A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
|
|
|
- William Gaines
- 5 years ago
- Views:
Transcription
1 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management Henry Chung, MD Chief Medical Officer, Montefiore Care Management Anne Meara, RN, MBA Associate Vice President, Montefiore Care Management Herb Fillmore Vice President, Strategic Innovation, Treo Solutions
2 Presentation Outline The Bronx Collaborative Description of the Care Transitions Program Predictive Model Evaluation Findings Lessons Learned Discussion Please note that the views expressed by the conference speakers do not necessarily reflect the views of the American Hospital Association and Health Forum. 2

3 The Bronx 1.4 million residents in the poorest urban county in the nation 30% live at or below the poverty line 12.5% unemployment rate 89% non-white minority 43% of children are at or below poverty 54% Hispanic, 37% African-American High burden of chronic disease 12% have diabetes 30% are obese 16% have asthma Per capita health expenditures 22% higher than national average 80% of health care costs paid for by government payers 3
4 What is the Bronx Collaborative? Incorporated as a New York State not-for-profit in 2009 with goal of improving health care delivery in the Bronx 3 major delivery systems Bronx Lebanon Hospital Center 593 beds, 29,000 admits/yr. Montefiore Medical Center 1,491 beds, 90,000 admits/yr. St. Barnabas Hospital 461 beds, 21,000 admits/yr. 2 major payers EmblemHealth Healthfirst Each of the 5 participating entities has equal representation on the Board of Directors Covers 16% of the county s population or 220,000 Bronx residents with Medicaid, Medicare and commercial insurance Accounts for 27% of Medicare managed care and 22% of Medicaid managed care markets in the Bronx 4
5 Why focus on care transitions? Potential win-win for providers and payers Program targets health plan members that hospitals are at risk for Medicare and Medicaid readmission penalties Research suggests readmissions can be reduced by addressing problems during transitions of care 5
6 Unique Features of the Collaborative s program Active participation of payers Program conducted across multiple hospitals RHIO used to establish electronic care transition record, facilitate data exchange/reporting and support program uniformity Using predictive model to target high-risk cases Focus on 60-day readmissions vs. 30-day More clinically diverse and socially disadvantaged population than most other programs 6
7 Care Transitions Program Financing Hospitals Facility-based staff Supervision, office space, equipment Payers One-time fee for cases with interventions Care transition home visits New York Community Trust Collaborative formation New York State Health Foundation Program design Electronic Care Transitions Record and RHIO costs Staff training Montefiore Care Management Project management Evaluation 7
8 Care Transitions Program Design Built on evidence-based models including: Project Red, BOOST, Coleman and Naylor Developed by team from all 5 partners IRB-approved design Standardized training Centralized project oversight and coordination Shared data collection system in RHIO Centralized evaluation resources 8
9 Eligible Population Bronx residents aged 50 and older Medicare, Medicaid and Commercial members of the 2 health plans English- or Spanish-speaking (patient or caregiver) with a telephone Admitted to Medicine Service and expected to be discharged home (not SNF) Excludes: HIV/AIDS, transplant, dialysis, psych, substance abuse, homeless, elective admits, and cognitively-impaired patients without an active caregiver 9
10 Staffing Operational Components 1 RN Care Transition Manager and.5-time Care Transition Analyst in 4 hospitals Shared Pharmacist Centralized Program Coordinator Reimbursement by payers Personal Discharge Record Predictive model Program and RHIO consents for all patients 10
 provides education on red flags, Rx review,")

")

 =")
11 Program Overview STEP 1 STEP 2 STEP 3 STEP 4 STEP 5 STEP 6 Care Transition Manager (CTM) provides education on red flags, Rx review, postdischarge MD visit, contact info hours CTM follows up on red flags, Rx reconciliation, referral to Pharmacist if needed, reinforce need for MD visit, address questions Care Transition Pharmacist does Rx reconciliation, resolves RX issues (only for those referred by the CTM) 7-14 days CTM checks on MD visit w/in 14 days and checks for problems, assists in resolving open issues days CTM follows up on any remaining issues, transitions to care management if needed Home care RN does transition home visit (only for those readmitted within 60 days) = Qualifying Interventions 11
12 12 Here s the problem
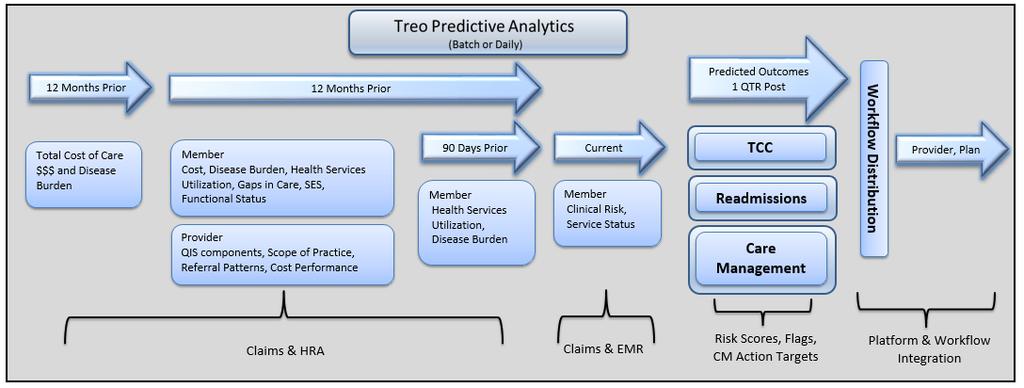
13 Treo Readmission Prediction Tool (RPT) Problem : Limited resources for care management Need to target patients most in need at a time of greatest vulnerability Solution: Prioritize new admissions for intensive care management interventions by Predicting probability of readmission on the morning after an admission using a small set of readily available administrative variables 13
14 RPT Applications Each morning a list of new admissions with key historical variables is automatically transmitted to Treo electronically RPT scores are applied, the list is ranked by priority and placed on a secure site for case manager retrieval Case managers retrieve list and begin working with those having highest priority of readmission 14
15 Readmission Prediction Tool (RPT) Raw data elements, before enrichment Discharges in last 12 months, Length of Stay of last previous admission, Readmissions in last 12 months, Health status and disease severity, Age, Gender, Race, Zip Code, Payer All of the above variables predate the current admission and are facility-specific Original training data set based on census of New York State, followed by census of Bronx discharges in Validation data set from census of Bronx discharges in
16 Why These Variables & Not Others These are the variables that are reliably available the day after admission. Other variables like diagnosis of current admission, source of admission, length of stay of current admission, EMR data, and patient social characteristics might improve the model. Even without additional variables, the current model s statistical performance is about 40% better than flipping a coin. (Validation C=.67) This performance is better than many disease-specific models with many times more variables requiring extensive data collection. 16
17 Other Predictive Models Most focus on specific diseases. Many do not report validation statistics Some mix readmission with mortality Some have no exceptions for trauma or metastatic malignancies or other conditions that would be expected to have readmissions Many rely on expensive non-administrative data 17

 has a C of")
18 The C The C-statistic (area under a ROC curve) measures the test s ability to discriminate between those who will be admitted from those who will not. A useless test (no better than flipping a coin) has a C 0.5. A perfect test (zero false positives and zero false negatives) has a C of
19 Other Models Model Year DepVar Admin C statistic data Only? LACE (Walraven) day death or unplanned No.684 (V) readmission Felker et al day death or all cause No.69 (NV) readmission among HF patients Yamokoski et al day all cause No.60 (NV) readmission among HF patients Kroch et al 2010 All cause 30 day No.682 CMS All cause 30 day readmission HF, heart attack, pneumonia PARR (Billings) 2006 All cause 365 day readmission Kansagara (Meta Review) JAMA October models. Most common depvar was 30 day.63 Yes *.685(V) Mixed * Inpt & Otpt

20 20 Here s the problem
21 21 Next Generation

22 Program Population 775 Selected using predictive model 190 Comparison Group 585 Intervention Group Qualifying Interventions 85 1 Qualifying Intervention 22
23 Population Profile--1 Descriptor Intervention (n=585) Comparison (n=190) Patients with previous admission (at index CTP hospital) 44% 51% Mean predictive score Mean age % Males 33.7% 30.0% Race - Black 32.9% 31.6% - Hispanic 46.5% 57.4% - White 6.8% 6.3% - Other/Missing 13.8% 4.7% Spanish speaking 33.5% 43.7% 23
24 Population Profile--2 Descriptor Intervention (n=585) Comparison (n=190) Line of business - Medicare 64.4% 59.5% - Medicaid 23.8% 32.6% - Commercial 11.8% 7.9% Index hospital - Bronx Lebanon 10.6% 24.2% - Moses (Montefiore) 34.4% 24.2% - St. Barnabas 11.8% 26.8% - Weiler (Montefiore) 43.2% 24.7% Average index LOS
25 Evaluation Methods Multivariate logistic regression to evaluate impact of the program on 60- day readmissions for all program participants (n = 585) Evaluated 500 individuals who received minimum of two qualifying interventions Performed further review of the 85 patients who received only one intervention 25
26 Data for Program Evaluation Care Transitions Record in Bronx RHIO Claims data from payers Hospital EMRs Program staff interviews 26
27 Levels of Intervention (n=585) 0% 20% 40% 60% 80% 100% At least 1 qualifying intervention Post-discharge booklet At least one completed post-discharge call 100% 99% 93% Two completed calls 62% Pre-discharge education session with CTM Call from the pharmacist 38% 46% 3 or more post-discharge calls Care transitions home visit 11% 11% 27
28 Outcome Metrics Intervention Total (n=585) Intervention Subgroup with at least 2 interventions (n=500) Intervention Subgroup with 1 intervention (n=85) Comparison (n=190) 60-day readmissions 22.8% 17.6% 52.9% 26.3% 30-day readmissions 14.9% 9.4% 47.1% 17.9% % of patients with ED visit within 60-days % of patients with MD visit within 14 days 18.4% 19.1% 22.4% 18.4% 70.4% 74.4% 47.1% 61.1% Note: Comparison Group received usual care. 28
29 Key metric: 60-day readmit rate 22.8% readmit rate for total Intervention group is 21.4% lower than the baseline rate of 29% 13.3% lower than the Comparison group rate of 26.3% 17.6% readmit rate for those with 2 or more qualifying interventions is 39.3% lower than the baseline rate 33.0% lower than the Comparison group rate 52.9% readmit rate for those with only 1 qualifying intervention is 200% higher than the rate of those with 2 or more qualifying interventions 100% higher than the Comparison group rate 29
30 Variation in Program Groups 30 1 Intervention (n=85) Intervention (n=585) 2 or more Interventions (n=500) Comparison (n=190) Usual Care 60-day Readmissions 52.9% 17.6% 26.3% Mean (Median) # days to readmit 11.5 (5) 28.4 (28) 23.8 (19) Mean Index LOS Index AMA Discharge 5.9% 0.8% 2.6% Office Visit Within 14 Days of Admission Patients with Previous Admission (at same hospital) 47% 74% 61% 51.7% 43.2% 50.5% Charlson Score Mean Predictive Score 21.9% 21.4% 22.5% Pre-Discharge Contact 34.1% 51.2% Not applicable Post-Discharge Contact 45.9% 99.8% Not applicable







31 5 key factors that contribute to readmissions Medicare patient No follow-up physician office visit w/in 14 days < 2 qualifying interventions Charlson score > 2 Readmission Longer lengths of stay 31
32 Lessons Learned: Collaboration All Collaborative members consider the program a success Collaboration and competition can co-exist if incentives are appropriately aligned Value in obtaining input/perspective from multiple organizations in program design Opportunities exist to: Leverage resources among hospitals, e.g. training Leverage resources of health plan, e.g. streamline hand offs for longer term case management 32
33 Lessons Learned: RHIO Value in utilizing RHIO for information exchange Problems using the RHIO as the primary platform for the care transition program Duplicate data entry required into hospital system and RHIO Need a care planning system designed to: take data from multiple sources without separate data entry support workflows to alert appropriate staff as needed 33
34 Lessons Learned: Predictive Model Patients with a prior admission more likely to be readmitted Model limited by data available at point of admission from all hospitals Need to Refine Predictive Model with additional data elements Use predictive results to stratify population Consider using 1 model at admission; 1 at discharge 34
35 Lessons Learned: Care Transitions Program Effectiveness--1 Key program activities: MD office visit within 14 days of discharge Minimum of 2 qualifying interventions (contacts) Dedicated staff with comprehensive, standardized training and oversight is effective, but difficult to scale Need to enhance usual care in hospital and post-discharge to address program scalability Need to develop an equitable reimbursement methodology 35
36 Lessons Learned: Care Transitions Program Effectiveness--2 Current evidence-based practices fit most, but not all, patients Very high readmit rates for those with only 1 qualifying intervention Staff feedback suggests psychosocial differences account for higher readmission rates Neither claims data nor medical record reviews explain high readmit rate for those with only 1 intervention Need to continue to explore causes of readmit rate variation to develop strategy for proactive identification of higher risk group and then identify appropriate interventions 36


37 Factors Affecting Readmission Clinical/ Health System Lack of timely follow up care (primary, specialty, testing, home care) Insufficient patient education on medication, signs and symptoms, Patient co-morbidities and severity of illness Stage of patient s primary disease Polypharmacy, medication adherence/ compliance Readmission Psychosocial Patient s insurance Homeless, unstably housed Transportation problems Lack of involved care giver Health literacy Financial barriers Language / cultural barriers Care giving responsibilities Self-perception of health Stress Depression Cognitive impairment Substance abuse 37


38 Accountability for Preventing Readmissions Accountable Care Community Patient/ Caregiver Hospital PCP/ Specialist Health System Health Plan Prevent Readmissions 38
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Examples of Measure Selection Criteria From Six Different Programs
 Examples of Measure Selection Criteria From Six Different Programs NQF Criteria to Assess Measures for Endorsement 1. Important to measure and report to keep focus on priority areas, where the evidence
Examples of Measure Selection Criteria From Six Different Programs NQF Criteria to Assess Measures for Endorsement 1. Important to measure and report to keep focus on priority areas, where the evidence
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care
 Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
The Memphis Model: CHN as Community Investment
 The Memphis Model: CHN as Community Investment Health Services Learning Group Loma Linda Regional Meeting June 28, 2012 Teresa Cutts, Ph.D. Director of Research for Innovation cutts02@gmail.com, 901.516.0593
The Memphis Model: CHN as Community Investment Health Services Learning Group Loma Linda Regional Meeting June 28, 2012 Teresa Cutts, Ph.D. Director of Research for Innovation cutts02@gmail.com, 901.516.0593
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes. James X. Zhang, PhD, MS The University of Chicago
 Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
Quality of Care of Medicare- Medicaid Dual Eligibles with Diabetes James X. Zhang, PhD, MS The University of Chicago April 23, 2013 Outline Background Medicare Dual eligibles Diabetes mellitus Quality
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Transitions of Care: An opportunity to improve care, experience and reduce waste
 Transitions of Care: An opportunity to improve care, experience and reduce waste Dr. Paresh Dawda, Visiting Fellow, Australian Primary Health Care Research Institute, ANU Adjunct Associate Professor, University
Transitions of Care: An opportunity to improve care, experience and reduce waste Dr. Paresh Dawda, Visiting Fellow, Australian Primary Health Care Research Institute, ANU Adjunct Associate Professor, University
From Risk Scores to Impactability Scores:
 From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
From Risk Scores to Impactability Scores: Innovations in Care Management Carlos T. Jackson, Ph.D. September 14, 2015 Outline Population Health What is Impactability? Complex Care Management Transitional
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Program Development. Completion of Gap Analysis. Review of Data. Multi-disciplinary team
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
I. Coordinating Quality Strategies Across Managed Care Plans
 Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Jennifer Kent Director California Department of Health Care Services 1501 Capitol Avenue Sacramento, CA 95814 SUBJECT: California Department of Health Care Services Medi-Cal Managed Care Quality Strategy
Adopting a Care Coordination Strategy
 Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Kristen Miranda Vice President Strategic Partnerships and Innovation March 20, 2013
 california case study: a model for accountable care Kristen Miranda Vice President Strategic Partnerships and Innovation March 20, 2013 1 program framework and core tenets To achieve measurable results,
california case study: a model for accountable care Kristen Miranda Vice President Strategic Partnerships and Innovation March 20, 2013 1 program framework and core tenets To achieve measurable results,
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
CMS Proposed Payment Rule FY Cheryl Phillips, MD Evvie Munley
 CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
Preventable Readmissions
 Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
MEDICAL RESPITE IN NEW YORK CITY
 MEDICAL RESPITE IN NEW YORK CITY ROSA M. Gil, DSW Founder, President & CEO Comunilife, Inc. 14th Annual New York State Supportive Housing Conference June 5, 2014 INTRODUCTION National attention is increasingly
MEDICAL RESPITE IN NEW YORK CITY ROSA M. Gil, DSW Founder, President & CEO Comunilife, Inc. 14th Annual New York State Supportive Housing Conference June 5, 2014 INTRODUCTION National attention is increasingly
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
RE-ADMITTING IN HOSPITALS: MODELS AND CHALLENGES. Murali Parthasarathy Dr. Paul Damien
 RE-ADMITTING IN HOSPITALS: MODELS AND CHALLENGES Murali Parthasarathy Dr. Paul Damien April 11, 2014 1 Major pain points Hospitals scored on five major pain points 1. Death rates among heart and surgery
RE-ADMITTING IN HOSPITALS: MODELS AND CHALLENGES Murali Parthasarathy Dr. Paul Damien April 11, 2014 1 Major pain points Hospitals scored on five major pain points 1. Death rates among heart and surgery
Passport Advantage Provider Manual Section 10.0 Care Management
 Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management Page 1 of 9 10.0
Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management Page 1 of 9 10.0
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care
 Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
REPORT OF THE BOARD OF TRUSTEES
 REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
Risk Adjustment for Socioeconomic Status or Other Sociodemographic Factors
 Risk Adjustment for Socioeconomic Status or Other Sociodemographic Factors TECHNICAL REPORT July 2, 2014 Contents EXECUTIVE SUMMARY... iii Introduction... iii Core Principles... iii Recommendations...
Risk Adjustment for Socioeconomic Status or Other Sociodemographic Factors TECHNICAL REPORT July 2, 2014 Contents EXECUTIVE SUMMARY... iii Introduction... iii Core Principles... iii Recommendations...
State FY2013 Hospital Pay-for-Performance (P4P) Guide
 Guide") State FY2013 Hospital Pay-for-Performance (P4P) Guide Table of Contents 1. Overview...2 2. Measures...2 3. SFY 2013 Timeline...2 4. Methodology...2 5. Data submission and validation...2 6. Communication,
State FY2013 Hospital Pay-for-Performance (P4P) Guide Table of Contents 1. Overview...2 2. Measures...2 3. SFY 2013 Timeline...2 4. Methodology...2 5. Data submission and validation...2 6. Communication,
Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage
 Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage American Public Health Association Monday, October 29, 2012: 10:30 AM-12:00 PM Kevin Hawkins, PhD
Evaluation of a High Risk Case Management Pilot Program for Medicare Beneficiaries with Medigap Coverage American Public Health Association Monday, October 29, 2012: 10:30 AM-12:00 PM Kevin Hawkins, PhD
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Organization. Hospital to SNF Communication. Care Coordination Goals. Chasing the Perfect Handoff The Missing Link to Interoperability 7/18/2016
 Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Essentia Health. A View on Information Technology. ND HIMS Conference April 12, Tim Sayler, COO Essentia Health - West
 Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling. Speaker: Thomas Martin November 2014
 Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs. Laura J. Dunlap, RN
 William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs Laura J. Dunlap, RN Background Research Questions Methods Results for North Carolina Results for Specific Counties
William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs Laura J. Dunlap, RN Background Research Questions Methods Results for North Carolina Results for Specific Counties
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Webinar. Reducing Readmissions with BI and Analytics. 23 March 2018 Copyright 2016 AAJ Technologies All rights reserved.
 Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
Webinar Reducing Readmissions with BI and Analytics Copyright Reducing 2016 Readmissions AAJ Technologies with BI and All rights Analytics reserved. www.aajtech.com Hospital Readmissions Michele Russell,
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
A Call to Action: Readmission Strategies from the Field
 A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
Minority Serving Hospitals and Cancer Surgery Readmissions: A Reason for Concern
 Minority Serving Hospitals and Cancer Surgery : A Reason for Concern Young Hong, Chaoyi Zheng, Russell C. Langan, Elizabeth Hechenbleikner, Erin C. Hall, Nawar M. Shara, Lynt B. Johnson, Waddah B. Al-Refaie
Minority Serving Hospitals and Cancer Surgery : A Reason for Concern Young Hong, Chaoyi Zheng, Russell C. Langan, Elizabeth Hechenbleikner, Erin C. Hall, Nawar M. Shara, Lynt B. Johnson, Waddah B. Al-Refaie
The Drive Towards Value Based Care
 The Drive Towards Value Based Care Thursday, March 3, 2016 Michael Aratow, MD, FACEP Chief Medical Information Officer, San Mateo Medical Center Gaurav Nagrath, MBA, Sr. Strategist, Population Health Research
The Drive Towards Value Based Care Thursday, March 3, 2016 Michael Aratow, MD, FACEP Chief Medical Information Officer, San Mateo Medical Center Gaurav Nagrath, MBA, Sr. Strategist, Population Health Research
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Disease Management at Anthem West Or: what have we learned in trying to design these programs?
 Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis
Disease Management at Anthem West Or: what have we learned in trying to design these programs? Lisa M. Latts, MD, MSPH Regional Medical Director May 12, 2003 Anthem Inc. Anthem Inc. Headquarters: Indianapolis