The Medical Home Model as a Solution to Diabetes Disparities
|
|
|
- Elinor Quinn
- 5 years ago
- Views:
Transcription

1 Kenyatta Lee, MD Clinical Director Community Clinics Department University of Florida/Shands Jacksonville The Medical Home Model as a Solution to Diabetes Disparities
2 Objectives: 1Provide an overview the history of the Patient Centered Medical Disparities: Home (PCMH) 2Discuss preliminary outcome data PCMH studies and demonstration projects 3Describe the Jacksonville Urban Disparity Institute Medical Home Model and its impact on diabetes disparities 4Summary: pros and cons of the PCMH

3 "Americans can always be counted on to do the right thingafter they have exhausted all other possibilities Disparities: [Winston Churchill]
4 What is the medical home model? Disparities: A primary care practice that provides patients with accessible, continuous, and coordinated care through a patient-centered, physicianguided, cost efficient and longitudinal approach to healthcare
5 Patient Centered Care is not a new concept Disparities: Putting the patient first In his classic address to the 1910 graduates of Rush Medical College, Dr Will Mayo stated "The best interest of the patient is the only interest to be considered
6 196 - American Academy of Pediatrics Coined the term Medical Home Disparities: Initially used to care for special populations of patients who needed specialty services and support functions for chronic diseases Evolved into a partnership with families to provide primary health care to all children and adolescents The care was to be accessible, coordinated, comprehensive, continuous, compassionate, and culturally sensitive
7 The Chronic Care Model 2001 Wagner et al suggest that traditional health care systems are poorly configured to meet the needs of the chronically ill Disparities: because they are designed to provide a symptom-driven response to acute illness
8 200 AOA, AAFP, AAP, and ACP developed the Joint Principles of the Patient-Centered Medical Home (200) Disparities: Represent 333,000 physicians An approach to providing comprehensive primary care for children, adolescents, and adults Facilitates partnerships between individual patients, their personal physicians, and when appropriate, the patient s family
9 The Patient Centered Primary Examples of Broad Stakeholder Support & Participation Care Collaborative Providers ACP AAP AAFP AOA ABIM ACC ACOI AHI Payers The Patient-Centered Medical Home Purchasers IBM General Motors FedEx General Electric Pfizer Microsoft Business Coalitions Merck Patients BCBSA United CIGNA WellPoint Aetna Humana HCSC NCQA AFL-CIO National Partnership for Women and Families Foundation for Informed Decision Making SEIU
10 Centered Medical Home (200) Payment Personal Physician Joint Joint Principles of the Patient Physiciandirected Medical Practice Enhanced Access Principles Joint Principles of the of the PCMH PCMH Whole Person Orientation Quality and Safety Care is Coordinated and/or Integrated
11 Health Care Reform and the Patient Centered Medical Home From HR 3590 Patient Protection and Affordable Care Act Disparities: Sec 203 State option to provide health homes for enrollees with chronic conditions Title V Sec 5301 Training in family medicine, general internal medicine, general pediatrics, and physician assistantship Sec 5501 Expanding access to primary care services and general surgery services Health Care and Education Reconciliation Act Sec 1202 Payments to primary care physicians
12 How will we know a medical home when we see Disparities: one?
13 NCQA Medical Home Recognition Standard 1: Access and Communication A Has written standards for patient access and patient communication** B Uses data to show it meets its standards for patient access and communication** Pts 4 5 Standard 5: Electronic Prescribing A Uses electronic system to write prescriptions B Has electronic prescription writer with safety checks C Has electronic prescription writer with cost checks Pts Standard 2: Patient Tracking and Registry Functions A Uses data system for basic patient information (mostly non-clinical data) B Has clinical data system with clinical data in searchable data fields C Uses the clinical data system D Uses paper or electronic-based charting tools to organize clinical information** E Uses data to identify important diagnoses and conditions in practice** F Generates lists of patients and reminds patients and clinicians of services needed (population management) Standard 3: Care Management A Adopts and implements evidence-based guidelines for three conditions ** B Generates reminders about preventive services for clinicians C Uses non-physician staff to manage patient care D Conducts care management, including care plans, assessing progress, addressing barriers E Coordinates care//follow-up for patients who receive care in inpatient and outpatient facilities Standard 4: Patient Self-Management Support A Assesses language preference and other communication barriers B Actively supports patient self-management** 9 Pts Pts Pts 2 4 Standard 6: Test Tracking A Tracks tests and identifies abnormal results systematically** B Uses electronic systems to order and retrieve tests and flag duplicate tests Standard : Referral Tracking A Tracks referrals using paper-based or electronic system** Standard 8: Performance Reporting and Improvement A Measures clinical and/or service performance by physician or across the practice** B Survey of patients care experience C Reports performance across the practice or by physician ** D Sets goals and takes action to improve performance E Produces reports using standardized measures F Transmits reports with standardized measures electronically to external entities Standard 9: Advanced Electronic Communications A Availability of Interactive Website B Electronic Patient Identification C Electronic Care Management Support 8 Pts 6 13 PT 4 4 Pts Pts **Must Pass Elements
14 Results in Recognition Levels Level 3: 5+ Points; 10/10 Must Pass Level 2: 50-4 Points; 10/10 Must Pass Level 1: Points; 5/10 Must Pass Increasing Complexity of Services 14 From the American College of Physicians- Michael S Barr, MD
15 Community Care of North Carolina Medicaid plan invested $40 million in 3500 primary care medical home Disparities: community physician practices Saved $231 million in 2005 and racial and ethnic access to care disparities are reduced &/or eliminated - get the care needed (preventive Soon care screenings You improved Won t! significantly in medical homes Commonwealth Fund health care quality survey IBM Patient Centered Medical Homes IBM employees pay 26-60% less overall for medical care Family insurance premiums 6% lower and Single insurance premiums 15% lower than comparable fair market rates
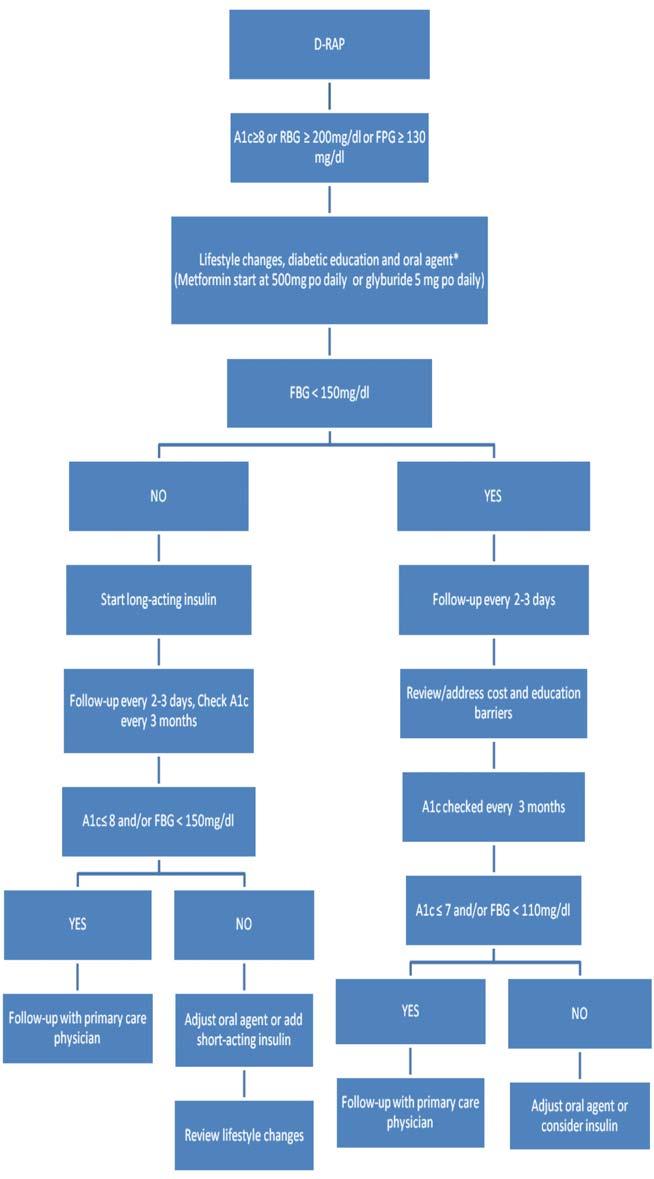
16 DIABETES RAPID ACCESS PROGRAM THE DISEASE MANAGEMENT PROTOTYPE


17 Historical Overview Community Affairs Department, 1989 Present Elizabeth Means, former VP established the department to address unmet medical needs in underserved communities The initial goal was to provide health education, health promotion, and community outreach in targeted communities Programs are primarily funded through grants, strategic partnerships, faith based organizations and community support The goal has expanded to provide free and reduced comprehensive health care to the medically underserved in the urban core

18 Community Affairs Department Community Responsive Medicine Medical Director Vice President Consultant JUDI Grant Writing Clinical Programs Community Programs Virtual Community Disparity Network Clinics Free Script D-RAP REACH HY-LIP CARE Anti-Coag Renal Delta Care Heal Thy People Shop Talk Healthy Start Sickle Cell Hep C Hispanic Initiative Women s Health Initiative Little Miracles Health Fairs HIV/AIDS Brown Bag Case Disparity Durkeeville Soutel Brentwood Eastside Management Mgmt C B C B McIntosh McIntosh Wellness Pediatric Childhood Obesity Proposed MRA PQRI Disease Case Mgmt Hybrid Traditiona l Paxon Murray Hill College Park Soutel
19 The Perfect Storm for health disparities Population - 12,512 (850,251) Gender - 53% female (48%) Adolescents ages % (142%) Adult ages % (61%) Senior adults 65 and older - 145% (10%) Race - 83% African American (29%) Median family income - $28,30 ($44,40) Children below poverty level - 384% (154%) Percent of population below poverty - 28% (119%) Unemployment - 1% (68%) Uninsured - 45% (9%) Leading health disparities health zone of the 6 health zones in Jacksonville and Duval County, Florida, in cancer, strokes, diabetes, HIV/AIDS, teen pregnancy, STD s and infant mortality *(Parentheses denote figure for Duval County, Florida)


20 JUDI-affiliated clinics and programs reflect the major causes of morbidity and mortality in Jacksonville, in both purpose and location Disparity Traditional Hybrid Soutel Wellness Durkeeville Shands Soutel 220 College Park Commonwealth Murray Hill Eastside Brentwood CB McIntosh 2
21 What makes JUDI a medical home? Standard 1: Access and Communication Disparities: Standard 2: Patient Tracking and Registry Functions Standard 3: Care Management Standard 4: Patient Self-Management Support
22 What makes JUDI a medical home? Standard 5: Electronic Prescribing Disparities: Standard 6: Test Tracking Standard : Referral Tracking Standard 8: Performance Reporting and Improvement 9: Advanced Electronic Communications

23 Diabetes Rapid Access Program (DRAP): Disparities: DRAP is a disease management program within the JUDI medical home model It was developed in 2006 and was the first of five disease management programs
24 Background The leadership within JUDI postulated that although providers were well trained and compassionate, the system of diabetes care within the practice and larger community was problematic Disparities: Providers: Unaware of the specific number of diabetic patients they cared no system in place to track patients and insure they were receiving appropriate and regular care Functioning at full capacity providing services to an average of patients needed assistance to organize and deliver complicated timeintensive care to these patients optimizing disease outcomes Expanded Providers (help) : The expanded provider s role was developed within JUDI to meet this goal This expanded provider group included nurses, clinical pharmacologists, medical assistants and registry specialists
25 Patient Enrollment: All diabetic patients in the JUDI Disparities: medical home clinic system are enrolled in the Diabetes Rapid Access Program (DRAP) Patients are identified through physician referral and active patient registries Patients may be enrolled in the DRAP and become targeted for individualized intervention
26 DRAP Active disease management : The care management nurses can initiate therapy based on established DRAP protocol (see Figure 1), Disparities: Any suggested modification in therapy is sent to the patient s primary care physician via the EHR Physicians can accept, decline or modify recommendations If the primary care physician accepts the recommendation, then medication additions are made or medication is titrated per protocol Using this method, patients may visit the disparity clinics for free, as often as needed until treatment goals are reached
27 Addressing Barriers: a)cost: A free prescription program is put in place to provide medications to patients who lack insurance and/or are unable to afford their prescriptions Insulin preparations are available through the program and are dispensed as needed Disparities: b) Time: The hours of operation of the program s clinics and the care management nurses availability are flexible enough to accommodate all patients with early morning and weekend clinic sessions offered as needed c) Education: Patients have free access to an ADA approved selfmanagement course taught by a Certified Diabetic Educator They can be referred to this course by their primary care physician, the care management nurse, or be self-enrolled based on their desire to learn more about diabetes
28 Disparities:
