Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training. Reviewed: 03/22/18
|
|
|
- Ashlie Avis Morton
- 5 years ago
- Views:
Transcription
 HCH Recertification Training Reviewed: 03/22/18")
1 Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training Reviewed: 03/22/18 1
2 Learning Objectives 1. Describe the Health Care Homes legislative criteria as required at recertification. 2. Review the progression of recertification as it addresses improvement to population health. 3. Describe the requirements for statewide quality improvement reporting and measurement for certified HCH clinics. 2



3 Health Reform in Minnesota Minnesota s 2008 health reform law seeks to fulfill the promise of the Institute for Healthcare Improvement s Triple Aim Improve the health of the population Improve the patient/consumer experience Improve the affordability of health care Institute of Medicine s Triple Aim 3
4 Minnesota Health Reform The health reform law resulted in the following MDH initiatives Health Care Homes (HCH) All Payer Claims Database (MN APCD) Statewide Health Improvement Partnership (SHIP) Statewide Quality Reporting and Measurement System (SQRMS) 4
5 The HCH Program The HCH Program is one of the centerpieces of Minnesota's health reform initiative. Through redesign of care delivery and meaningful engagement of patients, HCH Clinics are transforming care and lives - for millions of Minnesotans. The name "Health Care Homes" acknowledges a shift from a purely medical model of health care to a model which links primary care with wellness, prevention, self-management and community services. 5
6 Goals of the HCH Program Continue to build strong primary care foundation ensuring all Minnesotans have the opportunity to receive team-based, coordinated, patientcentered care. Increase care coordination and collaboration between primary care and community resources to facilitate the broader goals of improving population health and health equity. Improve the quality, experience, and value of care. 6

7 HCH Certification Updates Certified HCH Clinics Applicants are from all over the state. Variety of practice types such as solo, rural, urban, independent, community, FQHC and large organizations. All types of primary care providers are certified: family medicine, pediatrics, internal medicine, OB/GYN and geriatrics. 7

8 The Patient- and Family-Centered Health Care Home 8
9 Recertification Questions: Clinician and/or clinic changes As HCH model is implemented in new clinic sites (referred to as spread ) the new clinicians are certified. Find the Add Clinic Guide on the MDH HCH website. When a previously certified clinician leaves a clinic and goes to work at a non-certified clinic, the new clinic and clinician/s apply for their certification. The previous clinic employer identifies an end date for that clinician in the HCH online portal. Find the Amend Clinicians Guide on the MDH HCH website. 9
10 Recertification Timeline page2 Goal: Maintain relationship, provide ongoing technical assistance and facilitate forward movement of implementation of standards. Initial Certification Recertification: 3 years from initial certification date (HCH portal will generate a 180 and 90 day notice) Subsequent years: Repeat process of every 3 year recertification The Organization submits letter of intent, application/s, and assessment containing the odd numbered standards 1-9 only. The MDH Nurse Planner will then schedule a Health Care Home site visit evaluating the implementation of the odd numbered standards, 1-9 only. The Organization submits letter of intent, application/s, and assessment containing all standards. The MDH Nurse Planner schedules a team meeting to review all standards in the following manner; Changes with any odd numbered standards 1 9 Review of the even numbered standards Review of standard 11 Review any variances The Organization submits letter of intent, application/s, and assessment containing all standards. The MDH Nurse Planner schedules a team meeting to review all standards. Review any changes in standards Review any variances Analyze benchmarks *MDH Nurse Planner will contact the certified Health Care Home organization and offer optional check-ins during the 3-year certification cycle. 10
11 Progression Over Time HCH clinics are recertified every three years in a Team Meeting format. Recertification ensures the progression in the HCH model implementation over time. Clinics have the option of scheduling a technical assistance/coaching check-in visit or phone call with their designated nurse planner. The certifying HCH clinic/s meets all requirements or applies for a variance. A variance may be granted for good cause or when failure to grant a variance would result in hardship. 11
12 Recertification Requirements Continue to meet all initial certification requirements (.0040 Subparts 1,3,5,7,9). Submit documentation by exception. Updates to specific subparts are required: 1A; 5A; 8; 9A; 9D; 10A; 11 Address any recommendations and/or variances, if applicable. 12

