Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model
|
|
|
- Kevin Ramsey
- 6 years ago
- Views:
Transcription

1 Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model Robert Gabbay MD, PhD Director, Penn State Institute for Diabetes and Obesity Professor of Medicine Penn State College of Medicine
2 Today Development of the PA initiative Key aspects Early outcomes Unique features Questions to ponder 2
3 Origin and Purpose of the Governors Chronic Care Commission Established May 2007 by Executive Order with Commissioners appointed in their individual capacity. Purpose: to design the informational, technological and reimbursement infrastructure needed to implement and support widespread dissemination and implementation of the Chronic Care Model throughout Pennsylvania. 3
4 The Chronic Care Model Most widely accepted evidencebased model for Improving Chronic Care 4
5 The Chronic Care Model Community Health System Resources and Policies Self- Management Support Health Care Organization Delivery System Design Decision Support Clinical Info Systems Informed, Activated Patient Productive Interactions Prepared, Proactive Practice Team Improved Outcomes 5
6 Why Diabetes? 6

7 It s Where the Money is! 7
8 Avoidable Hospitalization Costs for Pennsylvanians with Chronic Disease Cost in $ Billions Heart Disease Lung Disease Diabetes Asthma Chronic Disease 8
9 Why Diabetes? High Morbidity and Mortality High Cost for preventable complications Consensus evidence based goals An epidemic is ahead Diabetes will double in next 20 years
10 The PA Chronic Care Commission Strategic Plan The Commission presented its Strategic Plan to the Governor and the Speaker of the House on February 13, 2008 The Plan provides a business case and framework for implementing the Chronic Care Model across the Commonwealth Implementation is incremental Diabetes (with co-morbidities) and lesser extent asthma primary focus of the initial rollout with spread to other chronic illnesses 10
11 The Intervention 1. Learning collaboratives 2. Practice coaches 3. Registry Reporting 4. Patient Centered Medical Home implementation 5. Reimbursement/infrastructure payments 11
12 Implementation of the Chronic Incremental rollout Care Model in PA Southeastern PA was the first regional rollout May 2008 Rollouts in South Central PA followed by Western, NW and NE PA and throughout the State Rollouts persist for at least three years To date- 780 providers across the state involved with population of 1 million patients 12
13 Partner Organizations Governors Office for Health Care Reform Governor s Chronic Care Commission Payers Independence Blue Cross, Highmark, Capital Blue Cross, Aetna, Keystone Mercy, Health Partners, Geisinger, Cigna, others (17 Total) Professional Organizations/Societies Improving Performance in Practice (IPIP) ABIM ACP PAFP 13
14 One of the Largest Multi- Payer PCMH Initiative in US 14
15 Goals Change processes of care Improve clinical outcomes (diabetes is the target disease but untimely spread to other diseases) Cost containment 15
16 Overall Framework 1. Learning collaboratives 2. Registry reporting 3. Practice coaches 4. Patient Centered Medical Home 5. Reimbursement/incentives changes 16
17 1. The Breakthrough Series Learning Collaborative 2 days each 3 months for One-year then every 6 months for next 2 years Sharing across teams facilitated by conference calls between sessions, listservs, websites for materials 17

18 PDSA Cycle 18
19 2. Registry Reporting Use your own otherwise State provides one free (RMD) Monthly reporting of outcomes along with narrative reports 19
20 3. IPIP Practice Coaches IPIP : Improving Performance in Practice piloted in Colorado and North Carolina RWJ supported Help practices problem solve during PDSA cycles Implement Registry 20
21 4.PPC-PCMH Content and Scoring Standard 1: Access and Communication A. Has written standards for patient access and patient communication** B. Uses data to show it meets its standards for patient access and communication** Standard 2: Patient Tracking and Registry Functions A. Uses data system for basic patient information (mostly non-clinical data) B. Has clinical data system with clinical data in searchable data fields C. Uses the clinical data system D. Uses paper or electronic-based charting tools to organize clinical information** E. Uses data to identify important diagnoses and conditions in practice** F. Generates lists of patients and reminds patients and clinicians of services needed (population management) Standard 3: Care Management A. Adopts and implements evidence-based guidelines for three conditions ** B. Generates reminders about preventive services for clinicians C. Uses non-physician staff to manage patient care D. Conducts care management, including care plans, assessing progress, addressing barriers E. Coordinates care//follow-up for patients who receive care in inpatient and outpatient facilities Standard 4: Patient Self-Management Support A. Assesses language preference and other communication barriers B. Actively supports patient self-management** Pt Pt Pt Pt s s s s Standard 5: Electronic Prescribing A. Uses electronic system to write prescriptions B. Has electronic prescription writer with safety checks C. Has electronic prescription writer with cost checks Standard 6: Test Tracking A. Tracks tests and identifies abnormal results systematically** B. Uses electronic systems to order and retrieve tests and flag duplicate tests Standard 7: Referral Tracking A. Tracks referrals using paper-based or electronic system** Standard 8: Performance Reporting and Improvement A. Measures clinical and/or service performance by physician or across the practice** B. Survey of patients care experience C. Reports performance across the practice or by physician ** D. Sets goals and takes action to improve performance E. Produces reports using standardized measures F. Transmits reports with standardized measures electronically to external entities Standard 9: Advanced Electronic Communications A. Availability of Interactive Website B. Electronic Patient Identification C. Electronic Care Management Support **Must Pass Elements 21 Pts Pts PT 4 4 Pts Pts
22 Focus on Chronic Care Model But reimbursement based on PCMH certification 22
23 5.Reimbursement 17 leading insurers initially involved and expanding GOHCR convener for negotiations Goal is to support implementation of the CCM 23
24 Reimbursement Reimburse for time away from practice at learning collaboratives Benchmark payments based on NCQA PCMH Certification (requires care management) Per FTE prorated by Carrier contribution of Practice s total revenue In NEPA- savings shared with practices Can be ~$30-50 K /FTE/ yr 24
25 Strengths of the PA Approach Government Convener Multi-Payer (17) Teaching practices to change Chronic Care Model Focus Lots of small practices All Practices Reporting Monthly Scope 780 Providers and 1 Million Patients 25
26 26

27 Implementation of the Chronic Care Model in PA 27
28 A Look at the Numbers Region Number of Practices Total Providers FTE'S Total Reported Patients Average FTE's/Practice Average Patients/FT E Year 1 Payments Total Estimated Payments By Insurers SEPA , ,391 $1,965,982 $13,599,231 SCPA , ,081 TBD $4,711,210 SWPA , ,413 TBD $6,219,842 NEPA , ,428 TBD $6,159,615 Total , ,941 $1,965,982 $30,689,898 NWPA , ,026 $192,000 NCPA , $168,000 SEPA , ,434 $276,000 Total , ,364 $636,000 Grand Total ,093, ,694 $2,601,982 $30,689,898
29 Charecteristics of reimbursed practices SEPA SCPA SWPA NEPA Number Participating Practices Number Participating Providers Percent Urban Practices 52% 0% 50% 0% Percent At-risk Populations African American Hispanic Percent of Practice Type FQHC Resident Family Medicine Internal Medicine 12% 37% 32% 16% 28% 24% 2% 2% 0% 0% 80% 20% 13% 1% 9% 0% 86% 5% 3% 3% 0% 7% 86% 7% Percent Practices with Providers 1 to 3 4 to 10 Greater than 10 20% 76% 4% 24% 68% 8% 50% 45% 5% 67% 26% 7% 29

30 Government-Payer-Provider Partnership
31 Outcomes Measures Clinical Patient centered Utilization Costs 31
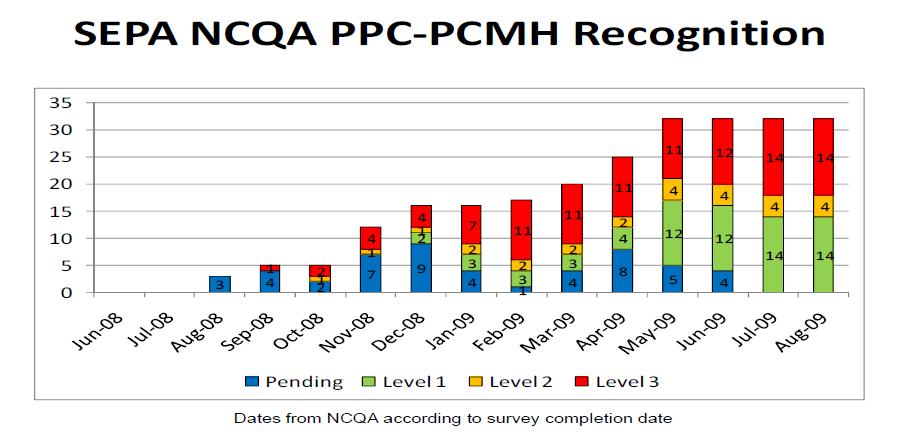
32 Preliminary Results: Southeastern PA 25 practices working on Diabetes 143 providers and 10,000 patients Improvement in complication screening, evidence based medication use, and clinical outcomes NCQA certification 32
33 Evidence Based Treatment Baseline Mean Value at One Year Aspirin Statin* ACE/ARB* SM Goal
34 34
35 Early Cost Data From One Major Insurer in SE First year of SEPA practices saw: 26% decrease in hospital admissions 30% decrease in emergency room visits 16% decrease in overall costs 35
36
37
38
39 Questions How is Success Determined and Who Defines Success? What parts of the intervention are most important Spreading to all Chronic illness Care 39
40 It Takes a Team.. Governor s Office of Health Care Reform Ann Torregrossa, Phil Magistro, Brian Ebersole, Gregory Howe and of course the Governor Ed Wagner, Michael Bailit, Connie Sixta, the brave practices, and many, many more PA Association of Family Practice/Improving Performance in Practice (IPIP)- Pat Bricker
41 Prescription for Pennsylvania Questions?
History of Pennsylvania s Chronic Care Initiative
 History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
Collaboration in Pennsylvania: Rapidly Spreading Improved Chronic Care for Patients to Practices
 Original Research Collaboration in Pennsylvania: Rapidly Spreading Improved Chronic Care for Patients to Practices PATRICIA L. BRICKER, MBA; RICHARD J. BARON, MD, FACP; JORGE J. SCHEIRER, MD; DARREN A.
Original Research Collaboration in Pennsylvania: Rapidly Spreading Improved Chronic Care for Patients to Practices PATRICIA L. BRICKER, MBA; RICHARD J. BARON, MD, FACP; JORGE J. SCHEIRER, MD; DARREN A.
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
The Medical Home Model as a Solution to Diabetes Disparities
 Kenyatta Lee, MD Clinical Director Community Clinics Department University of Florida/Shands Jacksonville The Medical Home Model as a Solution to Diabetes Disparities Objectives: 1Provide an overview the
Kenyatta Lee, MD Clinical Director Community Clinics Department University of Florida/Shands Jacksonville The Medical Home Model as a Solution to Diabetes Disparities Objectives: 1Provide an overview the
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
National Primary Care Extension Program in the United States: A Learning Network
 National Primary Care Extension Program in the United States: A Learning Network International Forum on Quality & Safety in Healthcare 2015, London England 21-24 April 2015 Robert A. Gabbay, MD, PhD, FACP
National Primary Care Extension Program in the United States: A Learning Network International Forum on Quality & Safety in Healthcare 2015, London England 21-24 April 2015 Robert A. Gabbay, MD, PhD, FACP
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F
 Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
NCQA s Patient-Centered Medical Home Recognition and Beyond. Tricia Marine Barrett, VP Product Development
 NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
NCQA s Patient-Centered Medical Home Recognition and Beyond Tricia Marine Barrett, VP Product Development National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Health Reform and The Patient-Centered Medical Home
 THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
THE COMMONWEALTH FUND Health Reform and The Patient-Centered Medical Home Melinda Abrams The Commonwealth Fund November 3, 2011 Grantmakers in Health Fall Forum Primary Care Foundation At Risk: Patient
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Patient-Centered Medical Home Best Practices: Case Study Examples
 Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training. Reviewed: 03/22/18
 Health Care Homes (HCH) HCH Recertification Training. Reviewed: 03/22/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training Reviewed: 03/22/18 1 Learning Objectives 1. Describe the Health Care Homes legislative criteria as required at
Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training Reviewed: 03/22/18 1 Learning Objectives 1. Describe the Health Care Homes legislative criteria as required at
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010
 Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
Patient Centered Medical Home Judith Schaefer, MPH MacColl Institute Missouri Foundation for Health September 27, 2010 What is the Medical Home? History of Medical Home Pediatrics -Started as a movement
Improving Medicaid Chronic Disease Care and Controlling Costs. The Case for Medical Homes and Community Networks
 Improving Medicaid Chronic Disease Care and Controlling Costs The Case for Medical Homes and Community Networks L. Allen Dobson,Jr. MD FAAFP Chair -Board of Directors NC Community Care Networks, Inc HOME
Improving Medicaid Chronic Disease Care and Controlling Costs The Case for Medical Homes and Community Networks L. Allen Dobson,Jr. MD FAAFP Chair -Board of Directors NC Community Care Networks, Inc HOME
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Executive Summary 1. Better Health. Better Care. Lower Cost
 Executive Summary 1 To build a stronger Michigan, we must build a healthier Michigan. My vision is for Michiganders to be healthy, productive individuals, living in communities that support health and
Executive Summary 1 To build a stronger Michigan, we must build a healthier Michigan. My vision is for Michiganders to be healthy, productive individuals, living in communities that support health and
Chronic diseases represent a significant
 Implementing the Chronic Care Model: A Statewide Focus on Improving Diabetes Care for Pennsylvania Linda Siminerio, RN, PhD, CDE, Edward H. Wagner, MD, Robert Gabbay, MD, PhD, and Janice Zgibor, RPh, PhD
Implementing the Chronic Care Model: A Statewide Focus on Improving Diabetes Care for Pennsylvania Linda Siminerio, RN, PhD, CDE, Edward H. Wagner, MD, Robert Gabbay, MD, PhD, and Janice Zgibor, RPh, PhD
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
NCQA s Patient-Centered Medical Home (PCMH) 2011
 2011") NCQA s Patient-Centered Medical Home (PCMH) 2011 Johann Chanin, Director, Product Development Mina Harkins, Assistant Vice President, Recognition Programs All materials 2011, National Committee for Quality
NCQA s Patient-Centered Medical Home (PCMH) 2011 Johann Chanin, Director, Product Development Mina Harkins, Assistant Vice President, Recognition Programs All materials 2011, National Committee for Quality
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Paving the Way for. Health Homes
 Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
Patient Centered Care
 Patient Centered Care and dthe Future of Healthcare e Delivery e PCH Group Patient Centered Health Group A Division of R.S. Williamsand and Associates, Inc. Introduction PCMH Background and the Medical
Patient Centered Care and dthe Future of Healthcare e Delivery e PCH Group Patient Centered Health Group A Division of R.S. Williamsand and Associates, Inc. Introduction PCMH Background and the Medical
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Meaningful Use Final Rule:
 Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Primary Care Transformation in Academic Medical Centers. Objectives of Session
 Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Implementing Patient-Centered Medical Home Pilot Projects:
 Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
Implementing Patient-Centered Medical Home Pilot Projects: Lessons from AF4Q Communities A resource from Aligning Forces for Quality s Ambulatory Quality Network As the patient-centered medical home (PCMH)
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Transforming Care for Vulnerable Populations:
 Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
Transforming Care for Vulnerable Populations: Lessons from the Safety Net Medical Home Initiative Kathryn E. Phillips, MPH July 2015 Safety Net Medical Home Initiative Goals for this Session Describe the
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Practice Facilitators - Catalyst for Medical Home Transformation
 March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
March 27, 2012 Practice Facilitators - Catalyst for Medical Home Transformation Lyndee Knox, PhD, Vanessa Nguyen, MPH, & Diana Traje, MPH Who we are 2 LA Net a Primary Care Practice Based Research & Resource
Patient Centered Medical Home (PCMH)
") Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Care Compact Guide Patient-Centered Specialty Care (PCSC) A Component of Medical Neighborhood Initiatives
 A Component of Medical Neighborhood Initiatives") Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
Compact Guide Patient-Centered Specialty (PCSC) A Component of Medical Neighborhood Initiatives Services provided by Empire HealthChoice HMO, Inc. and/or Empire HealthChoice Assurance, Inc., licensees
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
IHA District Meetings February-March, : Iowa Environmental Assessment in Quality and Patient Safety HEN, QIN, TCPI, SIM
 IHA District Meetings February-March, 2015 2015: Iowa Environmental Assessment in Quality and Patient Safety HEN, QIN, TCPI, SIM Looking Back 10 Years Ago IHA, AHA, CMS, IFMC, State of Iowa, JCAHO, AHRQ
IHA District Meetings February-March, 2015 2015: Iowa Environmental Assessment in Quality and Patient Safety HEN, QIN, TCPI, SIM Looking Back 10 Years Ago IHA, AHA, CMS, IFMC, State of Iowa, JCAHO, AHRQ
What the blue star means for you A guide to the Aexcel specialist performance network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions What the blue star means for you A guide to the Aexcel specialist performance network www.aetna.com 38.02.314.1
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions What the blue star means for you A guide to the Aexcel specialist performance network www.aetna.com 38.02.314.1
Requirements Document for the Blue Quality Physician Program sm Criteria Effective 08/03/2015
 All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
AAFP Talking Points: Patient Centered Medical Home
 November 2007 Patient Centered Medical Home What is a patient centered (or personal) medical home? The patient centered medical home model is based on the premise that the best health care is not episodic
November 2007 Patient Centered Medical Home What is a patient centered (or personal) medical home? The patient centered medical home model is based on the premise that the best health care is not episodic
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Articles of Importance to Read: UnitedHealthcare Goes Live With 13th Edition of Milliman Care Guidelines. Summer 2009
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Chronic Disease Management: Breakthrough Opportunities for Improving the Health And Productivity of Iowans
 Chronic Disease Management: Breakthrough Opportunities for Improving the Health And Productivity of Iowans A Report of the Iowa Chronic Care Consortium February 2003 Background The Iowa Chronic Care Consortium
Chronic Disease Management: Breakthrough Opportunities for Improving the Health And Productivity of Iowans A Report of the Iowa Chronic Care Consortium February 2003 Background The Iowa Chronic Care Consortium
WHITE PAPER. NCQA Accreditation of Accountable Care Organizations
 WHITE PAPER NCQA Accreditation of Accountable Care Organizations CONTENTS Introduction 3 What are ACOs, and what do we want them to achieve? 3 Building from patient-centered medical homes 4 Program elements
WHITE PAPER NCQA Accreditation of Accountable Care Organizations CONTENTS Introduction 3 What are ACOs, and what do we want them to achieve? 3 Building from patient-centered medical homes 4 Program elements
Care Coordination Overview. Janet Tennison, PhD UPV Standards October 8, 2013
 Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
Care Coordination Overview Janet Tennison, PhD UPV Standards October 8, 2013 What IS Care Coordination? The deliberate, proactive organization of patient care activities between two or more participants
University of Cincinnati Patient Centered Medical Home Leadership Decisions
 University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013
 NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
NCL MEDICATION ADHERENCE CAMPAIGN FREQUENTLY ASKED QUESTIONS 2013 1. WHAT EXACTLY IS MEDICATION ADHERENCE? Adhering to medication means taking the medication as directed by a health care professional-
Patient Centered Medical Home Foundation for Accountable Care
 Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Community Mental Health and Care integration. Zandrea Ware and Ricardo Fraga
 Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards
 and the NCQA PCMH 2011 Standards") Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
Moving Toward Recognition: Understanding Patient-Centered Medical Home (PCMH) and the NCQA PCMH 2011 Standards Presented by Lori-Anne Russo, Director of Clinical Programs to the PCMH Learning Collaborative
MD, MBA, FACHE, FAAPL
 Washington Association of Medical Staff Services Vancouver, Washington Ambulatory Credentialing and Privileging Jon Burroughs, MD, MBA, FACHE, FAAPL April 20, 2018 The Healthcare Transformation Journey:
Washington Association of Medical Staff Services Vancouver, Washington Ambulatory Credentialing and Privileging Jon Burroughs, MD, MBA, FACHE, FAAPL April 20, 2018 The Healthcare Transformation Journey:
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
National Survey of Physician Organizations and the Management of Chronic Illness II (Independent Practice Associations)
") If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
Does The Chronic Care Model Work?
 Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
Does The Chronic Care Model Work? A Chartbook created by the staff of: Improving Chronic Illness Care, At Group Health s s MacColl Institute Supported by The Robert Wood Johnson Foundation Grant # 48769
NCQA Criteria for Accountable Care Organizations. Margaret E. O Kane, President March 24, 2011
 NCQA Criteria for Accountable Care Organizations Margaret E. O Kane, President What Are ACOs? Provider-based organizations that are accountable for both quality and costs of care for a defined population
NCQA Criteria for Accountable Care Organizations Margaret E. O Kane, President What Are ACOs? Provider-based organizations that are accountable for both quality and costs of care for a defined population
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases?
 Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Multi-Payer Investments in Primary Care: Policy and Measurement Strategies
 Multi-Payer Investments in Primary Care: Policy and Measurement Strategies Prepared by: Center for Health Care Strategies & State Health Access Data Assistance Center July 2014 Table of Contents Introduction...
Multi-Payer Investments in Primary Care: Policy and Measurement Strategies Prepared by: Center for Health Care Strategies & State Health Access Data Assistance Center July 2014 Table of Contents Introduction...
Thursday, June 2, 2011, 2-3:30 PM ET
 CHCS Webinar: ROI Forecasting Calculator for Health Homes and Medical Homes Thursday, June 2, 2011, 2-3:30 PM ET For audio, dial: (866) 699-3239; Meeting/Event Number: 710 497 839. You may also listen
CHCS Webinar: ROI Forecasting Calculator for Health Homes and Medical Homes Thursday, June 2, 2011, 2-3:30 PM ET For audio, dial: (866) 699-3239; Meeting/Event Number: 710 497 839. You may also listen
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
2014 Patient Centered Medical Home (PCMH) Recognition
 Recognition") Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Collaboration Catalyst Community 2014 Patient Centered Medical Home (PCMH) Recognition PRESENTED BY: Oct. 2015 RuthAnn Craven, MS Transformation Coach AHI is an independent, nonprofit organization that
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Welcome to. Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes
 Welcome to ASTHO s Delivery and Payment Reform Technical Assistance Call Series Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes Presented by ASTHO and
Welcome to ASTHO s Delivery and Payment Reform Technical Assistance Call Series Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes Presented by ASTHO and
Laying the Foundation for Successful Clinical Integration
 The Governance Institute Laying the Foundation for Successful Clinical Integration Webinar November 29, 2011, 2:00pm ET/11:00am PT Daniel M. Grauman President & CEO DGA Partners, Bala Cynwyd, PA dgrauman@dgapartners.com
The Governance Institute Laying the Foundation for Successful Clinical Integration Webinar November 29, 2011, 2:00pm ET/11:00am PT Daniel M. Grauman President & CEO DGA Partners, Bala Cynwyd, PA dgrauman@dgapartners.com
Value-Based Care Emergent Care Services. Presented by Cliff Frank Partnera Partners LLC
 Value-Based Care Emergent Care Services Presented by Cliff Frank Partnera Partners LLC Problem Un-doctored consumers are driving $575 billion inappropriate emergent care Fee-for-service ER visits add another
Value-Based Care Emergent Care Services Presented by Cliff Frank Partnera Partners LLC Problem Un-doctored consumers are driving $575 billion inappropriate emergent care Fee-for-service ER visits add another
Emerging Opportunities: Pharmacy Care. NACDS Total Store Expo August 20, 2017
 Emerging Opportunities: Pharmacy Care NACDS Total Store Expo August 20, 2017 Presentation Objectives Current value based healthcare landscape Medication management as a critical component to achieve value
Emerging Opportunities: Pharmacy Care NACDS Total Store Expo August 20, 2017 Presentation Objectives Current value based healthcare landscape Medication management as a critical component to achieve value
Paying for Primary Care: Is There A Better Way?
 Paying for Primary Care: Is There A Better Way? Robert A. Berenson, M.D. Senior Fellow, The Urban Institute CHCS Regional Quality Improvement Initiative, Providence, R.I., July 25, 2007 1 Medicare Challenges
Paying for Primary Care: Is There A Better Way? Robert A. Berenson, M.D. Senior Fellow, The Urban Institute CHCS Regional Quality Improvement Initiative, Providence, R.I., July 25, 2007 1 Medicare Challenges
Alternative Payment Models- Recipes For Success
 Alternative Payment Models- Recipes For Success Elizabeth Lange, MD, PCMH-Kids Michael Magill, MD, Department of Family and Preventative Medicine-University of Utah Kevin Schendel, MD Timothy Willox, MD,
Alternative Payment Models- Recipes For Success Elizabeth Lange, MD, PCMH-Kids Michael Magill, MD, Department of Family and Preventative Medicine-University of Utah Kevin Schendel, MD Timothy Willox, MD,
MEDICAL HOME Implementation for Primary Care. Disclosure. Medical Home Building and Implementation for Primary Care: No Child Left Behind
 Medical Home Building and Implementation for Primary Care: No Child Left Behind A. Chris Olson, MD, MHPA Clinical Professor, University of Washington Medical Director, Sacred Heart Children s Hosp. Providence
Medical Home Building and Implementation for Primary Care: No Child Left Behind A. Chris Olson, MD, MHPA Clinical Professor, University of Washington Medical Director, Sacred Heart Children s Hosp. Providence
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill: