Medical Home Summit September 20, 2011
|
|
|
- Stewart Higgins
- 5 years ago
- Views:
Transcription


1 Medical Home Summit September 20,
2 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost


















3

4 Care Management : The unintended consequences of good intentions
5 Patient-Centered Medical Home 2009 Overview of Pilot Activity and Planning Discussions RI Multi-Payer pilot discussions/activity Identified pilot activity No identified pilot activity 6 States
6 A nonprofit collaborative working to redesign healthcare and promote integrated communities of care, using evidence based medicine and innovative systems to optimize health, improve quality and safety, reduce costs, and improve the care experience for patients and their healthcare teams. 6
7 The Colorado Multi-Payer PCMH Pilot
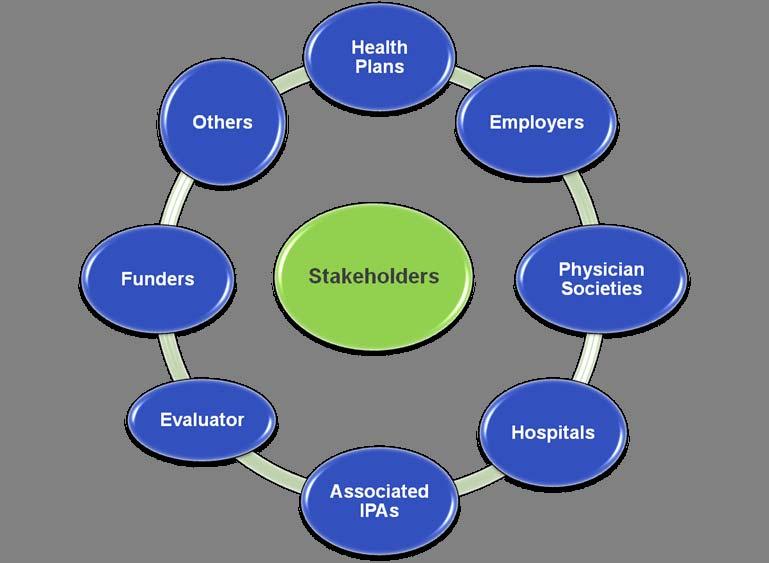
8 Multi-Payer Pilot Stakeholders 8

9 The Front Line Innovators! Belmar Family Medicine Broomfield Family Practice Clinix Health Services of CO Family Care Southwest Family Practice Associates Ideal Family Healthcare Internal Med Clinic of Ft. Collins Lakewood Family Medicine Lone Tree Family Practice Michael Mignoli MD Miramont Family Medicine Mountaintop Family Health Provident Adult & Senior Medicine Southpark Internal Medicine Westminster Medical Clinic 9
10 Pilot Parameters Three-year pilot Convened January 2008; TA December 2008 May 2009 April 2012 PCMH Joint Principles NCQA PCMH Recognition 14 at Level III; 2 at Level II 16 Family & Internal Medicine Practice sites 83 providers; 258 staff - various sizes 20,000 patients covered (100,000 affected) Three-tiered payment structure Fee for service (FFS); Care management fee (PMPM); P4P
11 New Payment Methods Allow a New Way of Thinking! Transition from FFS treadmill medicine to coordinated, planned management of entire panel, with extra care for those who need it Redefine VISITS Add Care Management/ Care Coordination BUT can do in the meantime in FFS model 2:1 ratio for MA/Nurse to Provider 11
12 Goals/Measures Improve quality Diabetes Cardiovascular disease Tobacco Depression Prevention Reduce cost trends Emergency room (ER) visits Hospital admissions Generic pharmacy Improve satisfaction Internal External Matched comparison design Meredith Rosenthal Harvard Patients/families Health care team 12
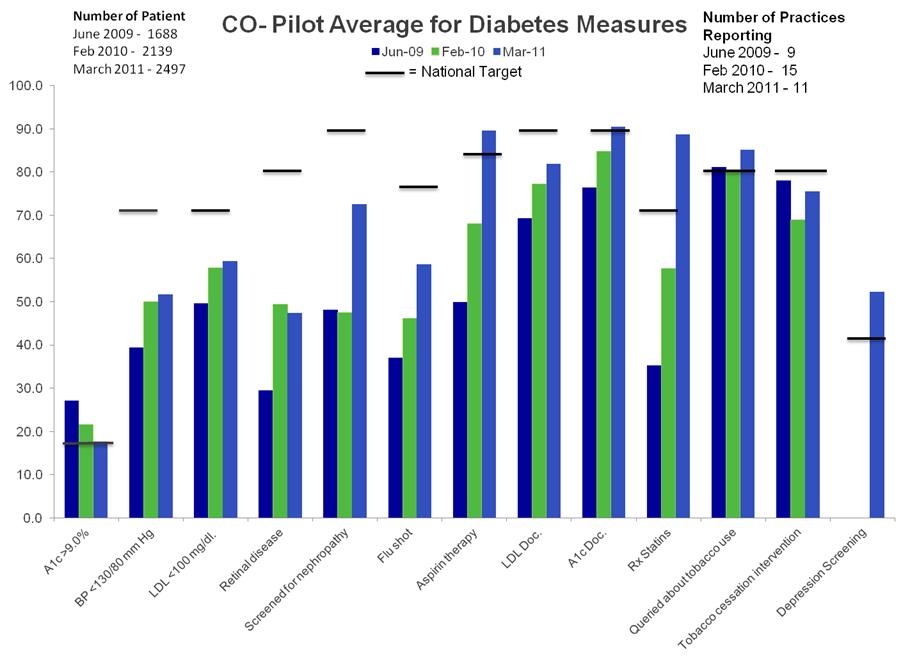
13 Diabetes


14 Putting It All Together Patient Centered Planned Care

15 Prioritizing Care Management & Care Coordination Multiple Chronic Conditions & Complex Patients 15
16
17 Key Elements Tactical Cultural/Behavioral Lab and Referral Tracking Registry/EMR Practice Point Person and Patient Navigator Leadership Team Based Care Communication Patient Activation Continuous Quality Improvement 17

18 Culture eats strategy for lunch over and over again. Anonymous 18
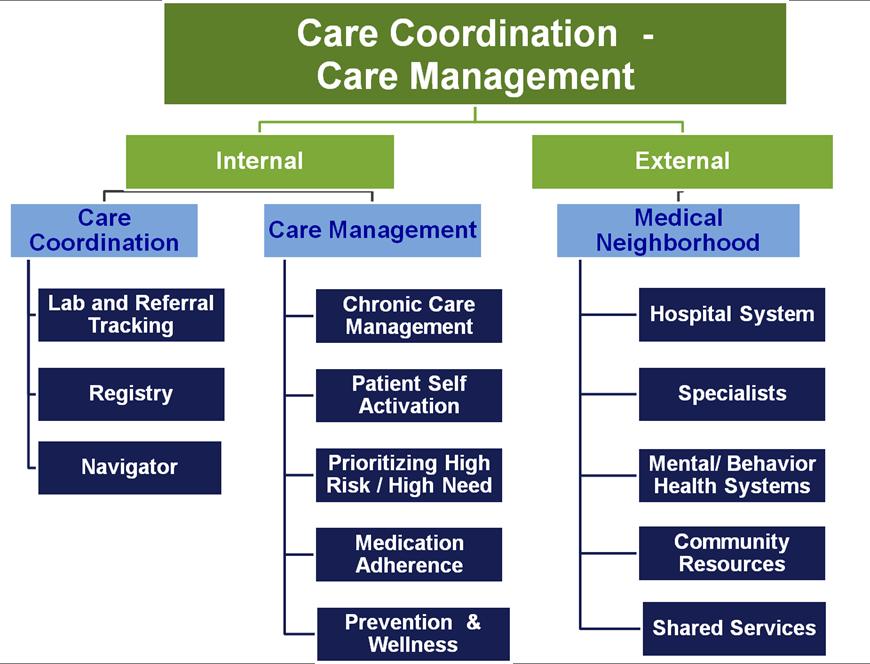
19 Internal Coordination and Management Care Coordination Lab And Referral Tracking Registry/EMR Navigator Care Management Chronic Care Management Patient Self Activation High Risk / High Need Medication Adherence Prevention & Wellness
20 Care Coordination Roles A. Help Patient Implement Individual Care Plan Track tests and referrals ordered Implement reliable process to get reports into medical record Filter information and reports coming into practice B. Registry Set-Up & Maintenance Ensure registry functionality and process to maintain it Manage and present reports on individual patients and overall practice population for team discussion Use outreach reports to identify patients overdue for services Use Health Plan and Hospital reports to prioritize those patients needing more intensive case management/care coordination C. Coordination of Care (Medical Neighborhood) Point person for outside entities to facilitate bi-directional communication and follow-up Navigator for patients for services outside clinic, including community resources. Skill Sets LPN, MA Data Person, Front Desk, MA, Practice Manager LPN, MA, Health Educator
21 Care Management Roles Skill Sets A. Help Patient Implement Individual Care Plan Assess barriers for patients struggling with care plan Self management support, motivational interviewing to assess patient s self-efficacy in reaching their goals. Use education materials, tools, counseling, group visits, etc. Discuss medication adherence, reconciliation and management using protocols developed by physicians RN, PA, MD, Social Worker, Health Educator (limited) (Requires higher skills, training/licensure/certification than Care Coordinator Role) B. Increase Patient Access Phone Calls, s, Extended Hours - 24/7 coverage MA, RN, PA, MD, Scheduler
22 Lessons Learned Guidance needed for new roles/responsibilities Clear job descriptions, particularly for turnover Clarify roles with providers, staff, neighbors, patients Hiring right; Initial and ongoing training Team-Based Approach Every staff member is part of care team Develop work flows and strategies for communication Follow-up calls make huge difference to patients Warm hand off by team works better for referrals Strategies for patient engagement/experience Do patients know what a PCMH is or philosophy of patient centered care? What is patients experience of their care?
23 Role of Physicians Customized Care Plan Shared Decision Making Prevention, Chronic Care, Acute Care issues Identify patients needing care coordination and more complex care management Hand off to care coordinators/managers Define roles of care team for patient Follow-up as necessary


24 Integrated Community of Care (Accountable A Medical Home Care Organizations) Without An Integrated Medical Neighborhood Is Just An Island 24
25 External Coordination Medical Neighborhood Specialists Hospital Systems Mental/ Behavioral Health Systems Community Resources
26 Building Your Medical Neighborhood Specialists including Behavioral Health Integration, co-location, referral Build relationships; clarify roles (Compacts) Monitor progress with regular communication/feedback Hospitals Identify Primary Care Provider (PCMH) - Wallet Cards Notify PCMH about patient in ER or Hospital Templates for content (fax, text, HIE) Care Coordinators login to Hospital EHR daily for list of patients and details of visit Challenge if no admitting privileges 26
27 Patient Wallet Card 27

28 Fax Referral Form 28
29 Challenges/Lessons Learned Specialists Fragmented system with misaligned incentives Varied awareness and reception to PCMH/Medical Neighborhood concept Mental/Behavioral health - HIPAA issues; payment/carve outs; culture/language barriers; timeliness Hospitals Varied responses from hospitals ( one off ) Login difficult without privileges PA/NP often aren t identified in system Re-evaluate need for patients to have a designated PCP?
30 Shared Services Model Complex Case Manager (i.e., RN) Clinical Pharmacist Social Worker Mental Health consultants Others
31 Making Sense of Various Care Coordination/Care Management Roles - Possible Scenario Care Coordination/Care Management (PCMH) Complex Case Management and other shared services (IPA, ACO, Community) Transitions/Health Coach (Hospital, ACO, community with bridge to PCMH) Lay and Professionals 31
32 In Summary 32

33 MacColl Institute at Group Health 33
34 Investment Required to Reduce CHAOS and Build Solid Infrastructure 34
35 35
36 IT S S ALL ABOUT RELATIONSHIPS!!



37 With Your PATIENTS! With Your TEAM With Your NEIGHBORS Building Accountability to Each Other and Our Communities 37

38 Start Small Start Somewhere!

39 Success is a journey, not a destination - Arthur Robert Ashe, Jr.
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
BCBSRI & Delivery System Transformation. Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016
 BCBSRI & Delivery System Transformation Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016 1 Overview Systems of Care Overview & Highlights Primary Care to Risk Arrangements
BCBSRI & Delivery System Transformation Gus Manocchia, MD Senior Vice President & Chief Medical Officer March 11, 2016 1 Overview Systems of Care Overview & Highlights Primary Care to Risk Arrangements
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions
 Project Frequently Asked Questions") Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
CareConcepts Integrating Payor Sponsored Disease Management into Primary Care Practice
 Integrating Payor Sponsored Disease Management into Primary Care Practice Physicians Foundation for Health Systems Excellence Grant # 9600013 (2005 PFHSE Grantees) January 2006 June 2009 PO Box 762, Farmington,
Integrating Payor Sponsored Disease Management into Primary Care Practice Physicians Foundation for Health Systems Excellence Grant # 9600013 (2005 PFHSE Grantees) January 2006 June 2009 PO Box 762, Farmington,
Overview. Patient Centered Medical Home. Demonstrations and Pilots: Judith Steinberg, MD, MPH March 6, 2009
 Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Patient Centered Medical Home Judith Steinberg, MD, MPH March 6, 2009 Patient Centered Medical Home Payment Reform & Incentive Alignment Transparency and Measurement Quality Improvement Practice Transformation
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home
 Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
Population Health for Rural Hospitals: 3. Patient Care Coordination and the Intensive Medical Home National Rural Health Resource Center Webinar Series: Population Health for Rural Hospitals For February
How to Build a Medical Home
 How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
How to Build a Medical Home NOTE: Make sure your computer speakers are turned ON. Audio will be streaming through your speakers. If you do not have computer speakers, call the ACCMA at 510-654-5383 for
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Deeper Dive on Team Roles: Part 2
 Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Reducing Care Fragmentation Executive Summary
 Reducing Care Fragmentation Executive Summary A TOOLKIT FOR COORDINATING CARE Reducing Care Fragmentation 49 Executive Summary Reducing Care Fragmentation: A Toolkit for Coordinating Care is for clinics,
Reducing Care Fragmentation Executive Summary A TOOLKIT FOR COORDINATING CARE Reducing Care Fragmentation 49 Executive Summary Reducing Care Fragmentation: A Toolkit for Coordinating Care is for clinics,
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Continuity of Care Implementing Compacts: A small practice journey
 Continuity of Care Implementing Compacts: A small practice journey R. Scott Hammond, MD Chair, CAFP PCMH Task Force Medical Director, SOC-PCMH Grant, Colorado Associate Clinical Professor, Dept. of Family
Continuity of Care Implementing Compacts: A small practice journey R. Scott Hammond, MD Chair, CAFP PCMH Task Force Medical Director, SOC-PCMH Grant, Colorado Associate Clinical Professor, Dept. of Family
Patient-Centered Medical Home Best Practices: Case Study Examples
 Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient-Centered Medical Home Best Practices: Case Study Examples Mona Chitre, PharmD, CGP Director of Clinical Services, Strategy, and Policy FLRx Pharmacy Management Excellus Health Plans Disclosures
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Leveraging HIE to Bolster Accountable Care Organizations. Healthcare Unbound / July 12, 2013
 Leveraging HIE to Bolster Accountable Care Organizations Healthcare Unbound / July 12, 2013 Types of Health Info. Exchange Direct (Point-to-Point) Query-Based 2013 Colorado Regional Health Information
Leveraging HIE to Bolster Accountable Care Organizations Healthcare Unbound / July 12, 2013 Types of Health Info. Exchange Direct (Point-to-Point) Query-Based 2013 Colorado Regional Health Information
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Patient Centered Medical Home Foundation for Accountable Care
 Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
Health Coaching in Team-Based Care. Recipes for Success
 Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
Health Coaching in Team-Based Care Recipes for Success Today s Presenters Iowa Chronic Care Consortium/Clinical Health Coach William Appelgate, PhD, CPC Executive Director ICCC, Founder and President,
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Journey PCMH & Practice Transformation PCMH 101. Kentucky Primary Care Association Lexington Kentucky June 11, 2014
 A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
A Journey PCMH & Practice Transformation PCMH 101 Kentucky Primary Care Association Lexington Kentucky June 11, 2014 Overview of Journey Today What an overview of PCMH Why PCMH & practice transformation
Building a Better Home: Transformation to a Patient Centered Health Home. Anna M. Gard, FNP-BC Association of Clinicians for the Underserved
 Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
Building a Better Home: Transformation to a Patient Centered Health Home Anna M. Gard, FNP-BC Association of Clinicians for the Underserved A Patient Centered Health Home is not a place but an approach
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017
 Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
A Pharmacist Network for Integrated Medication Management in the Medical Home
 A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Lessons Learned in Care Management. Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference
 Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing
Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Patient Centered Medical Home
 Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Patient Centered Medical Home A model of care where each patient has an ongoing relationship with a personal physician who leads a team that takes collective responsibility for patient care. The physician-led
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health
 PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
PCMH: Next Steps for UMass Dept. of Family Medicine and Community Health Spring Retreat March 19, 2010 Ashland, MA A PCMH provides Easy access to a PCP Who is working with a high-functioning team And a
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Primary Care Transformation in Academic Medical Centers. Objectives of Session
 Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Session A1 These presenters have nothing to disclose. Primary Care Transformation in Academic Medical Centers IHI Improving Patient Care in the Office Practice and Community March 10, 2014 Asaf Bitton,
Patient Centered Medical Home (PCMH)
") Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Patient Centered Medical Home (PCMH) The PCMH is a model of practice in which a Team of health professionals, guided by a personal physician, provides continuous, comprehensive, and coordinated care in
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases?
 Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression?
Impact of Patient Navigation in an Integrated Care Delivery System
 Impact of Patient Navigation in an Integrated Care Delivery System Chrissy Valania, MSW, LCSW Social Worker/Patient Navigator Geisinger Cancer Institute 1 Geisinger at a Glance 9 Hospitals in Pennsylvania
Impact of Patient Navigation in an Integrated Care Delivery System Chrissy Valania, MSW, LCSW Social Worker/Patient Navigator Geisinger Cancer Institute 1 Geisinger at a Glance 9 Hospitals in Pennsylvania
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Where Do We Go From Here? The Value of Sustaining Practice Transformation
 Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
Team Based Care Assessment & Action Plan
 Team Based Care Assessment & Action Plan In the tables below, consider how fully each item has been implemented or functions in your practice. Circle the number that best reflects the completeness of implementation
Team Based Care Assessment & Action Plan In the tables below, consider how fully each item has been implemented or functions in your practice. Circle the number that best reflects the completeness of implementation
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Patient Centered Medical Home Lessons Learned in North Carolina. Debra Thompson, DNP, FNP BC, PCMH CCE Wilson Gabbard, MBA
 Patient Centered Medical Home Lessons Learned in North Carolina Debra Thompson, DNP, FNP BC, PCMH CCE Wilson Gabbard, MBA Background Debra Thompson DNP, FNP BC, PCMH CCE Vidant Health Wilson Gabbard, MBA
Patient Centered Medical Home Lessons Learned in North Carolina Debra Thompson, DNP, FNP BC, PCMH CCE Wilson Gabbard, MBA Background Debra Thompson DNP, FNP BC, PCMH CCE Vidant Health Wilson Gabbard, MBA
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Patient Centered Specialty Practice: Are We Ready for. Course Schedule
 Patient Centered Specialty Practice: Are We Ready for MACRA? Xiaoyan Huang, MD, MHCM, FACC Providence Heart Clinic December 5 th, 2016 28 th IHI National Forum Course Schedule Morning: Introduction Xiaoyan
Patient Centered Specialty Practice: Are We Ready for MACRA? Xiaoyan Huang, MD, MHCM, FACC Providence Heart Clinic December 5 th, 2016 28 th IHI National Forum Course Schedule Morning: Introduction Xiaoyan
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
SAFETY NET MEDICAL HOME INITIATIVE
 SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
SAFETY NET MEDICAL HOME INITIATIVE Key Activities List Background and Description The Safety Net Medical Home Initiative (SNMHI) developed a framework The Change Concepts for Practice Transformation to
Recognition, Publications, & Activities
 Recognition, Publications, & Activities Research Publications Hammond, Barba. A Toolkit for Primary Care Specialty Care Integration. Medical Home News v3 no.2. Feb 2011. McDoniel, Hammond, A Comprehensive
Recognition, Publications, & Activities Research Publications Hammond, Barba. A Toolkit for Primary Care Specialty Care Integration. Medical Home News v3 no.2. Feb 2011. McDoniel, Hammond, A Comprehensive
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Building a Multi-System Clinically Integrated Network
 Building a Multi-System Clinically Integrated Network 22 nd Annual AHA Leadership Summit July 2014 Valence Health Has Been Helping Provider Organizations Progress Toward Value-Based Care Since 1996 Technology-enabled
Building a Multi-System Clinically Integrated Network 22 nd Annual AHA Leadership Summit July 2014 Valence Health Has Been Helping Provider Organizations Progress Toward Value-Based Care Since 1996 Technology-enabled
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
MGH is an integrated service organization in central Maine serving approx. 190,000 individuals KRHA (PHO) 28 PC sites serve 115,000
 28 PC sites serve 115,000") 1 MGH is an integrated service organization in central Maine serving approx. 190,000 individuals KRHA (PHO) 28 PC sites serve 115,000 KENNEBEC VALLEY COMMUNITY CARE TEAM JOAN ORR MCHES, MBA DIRECTOR ACCOUNTABLE
1 MGH is an integrated service organization in central Maine serving approx. 190,000 individuals KRHA (PHO) 28 PC sites serve 115,000 KENNEBEC VALLEY COMMUNITY CARE TEAM JOAN ORR MCHES, MBA DIRECTOR ACCOUNTABLE
Healthcare Clinic at Walgreens Access to Care Innovations Panel March 5, 2014
 Healthcare Clinic at Walgreens Access to Care Innovations Panel March 5, 2014 Dr. Alan London Vice President, Strategic Clinical Partnerships 2014 Walgreen Co. All rights reserved. Walgreens is Well-Positioned
Healthcare Clinic at Walgreens Access to Care Innovations Panel March 5, 2014 Dr. Alan London Vice President, Strategic Clinical Partnerships 2014 Walgreen Co. All rights reserved. Walgreens is Well-Positioned
New York University Prevention Research Center
 New York University Prevention Research Center May 9, 2013 New York City, New York Sergio Matos Executive Director Community Health Worker Network of NYC President Health Innovation Associates Leading
New York University Prevention Research Center May 9, 2013 New York City, New York Sergio Matos Executive Director Community Health Worker Network of NYC President Health Innovation Associates Leading
TO BE RESCINDED Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration
 The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011
 Accountable Care: Health System View CHC Best Practices Forum Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011 Who we are Southeastern New Jersey s largest health system
Accountable Care: Health System View CHC Best Practices Forum Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011 Who we are Southeastern New Jersey s largest health system
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Working at Top of License How do you reallocate work among a team? January 28, 2015
 Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance