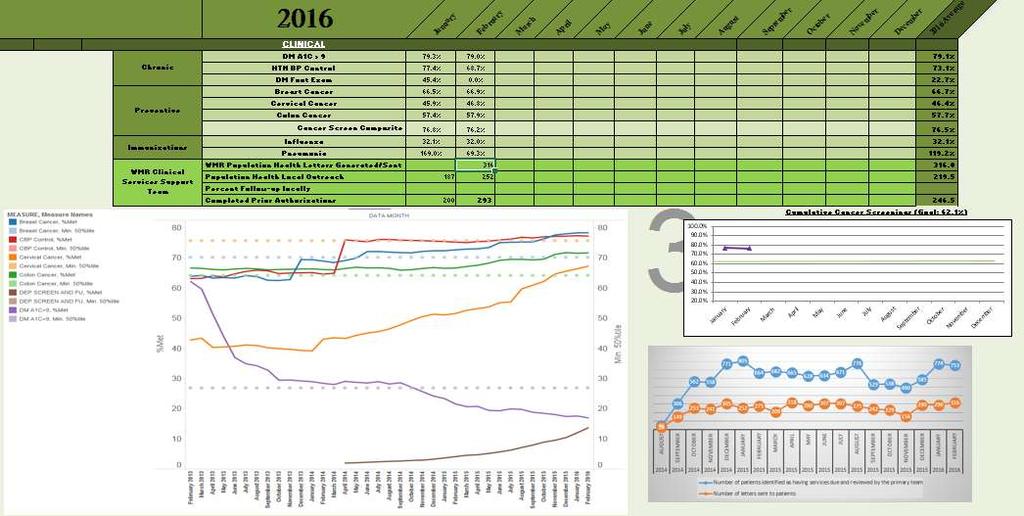
21 Monthly Dashboard- Example

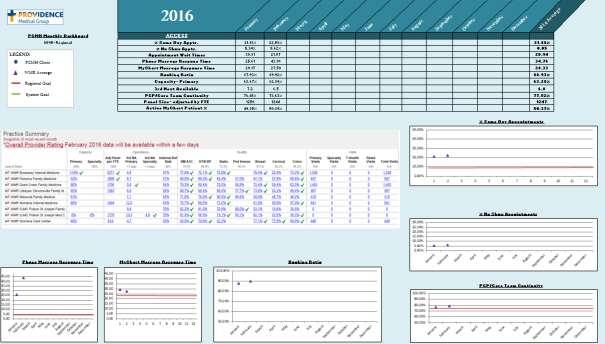
22 Provider Reporting- Example
23 Data/Metric Transmission
 under new MACRA legislation Source: CMS- Quality Initiatives Patient")
24 Continuous Quality Improvement Continual component of PCMH and value based models Strict data driven force- confidence in reporting functionalities! Team developed initiatives Embedded in future payment programs o PCMH is an example of Alternative Payment Models (APMs) under new MACRA legislation Source: CMS- Quality Initiatives Patient Assessment Instruments- Value Based Programs
25 Questions?
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
2017 HIMSS DAVIES APPLICANT
 2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Keith Salzman, M.D. Chief Medical Information Officer, IBM
 Keith Salzman, M.D. Chief Medical Information Officer, IBM Smarter Care through Transformation Keith L Salzman, MD, MPH CMIO-IBM GBS Federal keithsal@us.ibm.com USA 2012 Ogden UT IOM-The Healthcare Imperative:
Keith Salzman, M.D. Chief Medical Information Officer, IBM Smarter Care through Transformation Keith L Salzman, MD, MPH CMIO-IBM GBS Federal keithsal@us.ibm.com USA 2012 Ogden UT IOM-The Healthcare Imperative:
8 Factors for Success in the Transition to Value-Based Care
 8 Factors for Success in the Transition to Value-Based Care What does it take to successfully participate in value-based care programs? More than ever before, community practices are being challenged to
8 Factors for Success in the Transition to Value-Based Care What does it take to successfully participate in value-based care programs? More than ever before, community practices are being challenged to
Building the Oncology Medical Home. Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc.
 Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
New Models of Care- Looking at PCMH & Telehealth
 New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
Reimagining PCMH Recognition
 Reimagining PCMH Recognition August 2016 Michael S. Barr, MD, MBA, MACP Executive Vice President Quality, Measurement & Research Group Re-use without permission is prohibited 1 Where is PCMH in future
Reimagining PCMH Recognition August 2016 Michael S. Barr, MD, MBA, MACP Executive Vice President Quality, Measurement & Research Group Re-use without permission is prohibited 1 Where is PCMH in future
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018
 Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
Population Health Management. Ashley Rhude RHIA, CHTS-IM HIT Practice Advisor
 Population Health Management Ashley Rhude RHIA, CHTS-IM HIT Practice Advisor Mission of OFMQ OFMQ is a not-for-profit, consulting company dedicated to advancing healthcare quality. Since 1972, we ve been
Population Health Management Ashley Rhude RHIA, CHTS-IM HIT Practice Advisor Mission of OFMQ OFMQ is a not-for-profit, consulting company dedicated to advancing healthcare quality. Since 1972, we ve been
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
HIE Data: Value Proposition for Payers and Providers
 HIE Data: Value Proposition for Payers and Providers Session #21, March 6, 2018 Laura McCrary, Executive Director, KHIN Tara Orear, Senior Ambulatory Systems Analyst, Newman Regional Health Dirk Rittenhouse,
HIE Data: Value Proposition for Payers and Providers Session #21, March 6, 2018 Laura McCrary, Executive Director, KHIN Tara Orear, Senior Ambulatory Systems Analyst, Newman Regional Health Dirk Rittenhouse,
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community. Stewards of Change June 11, 2013
 An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
Care Coordination Overview. Janet Tennison, PhD UPV Standards October 8, 2013
 Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model. The New Accountable Care Business Model
 Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
Transitioning to a Value-Based Accountable Health System Preparing for the New Business Model Michael C. Tobin, D.O., M.B.A. Interim Chief medical Officer Health Networks February 12, 2011 2011 North Iowa
The content and/or presentation of the information will promote quality or improvements in healthcare and will not promote commercial interests
 Disclosure Statement: The content and/or presentation of the information will promote quality or improvements in healthcare and will not promote commercial interests UTILIZING POPULATION HEALTH DATA John
Disclosure Statement: The content and/or presentation of the information will promote quality or improvements in healthcare and will not promote commercial interests UTILIZING POPULATION HEALTH DATA John
Hudson Headwaters Journey to Patient Centered Medical Home Recognition
 Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations. April 26, 2018
 Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
The New York State Health Center Controlled Network (NYS-HCCN)
") The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Medicare Shared Savings Program ACO Learning System
 Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
Medicare Shared Savings Program ACO Learning System Coordinating Care for Beneficiaries with Complex Care Needs Wednesday, June 24, 2015 2:30 4:00 PM ET Audio for this session can be streamed through your
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management
 The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
The Value of Integrating EMR and Claims/Cost Data in the Transition to Population Health Management By Jim Hansen, Vice President, Health Policy, Lumeris November 19, 2013 EXECUTIVE SUMMARY When EMR data
Agenda. NE CAH Region Discussion
 NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Transforming Primary Care in the Adirondack Region of New York State
 Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Population Health. Collaborative Care. One interoperable platform. NextGen Care
 Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
Population Health. Collaborative Care. One interoperable platform. NextGen Care We ve become very proactive in identifying at-risk patients and getting them in our door before they get sick. Our physicians
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
COLLABORATING FOR VALUE. A Winning Strategy for Health Plans and Providers in a Shared Risk Environment
 COLLABORATING FOR VALUE A Winning Strategy for Health Plans and Providers in a Shared Risk Environment Collaborating for Value Executive Summary The shared-risk payment models central to health reform
COLLABORATING FOR VALUE A Winning Strategy for Health Plans and Providers in a Shared Risk Environment Collaborating for Value Executive Summary The shared-risk payment models central to health reform
Maximize the value of CHF population management programs with advanced analytics PLAYBOOK
 Maximize the value of CHF population management programs with advanced analytics PLAYBOOK STEP ONE: Analyze your patient population Bend the cost curve: Learning more about your patients can lead to higher-quality
Maximize the value of CHF population management programs with advanced analytics PLAYBOOK STEP ONE: Analyze your patient population Bend the cost curve: Learning more about your patients can lead to higher-quality
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Introducing AmeriHealth Caritas Iowa
 Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State
 Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
Population Health Management Tools to Improve Care for Individuals and Populations of Patients
 June 1, 2015 Population Health Management Tools to Improve Care for Individuals and Populations of Patients Joel Diamond, MD, FAAP Building Population Health Information-powered clinical decision-making
June 1, 2015 Population Health Management Tools to Improve Care for Individuals and Populations of Patients Joel Diamond, MD, FAAP Building Population Health Information-powered clinical decision-making
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination
 Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Insights as a Service. Balaji R. Krishnapuram Distinguished Engineer, Director of Analytics, IBM Watson Health
 Insights as a Service Balaji R. Krishnapuram Distinguished Engineer, Director of Analytics, IBM Watson Health Data & Knowledge Explosion: New data about individuals, used in new ways helps determines health
Insights as a Service Balaji R. Krishnapuram Distinguished Engineer, Director of Analytics, IBM Watson Health Data & Knowledge Explosion: New data about individuals, used in new ways helps determines health
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases?
 Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
Texas ACO invests in the Quanum portfolio to improve patient care
 Case study: Premier Management Company North Texas Texas ACO invests in the Quanum portfolio to improve patient care Premier Management Company (PMC) manages 3 accountable care organizations (ACOs) in
Case study: Premier Management Company North Texas Texas ACO invests in the Quanum portfolio to improve patient care Premier Management Company (PMC) manages 3 accountable care organizations (ACOs) in
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
PCMH Strategies Implementation and Sustainability 12/17/2013 Joseph K. Weidner, Jr. MD FAAFP
 PCMH Strategies Implementation and Sustainability 12/17/2013 Joseph K. Weidner, Jr. MD FAAFP Why is this needed? Defining a PCMH Improving Costs Better Provision of Care Improved Population Health PCMH
PCMH Strategies Implementation and Sustainability 12/17/2013 Joseph K. Weidner, Jr. MD FAAFP Why is this needed? Defining a PCMH Improving Costs Better Provision of Care Improved Population Health PCMH
2017 HIMSS DAVIES APPLICANT
 2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Implementing Patient-Centered Medical Home Pilot Projects:
 Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
AmeriHealth Michigan Provider Overview. April, 2014
 AmeriHealth Michigan Provider Overview April, 2014 Who We Are Our Mission Dual Demonstration of Michigan AmeriHealth VIP Care Plus Agenda Our Record of Success Integrated Care Management Provider Partnerships
AmeriHealth Michigan Provider Overview April, 2014 Who We Are Our Mission Dual Demonstration of Michigan AmeriHealth VIP Care Plus Agenda Our Record of Success Integrated Care Management Provider Partnerships
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future
 Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians
 Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:
 Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:") 2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS
 UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
UNITED STATES HEALTH CARE REFORM: EARLY LESSONS FROM ACCOUNTABLE CARE ORGANIZATIONS Stephen M. Shortell, Ph.D., M.P.H, M.B.A. Blue Cross of California Distinguished Professor of Health Policy and Management
Primary Care Renewal. Building Successful Practices In The Era Of Accountability Creating Contagious Change
 Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
A Values Based Approach to Accountable Care
 December 4, 2016 Orlando, FL A Values Based Approach to Accountable Care Evan Benjamin, MD, FACP George Kerwin, FACHE Saranya Loehrer, MD, MPH Agenda 2 Time 1:00pm-1:10pm 1:10pm-1:40pm 1:40pm-2:30pm 2:30pm-2:45pm
December 4, 2016 Orlando, FL A Values Based Approach to Accountable Care Evan Benjamin, MD, FACP George Kerwin, FACHE Saranya Loehrer, MD, MPH Agenda 2 Time 1:00pm-1:10pm 1:10pm-1:40pm 1:40pm-2:30pm 2:30pm-2:45pm
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services HANYS Solutions Patient-Centered Medical
 Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2015 HANYS Solutions Patient-Centered Medical Home Advisory Services Objectives After today s presentation, you will Understand how
Nicole Harmon, MBA, PCMH CCE Senior Director, PCMH Advisory Services 2015 HANYS Solutions Patient-Centered Medical Home Advisory Services Objectives After today s presentation, you will Understand how
Patient-Centered Specialty Practice Readiness Assessment
 Patient-Centered Specialty Practice Readiness Assessment Daryn Eikner Vice President, Health Care Delivery National Family Planning & Reproductive Health Association Melissa Kleder Manager, Health Care
Patient-Centered Specialty Practice Readiness Assessment Daryn Eikner Vice President, Health Care Delivery National Family Planning & Reproductive Health Association Melissa Kleder Manager, Health Care
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Using Updox to Succeed with MIPS
 Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts
 PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
PBGH Response to CMMI Request for Information on Advanced Primary Care Model Concepts 575 Market St. Ste. 600 SAN FRANCISCO, CA 94105 PBGH.ORG OFFICE 415.281.8660 FACSIMILE 415.520.0927 1. Please comment
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
NACDD and CDC Health Payer 101 Webinar Series. Webinar #4: Contracting 101
 NACDD and CDC Health Payer 101 Webinar Series Webinar #4: Contracting 101 Jennifer Nolty, Director, Innovative Primary Care National Association of Community Health Centers June 30, 2016 Contracting 101
NACDD and CDC Health Payer 101 Webinar Series Webinar #4: Contracting 101 Jennifer Nolty, Director, Innovative Primary Care National Association of Community Health Centers June 30, 2016 Contracting 101
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
The Future of Physician Reimbursement
 The Future of Physician Reimbursement EBG (PQRS-Quality Measures) yield Outcome Report Yield Increased Quality Yield Decreased Cost yield Increased Patient Satisfaction - CAHPS Consumer Assessment of Healthcare
The Future of Physician Reimbursement EBG (PQRS-Quality Measures) yield Outcome Report Yield Increased Quality Yield Decreased Cost yield Increased Patient Satisfaction - CAHPS Consumer Assessment of Healthcare
2014 PCMH STANDARDS. Renewals & Annual Data Requirements
 2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
FIVE FIVE FIVE FIVE FIV
 Technology and Data s Impact on Population Health FIVE FIVE FIVE FIVE FIV 5 Steps to an Effective and Sustainable Population Health Management Program This ebook will share critical information about population
Technology and Data s Impact on Population Health FIVE FIVE FIVE FIVE FIV 5 Steps to an Effective and Sustainable Population Health Management Program This ebook will share critical information about population
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
2.b.iii ED Care Triage for At-Risk Populations
 2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016
 Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016 Norris, Susan, Ph.D., Chief Clinical Officer, InfoMC Daniels, Allen S., Ed.D., Clinical Director,
Population Health Management Tools and Strategies to Support Care Coordination An InfoMC White Paper April 2016 Norris, Susan, Ph.D., Chief Clinical Officer, InfoMC Daniels, Allen S., Ed.D., Clinical Director,