29 Patient Registries: The patient registries are maintained and updated daily by registry specialists A Physician Quality Reporting Initiative (PQRI) form as defined by the Centers of Medicare and Medicaid Services (CMS) is complete at each encounter Disparities: This information is subsequently forwarded and entered into the database by the registry specialist In addition, the most recent available fasting (FBG) or random blood glucose (RBG) reading for each patient is reviewed and tabulated in the registry Patients with a hemoglobin A1C 8%, and /or a fasting blood glucose (FBG) 130 mg/dl, or a random blood glucose (RBG) 200 mg/dl or diabetics who have not had a hemoglobin A1C visit in a period of three months or more are identified by the registry specialist These patients are contacted by mail and advised to come to any of the program s clinics for evaluation by nurse case managers and/or blood testing free of charge
30 Diabetes Spreadsheet DM TRACKING Patient name Date of Birth SEX MRN Date A1C LDL CK Date A1C LDL CK Date A1C LDL CK ABRAHAM,FRANCISCA 24-Oct-52 F /10/ /14/ /19/ ADAMS,RANDY 1-Jan-66 M /23/ ALLEN,LENORA 21-Nov-48 F /24/06 62 N/D 2/8/ /13/0 4 N/D ALVIN,NELLIE 2-Mar-33 F /5/ AUSTIN,CHARLENE 18-Jan-58 F /22/ /19/ /23/ BANKS,MICIAH 15-Jun-66 M // BARTLEY,JAMES 16-Feb-60 M 933 9/29/ /2/ BARTLEY,STEVE 22-Jun-60 M /15/ /13/ /1/ BENTON,JOANN 2-May-50 F /30/ BESHEARS,JOE 6-Sep-46 M /18/ // BLUE,JUNE 18-Feb-30 F /26/ /31/ BOSTIC,JANICE -Apr-53 F /9/ RESULTS AT START 1st RESULTS AFTER START 2nd RESULTS BROOKINS,ORSIE 15-Aug-21 F /26/0 0 N/D 8/3/0 93 N/D 12/20/0 64 N/D Averages Averages Averages 8 118
31 National A1c Average Brentwood College Park Eastside M urray Hill Paxon Soutel Average A1C Result Per Office Baseline First Second Third Fourth
32 Disparities:
33 Disparities:
34 In summary, patients demonstrated significantly improved glycemic control regardless of race, sex or clinic location Disparities: The success of this program across all the clinical sites highlights the applicability of the model irrespective of racial make-up of the participants seen at these sites Another key factor in the program s success was the active participation of a well-trained expanded network of providers including nurses, clinical pharmacologists, and medical assistants who took ownership of the active disease management (DRAP) program This shows that allowing a team-based patient-centered approach in such programs may facilitate delivery of services and enhance outcomes
35 Medical Home Model Implications Cons Medical Darwinism (P4P, PCMH, PQRI, MRAs, EHR, meaningful use) Margins are tight Barely Funded Mandate (presently reward does not justify the expense) Pros Improved outcomes Decreased disparities Decreased cost
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model
 Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model Robert Gabbay MD, PhD Director, Penn State Institute for Diabetes and Obesity Professor of Medicine Penn State College
Prescription for Pennsylvania The Pennsylvania Multi-Payer Statewide Medical Home Model Robert Gabbay MD, PhD Director, Penn State Institute for Diabetes and Obesity Professor of Medicine Penn State College
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Adirondack Medical Home Pilot Overview. Dennis Weaver MD MBA November 2, 2010
 Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Adirondack Medical Home Pilot Overview Dennis Weaver MD MBA November 2, 2010 Critical Success Factors Lessons Learned Partnership among all stakeholders is essential Must define common goals and timelines
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:
 Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:") 2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Stage 1 Meaningful Use Objectives and Measures
 Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
2012 Community Health Needs Assessment
 2012 Community Health Needs Assessment University Hospitals (UH) long-standing commitment to the community spans more than 145 years. This commitment has grown and evolved through significant thought and
2012 Community Health Needs Assessment University Hospitals (UH) long-standing commitment to the community spans more than 145 years. This commitment has grown and evolved through significant thought and
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Presbyterian Healthcare Services Care Management
 Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
2015 DUPLIN COUNTY SOTCH REPORT
 2015 DUPLIN COUNTY SOTCH REPORT Reported March 2016 State of the County Health Report The State of the County Health Report provides a review of the current county health statistics and compares them to
2015 DUPLIN COUNTY SOTCH REPORT Reported March 2016 State of the County Health Report The State of the County Health Report provides a review of the current county health statistics and compares them to
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers
 Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
Cardiovascular Disease Prevention and Control: Interventions Engaging Community Health Workers Community Preventive Services Task Force Finding and Rationale Statement Ratified March 2015 Table of Contents
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
New Models of Care- Looking at PCMH & Telehealth
 New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Primary Care Collaborative and the National Patient Centered Medical Home Movement
 Patient Centered Primary Care Collaborative and the National Patient Centered Medical Home Movement February 2011 Edwina Rogers Executive Director Patient Centered Primary Care Collaborative 601 Thirteenth
Patient Centered Primary Care Collaborative and the National Patient Centered Medical Home Movement February 2011 Edwina Rogers Executive Director Patient Centered Primary Care Collaborative 601 Thirteenth
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
2012 Community Health Needs Assessment
 Indiana University Health Goshen 2012 Community Health Needs Assessment A Report on Implementation Strategies to Address Community Health Needs Summary Report Our Commitment to You We are here for you,
Indiana University Health Goshen 2012 Community Health Needs Assessment A Report on Implementation Strategies to Address Community Health Needs Summary Report Our Commitment to You We are here for you,
Community Health Improvement Plan
 Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
CLOSING THE DIVIDE: HOW MEDICAL HOMES PROMOTE EQUITY IN HEALTH CARE
 CLOSING DIVIDE: HOW MEDICAL HOMES PROMOTE EQUITY IN HEALTH CARE RESULTS FROM 26 HEALTH CARE QUALITY SURVEY Anne C. Beal, Michelle M. Doty, Susan E. Hernandez, Katherine K. Shea, and Karen Davis June 27
CLOSING DIVIDE: HOW MEDICAL HOMES PROMOTE EQUITY IN HEALTH CARE RESULTS FROM 26 HEALTH CARE QUALITY SURVEY Anne C. Beal, Michelle M. Doty, Susan E. Hernandez, Katherine K. Shea, and Karen Davis June 27
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
HPV Vaccination Quality Improvement: Physician Perspective
 HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PCMH 2014 Record Review Workbook (RRWB)
") PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
Commonwealth Fund Scorecard on State Health System Performance, Baseline
 1 1 Commonwealth Fund Scorecard on Health System Performance, 017 Florida Florida's Scorecard s (a) Overall Access & Affordability Prevention & Treatment Avoidable Hospital Use & Cost 017 Baseline 39 39
1 1 Commonwealth Fund Scorecard on Health System Performance, 017 Florida Florida's Scorecard s (a) Overall Access & Affordability Prevention & Treatment Avoidable Hospital Use & Cost 017 Baseline 39 39
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare
: Billing, Codes and Need at Adelante Healthcare") Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F
 Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
Topic 3B: Documentation Prep for NCQA Recognition Focus on Standards 3, 4, and 1F Diane Altman Dautoff, MSW, EdD, Senior Consultant Heather Russo, Consultant January 2013 Welcome Introductions and Housekeeping
meaningful reality Katie Coleman, MSPH
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
Patient-centered care - from buzz word to meaningful reality. Current Health Care System
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Stage 2 Meaningful Use Objectives and Measures
 Stage 2 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Stage 2 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
medicaid commission on a n d t h e uninsured May 2009 Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid SUMMARY
 kaiser commission on medicaid SUMMARY a n d t h e uninsured Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid Why is Community Care of North Carolina (CCNC) of Interest?
kaiser commission on medicaid SUMMARY a n d t h e uninsured Community Care of North Carolina: Putting Health Reform Ideas into Practice in Medicaid Why is Community Care of North Carolina (CCNC) of Interest?
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Community Health Needs Assessment. Implementation Plan FISCA L Y E AR
 Community Health Needs Assessment Implementation Plan FISCA L Y E AR 2 0 1 5-2 0 1 8 Table of Contents: I. Background 1 II. Areas of Priority 2 a. Preventive Care and Chronic Conditions b. Community Health
Community Health Needs Assessment Implementation Plan FISCA L Y E AR 2 0 1 5-2 0 1 8 Table of Contents: I. Background 1 II. Areas of Priority 2 a. Preventive Care and Chronic Conditions b. Community Health
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE
 THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
Brave New World: The Effects of Health Reform Legislation on Hospitals. HFMA Annual National Meeting, Las Vegas, Nevada
 Brave New World: The Effects of Health Reform Legislation on Hospitals HFMA Annual National Meeting, Las Vegas, Nevada Highlights of PPACA Requires most Americans to have health insurance Expands coverage
Brave New World: The Effects of Health Reform Legislation on Hospitals HFMA Annual National Meeting, Las Vegas, Nevada Highlights of PPACA Requires most Americans to have health insurance Expands coverage
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information
 2011 Military Health System Conference Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information The Quadruple Aim: Working Together, Achieving Success Forum Moderator:
2011 Military Health System Conference Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information The Quadruple Aim: Working Together, Achieving Success Forum Moderator:
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Iatric Systems Supports the Achievement of Meaningful Use
 Iatric Systems Supports the Achievement of Meaningful Use Iatric Systems offers a wide variety of solutions to assist with today s business challenges and support hospitals in providing superior patient
Iatric Systems Supports the Achievement of Meaningful Use Iatric Systems offers a wide variety of solutions to assist with today s business challenges and support hospitals in providing superior patient
Meaningful Use Final Rule:
 Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Shana Scott, JD, MPH, Health Systems Team Lead Tuesday, October 3, 2017
 Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Community Health Needs Assessment for Corning Hospital: Schuyler, NY and Steuben, NY:
 Community Health Needs Assessment for Corning Hospital: Schuyler, NY and Steuben, NY: November 2012 Approved February 20, 2013 One Guthrie Square Sayre, PA 18840 www.guthrie.org Page 1 of 18 Table of Contents
Community Health Needs Assessment for Corning Hospital: Schuyler, NY and Steuben, NY: November 2012 Approved February 20, 2013 One Guthrie Square Sayre, PA 18840 www.guthrie.org Page 1 of 18 Table of Contents
Driving the value of health care through integration. Kaiser Permanente All Rights Reserved.
 Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Mental Health Screening in Pediatric Primary Care: Results from a Quality Improvement Learning Collaborative
 Leandra Godoy, PhD, Melissa Long, MD, Tamara John Li, MPH, Mark Weissman, MD, Lee Savio Beers, MD April 1, 2016 Society for Behavioral Medicine Mental Health Screening in Pediatric Primary Care: Results
Leandra Godoy, PhD, Melissa Long, MD, Tamara John Li, MPH, Mark Weissman, MD, Lee Savio Beers, MD April 1, 2016 Society for Behavioral Medicine Mental Health Screening in Pediatric Primary Care: Results
Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP)
") Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP) 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois
Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP) 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois