Building & Strengthening Patient Centered Medical Homes in the Safety Net
|
|
|
- David Carson
- 5 years ago
- Views:
Transcription

1 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips, MPH Regina Neal, MPH MS
2 Objectives Review the history, structure, and promise of the PCMH model Review the SNMHI model change package for Practice Transformation Review payment and financing considerations Understand lessons from the field on PCMH implementation 2
3 The PCMH: Overview 3
4 What is a Patient-Centered Medical Home? A model of comprehensive, coordinated care that assures: Patient-centered approach to care delivery Enhanced access to services A holistic view of the patient Continuity of care A focus on continuous performance measurement and improvement 4
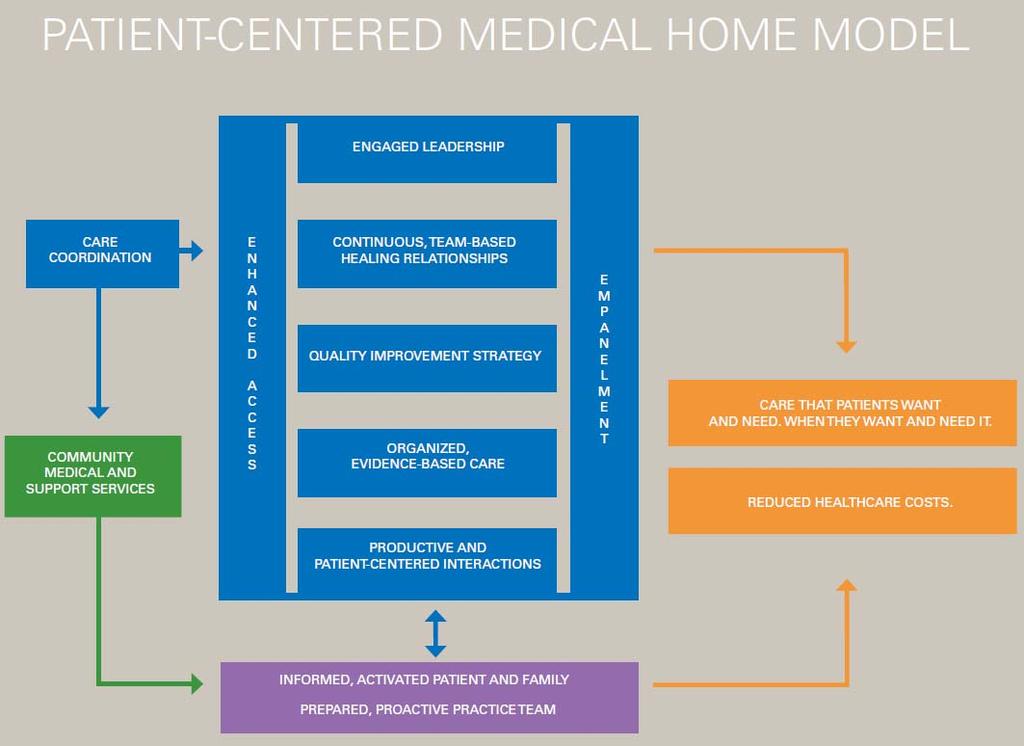
5 5
6 Typical Practice Setting Providers are responsible for the universe of patients who seek care in the practice. Care is delivered in reaction to today s problem. Providers believe that their extensive training translates to high quality care. Care varies by scheduled time and memory or skill of the provider. The productivity treadmill requires providers to work harder and assume longer work days. The provider functions as a solo act, even when support staff are available. PCMH Care Patients are paired with a continuity provider who is responsible for a defined panel of patients. Care is determined by a proactive plan to meet health needs, with or without clinic visits. Quality is assured through the measurement of adherence to evidence-based guidelines, and we develop action plans to continuously improve the quality of care we provide. The practice aligns appointment capacity with appointment demand, adjusting staffing and other variables to balance the workload. An interdisciplinary team works together to serve patients efficiently and effectively, coordinating care, tracking tests and consultations, and providing outreach and follow-up after ED visits and hospitalizations. 6
7 Why Create a Medical Home? Enhanced access to care Improved clinical outcomes Reduced health disparities Improved patient experience Improved staff satisfaction Greater efficiency in care delivery Reduced cost of healthcare overall 7
8 Who Else is Doing This? Pilots/demonstration or projects in 39 states (NASHP, Feb ) Health plans NC 2011) State Medicaid agencies State primary care associations Private foundations Public-private partnerships QA PCMH recognition stats (NCQA, April 10,100 + clinicians 2189 sites 45 states 8
9 Published Outcomes 15%-20% reduced healthcare spending Patients at PCMH sites have 15%-20% reduced total healthcare spending per year compared to patients treated by regional peers. 1 Group Health Cooperative, Seattle, WA 2 4% increase in patients meeting target levels on HEDIS measures 29% reduction in emergency department utilization 16% reduction in avoidable hospitalizations Utilization changes resulted in a net cost reduction of $10.30 PMPM. ROI: Saved $1.50 for every $1.00 invested in its PCMH program. Gennesee Health Plan, Flint, MI 2 74% improvement in preventive care measures 35% improvement in diabetes care measures 50% decrease in ER visits 15% fewer inpatient hospitalizations 1. Milstein A, Gilbertson E. American Medical Home Runs: Four real life examples of primary care practices that show a better way to substantial savings. Health Aff (Millwood). 2009;28(5): Rogers, E. Patient Centered Medical Home. Patient Centered Primary Care Collaborative. centered medicalhome. Accessed March 23,
10 Change Concepts for Practice Transformation
11 Change Concepts 1. Empanelment 2. Continuous and Team-based Healing Relationships 3. Patient-centered Interactions 4. Engaged Leadership 5. Quality Improvement Strategy (includes HIT) 6. Enhanced Access 7. Care Coordination 8. Organized, Evidence-based Care 11
12 Development Safety Net Medical Home Initiative Sponsored by The Commonwealth Fund and conducted in partnership with the MacColl Institute for Healthcare Innovation Developed by Technical Expert Panel in 2008 Vetted by the WA State PCMH Collaborative and now used by many others 12
13 Sequencing and Emphasis 1. Empanelment 2. Continuous and Team-based Healing Relationships 3. Patient-centered Interactions 4. Engaged Leadership 5. Quality Improvement Strategy (includes HIT) 6. Enhanced Access 7. Care Coordination 8. Organized, Evidence-based Care 13

14 Engaged Leadership Quality Improvement Strategy (includes HIT) Empanelment Continuous and Team-based Healing Relationships Patient-centered Interactions Enhanced Access Care Coordination Organized, Evidence-based Care 14
15 PCMH-A Background & Context Developed to measure a site s progress towards achieving the 8 Change Concepts Self-administered assessment Aids in the identification of improvement opportunities Stimulates conversations with other sites to learn, share, & transform Serves as a standardized measure of progress 15
16 PCMH-A Self-Assessment Sample Empanelment Questions Components Level D Level C Level B Level A Patients are not assigned to specific patient panels are assigned to specific practice panels but panel assignments are not routinely used by the practice for administrative or other purposes. are assigned to specific practice panels and panel assignments are routinely used by the practice mainly for scheduling purposes. are assigned to specific practice panels and panel assignments are routinely used for scheduling purposes and are continuously monitored to balance supply and demand. Score Registry or panel data are not available to assess or manage care for practice populations are available to assess and manage care for practice populations, but only on an ad hoc basis. are regularly available to assess and manage care for practice populations, but only for a limited number of diseases and risk states. are regularly available to assess and manage care for practice populations, across a comprehensive set of diseases and risk states. Score



17 SNMHI PCMH Resources PCMH-A Implementation guides Policy briefs Medical Home Digest Webinars Videos 17
18 Thoughts on Payment Reform 18
; (3) explicitly intended to advance medical homes for Medicaid or CHIP participants; and (4) evidence of commitment, such as workgroups, legislation, executive orders, or")
19 PCMH Landscape: Transformation and Financing 39 states Medical Home States : (1) program implementation (or major expansion or improvement) in 2006 or later; (2) Medicaid or CHIP agency participation (not necessarily leadership); (3) explicitly intended to advance medical homes for Medicaid or CHIP participants; and (4) evidence of commitment, such as workgroups, legislation, executive orders, or dedicated staff. 74 medical home projects nationally 46 include enhanced payment 19
20 The Case for PCMH Financing Why Payment Reform? Value over volume Move away from visit churn Reward outcomes Clinical quality Patient experience Cost reductions Incentivize primary care Workforce Coordinated care Why Enhanced Payment? Infrastructure support Telephone and system upgrades, HIT New staff Lost revenue during QI work Staff training Proactive outreach Traditionally unreimbursed services Telephonic and visits Group visits Education/support visits Multiple visits in single day 20

21 10 PCMH Payment Models 5 categories: FFS w/ adjustments FFS plus Shared savings Comprehensive Grant-based FFS: Fee for service PMPM: Per member per month PMPY: Per member per year 21
22 Tiering Payments Participation Level of recognition / certification Learning collaborative Data submission Complexity Patient characteristics Population characteristics Medical Social Behavioral Outcomes Clinical quality Patient experience Access Efficiency Costs saved 22
23 Tiering Examples Colorado Multi-payer Medical Home Pilot Includes supplemental PMPM payment (range) and P4P bonus. PMPM Considerations: Costs incurred including EMR, care coordinator QI time and participation time Actuarial analysis of reasonable PMPM to recoup costs NCQA Level PMPM Payment CareOregon Tiers on self-defined medical home achievement Balances participation and outcomes Level 1 Level 2 Level 3 $4.00 to $5.50 PMPM $6.00 to $7.00 PMPM $7.25 to $8.50 PMPM Tier Medical Home Engagement and Outcomes 1 Participation in collaborative, workgroups, learning sessions, and reporting data. 2 Hitting targets on key metrics including access to care, HEDIS and full participation in the collaborative. 3 Payment for decreasing ambulatory care-sensitive hospital admissions, emergency department visits, and achieving HEDIS >90 th percentile. Source: Klein S, McCarthy D. CareOregon: Transforming the Role of a Medicaid Health Plan from Payer to Partner. Commonwealth Fund ; Accessed January
24 PMPM Commercial Population Size (# of patients) NCQA Level < 10,000 $4.68 $5.34 $ ,000-20,000 Maryland PCMH Pilot (July 2011) $3.90 $4.45 $5.01 > 20,000 $3.51 $4.01 $4.51 Size (# of patients) PMPM Medicaid Population NCQA Level < 10,000 $5.45 $6.22 $ ,000-20,000 $4.54 $5.19 $5.84 > 20,000 $4.08 $4.67 $5.25 PMPM Medicare Population Year 1: Level 1+ or higher; Year 2: Level 2+ or higher < 10,000 $ ,000-20,000 $9.62 Source: Bailit M. Payment Rate Brief. Patient Centered Primary Care Collaborative. March Accessed June
 Global and bundled payments Accountable Care Organizations Medical home")
25 PPACA: New Opportunities New Funding & New Coverage: Increased FFS for primary care Enhanced preventive care Coverage and service expansion Health center payment protections Payment & Delivery Demonstrations: CMS Innovation Center (Section 3201) Global and bundled payments Accountable Care Organizations Medical home demonstrations 25
26 Section 2703: Medicaid Medical Home State Option Permits Medicaid enrollees with at least two chronic conditions, one condition and risk of developing another, or at least one SPMI to designate a provider as a health home. Went into effect Jan 1, Offers states a 90% FMAP match for two years for home health-related services, including care management, care coordination, and health promotion. State planning grants also available. 26
27 Getting Started: Lessons from the Field Help set the Stage for Success 27
28 Leadership Engagement is Critical The multidisciplinary leadership team Executive Physician Nursing IT Quality Improvement Beware The County Syndrome Understand and work with terminal uniqueness 28
29 Prepare for the Paradigm Shift PCMH is an epic-level of transformation From acute, responsive care to pro-active, planned care From solo provider mindset to team-based care From volume to value From chaos to control 29
30 Staffing Considerations PCMH is a driver for provider recruitment and retention Anticipate HR and union issues The Magic Formula 1 provider: 1.5 MA : 0.5 RN : 3 exam rooms 30
31 Select an Appropriate Assessment Tool Multiple uses: Stimulates team discussion about current operations and sets the expectations for the future state Provides a gap analysis Identifies opportunities for improvement and TA needs Quantifies progress for monitoring purposes Allows a means of comparing sites to each other 31
32 Health Plans Must be in the Game PCP assignment process Rules for appropriate referrals Requirements for specialists communication with PCP Data mining and data sharing Consider piloting payments for innovative visit models Provide support to network providers 32
33 General Operations Safety Net Clinics can become continuity clinics Open Access can be a barrier to care Empanelment requires continuous attention Information Systems can impede transformation PCMH readiness can guide EMR design and implementation PCMH effort can guide space planning efforts for new facilities or renovations 33
34 Large-scale Project Planning Articulate goals Adopt a project framework and assessment tool Define measurement approach early on and stick with it Establish reasonable timelines Establish relationships with community partners Provide different modalities of support Encourage and actively facilitate peer-to-peer learning Address payment and financing 34
35 At the Practice Site Level Get Ready Review your organization s goals Adopt a project framework Develop a multi-disciplinary Project Team Assign a Project Leader Develop a plan for regular communication with staff Define a measurement structure; ensure that IT systems provide the right data Select a PCMH self-assessment tool 35
36 Get Set Conduct a scored self-assessment to establish a baseline Review scoring; understand gaps Develop an Action Plan Use a Tracking Sheet / Monitoring Tool to chart progress over time 36
37 . GO!! Keep the Vision Walk the Talk Stay the Course 37
38 Resources SNMHI website: PCPCC: National Academy for State Health Policy: The Commonwealth Fund: 38
39 Questions Kathryn Phillips, MPH Director, SNMHI Regina Neal, MPH MS Senior Consultant 39
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A)
") SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
SAFETY NET MEDICAL HOME INITIATIVE PATIENT-CENTERED MEDICAL HOME ASSESSMENT (PCMH-A) Organization name Site name Date completed Introduction To The PCMH-A The PCMH-A is intended to help sites understand
Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010
 Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
NCQA s Patient-Centered Medical Home Recognition and Beyond. Tricia Marine Barrett, VP Product Development
 NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
Primary Care Transformation in Academic Medical Centers. Objectives of Session
 Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Where Do We Go From Here? The Value of Sustaining Practice Transformation
 Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the second module of Coach Medical Home a six module curriculum designed for practice facilitators who are coaching primary care practices around patient centered medical home (PCMH) transformation.
This is the second module of Coach Medical Home a six module curriculum designed for practice facilitators who are coaching primary care practices around patient centered medical home (PCMH) transformation.
Health Reform and The Patient-Centered Medical Home
 THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
Deeper Dive on Team Roles: Part I
 Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
Deeper Dive on Team Roles: Part I Moderator: Diane Altman Dautoff, MSW, EdD, Sr. Consultant, Qualis Health Speakers: Ed Wagner, MD, MPH, Director (Emeritus), MacColl Institute for Healthcare Innovation
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
2019 Quality Improvement Program Description Overview
 2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
Community Health Centers: Medical Homes in the Safety Net. Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health
 Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
Community Health Centers: Medical Homes in the Safety Net Jonathan R. Sugarman, MD, MPH President and CEO Qualis Health Fifth National Medicaid Congress Preconference Symposium II: Medicaid and the Medical
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Lessons from the States: Oregon s APM Model
 Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
Lessons from the States: Oregon s APM Model F R I D AY, N O V E M B E R 6, 2 0 1 5 2 : 0 0 P M E T C R A I G H O S T E T L E R, E X E C U T I V E D I R E C T O R, O P C A K E R S T E N B U R N S L A U
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
The New York State Health Center Controlled Network (NYS-HCCN)
") The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
The New York State Health Center Controlled Network (NYS-HCCN) A HRSA-Funded Project of the Community Health Care Association of New York State PCMH 2014 Must Pass Elements Qualis Health November 16, 2015
BCBSRI & Delivery System Transformation. Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016
 BCBSRI & Delivery System Transformation Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016 1 Overview Systems of Care Overview & Highlights Primary Care to Risk Arrangements
BCBSRI & Delivery System Transformation Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016 1 Overview Systems of Care Overview & Highlights Primary Care to Risk Arrangements
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Payment Reform Strategies. Ann Thomas Burnett BlueCross BlueShield of South Carolina
 Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Improving Systems of Care for Children and Youth with Special Health Care Needs
 Improving Systems of Care for Children and Youth with Special Health Care Needs L E A R N I N G C O L L A B O R A T I V E O N I M P R O V I N G Q U A L I T Y A N D A C C E S S T O C A R E I N M A T E R
Improving Systems of Care for Children and Youth with Special Health Care Needs L E A R N I N G C O L L A B O R A T I V E O N I M P R O V I N G Q U A L I T Y A N D A C C E S S T O C A R E I N M A T E R
Transformational Payment Reform: How will FQHC s survive?
 Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Transformational Payment Reform: How will FQHC s survive? Arthur Chen, MD Senior Fellow/Family Practice Asian Health Services Oakland, CA artc@ahschc.org Learning Objectives Familiarity with major Payment
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS. By: Susan Price, Senior Attorney
 December 8, 2011 2011-R-0394 MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS By: Susan Price, Senior Attorney You asked how many state Medicaid programs using a patient-centered medical
December 8, 2011 2011-R-0394 MEDICAID MEDICAL HOMES PAYING ON A PER MEMBER, PER MONTH BASIS By: Susan Price, Senior Attorney You asked how many state Medicaid programs using a patient-centered medical
Why Are We Doing This?
 ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
ALIGNING PAYMENT WITH PATIENT-CENTERED CARE AND VALUE-BASED PAY Craig Hostetler MPCA Annual Conference August 5 th, 2013 Why Are We Doing This? Why Take the Risk? Our stakeholders wanted something better
The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure
 The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure Marci Nielsen, PhD, MPH Executive Director Amy Gibson, MS, RN Chief Operating Officer Patient-Centered
The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure Marci Nielsen, PhD, MPH Executive Director Amy Gibson, MS, RN Chief Operating Officer Patient-Centered
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010
 The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
How to Build a Medical Home
 How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
Patient Centred Medical Home Self-assessment (PCMH-A)
") Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Centred Medical Home Self-assessment (PCMH-A) Practice name: Your name: Date completed: For more information, contact: Colleen Watkins, NQPHN Chronic Care Team m: 0 0 e: info@nqpcmh.com.au w: nqpcmh.com.au
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
College-wide Patient-Centered Medical Home Program Meharry Medical College
 + The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
+ The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
MEDICAL HOMES Arkansas Hospital Association
 MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
MEDICAL HOMES Arkansas Hospital Association Framing our discussion Environmental snapshot of health care Hospitals and the PCMH Arkansas Medical Homes Patients/Consumers 2 1 Health Policy is changing Budget
Transforming Care for Vulnerable Populations:
 Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Draft Covered California Delivery Reform Contract Provisions Comments Welcome and Encouraged
 TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
Comprehensive Primary Care: Our Success Story
 Comprehensive Primary Care: Our Success Story March 2, 2016 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura Health Will McConnell,
Comprehensive Primary Care: Our Success Story March 2, 2016 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura Health Will McConnell,
Putting Patients and Families at the Center of Care: Innovative State Strategies for Medical Homes and Health Homes
 Putting Patients and Families at the Center of Care: Innovative State Strategies for Medical Homes and Health Homes Mary Takach National Academy for State Health Policy National Medical Home Summit March
Putting Patients and Families at the Center of Care: Innovative State Strategies for Medical Homes and Health Homes Mary Takach National Academy for State Health Policy National Medical Home Summit March
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future
 Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
of Program Success and
 PCMH Evaluations: Key Drivers of Program Success and Measurement Development Robert Phillips, MD, MSPH, American Board of Family Medicine Deborah Peikes, PhD, MPA, Mathematica Michael Bailit, MBA, Bailit
PCMH Evaluations: Key Drivers of Program Success and Measurement Development Robert Phillips, MD, MSPH, American Board of Family Medicine Deborah Peikes, PhD, MPA, Mathematica Michael Bailit, MBA, Bailit
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and the Care of Complex High Cost Patients
 PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
PCMH and the Care of Complex High Cost Patients 15 th Annual International Summit on Improving Patient Care in the Office Practice and the Community March 10, 2014 Session A8/B8 Lucy Loomis, MD, MSPH,
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Implementing Patient-Centered Medical Home Pilot Projects:
 Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature
 New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature November 2012 Division of Medical Assistance and Health Services NJ Department of Human Services Introduction In September,
New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature November 2012 Division of Medical Assistance and Health Services NJ Department of Human Services Introduction In September,
September, James Misak, M.D. Linda Stokes, MSPH The MetroHealth System
 Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
EMPANELMENT. Addressing Staff Pushback for Empanelment. Provider / Manager Push Back. Management Opportunity
 Addressing Staff Pushback for Empanelment This sounds like thinly disguised productivity jargon. This is not about productivity demands. It is about understanding providers workload and applying balance
Addressing Staff Pushback for Empanelment This sounds like thinly disguised productivity jargon. This is not about productivity demands. It is about understanding providers workload and applying balance
Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017
 Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura
Leveraging Health IT to Risk Adjust Patients Session ID: QU2; February 19 th, 2017 Tamra Lavengood, RN, BSN, MSN CPC Coordinator and Clinical Performance Coordinator Centura Health Physician Group, Centura
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Primary Care Renewal. Building Successful Practices In The Era Of Accountability Creating Contagious Change
 Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Primary Care Renewal Building Successful Practices In The Era Of Accountability Creating Contagious Change David Labby, MD PhD Director of Clinical Support and Innovation May 27, 2011 CareOregon Our Vision:
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs
 Transformation and Recognition/Certification Programs") Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
Patient-Centered Medical Home (PCMH) Transformation and Recognition/Certification Programs Ruth S. Gubernick, PhDc, MPH, PCMH CCE For the NJAAP s Systems Integration Medical Home Project October 27, 2016
The Patient Centered Medical Home (PCMH): Overview of the Model and Movement Part II. July 2010
: Overview of the Model and Movement Part II. July 2010") The Patient Centered Medical Home (PCMH): Overview of the Model and Movement Part II July 2010 Shari M. Erickson, MPH Senior Associate, Center for Practice Improvement & Innovation American College of
The Patient Centered Medical Home (PCMH): Overview of the Model and Movement Part II July 2010 Shari M. Erickson, MPH Senior Associate, Center for Practice Improvement & Innovation American College of
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
producing an ROI with a PCMH
 REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Opportunities to Promote CV Risk Reduction within the PCMH. Objectives. Disclosure 4/15/2013
 Opportunities to Promote CV Risk Reduction within the PCMH Cardiovascular Health Summit April 12, 2013 Billings, Montana F. Douglas Carr, MD, MMM, FACP Medical Director, Education & System Initiatives
Opportunities to Promote CV Risk Reduction within the PCMH Cardiovascular Health Summit April 12, 2013 Billings, Montana F. Douglas Carr, MD, MMM, FACP Medical Director, Education & System Initiatives
Long term commitment to a new vision. Medical Director February 9, 2011
 ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Identify Best Practices of Behavioral Health Home Organizations to Prevent Admissions and Readmissions
 Orlando, Florida No Disclosures DE2: MaineCare Behavioral Health Homes: An Innovative and Integrated Approach to Care Liz Miller, MPH, Project Manager, Maine Quality Counts Mary Beyer, MS, Quality Improvement
Orlando, Florida No Disclosures DE2: MaineCare Behavioral Health Homes: An Innovative and Integrated Approach to Care Liz Miller, MPH, Project Manager, Maine Quality Counts Mary Beyer, MS, Quality Improvement
A legacy of primary care support underscores Priority Health s leadership in accountable care
 Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
America s Voice for Community Health Care
 America s Voice for Community Health Care The NACHC Mission To promote the provision of high quality, comprehensive and affordable health care that is coordinated, culturally and linguistically competent,
America s Voice for Community Health Care The NACHC Mission To promote the provision of high quality, comprehensive and affordable health care that is coordinated, culturally and linguistically competent,
Our Response to Health Reform: Collaborative Initiatives for Success
 Our Response to Health Reform: Collaborative Initiatives for Success February 11, 2012 Joseph R Swedish, FACHE President and CEO Trinity Health Trinity Health: Unified Enterprise Ministry Serving Ten States
Our Response to Health Reform: Collaborative Initiatives for Success February 11, 2012 Joseph R Swedish, FACHE President and CEO Trinity Health Trinity Health: Unified Enterprise Ministry Serving Ten States
Low-Income Health Program (LIHP) Evaluation Proposal
 Evaluation Proposal") Low-Income Health Program (LIHP) Evaluation Proposal UCLA Center for Health Policy Research & The California Medicaid Research Institute Background In November of 2010, California s Bridge to Reform 1115
Low-Income Health Program (LIHP) Evaluation Proposal UCLA Center for Health Policy Research & The California Medicaid Research Institute Background In November of 2010, California s Bridge to Reform 1115
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance