The Pennsylvania Chronic Care Initiative
|
|
|
- Frederick Hill
- 6 years ago
- Views:
Transcription
1 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family Medicine Residency Program 1
2 Pilot to Mainstream Pennsylvania s Multi-stakeholder Chronic Care Initiative Extending the Work with CMS IBC s Approach to Primary Care Transformation in SEPA Transforming the Role of the Plan 2
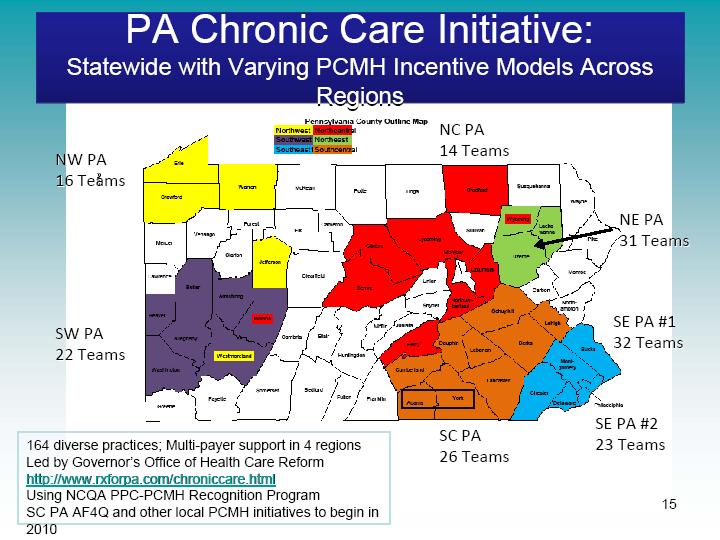
3 PA s Multi-stakeholder Chronic Care Initiative Distinguishing Features Government as Convener Multi-stakeholder participation Transformational care for all Transparent and adequate funding Practice support Scale to yield reliable outcomes Transferrable (regional and national) 3
4 Chronic Care Commission Goal - Improve chronic care delivery (access, quality, cost) Desired features of Pennsylvania model Regional Learning Collaborative rollouts Practice coach support Technology Registry/EMR, e-rx, open access scheduling Communication telephonic, encrypted Team health educators, case managers, CRNPs, PCPs Self-management skills Provider and consumer incentive alignment Third party assessment - NCQA PPC-PCMH Clinical, financial and satisfaction outcomes reporting 4
5 Role of GOHCR Convener Staffing Funding Consultants Faculty / expenses for year-long learning collaborative Registry Data collection, aggregation, evaluation and reporting activities through a 3 rd party, including surveys Coordinating Flow of data between practices and payers Flow of funds from payers to practices and IPIP Baseline and subsequent satisfaction surveys 5
6 Requirements of Primary Care Practices Attend Learning Collaborative meetings Team(s) from each practice Seven days in year 1, then less frequently Initial focus on diabetes and pediatric asthma Work with IPIP practice coach to transform practice Use a patient registry (or EMR) to track patients Report data from the patient registry and other sources required for evaluation purposes Achieve L1 NCQA PPC-PCMH Recognition* in year 1 Invest funds in staff and technology at practice site * Later rollouts have not required recognition in year 1; focusing on care mgmt. 6
7 Requirements of Payers Three year commitment to fund and support Payment to IPIP for Practice Coaches Payment to PCP Practices are intended to offset costs Infrastructure development Registry license /data entry NCQA recognition application / filing fee $9,515/practice Time for practice team to attend learning collaborative meetings Seven days during 1 st year $11,655/team Monthly or Quarterly payments that yield up to $4PMPM Support hiring care managers, health educators Support systems implementation (EMR, registry, e-rx, Addition of services that support self management Behavioral health integration 7
8 Requirements of IPIP Provide Practice Coaches to assist with Transforming the practice Data collection, aggregation, reporting and socializing Linking practices to community resources Completing the NCQA PPC-PCMH recognition process 8
9 Stakeholders in Collaboratives Participating Payers across 4 of 7 Regional Rollouts Commercial: Blues, Aetna, UPMC, Geisinger, CIGNA Medicaid: All Managed Medicaid Plans Medicare Advantage: Blues, Aetna Account for 75-80% of revenue Participating Practices Pediatric, Family Medicine, Internal Medicine, CRNP-led 1,000 FTEs (solo, small, medium and large) 1,200,000 Pennsylvanians Mix of independent, academic and FQHC practices The Primary Care Coalition (the RWJF IPIP grantee in PA) The PA Academy of Family Physicians The PA Chapter, American Academy of Pediatrics The PA Chapter, American College of Physicians 9
10 10


11 SE PA NCQA PPC-PCMH Recognition Dates from NCQA according to survey completion date 11
12 Building a Quality Medical Home Transforming VISIT POPULATION Management Measure with DATA Educate Physicians and ENTIRE Staff Redesign Work Flow Tasks for Staff; Decisions for Physicians Empower Employees Function at the highest level of job description VISIT Management Working SMARTER, not HARDER! No extra $$ spent time/energy only! INWARD Focus = VISIT Management (Numerator Management) 12
13 DM Foot Monofilament Testing Pct of DM patients w ith foot exam MAs Start Monofilaments Physicians Perform Monofilaments 13
14 DM Pneumovax Administration Pct of DM pts w ith pnuemo vacc 100 Pneumovax Lunch and Learn Session Ju Ju A S O N D Ja Fe M A M Ju Ju A S O N 14
15 Building a Quality Medical Home Transforming VISIT POPULATION Management Measure with DATA Educate Physicians and ENTIRE Staff Redesign Work Flow Tasks for Staff; Decisions for Physicians Empower Employees Function at the highest level of job description Hire Key PCMH Employee Develop Informed and Activated Patients Build Multidisciplinary Teams Involve the Community 15
16 Hire Key PCMH Employee Hire (full or part-time) a Case Manager RN Case Manager Level 1 billing for visits NP/PA Case Manager Level 2+ billing for visits Social Worker with CM skills Nonbillable Clinical Pharmacist?Billable for visits Certified Health Educator?Billable for visits Nutritionist/Dietician?Billable for visits OUTWARD Focus = PRACTICE Management (Denominator Management) 16
17 DM Foot Monofilament Testing: Denominator Management Example Pct of DM patients w ith foot exam MAs Start Monofilaments Physicians Perform Monofilaments Need Denominator Mgt 17
18 What Are The Practices Doing Focusing on planned visits to ensure patients get all needed care at visits Bringing patients in for overdue services Providing team-based care Establishing standing orders Overcoming clinical inertia with clinical guidelines Holding group visits Stratifying patients for care management and self-management support Setting goals with patients and following up on goals Producing patient report cards 18
19 Management of Diabetes % with A1C>9 % with A1C<7 S E P A 35% 30% 25% 20% 15% 10% 5% 0% 33% 27% 24% % 40% 35% 30% 25% 20% 15% 10% 5% 0% 35% 43% 43% S T A T E 19
20 Management of Diabetes % with BP < 140/90 % with BP < 130/80 S E P A 80% 70% 60% 50% 40% 30% 20% 10% 0% 75% 69% 57% % 70% 60% 50% 40% 30% 20% 10% 0% 45% 44% 47% S T A T E 20
21 Management of Diabetes % with LDL < 130 % with LDL < 100 S E P A 70% 60% 50% 40% 30% 20% 10% 0% 69% 62% 46% % 60% 50% 40% 30% 20% 10% 0% 35% 43% 43% S T A T E 21
22 Management of Diabetes % with Statin Script % with ACE/ARB Script S E P A 80% 70% 60% 50% 40% 30% 20% 10% 0% 57% 75% % 70% 60% 50% 40% 30% 20% 10% 0% 62% 77% S T A T E 22

23 Cost Savings of Diabetic Care 23

24 PCMH vs. Control Groups: Diabetes PCMH Groups Trends Members with Diabetes Control Groups Trends Members with Diabetes Care Gaps were about 50% fewer amongst members in PCMH practices 24

25 PCMH vs. Control Groups: Total Population PCMH Groups Trends Total Population Control Groups Trends Total Population 25
26 Evaluation IPIP reporting at practice and Collaborative level to support day to day practice level management Evaluation by UPMC and Rand Payer, provider, and survey data to be aggregated Collaborative practices to be compared to control practices both at a regional and a State-wide level Measurement domains: Engaged providers Patient self-care knowledge and skills Patient function and health status Primary care practice satisfaction Appropriate and efficient utilization of services Clinical care quality Cost 26
27 Quality Incentive Payment System Over 15 Years of Experience with focus on: Quality Measures (HEDIS, etc.) Generic Prescribing Access Provider Portal use Newly revised program rewards: Quality Measures (HEDIS, etc.) Generic Prescribing PCMH NCQA Recognition Level 1: $1.25PMPM Level 2: $2.00PMPM Level 3: $3.00 PMPM Medical Cost Management 27
28 Transforming the Role of the Plan Where should current Plan functions reside in a transformed PCMH world? Disease Management Decision Support Case Management What does the PCMH need from the Plan? Collaboration Accurate / Timely Information Tools / Support 28
29 National Health Care Transformation Demonstration Project Pennsylvania one of 8 States awarded by CMMI SEPA, NEPA and SCPA Chronic Care Initiatives $33M CMS infusion to PCMHs Commonwealth owns contract Extends the above CCIs for 3 additional years Will likely include IM and FM practices All Payers have committed to stay on with CMS Funding averages $4pmpm in a CM fee GOHCR seeking Shared Savings model 29
30 Transforming Primary Care Practice Questions? 30
Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model
 Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model Robert Gabbay MD, PhD Director, Penn State Institute for Diabetes and Obesity Professor of Medicine Penn State College
Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model Robert Gabbay MD, PhD Director, Penn State Institute for Diabetes and Obesity Professor of Medicine Penn State College
History of Pennsylvania s Chronic Care Initiative
 History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Collaboration in Pennsylvania: Rapidly Spreading Improved Chronic Care for Patients to Practices
 Original Research Collaboration in Pennsylvania: Rapidly Spreading Improved Chronic Care for Patients to Practices PATRICIA L. BRICKER, MBA; RICHARD J. BARON, MD, FACP; JORGE J. SCHEIRER, MD; DARREN A.
Original Research Collaboration in Pennsylvania: Rapidly Spreading Improved Chronic Care for Patients to Practices PATRICIA L. BRICKER, MBA; RICHARD J. BARON, MD, FACP; JORGE J. SCHEIRER, MD; DARREN A.
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010
 Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
PCMH to ACO: Carilion Clinic s Journey
 PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
NCQA s Patient-Centered Medical Home Recognition and Beyond. Tricia Marine Barrett, VP Product Development
 NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
How to Build a Medical Home
 How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home
 Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Employer Breakout Session Payment Change in Ohio: What it Means for Employers
 Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Employer Breakout Session Payment Change in Ohio: What it Means for Employers Moderators Jeff Biehl, Health Collaborative of Greater Columbus Frank A. Johnson, Maine Health Management Coalition Who is
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
New Models of Health Care: The Patient Centered Medical Home. Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
 New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model. ACO Congress November 5, 2013 Charles Kennedy
 Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Reimagining PCMH Recognition
 Reimagining PCMH Recognition August 2016 Michael S. Barr, MD, MBA, MACP Executive Vice President Quality, Measurement & Research Group Re-use without permission is prohibited 1 Where is PCMH in future
Reimagining PCMH Recognition August 2016 Michael S. Barr, MD, MBA, MACP Executive Vice President Quality, Measurement & Research Group Re-use without permission is prohibited 1 Where is PCMH in future
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions
 Project Frequently Asked Questions") Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
IT Enabled Care: Connecting the Dots EMR Validated Data - Driving Quality and Clinical Performance Improvement
 5 th National Pay for Performance Summit March 9, 2010 San Francisco, CA IT Enabled Care: Connecting the Dots EMR Validated Data - Driving Quality and Clinical Performance Improvement The Melting Pot Accountable
5 th National Pay for Performance Summit March 9, 2010 San Francisco, CA IT Enabled Care: Connecting the Dots EMR Validated Data - Driving Quality and Clinical Performance Improvement The Melting Pot Accountable
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
August 8, :00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell
 August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
August 8, 2013 12:00pm to 1:00pm Pamela Lester, Molly Layton and Janeen Boswell 1) NCQA PCMH Recognition, what it means and its process. 2) Understand the rationale and benefits of becoming recognized
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Catholic Medical Partners
 Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Medical Assistance Program Oversight Council. January 10, 2014
 Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD
 MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD Outline of Presentation Introduction Overview of MACRA/MIPS Clinical Practice Improvement Activities
MIPS Collaborative: Clinical Practice Improvement Activities April 19, 2017 Francis R Colangelo, MD Outline of Presentation Introduction Overview of MACRA/MIPS Clinical Practice Improvement Activities
A legacy of primary care support underscores Priority Health s leadership in accountable care
 Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
MULTI-STAKEHOLDER APPROACH TO VALUE-BASED HEALTHCARE
 MULTI-STAKEHOLDER APPROACH TO VALUE-BASED HEALTHCARE Randa Deaton, MA Corporate Director, UAW/Ford Community Healthcare Initiative Co-Executive Director, Kentuckiana Health Collaborative 1 WHO is the KHC?
MULTI-STAKEHOLDER APPROACH TO VALUE-BASED HEALTHCARE Randa Deaton, MA Corporate Director, UAW/Ford Community Healthcare Initiative Co-Executive Director, Kentuckiana Health Collaborative 1 WHO is the KHC?
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Paving the Way for. Health Homes
 Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
producing an ROI with a PCMH
 REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Opportunities to Promote CV Risk Reduction within the PCMH. Objectives. Disclosure 4/15/2013
 Opportunities to Promote CV Risk Reduction within the PCMH Cardiovascular Health Summit April 12, 2013 Billings, Montana F. Douglas Carr, MD, MMM, FACP Medical Director, Education & System Initiatives
Opportunities to Promote CV Risk Reduction within the PCMH Cardiovascular Health Summit April 12, 2013 Billings, Montana F. Douglas Carr, MD, MMM, FACP Medical Director, Education & System Initiatives
PATH Program. Getting Started Guide
 PATH Program Getting Started Guide We have a BIG opportunity. Together, we can empower and encourage people to take an active role in their health. Preventive health care services help people find and
PATH Program Getting Started Guide We have a BIG opportunity. Together, we can empower and encourage people to take an active role in their health. Preventive health care services help people find and
Maine PCMH Pilot & Community Care Teams: A Targeted Strategy to Improve Care & Control Costs for High Needs Patients
 Maine PCMH Pilot & Community Care Teams: A Targeted Strategy to Improve Care & Control Costs for High Needs Patients Lisa M. Letourneau MD, MPH May 2013 Maine PCMH Pilot & CCT Leadership DHA s Maine Quality
Maine PCMH Pilot & Community Care Teams: A Targeted Strategy to Improve Care & Control Costs for High Needs Patients Lisa M. Letourneau MD, MPH May 2013 Maine PCMH Pilot & CCT Leadership DHA s Maine Quality
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management
 Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management PCPCC June 26, 2014 Karen Jones MD FACP VP, Chief Medical Officer, WMG Laurie Brown BSN, MBA
Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management PCPCC June 26, 2014 Karen Jones MD FACP VP, Chief Medical Officer, WMG Laurie Brown BSN, MBA
Health Reform and The Patient-Centered Medical Home
 THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities
 CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities MODERATOR: Jonathan Sugarman, MD, MPH, President and CEO of Qualis Health SPEAKERS:
CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities MODERATOR: Jonathan Sugarman, MD, MPH, President and CEO of Qualis Health SPEAKERS:
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community. Stewards of Change June 11, 2013
 An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
University of Cincinnati Patient Centered Medical Home Leadership Decisions
 University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
Team Care Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc.
 2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012
 Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Dr. Kevin Rich Chief Medical Officer Family Medicine Residency of Idaho January 2016
 Dr. Kevin Rich Chief Medical Officer Family Medicine Residency of Idaho January 2016 IDAHO STATE HEALTH INNOVATION PLAN HOW DID WE GET HERE? Idaho Healthcare System Redesign Efforts 2007 Governor Otter
Dr. Kevin Rich Chief Medical Officer Family Medicine Residency of Idaho January 2016 IDAHO STATE HEALTH INNOVATION PLAN HOW DID WE GET HERE? Idaho Healthcare System Redesign Efforts 2007 Governor Otter
Patient Centered Care
 Patient Centered Care and dthe Future of Healthcare e Delivery e PCH Group Patient Centered Health Group A Division of R.S. Williamsand and Associates, Inc. Introduction PCMH Background and the Medical
Patient Centered Care and dthe Future of Healthcare e Delivery e PCH Group Patient Centered Health Group A Division of R.S. Williamsand and Associates, Inc. Introduction PCMH Background and the Medical
Building the Oncology Medical Home John D. Sprandio, M.D., FACP Consultants in Medical Oncology & Hematology, P.C. Oncology Management Services, LLC
 Building the Oncology Medical Home John D. Sprandio, M.D., FACP Consultants in Medical Oncology & Hematology, P.C. Oncology Management Services, LLC Oncology Patient-Centered Medical Home Update Background
Building the Oncology Medical Home John D. Sprandio, M.D., FACP Consultants in Medical Oncology & Hematology, P.C. Oncology Management Services, LLC Oncology Patient-Centered Medical Home Update Background
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Patient-Centered Medical Home Best Practices: Case Study Examples
 Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Performance Incentives in the Southern California Permanente Medical Group (SCPMG):
:") Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Blue Quality Physician Program: Detailed Overview
 2018 Blue Quality Physician Program: Detailed Overview Program Definition The Blue Quality Physician Program is comprised of many components with one purpose: improve the care and quality for our members.
2018 Blue Quality Physician Program: Detailed Overview Program Definition The Blue Quality Physician Program is comprised of many components with one purpose: improve the care and quality for our members.
Incorporating the ABMS MOC
 A Blue Cross and Blue Shield Association Presentation Incorporating the ABMS MOC An Alternative to the Use of Claims-based Metrics for P4P Sarah Begor, MS, CMPE BlueCross BlueShield Association Jason Aronovitz,
A Blue Cross and Blue Shield Association Presentation Incorporating the ABMS MOC An Alternative to the Use of Claims-based Metrics for P4P Sarah Begor, MS, CMPE BlueCross BlueShield Association Jason Aronovitz,
PCMH and the Care of Complex High Cost Patients
 PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
A. DIABETES AND HEART/STROKE Data Detail
 A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
The Virtual Connection: Electronic Visits. Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009
 The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
Practice Transformation Network (PTN) An Overview for FQHC Leadership
 An Overview for FQHC Leadership") Practice Transformation Network (PTN) An Overview for FQHC Leadership PTN What Is It? The Practice Transformation Network is: A group that joins together (CHCACT member organizations, specialty providers,
Practice Transformation Network (PTN) An Overview for FQHC Leadership PTN What Is It? The Practice Transformation Network is: A group that joins together (CHCACT member organizations, specialty providers,
Value-Based Models: Two Successful Payer-Provider Approaches March 1, 2016
 Value-Based Models: Two Successful Payer-Provider Approaches March 1, 2016 Clifford T. Fullerton, MD, MSc President, Baylor Scott & White Quality Alliance Chief Population Health Officer, Baylor Scott
Value-Based Models: Two Successful Payer-Provider Approaches March 1, 2016 Clifford T. Fullerton, MD, MSc President, Baylor Scott & White Quality Alliance Chief Population Health Officer, Baylor Scott
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care
 Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Patient-Centered Primary Care
 Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
Patient-Centered Primary Care Greg Moody, Director Office of Health Transformation July 30, 2014 www.healthtransformation.ohio.gov Agenda 1. Health System Challenges 2. Health System Trends in Primary
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
The PCMH St Joseph s Experience
 The PCMH St Joseph s Experience Priya Radhakrishnan, MD Roshni Kundranda, MD, MSPH Binh Doung, DO Jenni Schroeder, RN, BSN ACP Regional Meeting Tucson, 2013 Disclosure No financial conflicts of interest
The PCMH St Joseph s Experience Priya Radhakrishnan, MD Roshni Kundranda, MD, MSPH Binh Doung, DO Jenni Schroeder, RN, BSN ACP Regional Meeting Tucson, 2013 Disclosure No financial conflicts of interest
Our Response to Health Reform: Collaborative Initiatives for Success
 Our Response to Health Reform: Collaborative Initiatives for Success February 11, 2012 Joseph R Swedish, FACHE President and CEO Trinity Health Trinity Health: Unified Enterprise Ministry Serving Ten States
Our Response to Health Reform: Collaborative Initiatives for Success February 11, 2012 Joseph R Swedish, FACHE President and CEO Trinity Health Trinity Health: Unified Enterprise Ministry Serving Ten States
Performance Measurement Work Group Meeting 10/18/2017
 Performance Measurement Work Group Meeting 10/18/2017 Welcome to New Members QBR RY 2020 DRAFT QBR Policy Components QBR Program RY 2020 Snapshot QBR Consists of 3 Domains: Person and Community Engagement
Performance Measurement Work Group Meeting 10/18/2017 Welcome to New Members QBR RY 2020 DRAFT QBR Policy Components QBR Program RY 2020 Snapshot QBR Consists of 3 Domains: Person and Community Engagement
Restructuring Healthcare The Role of Technology
 Restructuring Healthcare The Role of Technology Philip Gaziano, MD October 11, 2012 2 Physician Owned & Lead Organizations Accountable Care Associates, LLC (ACA): Founded in 2010, it is physician owned
Restructuring Healthcare The Role of Technology Philip Gaziano, MD October 11, 2012 2 Physician Owned & Lead Organizations Accountable Care Associates, LLC (ACA): Founded in 2010, it is physician owned
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Clinical Integration & ACO Contracting
 & Clinical Integration & ACO Contracting 1 The First TXCIN ACO Contract: Cigna Collaborative Accountable Care (CAC) Benefits of ACO Contract Participation: 1. Patients Attributed to PCPs (IM, FP, PEDS,
& Clinical Integration & ACO Contracting 1 The First TXCIN ACO Contract: Cigna Collaborative Accountable Care (CAC) Benefits of ACO Contract Participation: 1. Patients Attributed to PCPs (IM, FP, PEDS,
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Weaving Expanded Roles of the RN into Population Management
 Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
FINANCING THE PEDIATRIC MEDICAL HOME. Mark Weissman, MD, FAAP Maryland AAP Meeting September 8, 2012
 FINANCING THE PEDIATRIC MEDICAL HOME Mark Weissman, MD, FAAP Maryland AAP Meeting September 8, 2012 Faculty disclosures No conflicts of interest Additional disclosures I am a very general pediatrician
FINANCING THE PEDIATRIC MEDICAL HOME Mark Weissman, MD, FAAP Maryland AAP Meeting September 8, 2012 Faculty disclosures No conflicts of interest Additional disclosures I am a very general pediatrician