13 MDH HCH website Portal link 13

14 Log-in to the MDH HCH Portal 14
15 Recertification Steps for the Applicant Guides & Tools Step 1: Complete LOI Step 2: Verify Clinic/s Step 3: Update Assessments (Odd number) Step 4: Update Assessments (Even number) Step 5: Team Visit Step 6: MDH Notification Optional Step: Variance and Appeals 15
16 Guides & Tools Preparation and guidance 16
17 Step 1: Letter of Intent I. Applicant Intent II. Applicant Demographic Information Organization/clinic name, address, applicant clinician(s) information III. HCH Information Yes/ No questions regarding health care home policies and procedures IV. Additional Information V. Contact Information 17
18 Step 2: Verify Clinic Update Application for each Clinic/Clinicians. I. Applicant Demographic Info Organization/ clinic name, address, applicant clinician(s) information II. Additional Clinician Info Providers and services available to clinic, hours working on HCH III. Clinic s Patient Profile Age, race, gender, payer mix, language, patient characteristics IV. Representations and Signature of Authorized Person 18
19 Steps 3 & Steps 4 Recertification Assessments Recertification Assessment Tool Online submission of individual subparts 19
20 Recertification Assessment Tool Documentation and Data Sources At initial certification the clinic meets the ODD numbered subparts (1,3,5,7,9). There are ten documents to submit. Progression is ensured through the addition of the EVEN numbered subparts (2,4,6,8,10). Documentation examples include: written policies, protocols and procedures workflows guidelines forms, flow sheets EMR and registry screen shots patient education materials, prepared resources, pamphlets meeting minutes with dates and member roles de-identified patient medical records PDSA cycles 20
21 Submission of individual Subparts The hyperlinks to Rule Intent and Rule Language correlate with the Certification Assessment Tool. The clinic may note see attachment if all the information is summarized in the document. The clinic s brief narrative describes the work for the subparts where a document is not attached. Statements should be concise and succinct, initial certification provides baseline information. 21
22 Step 3: Update Assessments Complete Odd Numbered Standards. The recertification self-assessment is used to determine if the applicant meets the documentation requirements for HCH recertification and is ready for a team visit. Applicants submit their HCH Assessment online at least three weeks prior to their recertification team visit. Site evaluators will review the clinics submitted assessment prior to the team visit. 22
.")
23 Eligibility Requirements A - Clinic organizational Structure *required document (*consider the position of the patient) B - Board Certification/Licensure: HCH Structure *required document (*this is met in the contents of the LOI) 23

24 Access and Communication Standard A 1,2 - Services to all patients with chronic & complex conditions interested in participation in care coordination services. *required document B 1,2 a,b,c,d & 3 a,b - Access to patient information. *required document C - Collect and apply cultural and language information D - The patient s preferred method of communication E - Inform patients of access to specialty resources F - Ensure compliance with privacy and security 24
25 Access and Communication Standard A 1,2 The applicant establishes a process to systematically screen patients to identify patients who would benefit from care coordination services based on the patient s medical and non-medical complexity. A population screening Defines patient risk level Trigger to identify as a patient receiving CC services Policy/protocol outlines the who does what and how of identifying patients for care coordination. 25
26 Access and Communication Standard B 1,2 a,b,c,d & 3 a,b Aa system to support continuous access during and after regular clinic hours for patient to communicate with the HCH team and the team knows the patient s preferred communication method. 1) Patients are informed that they have continuous access 2) the designated clinic staff has continuous access to medical record information: (a) contact information, PCP name and contact information, patient identified as receiving CC services. (b) racial or ethnic background, primary language and preferred means of communication (c) Consents and restrictions for releasing medical information (d) the patient's diagnoses, allergies, medications related to chronic and complex conditions, and whether a care plan has been created for the patient 3) appointment scheduling is appropriate based on: (a) acuity (b) access to avoid unnecessary ER visit or hospitalization 26
27 Access and Communication Standard C Language, ethnic and racial background supports the provision of relevant care, that is of value to the patient and supports a culturally appropriate care plan. Process to document the information Staff is trained Plan to access interpreters as appropriate 27
28 Access and Communication Standard D The clinic asks the patient and their family about their preferred method of communication. This information is accessible to the HCH clinic team. 28
29 Access and Communication Standard E The patient may choose a specialty care resource without regard to whether a specialist is a member of the same provider group or network as the patient's health care home, and that the patient is then responsible for determining whether specialty care resources are covered by the patient's insurance. 29
30 Access and Communication Standard F The applicant has privacy and security measures to comply with the requirements of the Health Insurance Portability and Accountability Act, Code of Federal Regulations, title 45, parts to , and the Minnesota Government Data Practices Act, Minnesota Statutes, chapter 13 30
31 Registry Standard 3A - Searchable registry for systematic population review *required document The applicant uses a registry and process to guide the management of health care services, provide appropriate follow-up and identify any gaps in care for clinic populations. 3B 1,2 - Electronic registry data elements necessary to track care. (name, age, gender, contact information, and identification number) 31
32 Care Coordination Standard 5A 1,2,3 - Requirements for care coordination team 5B - Use of health care team, designation of personal clinician, & patient is informed *required document 5C - Routine face-to-face discussion between personal clinician & care coordinator 5D - Dedicated time for care coordinator *required document 5E 1,2,3,4,5,6 - Care Coordination processes & documentation 32
33 Care Coordination Standard 5A 1,2,3 HCH team relationships are central to the HCH. The PCP, CC and patient relationships support effective information sharing, goal setting, care coordination, care planning and follow-up support. The patient and the care team set goals and identify resources to achieve goals. The PCP and CC ensure continuity of care. The patient and care team identify method of contact with the care team and community services. 33
34 Care Coordination Standard 5B Health care team, designation of PCP, and patient is informed *required document To assure continuity of care, each patient has a designated primary care provider. Patients receiving care coordination services also have a designated care coordinator. The health care home teams provide and coordinate the patient s care, including communication and collaboration with specialists. Process for selecting PCP PCP and CC (if receiving CC services) are identified in the EMR 34
35 Care Coordination Standard 5C Routine face-to-face discussion between personal clinician and care coordinator Direct communication in which routine, face-to-face discussions take place between the PCP and the care coordinator. Definition: Subp. 15. Direct communication. "Direct communication" means an exchange of information through the use of telephone, electronic mail, video conferencing, or face-to-face contact without the use of an intermediary. For purposes of this definition, an interpreter is not an intermediary. 35
36 Care Coordination Standard *required document 5D Dedicated time for care coordinator Designated protected time is essential to performing care coordination functions and making improvements in population outcome measurements. Job description Job responsibilities Job training 36
37 Care Coordination Standard 5E Care coordination processes reflect a plan for communication between the team and the patient to assure continuity of care and services. 1. Referral tracking and follow up 2. Tests ordered, results tracked and timely notification to patients 3. Admissions to hospital or skilled nursing facilities are tracked 4. Timely discharge planning 5. Medication reconciliation and pharmacy communication 6. Links to external team members and care plans 37
38 Care Plan Standard 7A 1,2,3,4,5,6 - Care plan policies & procedures *required document 7B 1,2,3,4 & C - Care plan goals & action plans 38
39 Care Plan Standard 7A 1,2,3,4,5,6 Care Planning Policy/Procedure document *required document 1) actively engage and verify joint understanding of the care plan 2) engage all appropriate members of the health care team 3) incorporate pertinent elements of the assessment about the patient s health risks and chronic conditions 4) review, evaluate, and, if appropriate, amend the care plan, jointly with the patient, at specified intervals appropriate to manage health and measure progress toward goals 5) provide a copy of the care plan to the patient upon completion of creating or amending the plan 6) Use and document the use of evidence-based guidelines for medical services and procedures. 39
40 Care Plan Standard 7B 1,2,3,4 & C Care plan goals & action plans PCP and CC; preventive care; care of chronic conditions; management plan for exacerbations of chronic conditions; end of life planning; patient identified, patient centered goals and resources to achieve those goals. De-Identified Care Plans uploaded or available at the site visit for review by the MDH HCH Team- will review for the required elements, and SMART Goals. 40
41 Quality Improvement (QI) Standard 9A 1,2,3,4 - Establishes HCH quality team that reflects clinic structure *required document 9B - Quality team has a mechanism for communication & feedback *required document 9C - Quality team demonstrates ability to do quality measurement 9D 1,2,3,4 - Participation in the learning collaborative 9E - Team has mechanism for communication & feedback for information from Learning Collaborative 41
42 Quality Improvement Standard 9A 1,2,3,4 HCH quality team that reflects clinic structure *required document A patient- and family-centered health care home relies on patients and health care team members to provide input to the clinic s quality activities. Patient Partners two or more Personal Clinician Clinic administration or management Care Coordinator Submit six months of quality team meeting minutes 42
43 Quality Improvement Standard 9B Quality team has a mechanism for communication & feedback *required document The applicant follows procedures to share their work and elicit feedback from HCH team members staff regarding quality improvement. Process How are staff informed of QI How are patients informed of QI 43
44 Quality Improvement Standard 9C Quality team demonstrates ability to measure, analyze, and track changes in at least one quality indicator selected by the applicant based upon the opportunity for improvement. Patient advisory involvement? What is the objective? What are the methods How will you measure What was the outcome? Next Steps? A PDSA process 44
45 Quality Improvement Standard 9D 1,2,3,4 Participation in the learning collaborative. The MDH HCH Learning Collaborative provides a supportive learning environment for the clinic. Participation through representatives that reflect the structure of the clinic is encouraged: (1) one or more clinicians who deliver services in the HCH (2) one or more care coordinators (3) one or more administration/management participants (4) two or more patient representatives *Documentation of staff attending, dates, sessions. 45

46 Quality Improvement Standard 9E Team has mechanism for communication & feedback for information from Learning Collaborative *required document The applicant has a process for sharing information and eliciting feedback as a result of participation in the MDH HCH Learning Collaborative. *This process could be addressed in 9B 46
47 Step 4: Update Assessments Complete Even Numbered Standards. The recertification self-assessment is used to determine if the applicant meets the documentation requirements for HCH recertification and is ready for a team visit. Applicants submit their HCH Assessment online at least three weeks prior to their recertification team visit. Site evaluators will review the clinics submitted assessment prior to the team visit. 47
48 Recertification Subparts to reflect progress Subpart 2 Patient Activation Subpart 4 Registries to Track Gaps in Care Subpart 6 Shared Decision Making, Community Partnerships, Teams working to the full extent of licensure, Transitions in Care Subpart 8 External Care Plans Subpart 10 Quality Measurement and Triple Aim Quality Plan 48


49 Access and Communication Standard.0040 Subpart 2 Patient Participation Submit strategies used to encourage patients to take an active role in managing their care. Describe the clinic s progress in one area: Patient s readiness for change Literacy level Barriers to learning 49
 Literacy")
50 .0040 Subpart 2 Patient Participation Examples: Clinic Level Process: Measurement of patient and family centered care: PCMH-A (questions 9-11) Family voices The Institute for patient & family centered care Individual Patient Process: Teach-Back Method Ask Me 3 Patient Activation Measure (PAM) Literacy Assessment/Questionnaire 50

51 .0040 Subpart 4 Registries & Tracking Gaps in Care Documented process with identified staff time for: Pre-visit planning Call reminders for preventive care or procedures Follow-up appointments for chronic conditions Guidelines to identify patients with gaps in services Evidence that the registry is actively worked by the care team Internal audit process Job performance review Blinded copies of completed work tools Work assignments 51
52 Examples:.0040 Subpart 6A Shared Decision-Making Workflows to solicit patient participation & shared decision-making Policies patient and family-centered principles Job descriptions Education programs Tools: Patient Activation Measure (PAM), Ottawa Shared Decision Making tools, questionnaires or other tools Measurement of patient /family centered care Patient stories/chart documentation 52

53 .0040 Subpart 6B Community Partnerships Demonstration of on-going partnership with at least one community resource. Meeting Minutes Communication or education plan Formal referral agreements Work plan Examples of community resources Waiver or Senior services Local public health Home Health Assisted living Schools Behavioral Health 53

54 .0040 Subpart 6C Care Team Practices to the top of licensure Clinicians & team members working at the top of their education, licensure, and training. Job descriptions/responsibilities Workflows, swim lanes QI project related to workflow or team responsibilities 54
55 .0040 Subpart 6D Planning for Transitions in Care Anticipatory planning care transitions: Pediatric to adult care Transition to assisted living, skilled nursing or memory care facility Transition to temporary rehabilitation Transition to palliative care or hospice 55
56 .0040 Subpart 8 External Care Plans Identify patients with care plans who also have external care plans. Process used to create a comprehensive care plan which adds relevant information from the external care plan. Examples: wound care, falls prevention, behavioral health, asthma action plan. Submit evidence/documentation demonstrating integration of external care plans. 56
57 .0040 Subpart 10 Quality Measures Examples of Triple Aim Indicators: Reduced duplication of services Hospital readmissions, ER usage Poly pharmacy Patient satisfaction surveys Immunization rates Advanced directives, physician orders for life sustaining treatment (POLST) Optimal care scores 57
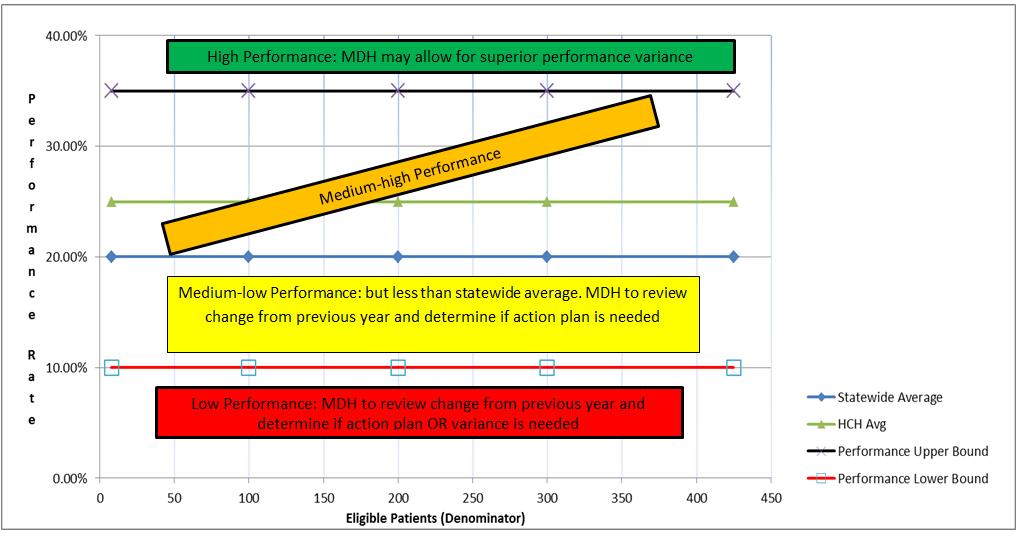
58 .0040 Subpart 10 A Reporting & Quality Improvement1 Statewide Quality Reporting Patient level data: Pursuant to Minnesota Rules, chapter , and Minnesota Statutes, section 256B.0752, the applicant will submit health care homes data in the manner prescribed by the commissioner to fulfill evaluation requirements. To meet this requirement, the applicant will submit patient level data to MDH, in the manner prescribed by the commissioner. The applicant will submit data through the MDH contracted data collection vendor; the data collection vendor will provide de-identified patient-level data from the applicant to MDH for the purposes of evaluation. 58
59 .0040 Subpart 10 A Reporting & Quality Improvement2 Statewide Quality Reporting Please see the HCH Performance Measurement & Evaluation Data Submission webpage for current SQRMS measures. 59

60 .0040 Subpart 10 B Quality Improvement Planning The clinic demonstrates they have measured, analyzed, and tracked an indicator from each Triple Aim of health improvement: Improvement in patient health Quality of patient experience Cost effectiveness of services 60
61 Health Quality Care Homes Plan Document Recertification Quality Plan Document Standard 10B: At Recertification the HCH selects at least one quality indicator from each of the following categories below ( triple aim ) and measures, analyzes and tracks those indicators throughout the year. To meet this standard the HCH submits its annual quality plan and quality reports with data that has been measured, analyzed and tracked. The quality plan may include the quality measures that are submitted to the Statewide Quality Reporting System or may be based on other quality needs. Quality plans may be submitted in any form. The following is an example template of how the clinic might organize their quality plan. PDSA (Plan, Do, Study, Act) planning cycles also work well to meet this standard by demonstrating the quality work in the quality plan, or other structured QI methods. Quality Plan Quality Goals in Each Category. Data Collection Methods (Measures / Tools / Methods) Clinical improvement in patient health Action Plan (Timeline, responsible person, PDSA.) Patient Experience Cost Effectiveness 61
62 Quality Plan Document Example 62

