Organized, Evidence-based Care
|
|
|
- William Gilbert
- 5 years ago
- Views:
Transcription
1 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner, MD, MPH, Director and Senior Investigator, MacColl Institute for Healthcare Innovation, Group Health Research Institute Brian Austin, Associate Director, MacColl Institute for Healthcare Innovation, Group Health Research Institute Central City Concern: Krista Collins, Data Analyst Idaho State University Department of Family Medicine: John Holmes, PharmD
2 Delivering Organized, Evidence- Based Care: The Heart of the Medical Home Ed Wagner, MD, MPH, MACP and Brian Austin MacColl Institute for Healthcare Innovation Group Health Research Institute Safety Net Medical Home Initiative June 7, 2011
3 Understanding the origins of the Patient-Centered Medical Home 1. Pediatric Medical Home 2. The Centrality of Primary Care First-contact Care Responsibility over time Comprehensive Coordination across providers, settings and conditions 3. Redesigned Systems of Care (aka, the Chronic Care Model)
4 Medical home Chronic Care Model Duplicative, Complementary or Antagonistic? Both models advocate that every health care experience (visit, referral, admission, etc) connects the patient back to their PCP. Both emphasize and support patient role in decisionmaking and care Both the PCMH and CCM rest on the clinical evidence of practice changes that lead to improvements in patient care and outcomes. PMH underscores primary care s responsibility for access, continuity, comprehensiveness, and coordination CCM redesigns care delivery for planned, whole person care
5 Changing demography and practice content Proportion of Office Visits for Chronic Illness Care by Age All patients Chronic Problem, Routine 30% Chronic Problem, Flare-up 9% Age Age Age % 37% 42% 9% 10% 11% NAMCS, Advance Data No. 387, 2007
6 What do Chronically Ill Patients Need to Optimize Outcomes? A continuous healing relationship Clinical therapy that gets them safely to the therapeutic goals Effective self/family-management Services to meet major clinical and other needs, and coordination of those services Preventive interventions at recommended time Evidence-based monitoring and self-monitoring Follow-up tailored to severity
7 Patient Needs Practice Roles/Functions Drug therapy that gets them safely to the therapeutic target Effective self-management support Medication Management Self-management Support Preventive interventions at recommended time Visit Planning/Population Management Evidence-based monitoring and follow-up tailored to severity Follow-up/Care Management Coordinated services Care Coordination
8 Population Management Population management Maintain a database (Registry) that includes key information on important patient groups within a practice population. Monitor the database to identify and reach out to those needing service.
9 Medication Management Many chronic conditions treated by stepped care protocols that increase treatment intensity to reach goal. Clinical Inertia Treatment is often not changed in visits with individuals not achieving therapeutic goals. Medication Management Nurses or other care managers initiate and monitor, by telephone or brief visit, medication adjustment in patients not at goal. Requires agreement on and use of evidence-based protocols.
10 Clinical Inertia Patient has not reached treatment goal Patient is taking medications as prescribed Therapy (usually limited to drugs) has not been intensified First described by Phillips et al., Ann Int Med 2001
11 Care Management The provision of more intensive monitoring, clinical management, and self-management support to high risk patients. Usually provided by a nurse or other health professional.
12 Care Coordination Developing linkages and agreements with specialists and community resources Helping patients access outside resources Assuring timely flow of relevant information to and from referral sources
13 Three Areas of Emphasis in this Guide 1. Planned Care. 2. Decision Support. 3. Care Management.
14 The Importance of Planned Care Only half of recommended services are delivered Care is often reactive, even though many patient needs are predictable Planned Care creates an agenda for the encounter Planned Care can be delivered in patient- or provider-initiated visit, or even opportunistically
15 What is a Planned Visit? A Planned Visit is an encounter that uses patient data, team and practice organization, and decision support to assure a productive interaction. Can be patient-initiated or practice-initiated Pre-visit planning (huddle) assures that patient needs are met; post-visit huddle assures followup.
16 Steps for Planned Care 1. Identify the key clinical tasks associated with evidence-based care 2. Decide who on the team should do the task 3. Review patient data prior to the encounter to identify needed services 4. Structure the encounter so the relevant team members deliver all needed care
17 Decision Support Embed evidence-based guidelines into daily clinical practice. Integrate specialist expertise and primary care. Use proven provider education methods. Share guidelines and information with patients.
18 Decision Support Can be linked to ordering a clinical service or triggered via patient data Increasingly built into EMRs, making the right thing to do the easy thing to do. Meaningful Use core criteria place special emphasis on decision support mechanisms
19 Will greater sharing of care between primary and specialty care improve care for complex patients? Recent meta-analysis* of interventions to increase collaboration between primary and specialist physicians found consistently positive effects on patient outcomes in mental illness and diabetes. Effective interventions include: < interactive communication telephone, , videoconference < quality of information structured information, pathways to improve information quality < Needs assessment input based on initial and continuing identification and tracking of needs. It is not clear how this might work with the multi-problem patient. * Foy et al. Ann Int Med 2010; 152:
20 Care Management Usually provided by a nurse or other health professional. Care management is far more effective when the care manager: < is an integral member of the practice team < can influence medications < is supported by relevant medical specialist(s).
21 Relationship Between Care Coordination and Care Management Activities in Primary Care Logistical Clinical Care Management Medication mgmt Logistical Clinical Monitoring Clinical Follow-up Care Clinical Monitoring Care Coordination Logistical MacColl Institute for Healthcare Innovation, Group Health Research Institute 2011
22 Will care manager interventions be effective for multi-problem patients? Nurse and pharmacist care manager interventions improve outcomes in diabetes, depression, bipolar disorder, CHF, etc. Care managers in studies usually have experience and expertise in the targeted condition. Some care manager interventions now targeting complex patients with evidence of effectiveness e.g., TeamCare*,Guided Care. Integration of the care manager with primary care appears critical. *Katon et al., NEJM (27): p
23 Implementing Care Management 1. Decide which populations are to be managed 2. Choose which services are required 3. Develop and use a case identification strategy 4. Identify and train a clinical care manager 5. Create a support structure for the manager

24 A toolbox for improving care systems

25 What s in the Kit Step by step advice on Implementing the CCM Over 60 tools hyperlinked Additional resources cataloged A companion practice coaching manual is also available. Find it at:
26 To learn more: Thanks

27 Point-of-Care Reminders in a Paper-Based World Creating Delivery Systems that Drive Patient Care Krista Collins, Data Analyst

28 The Old Town Clinic FQHC and Safety Net clinic located in Portland, Oregon Part of Central City Concern, one of Portland s largest agencies serving single adults and families impacted by homelessness, poverty and addiction. The clinic sees 2,600 patients annually, with over 15,000 visits Of those, 40% of patients are uninsured, and the majority are < 100% FPL Up until May of 2011, the OTC did not have an EMR system in place for providing patient care
29 Without an EMR, we had to be creative And one very creative idea lead to an entirely new innovative process One Panel Manager created a handwritten form (called a Health Summary ) to summarize chronic disease prevention measures for each patient on her panel prior to their visit. The format was later standardized by one of our providers, who added several other crucial health measures to track. The OTC Operations Team coordinated with our IT dept to create an electronic version of this form. The modern day Health Summary - an electronic form printed before every GM appointment that summarizes a patient s recent lab results, imaging results and vitals at last visit.

30 Health Summary Highlights Focuses on populationspecific needs for OTC pts Lists last test date / last results Testing criteria displayed for reference Highlights pay for performance measures Printed prior to every GM visit
31 The Health Summary Who Makes it Happen? (Designed Delivery System) Health Assistant - Team Assistant enters data into CCCER (labs imported automatically); prints Health Summary before each session Panel Managers - Patient Care Coordinators Coordinates care of panels and supports the PCP in clinical care assessment (huddles) Medical Assistants facilitates communication with patient about needed tests, place orders schedules tests after visit Providers - The patient s PCP; oversees all clinical care with each patient and signs off on referrals /orders Medical Records Identifies records (mammograms, DEXA scans) and routes them from fax directly to Health Assistant The Health Summary From Start to Finish (Healthcare Organization) Health Assistant prints HS form & attaches it to the chart PM reviews during huddle prep and highlights next steps for provider Provider coordinates w MA to order tests / exams prior to appt MA talks w pt during check-in and arranges tests / orders if patient agrees HS is placed in chart and discarded only when a new form is printed
32 HBA1C Tests Performed 100% The Result Quick and Efficient Patient Data that Drives Patient Care 80% 60% 65% 64% 67% 71% 73% 71% 70% 40% 20% 0% If reminding providers is All that we need to do, then why wasn t there more of an improvement? Q Q Q Q Q Q Q1 2011
33 Important Lessons Learned Point of care reminders, while very helpful, for us only created a modest improvement in our measures POC Reminders don t reach patients that do not visit the clinic on a regular basis Tyranny of the urgent during appointments is still is an issue Every visit to the clinic-especially a medical home-is not created equal due to the variety of services offered Patients were visiting the clinic, but not necessarily for a PCP appt but for mental health, specialty visits (LAOC, OT, etc), thus bypassing the Health Summary process Definitions need to be established as to who can act on point-of-care reminders (e.g. if a MH clinician notices a pt needs an HBA1c, what do they do?) Patients with complex conditions often require more time for appointments Huddles are extremely vital in mitigating this issue, and organizing labs prior to the appt is essential. Entire team needs to commit to attending and acting on huddle this is now one of our team in process measures
34 The next steps for the OTC on improving patient-centered care: Proactive and Organized Outreach Accurate Panels / regimented cleaning process Data - Recording in-process measures that drive patient care and improvement Adapting our Health Summary to our new EMR we miss it! It is not enough to do your best; you must know what to do, and then do your best. Dr. W. Edwards Deming
35 ORGANIZED EVIDENCE-BASED CARE DIABETES EMR TEMPLATE John Holmes, PharmD Idaho State University Department of Family Medicine
36 CLINIC AND PATIENT DEMOGRAPHICS Family Medicine Residency Currently a residency 6-7 new resident providers every year Patients Mostly Caucasian About 30% have private health insurance About 35% have Medicare and 25% have Medicaid About 10% uninsured Pocatello, Idaho About 80,000 people in the greater Pocatello area Serve many patients from rural areas around Pocatello
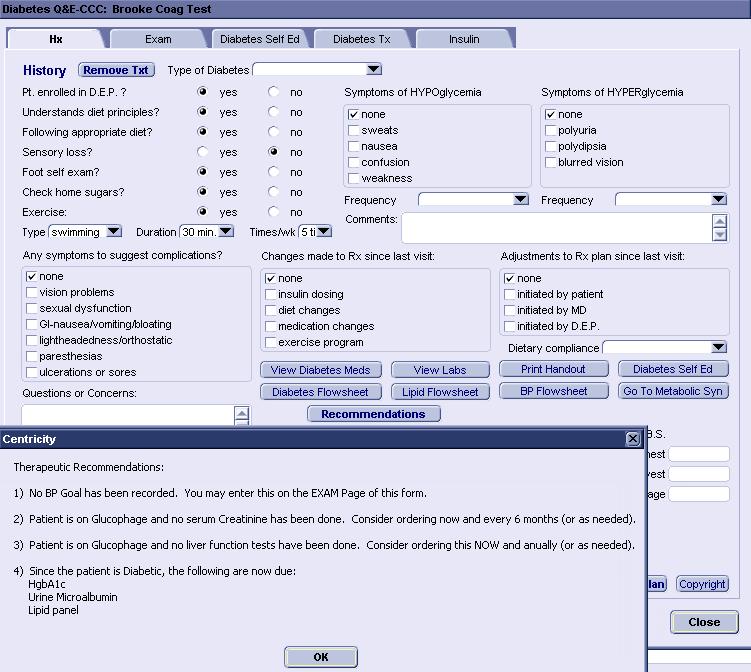
37
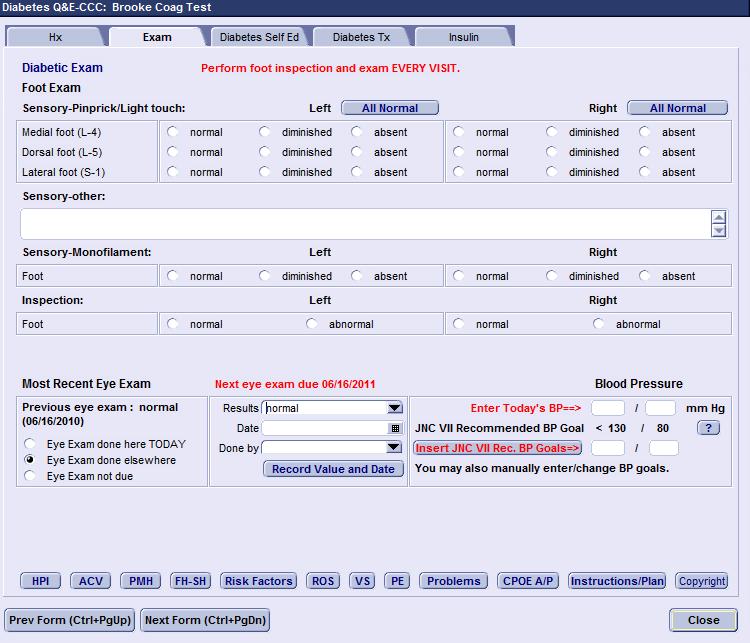
38

39
40 OTHER CUSTOMIZED TEMPLATES Depression Congestive heart failure Asthma Back pain Osteoporosis Dyspepsia Headache Smoking Cessation Hypertension Dyslipidemia Obesity Metabolic syndrome Menopause Diabetes Preventive care
41 BENEFITS OF EMR TEMPLATES Standardized entry of data into the EMR Easily searchable data for QI initiatives diabetes eye exams, foot exams, etc. Patient-centered clinical decision support Aid providers in appropriately assessing, evaluating, and treating patients Significant role in FM residency program (training tool) Easily accessible provider and patient education materials Customization of templates Improved efficiency and quality of care


42 % OF ADULT PATIENTS WITH DIABETES AT GOAL HBA1C LEVELS 100% 90% 80% 70% 60% 50% 40% 30% 9% 7 - <9% <7% 20% 10% 0%
43 % OF DM PATIENTS WITH DOCUMENTED DIABETIC EYE AND FOOT EXAM 90% 80% 70% 60% 50% 40% 30% 20% Eye Exam Foot Exam 10% 0%
44 BARRIERS TO TEMPLATES Universal use Discuss new templates at department/resident meetings 1 EMR noon conference/month EMR committee Individual meetings with staff/providers if necessary Work flow issues Time intensive training Need to update templates frequently
45




46 SNMHI Sponsors and Co-Funders
Deeper Dive on Team Roles: Part I
 Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Does The Chronic Care Model Work?
 Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Patient Centered Medical Home
 Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A)
") SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
SAFETY NET MEDICAL HOME INITIATIVE
 SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
Topic 4A: Foundational Changes Reducing Barriers to Care Webinar
 The Patient-centered Medical Home Webinar #4 Topic 4A: Foundational Changes Reducing Barriers to Care Webinar Ed Wagner, MD, MPH, MACP MacColl Center for Health Care Innovation Group Health Research Institute
The Patient-centered Medical Home Webinar #4 Topic 4A: Foundational Changes Reducing Barriers to Care Webinar Ed Wagner, MD, MPH, MACP MacColl Center for Health Care Innovation Group Health Research Institute
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Transforming Care for Vulnerable Populations:
 Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Primary Care Transformation in Academic Medical Centers. Objectives of Session
 Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
Kern County s Health Care Coverage Initiative Network Structure: Interim Findings
 Kern County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The Health Care Coverage Initiative (HCCI) program in Kern County is known as the Kern Medical Center Health
Kern County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The Health Care Coverage Initiative (HCCI) program in Kern County is known as the Kern Medical Center Health
New Models of Care- Looking at PCMH & Telehealth
 New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Catholic Medical Partners
 Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Where Do We Go From Here? The Value of Sustaining Practice Transformation
 Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health
 PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Community Health Centers: Medical Homes in the Safety Net. Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health
 Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Working at Top of License How do you reallocate work among a team? January 28, 2015
 Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Medicaid Payments to Incentivize Delivery System Reform Webinar Dec. 17, :00 3:00 pm ET
 Medicaid Payments to Incentivize Delivery System Reform Webinar Dec. 17, 2013 2:00 3:00 pm ET TODAY S SPEAKERS: Beth Feldpush, DrPH Senior Vice President for Policy and Advocacy, America s Essential Hospitals
Medicaid Payments to Incentivize Delivery System Reform Webinar Dec. 17, 2013 2:00 3:00 pm ET TODAY S SPEAKERS: Beth Feldpush, DrPH Senior Vice President for Policy and Advocacy, America s Essential Hospitals
Deeper Dive on Team Roles: Part 2
 Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Patient Centred Medical Home Self-assessment (PCMH-A)
") Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs
 Transformation and Recognition/Certification Programs") Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Rina Ramirez, MD, FACP Teresita Lawson, BSPharm, RPh, CDE Suyen Segura, MPH, CHES
 Rina Ramirez, MD, FACP Teresita Lawson, BSPharm, RPh, CDE Suyen Segura, MPH, CHES 1 Name three approaches that address specific health needs of seniors Discuss how different disciplines may be integrated
Rina Ramirez, MD, FACP Teresita Lawson, BSPharm, RPh, CDE Suyen Segura, MPH, CHES 1 Name three approaches that address specific health needs of seniors Discuss how different disciplines may be integrated
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home Domains of Function. Interpretive Guidelines
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
New Models of Health Care: The Patient Centered Medical Home. Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
 New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
Improvement Activities Data Validation Criteria
 Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Staying Connected with Patient-Generated Health Data
 Staying Connected with Patient-Generated Health Data April 14, 2015 Dr. Danny Sands, Chief Medical Officer Dr. Philip Marshall, Chief Product Officer DISCLAIMER: The views and opinions expressed in this
Staying Connected with Patient-Generated Health Data April 14, 2015 Dr. Danny Sands, Chief Medical Officer Dr. Philip Marshall, Chief Product Officer DISCLAIMER: The views and opinions expressed in this
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Health Coaching in Team-Based Care. Recipes for Success
 Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
RN Behavioral Health Care Manager in Behavioral Health Settings
 RN Behavioral Health Care Manager in Behavioral Health Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Behavioral Health Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion. All Ohio Institute on Community Psychiatry March 25, 2017
 Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities
 CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities MODERATOR: Jonathan Sugarman, MD, MPH, President and CEO of Qualis Health SPEAKERS:
CMS FQHC Advanced Primary Care Practice Demonstration: NCQA Recognition Support and Other New Federal PCMH Opportunities MODERATOR: Jonathan Sugarman, MD, MPH, President and CEO of Qualis Health SPEAKERS:
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
PCMH and the Care of Complex High Cost Patients
 PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Keenan Pharmacy Care Management (KPCM)
") Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
History of Pennsylvania s Chronic Care Initiative
 History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
The New York State Health Center Controlled Network (NYS-HCCN)
") The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
INTEGRATING SELF-MANAGEMENT FOR CHRONIC ILLNESSES AND PREVENTIVE BEHAVIORS INTO HEALTH CARE
 INTEGRATING SELF-MANAGEMENT FOR CHRONIC ILLNESSES AND PREVENTIVE BEHAVIORS INTO HEALTH CARE Russell E. Glasgow, Ph.D. Kaiser Permanente Colorado Denver, Colorado Overview of Presentation! The Health Care
INTEGRATING SELF-MANAGEMENT FOR CHRONIC ILLNESSES AND PREVENTIVE BEHAVIORS INTO HEALTH CARE Russell E. Glasgow, Ph.D. Kaiser Permanente Colorado Denver, Colorado Overview of Presentation! The Health Care
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
An RHC Patient Centered Medical Home Experience
 An RHC Patient Centered Medical Home Experience NARHC October 19, 2017 Kate Hill, RN The Compliance Team MACRA Recognition TCT Recognized for it s PCMH Program Today s Objectives Understand the difference
An RHC Patient Centered Medical Home Experience NARHC October 19, 2017 Kate Hill, RN The Compliance Team MACRA Recognition TCT Recognized for it s PCMH Program Today s Objectives Understand the difference
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This