63 HCH Benchmark Reporting 63
64 .0040 Subpart 11 A, B Shows internal improvement over time Reflects comparison of MN HCH certified clinics Follows established state or federal standards Uses best practices, outcome-based measures Assures accountability at recertification Reflects the framework for statewide quality improvement 64
65 HCH Benchmarks 65
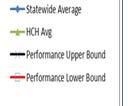
66 Benchmarking Approach Internal and external benchmarking using a hierarchy approach: A performance (comparison) benchmark, and An internal improvement benchmark Benchmarks are established at the clinic level. Statewide averages are the aggregate of all the optimal patients eligible to be in the measure. Health Care Home averages are the aggregate of all the optimal patients eligible for the certified health care home. 66
67 Statewide and HCH Averages The statewide average is calculated by taking the total number of optimal patients in the state (numerator) divided by the total number of eligible patients in the state (denominator). The health care home average is calculated by taking the total number of optimal patients at the HCH clinic sites (numerator) divided by the total number of eligible patients at the HCH clinic sites (denominator). 67
68 Improvement Benchmark If a clinic s rate is less than the statewide average then MDH will review the relative percent change from the previous year. Factors to consider when reviewing the relative percent change from the previous year are: High improvement can be considered a 10 % change or greater from the previous year. Stable performance can be considered a change in performance between (-9.9% to 9.9%) from the previous year. Reduced performance can be considered a change greater than 10 % from the previous year. 68
69 Performance Benchmarks 69
70 Improvement Benchmark If a clinic s rate falls into the low performance range then MDH will review the change in performance from the previous year and work directly with the clinic to determine if an action plan and variance is needed to meet the standard. 70
71 Benchmarking - Baseline and Beyond One year following the initial HCH certification the benchmarking results serve as the baseline for the clinic. Three years following initial HCH certification benchmarking results are a major component of the recertification process. Benchmark results become the measure of clinical quality. 71

72 Access to MNCM Benchmarking Reports 72


73 Recertification Team Visit 73
74 Step 5: Team Visit The Team meeting is an opportunity for the clinic or organization to share their story of HCH progression. Applicants should include care team representation, care coordinator(s), leadership, and patient partners. Assesses the progression in HCH implementation within the care delivery model. Completed by trained reviewers from clinical staff, consumers and Minnesota State employees. Completed in a two hour team meeting format. 74
75 Preparing for Team Visit Planning will take place with your regional HCH Nurse Planner. Some common topics include: Culture change and care team development Successes and challenges New planned initiatives Required updates to subparts Review of previously unresolved recommendations and variances Review of quality improvement activities, committee structure changes, and data collection Review of SQRMS Benchmark report 75
76 Team meeting: Benchmark Reporting Review and discuss HCH benchmarking data at the team meeting. Based on results the certified clinic may: Submit a variance for superior outcomes and continued progress on standards if eligible, or Continue with present improvement plan, or Submit a variance with action plan for justifiable failure to show measureable improvement. 76
77 Application Process An automated MDH notifies the applicant that the recertification completion date is 90 days away. During this time period: Required letter of intent, application and self assessment have been submitted. Required documents have been submitted and reviewed. Team visit has been completed. 77


78 Step 6: MDH Notification MDH will notify the applicant of certification status. The report summarizes how the clinic is meeting each of the standards. Applicants meeting all of the standards are recertified. Celebrate! Payer notification to be completed by the applicant. 78
79 Variances and Recommendations 79
80 Optional Step: Variance and Appeals Options for unmet standards: Submit a request for a variance. Request support or technical assistance from MDH. Develop and submit a corrective action plan which is reviewed by MDH. File an appeal. The applicant has 30 days from the date of receiving a certification denial notice to appeal the decision. 80
81 Variance Criteria Subpart 1 At certification or recertification, the applicant may request a variance or the renewal of a variance from a requirement in parts to
82 Variance Types Minor variance may be granted to the HCH for good cause or when failure to grant a variance would result in hardship. It is identified that a minor element of the rule is not implemented. Experimental variance may be granted where a HCH offers an innovative replacement to meet the standard. Hardship Variance: A significant hardship that prevents implementation. 82
83 Variance Process Applicant submits a variance for an identified subpart within the HCH online portal. The Nurse Planner is available to support the applicant with this process. 83
84 Variance submission A variance may be submitted: During the application process After the site visit During remedial planning After an appeal 84
85 Variance Duration Subpart 2. Conditions and duration. The commissioner may impose conditions on the granting of a variance according to Minnesota Statutes, section The commissioner may limit the duration of a variance and may renew a variance. Variances are normally in place for one year or until resolved. Clinics may submit a request to extend a variance. 85
86 Recommendations Recommendations are observations made by the site visit evaluators reflecting opportunity for improvement. Recommendations are: Not prescriptive Addressed by the clinic as appropriate Reviewed at the following recertification to describe how they were addressed. 86

87 Reimbursement for Care Coordination Services 87
88 Care Coordination: Billing and Reimbursement Legislative Requirements for HCH Care Coordination Payment: [256B.073] DHS and MDH developed a system of per-person care coordination payments to certified HCHs Fees vary by thresholds of patient complexity Agencies consider feasibility of including non-medical complexity information Implemented for all public program enrollees by July 1, [62U.03] Covers SGIP, small group self-insured 88
89 Care Coordination Payment Guiding Principles HCHs provide population management. Every patient is part of the clinic s HCH. HCHs determine which patients will benefit from: care coordination and are eligible for reimbursement routine panel management (preventive care, appointment follow-up). Clinics implement key processes for successful care coordination billing. 89
90 Population Management Goal Clinics implement processes to identify patients from the entire clinic population who would benefit from care coordination services. New patients Current patients with health changes Established patients with chronic conditions. Patients who are identified and decline care coordination services. 90

91 Population Management What does your population look like? 91

92 Implement HCH Tier Tool 92
93 Complexity Tier Level Needed for Payment Patient s Tier Level (based on the count of major condition groups) Tier 0 (none) Tier 1 (1-3) Tier 2 (4-6) Tier 3 (7-9) Tier 4 (10 or more) Presence of either of the two supplemental complexity factors 93
94 Workflow Development: Tiering & Billing Determine who does what and when. Complete the Care Coordination Tier Assignment tool. The care team establishes a work flow for communication of the tier score. Key: Establish billing and accounting department workflows and communication processes. Establish payer contracting (see slide #98). Develop automated workflows within EMR. May begin with a manual process. Tier level is supported by documentation. 94
95 Coding Structure for Billing 95
96 Key Billing Process Steps 96
97 Key Denial Process Steps 97
98 Multi- Payer Communication Prior to Certification, identify payer networks supporting care coordination reimbursement. Work with payers to establish payment rates and method of claim submission and payment Tiering Methodology (Medicaid; private and commercial plans) PMPM Contract Arrangements CMS Medicare Care Coordination (chronic care management codes see slide #99-100) Identify payers where there may be a patient co-pay and determine a process. Address how to manage billing for uninsured. 98
99 New Medicare -CMS Chronic Care Management (CCM) Codes, January 2015 As of January 1, 2015, practices began submitting claims under new CCM codes. Payment/PhysicianFeeSched/index.html 99
100 CMS Chronic Care Management Codes Replaces Medicare: MAPCP, CPI and other PCMH demos. Practices need to meet standards similar to the HCH standards to submit claims. (see CMS requirements). Patient agreement to services is required. Service requirement of at least 20 minutes of clinical staff time directed by a physician or qualified health care professional per calendar month. Patient has two or more chronic conditions expected to last at least 12 months. Electronic health records requirement; specific requirement for an electronic care plan. A comprehensive care plan is established, implemented, revised and monitored. PCMH certification is not required. 100

101 Create Your Clinic s Roadmap Population Management in Health Care Homes Care Coordination Tiering Processes Billing Workflows Multi-payer Input 101
102 Evaluation Health Care Homes, Five Year Program Evaluation: Key findings from the University of Minnesota Evaluation 102

103 Health Care Homes A Business Case 103
104 Thank you! Visit the MDH HCH website: MDH HCH main phone number: questions to 104
105 HCH Nurse Planners Contact Information Bonnie LaPlante, MDH HCH Program Director Tina Peters Metro Area Kathleen Conboy Metro Area Joan Kindt Southern Region Danette Holznagel Northern Region
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Health Care Home Benchmarking. Marie Maes-Voreis MDH Director, Health Care Homes Nathan Hunkins MNCM Account/Program Manger
 Health Care Home Benchmarking Marie Maes-Voreis MDH Director, Health Care Homes Nathan Hunkins MNCM Account/Program Manger Presentation Objectives Background: HCH Measurement & Benchmarks (Marie Maes-Voreis)
Health Care Home Benchmarking Marie Maes-Voreis MDH Director, Health Care Homes Nathan Hunkins MNCM Account/Program Manger Presentation Objectives Background: HCH Measurement & Benchmarks (Marie Maes-Voreis)
Evaluation of Health Care Homes:
 Division of Health Policy PO Box 64882 St. Paul, MN 55164-0882 651-201-3626 www.health.state.mn.us Evaluation of Health Care Homes: 2010-2012 Minnesota Department of Health Minnesota Department of Human
Division of Health Policy PO Box 64882 St. Paul, MN 55164-0882 651-201-3626 www.health.state.mn.us Evaluation of Health Care Homes: 2010-2012 Minnesota Department of Health Minnesota Department of Human
Patient Experience of Care
 Minnesota Department of Health: Protecting, maintaining and improving the health of all Minnesotans Minnesota Statewide Quality Reporting and Measurement System (SQRMS): Patient Experience of Care March
Minnesota Department of Health: Protecting, maintaining and improving the health of all Minnesotans Minnesota Statewide Quality Reporting and Measurement System (SQRMS): Patient Experience of Care March
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Minnesota Accountable Health Model Practice Transformation Grant Program
 Amendment to the Request for Proposals Minnesota Accountable Health Model Practice Transformation Grant Program Posted October 20, 2014 Amended November 5, 2014 As of October 23, 2014, the following changes
Amendment to the Request for Proposals Minnesota Accountable Health Model Practice Transformation Grant Program Posted October 20, 2014 Amended November 5, 2014 As of October 23, 2014, the following changes
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
Minnesota Health Care Home Care Coordination Cost Study
 Minnesota Health Care Home Care Coordination Cost Study Lacey Hartman, Elizabeth Lukanen, and Christina Worrall State Health Access Data Assistance Center (SHADAC) Minnesota Health Care Home Learning Days
Minnesota Health Care Home Care Coordination Cost Study Lacey Hartman, Elizabeth Lukanen, and Christina Worrall State Health Access Data Assistance Center (SHADAC) Minnesota Health Care Home Learning Days
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Fact Sheet: Stratifying Quality Measures BY RACE, ETHNICITY, PREFERRED LANGUAGE, AND COUNTRY OF ORIGIN
 MINNESOTA STATEWIDE QUALITY REPORTING AND MEASUREMENT SYSTEM Fact Sheet: Stratifying Quality Measures BY RACE, ETHNICITY, PREFERRED LANGUAGE, AND COUNTRY OF ORIGIN Overview Minnesota s 2008 Health Reform
MINNESOTA STATEWIDE QUALITY REPORTING AND MEASUREMENT SYSTEM Fact Sheet: Stratifying Quality Measures BY RACE, ETHNICITY, PREFERRED LANGUAGE, AND COUNTRY OF ORIGIN Overview Minnesota s 2008 Health Reform
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
HITECH* Update Meaningful Use Regulations Eligible Professionals
 HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Fact Sheet. Minnesota All Payer Claims Database Submission Requirements and Variance Management. Background. MN APCD Submission Requirements
 Fact Sheet Minnesota All Payer Claims Database Submission Requirements and Variance Management Background As part of a bi-partisan response to concerns about the sustainability of health care spending
Fact Sheet Minnesota All Payer Claims Database Submission Requirements and Variance Management Background As part of a bi-partisan response to concerns about the sustainability of health care spending
Welcome to. Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes
 Welcome to ASTHO s Delivery and Payment Reform Technical Assistance Call Series Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes Presented by ASTHO and
Welcome to ASTHO s Delivery and Payment Reform Technical Assistance Call Series Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes Presented by ASTHO and
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
REPORT OF THE BOARD OF TRUSTEES
 REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 2/4/2018 The following program policies are applicable to all contracted providers and practices recognized
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 2/4/2018 The following program policies are applicable to all contracted providers and practices recognized
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
NEVADA County Behavioral Health Quality Improvement Work Plan Fiscal Year 2016-2017 Table of Contents I. Quality Improvement Program Overview...1 A. Quality Improvement Program Characteristics...1 B. Annual
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
The Minnesota Accountable Health Model
 The Minnesota Accountable Health Model L E A R N I N G S F R O M S I M : I N T E G R AT I O N O F P R I M A R Y A N D B E H AV I O R A L H E A LT H R U R A L H E A LT H C O N F E R E N C E J U N E 2 0,
The Minnesota Accountable Health Model L E A R N I N G S F R O M S I M : I N T E G R AT I O N O F P R I M A R Y A N D B E H AV I O R A L H E A LT H R U R A L H E A LT H C O N F E R E N C E J U N E 2 0,
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
Health Reform in Minnesota: An Analysis of Complementary Initiatives Implementing Electronic Health Record Technology and Care Coordination
 Health Reform in Minnesota: An Analysis of Complementary Initiatives Implementing Electronic Health Record Technology and Care Coordination Karen Soderberg 1*, Sripriya Rajamani 2, Douglas Wholey 3, Martin
Health Reform in Minnesota: An Analysis of Complementary Initiatives Implementing Electronic Health Record Technology and Care Coordination Karen Soderberg 1*, Sripriya Rajamani 2, Douglas Wholey 3, Martin
Reimagining PCMH Recognition
 Reimagining PCMH Recognition August 2016 Michael S. Barr, MD, MBA, MACP Executive Vice President Quality, Measurement & Research Group Re-use without permission is prohibited 1 Where is PCMH in future
Reimagining PCMH Recognition August 2016 Michael S. Barr, MD, MBA, MACP Executive Vice President Quality, Measurement & Research Group Re-use without permission is prohibited 1 Where is PCMH in future
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
SWAN Alerts and Best Practices for Improved Care Coordination
 SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
SWAN Alerts and Best Practices for Improved Care Coordination IHIN and SWAN Course Overview Our Goal: To educate healthcare providers in how to manage SWAN alerts for meaningful impact at the point of
Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System
 Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System JUNE 2016 HEALTH ECONOMICS PROGRAM Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive
Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System JUNE 2016 HEALTH ECONOMICS PROGRAM Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
CMS Incentive Programs: Timeline And Reporting Requirements. Webcast Association of Northern California Oncologists May 21, 2013
 CMS Incentive Programs: Timeline And Reporting Requirements Webcast Association of Northern California Oncologists May 21, 2013 Objective This webcast will address CMS s Incentive Program reporting requirements
CMS Incentive Programs: Timeline And Reporting Requirements Webcast Association of Northern California Oncologists May 21, 2013 Objective This webcast will address CMS s Incentive Program reporting requirements
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Health Home State Plan Amendment
 Health Home State Plan Amendment OMB Control Number: 0938-1148 Expiration date: 10/31/2014 Transmittal Number: OK-14-0011 Supersedes Transmittal Number: Proposed Effective Date: Jan 1, 2015 Approval Date:
Health Home State Plan Amendment OMB Control Number: 0938-1148 Expiration date: 10/31/2014 Transmittal Number: OK-14-0011 Supersedes Transmittal Number: Proposed Effective Date: Jan 1, 2015 Approval Date:
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
John W. Gahan Jr. Department of Health
 John W. Gahan Jr. Department of Health Indigent Care Pool Electronic Health Record Medicaid Reimbursement FQHC s Other Clinics Appeals Meaningful Use Primary Medical Home General Billing 2010 AHCF-1 Questions
John W. Gahan Jr. Department of Health Indigent Care Pool Electronic Health Record Medicaid Reimbursement FQHC s Other Clinics Appeals Meaningful Use Primary Medical Home General Billing 2010 AHCF-1 Questions
Minnesota Accountable Health Model Accountable Communities for Health Grant Program
 Request for Proposals Minnesota Accountable Health Model Accountable Communities for Health Grant Program September 2, 2014 Page 1 of 79 Contents: 1. Overview... 3 2. Available Funding and Estimated Awards...
Request for Proposals Minnesota Accountable Health Model Accountable Communities for Health Grant Program September 2, 2014 Page 1 of 79 Contents: 1. Overview... 3 2. Available Funding and Estimated Awards...
INSERT ORGANIZATION NAME
 INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Health Care Home (HCH) Payment Methodology. Webinar 3/24/10
 Payment Methodology. Webinar 3/24/10") Health Care Home (HCH) Payment Methodology Webinar 3/24/10 Plan for Today Place the payment system in context Provide an overview and examples of how the payment system will work Talk about next steps
Health Care Home (HCH) Payment Methodology Webinar 3/24/10 Plan for Today Place the payment system in context Provide an overview and examples of how the payment system will work Talk about next steps
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System
 Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System JUNE 2015 DIVISION OF HEALTH POLICY/HEALTH ECONOMICS PROGRAM Minnesota Statewide Quality Reporting and Measurement
Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System JUNE 2015 DIVISION OF HEALTH POLICY/HEALTH ECONOMICS PROGRAM Minnesota Statewide Quality Reporting and Measurement
Health Current: Roadmap Practice Transformation using Information & Data
 Health Current: Roadmap Practice Transformation using Information & Data Melissa A. Kotrys, MPH Chief Executive Officer July 2017 2 Arizona Health-e Connection is now Health Current. Powering the future
Health Current: Roadmap Practice Transformation using Information & Data Melissa A. Kotrys, MPH Chief Executive Officer July 2017 2 Arizona Health-e Connection is now Health Current. Powering the future
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Medicaid EHR Incentive Program What You Need to Know about Program Year 2016
 Medicaid EHR Incentive Program What You Need to Know about Program Year 2016 February 2017 Carrie Ortega, Health IT Project Manager Imeincentives@dhs.state.ia.us 1 Attestation Reminders 2016 Dates to Remember
Medicaid EHR Incentive Program What You Need to Know about Program Year 2016 February 2017 Carrie Ortega, Health IT Project Manager Imeincentives@dhs.state.ia.us 1 Attestation Reminders 2016 Dates to Remember
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Minnesota Statewide Quality Reporting and Measurement System (SQRMS):
:") Minnesota Department of Health: Protecting, maintaining and improving the health of all Minnesotans Minnesota Statewide Quality Reporting and Measurement System (SQRMS): Clinic and Provider Registration,
Minnesota Department of Health: Protecting, maintaining and improving the health of all Minnesotans Minnesota Statewide Quality Reporting and Measurement System (SQRMS): Clinic and Provider Registration,
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Professionals
 Incentive Program: A Webinar for Eligible Professionals") Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Professionals Presenters Ivy Bela, HHSC Leo Gutierrez, TMHP Craig Earls, CGI Wendy Wacasey, NTREC February 3, 2011 1 Overview
Medicaid Electronic Health Record (EHR) Incentive Program: A Webinar for Eligible Professionals Presenters Ivy Bela, HHSC Leo Gutierrez, TMHP Craig Earls, CGI Wendy Wacasey, NTREC February 3, 2011 1 Overview
Meaningful Use Stage 2
 Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Minnesota Statewide Quality Reporting and Measurement System:
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE. Angel L. Moore, MAEd, RHIA Eastern AHEC REC
 THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
ATTACHMENT A Delivery System Reform Incentive Payment (DSRIP) Program Renewal Request
 Program Renewal Request") Background ATTACHMENT A The New Jersey Department of Health (DOH) operates the Delivery System Reform Incentive Payment (DSRIP) program as required by Section 93(e) of the Special Terms and Conditions
Background ATTACHMENT A The New Jersey Department of Health (DOH) operates the Delivery System Reform Incentive Payment (DSRIP) program as required by Section 93(e) of the Special Terms and Conditions
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
Clinical Medical Standing Orders (PCMH 1G) Delegation of Duties (NM Medical & Nurse Practice Acts, FTCA) CLIA Waived Testing (CLIA)
 Delegation of Duties (NM Medical & Nurse Practice Acts, FTCA) CLIA Waived Testing (CLIA)") Rev. 2/26/2013 REQUIRED POLICY Administration Governance (HRSA, BPHC, NM Licensure) Conflict of Interest (BPHC) Scope of Services/Locations (HRSA, BPHC) Hours of Operations & After Hours Coverage (BPHC,
Rev. 2/26/2013 REQUIRED POLICY Administration Governance (HRSA, BPHC, NM Licensure) Conflict of Interest (BPHC) Scope of Services/Locations (HRSA, BPHC) Hours of Operations & After Hours Coverage (BPHC,
Community Paramedicine Seminar Milbank Memorial Fund, Nov
 Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Draft Covered California Delivery Reform Contract Provisions Comments Welcome and Encouraged
 TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
Shana Scott, JD, MPH, Health Systems Team Lead Tuesday, October 3, 2017
 Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Wisconsin State Plan to Serve More Children and Youth within Medical Homes
 Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
Wisconsin State Plan to Serve More Children and Youth within Medical Homes Including those with special health care needs Acknowledgments The Wisconsin Children and Youth with Special Health Care Needs
Meaningful Use Participation Basics for the Small Provider
 Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions
 Project Frequently Asked Questions") Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI