Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases?
|
|
|
- Della Dickerson
- 6 years ago
- Views:
Transcription
1
2
3 Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases? Providing care for long-term cancer survivors? Managing depression? Treating substance abuse?
4 A. The US doesn t spend enough on health care. B. Doctors don t know these are problems that should be addressed. C. Competing demands make it impossible to do everything. D. Practices are designed for care of acute problems and single chronic diseases. E. The United States doesn t address the underlying determinants of health.
5 In late January 2015, Tom s father was diagnosed with Acute Myelogenous Leukemia. This was quite a shock as his father had been walking nearly eight miles a day through the end of 2014 and had otherwise been very healthy. As a result of his diagnosis, Tom s father was hospitalized for a couple of weeks and is now completing his second round of chemotherapy.
6 What struck Tom as he sat in his father s hospital room the first week after he was diagnosed was how little choice his dad was given in his treatment. He particularly noted the nurses and oncologists being clear that they would be meeting without his dad to determine the best course of treatment and they would let him know how they would proceed. A couple of years previously, before his role as Executive Director of NAPCRG, it may have been reassuring or comforting that the doctors were handling things on behalf of his dad. But now, he was actually quite shocked by their complete lack of consideration for what his dad might actually want in terms of his treatment.
7 After spending the better part of the past two years working alongside Jack Westfall, MD to create and manage the Patient and Clinician Engagement initiative that PCORI has generously funded - it was like a light went off in my brain and now I can t shut it off. My observations of my dad s care do not square with the values we are working to achieve in valuing and respecting the patient first and foremost. I suddenly had a very real and deep appreciation for our work and I m grateful for it.


8 Adult population at risk Adults reporting one or more illnesses or injuries per month Adults consulting a physician one or more times per month Adult patients admitted per month Adapted from Adult patients referred to another physician per month Adult patients referred to a university medical center per month
9 Helen slumps in the corner of the exam room. Dr. Jones, a family doctor, enters for his 10 minute visit. Dr. Jones looks at Helen and asks, How many seizures are you having? This is the 12th visit in 2 years with multiple providers for this 46 year old woman with chronic problems of abdominal complaints, seizures, hypertension, type 2 diabetes, and depression. How can Dr. Jones meet the patientcentered needs of Helen? 9

10


11 Barbara Starfield s international comparisons of primary care and the lag by US IOM Chasm Report of 2001 finds huge quality gaps Future of Family Medicine Report of 2004 proposes major practice redesign NCQA, ACA, Meaningful Use and a whole host of disruptions!
12 Chronic Care Model Resources and Policies Community Health System Health Care Organization Community and Practice Resources Self- Management Support Delivery System Design Decision Support Clinical Information Systems Informed, Activated Patient Productive Interactions Prepared, Proactive Practice Team Improved Outcomes 12
13 ACO & PCMH Corporate, Retail Employed Practices Small Independent Practices Small Independent Practices
14 2000 Keystone III Conference Family Medicine recognition that the health care system is in serious trouble, commissioned study in Future of Family Medicine Report New Model of practice and recommended proof of concept demonstration project in typical family practices 2006 AAFP creates TransforMED and begins NDP 36 family medicine practices randomized to two arms to implement NDP Model with independent evaluation
15
16 2007 Joint Principles of a Patient Centered Medical Home AAFP, ACP, AAP and AOA release consensus statement 2007 NCQA announces Physician Practice Connections A program with criteria that medical practices should meet to be recognized as medical homes 2008 Primary Care Patient-Centered Collaborative Announces16 significant state-level or multi-payer medical home demonstration projects are underway.





17 Access and communication Patient tracking and registries Care management Patient self-management support Electronic prescribing Test tracking Referral tracking Performance reporting and improvement Advanced electronic communications
 take off 2011 NCQA Updates Recognition")

18 2010 ACA in March 2010 creates integrated delivery systems platforms with PCMH often a major part Accountable Care Organizations (ACOs) take off 2011 NCQA Updates Recognition Criteria New NCQA criteria are announced with the PCMH Survey tool. This was updated again in Struggles continue to define ACOs and the role of the PCMH and primary care within ACOs


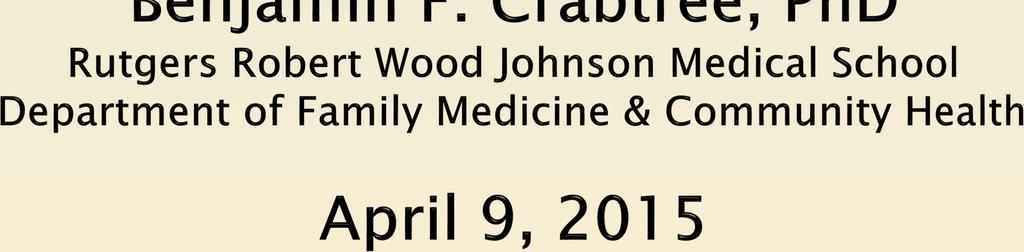
19 Patient Centered Medical Home
20 Team of people embedded in a community seeking to improve health and healing in that community & consisting of: Fundamental tenets of primary care First contact access Comprehensiveness Integration / coordination Relationships involving sustained partnership New ways of organizing practice Development of practice internal capabilities Health care delivery system & payment changes

21
22
23 Vermont Blueprint for Health created Community Health Teams to work with primary care providers to assess patients needs, coordinate support services, and provide multidisciplinary care. Web-based central health registry of patient data. State support for practice facilitators to work with primary care practices to obtain NCQA PCMH Recognition.

24 Service Practice Patient Disease Cost

25
26 Virginia Mason Bainbridge Island adopted Toyota Lean and taught this to all leaders and many staff. Using their existing personnel, they created teams of 2 physicians, one mid level, 1 RN, and 2 MA s, with all teams sharing a clinical pharmacist. Joint workspaces created for MA s/clinicians, with nurses located. Created Flow Stations by up-skilling traditional MA roles and creating partnerships of a clinicians and MA s who always worked together. MA called flow manager and manages the flow of patients and all the paperwork. Pharmacy and Care manager are available if needed to keep things flowing. All work is finished by end of the day.


27 Service Practice Patient Disease Cost

28
29 Lehigh Family Medical Associates combined elements of Virginia Mason and the Vermont Blueprint. Created Community Health Teams to work with primary care providers to assess patients needs, coordinate support services, and provide multidisciplinary care. Using their existing personnel, they created teams of physicians, mid-levels, RN s, and MA s who also work together.


30 Service Practice Patient Disease Cost


31
32 Southcentral Foundation is an Alaska Nativeowned, nonprofit health care organization run by a community board Primary care provider and teams include: One or two medical assistants Full-time nurse care coordinator Administrative assistant for case management support Members added or subtracted needs change: Pharmacists Nurse midwives Chiropractors Other specialists Reduced urgent care and ER utilization by 50%, hospital admissions by 53%, and specialist use by 65% while rising to the 75-90th percentile on most HEDIS outcome and quality measures.

33 Service Practice Patient Disease Cost


34
35

36

37 NCQA Recognition Accountable Care Organizations Meaningful Use Pay for performance on disease outcomes Employer mandates


38 46% Use of information technology 14% Care for 3 specific chronic diseases 13% Systems for coordinating care 9% Processes for accessibility 5% Performance reporting 4% Tools for organizing clinical data 2% Use of non-physician staff 2% Collection of data on patient experience 1% Preventive service delivery 1% Continuity of care 1% Patient communication preferences O'Malley AS, Peikes D, Ginsburg PB. Qualifying a Physician Practice as a Medical Home Policy Perspective: Insights into Health Policy Issues. No. 1 December, Available at:
39 Network of doctors and hospitals that share financial and medical responsibility for providing coordinated care. Since January 2013, nearly 200 new public and private ACOs have been formed: Medicare Shared Savings Program (MSSP) Accountable Care Organizations Medicaid Accountable Care Organizations Integrated Delivery Systems Multispecialty Group Practice (usually don t own the health plan, but contract with multiple plans) Independent Practice Associations Drastic shift away from private independent practices to affiliated and owned practices
40 Implement drug-drug and drug-allergy interaction checks Maintain up-to-date problem list of current and active diagnoses Generate and transmit permissible prescriptions electronically Maintain active medication list Record demographics and vital signs Implement clinical decision support rule for high clinical priority and track compliance Patients can view online, download, and transmit information Provide clinical summaries for patients for each office visit

41 Focus on technology for information management and control Diseases controlled care and not necessarily patient-centered care Focus on corporate mandates
42


43

44 Crabtree BF, Nutting PA, Miller WL, McDaniel RR, Stange KC, Jaen CR, Stewart EE. Primary care practice transformation is hard work: Insights from a 15 year developmental program of research. Medical Care, 49(Dec Suppl): S28-35, 2011.
45 Observation DOPC Direct Observation of Primary Care ( ) NCI R01 P&CD Prevention & Competing Demands in Primary Care ( ) AHRQ R01 IMPACT Insights from Multimethod Practice Assessment of Change over Time ( ) NCI R01 Intervention STEP-UP Study To Enhance Prevention by Understanding Practice ( ) NCI R01 ULTRA Using Learning Teams for Reflective Adaptation ( ) NHLBI R01 SCOPE Supporting Colorectal Outcomes through Participatory Enhancements ( ) NCI R01
46 Follow-up Baseline Motivation of key stakeholders Motivation, Innovation & Independence Resources & Capability for change External contingencies & capability to change Co-evolution & response to interventions Evaluating & exercising choices for change Outside Motivators External influences on change option landscape Choices for Change Cohen D, et al. A practice change model for quality improvement in primary care practice. J Healthcare Management, 49(3):155-68,
47 Observation DOPC Direct Observation of Primary Care ( ) NCI R01 P&CD Prevention & Competing Demands in Primary Care ( ) AHRQ R01 IMPACT Insights from Multimethod Practice Assessment of Change over Time ( ) NDP NCI R01 National Demonstration Project ( ) Intervention STEP-UP Study To Enhance Prevention by Understanding Practice ( ) NCI R01 ULTRA Using Learning Teams for Reflective Adaptation ( ) NHLBI R01 SCOPE Supporting Colorectal Outcomes through Participatory Enhancements ( ) NCI R01
48 Practices are complex systems Change is HARD RELATIONSHIPS matter LEADERSHIP is key PERSONAL transformation is needed There is no such thing as Plug n Play The promise of the patient-centered medical home remains elusive AND, the healthcare world is rapidly changing and our thinking needs to extend beyond the individual practice.
49


50
51 Does community ownership change the model? What is the impact of hierarchical corporate governance? What is the appropriate corporate scale? (local, regional, national) What kind of ACO can be family and patientcentered? (physician led, hospital led, community led) What is a Patient-Centered Health Care Neighborhood?
52 Current physicians (and others) must transform themselves. Future professionals need to learn the basics of leadership, teamwork, and organizational behavior. New professional roles need to be conceptualized and programs created to train for the future. Cultures of teamwork and collaboration need to be established within and across primary care and specialty practices, as well as throughout the neighborhood.




53 We need new comprehensive study designs Scammon D, et al. Connecting the Dots and Merging Meaning: Using Mixed Methods to Study Primary Care Deliver Transformation. Health Services Research, 2013; 48(6 Pt2):
54



55
Culture Change. Bryan J. Weiner, Ph.D.
 Culture Change Bryan J. Weiner, Ph.D. bjweiner@uw.edu WHAT IS ORGANIZATIONAL CULTURE? The way things are done around here. WHAT KIND OF CULTURE SUPPORTS PERFORMANCE IMPROVEMENT? Learning Organization:
Culture Change Bryan J. Weiner, Ph.D. bjweiner@uw.edu WHAT IS ORGANIZATIONAL CULTURE? The way things are done around here. WHAT KIND OF CULTURE SUPPORTS PERFORMANCE IMPROVEMENT? Learning Organization:
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient Centered Medical Home Foundation for Accountable Care
 Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
Patient Centered Medical Home Foundation for Accountable Care Outline of Presentation History and tenants of the patient-centered care and PCMH model Defining, measuring, recognizing, and evaluating the
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs
 The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
The Patient Centered Medical Home Guidelines: A Tool to Compare National Programs Medical Group Management Association (MGMA ) publications are intended to provide current and accurate information and
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
The Patient Centered Medical Home: 2011 Status and Needs Study
 The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
The Patient Centered Medical Home: 2011 Status and Needs Study Reestablishing Primary Care in an Evolving Healthcare Marketplace REPORT COVER (This is the cover page so we need to use the cover Debbie
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE
 THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin
 Johann Chanin") Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
Physician Practice Connections Patient-Centered Medical Home (PPC-PCMH ) Johann Chanin Colorado Patient-Centered Medical Home Demonstration Project Meeting January 15, 008 Today NCQA quality measurement
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Keith Salzman, M.D. Chief Medical Information Officer, IBM
 Keith Salzman, M.D. Chief Medical Information Officer, IBM Smarter Care through Transformation Keith L Salzman, MD, MPH CMIO-IBM GBS Federal keithsal@us.ibm.com USA 2012 Ogden UT IOM-The Healthcare Imperative:
Keith Salzman, M.D. Chief Medical Information Officer, IBM Smarter Care through Transformation Keith L Salzman, MD, MPH CMIO-IBM GBS Federal keithsal@us.ibm.com USA 2012 Ogden UT IOM-The Healthcare Imperative:
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group
 Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group Describe the main characteristics of a PCMH Analyze potential benefits of becoming a PCMH Examine the criteria
Gonzalo Paz-Soldán, MD, FAAP, CPE Executive Medical Director - Pediatrics Reliant Medical Group Describe the main characteristics of a PCMH Analyze potential benefits of becoming a PCMH Examine the criteria
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Blueprint For Success: The Patient Centered Medical Home
 Blueprint For Success: The Patient Centered Medical Home Kay Lynn Olmsted, DNP, FNP-BC Assistant Professor, University of South Alabama Donna Hodnicki, PhD, FNP-BC, FAAN Professor Emeritus, Georgia Southern
Blueprint For Success: The Patient Centered Medical Home Kay Lynn Olmsted, DNP, FNP-BC Assistant Professor, University of South Alabama Donna Hodnicki, PhD, FNP-BC, FAAN Professor Emeritus, Georgia Southern
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP)
 & Patient-Centered Specialty Practice (PCSP)") Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
Patient-Centered Medical Home (PCMH) & Patient-Centered Specialty Practice (PCSP) Foundation for a Better Health Care System Presenter Jeanette Ikan, M.D., MHAI Objectives: Definition and benefits of PCMH,
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Medical Home Summit September 20, 2011
 Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
Medical Home Summit September 20, 2011 1 Three Dimensions of Value by Institute of Healthcare Improvement Population Health Experience of Care Per Capita Cost Care Management : The unintended consequences
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
How Title Xx Vermont s Broadening
 How Title Xx Vermont s Broadening Subtitle Xx APCD Offers New Opportunities to Drive Value & Efficiencies Adam Moody, Director of Analytic Operations Onpoint Health Data Pat Jones, Assistant Director Presenter,
How Title Xx Vermont s Broadening Subtitle Xx APCD Offers New Opportunities to Drive Value & Efficiencies Adam Moody, Director of Analytic Operations Onpoint Health Data Pat Jones, Assistant Director Presenter,
Integrating Population Health into Delivery System Reform
 Integrating Population Health into Delivery System Reform Population Health Roundtable IOM Jim Hester Washington DC June 13, 2013 Theme The health care system is transitioning from payment rewarding volume
Integrating Population Health into Delivery System Reform Population Health Roundtable IOM Jim Hester Washington DC June 13, 2013 Theme The health care system is transitioning from payment rewarding volume
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Agenda. NE CAH Region Discussion
 NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
What is Mental Health Integration?
 What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
Sustaining a Patient Centered Medical Home Program
 Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Sustaining a Patient Centered Medical Home Program Partners Healthcare, Center for Population Health Colleen Blanchette Keri Sperry Terry Wilson-Malam Learning Objectives After this presentation, you will
Kaiser Permanente QUALITY OVERVIEW OVERALL RATING : 3.4 COMPANY AT A GLANCE. Company Statistics. Accreditation Exchange Product
 QUALITY OVERVIEW Permanente As the state s largest nonprofit health plan, Permanente is committed to improving the health of our members and our state as a whole. Permanente is made up of: Foundation Hospitals
QUALITY OVERVIEW Permanente As the state s largest nonprofit health plan, Permanente is committed to improving the health of our members and our state as a whole. Permanente is made up of: Foundation Hospitals
Health Reform and Medicare: What Does it Mean for a Restructured Delivery System?
 Health Reform and Medicare: What Does it Mean for a Restructured Delivery System? Gary S. Kaplan, MD Chairman and CEO Virginia Mason Medical Center May 25, 2011 Our Strategic Plan Virginia Mason Medical
Health Reform and Medicare: What Does it Mean for a Restructured Delivery System? Gary S. Kaplan, MD Chairman and CEO Virginia Mason Medical Center May 25, 2011 Our Strategic Plan Virginia Mason Medical
PCMH 2014 Record Review Workbook (RRWB)
") PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
Essentia Health. A View on Information Technology. ND HIMS Conference April 12, Tim Sayler, COO Essentia Health - West
 Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Managing Population Health in Northeast Georgia: One Medical Group's Experience
 September 21, 2013 Managing Population Health in Northeast Georgia: One Medical Group's Experience By Mark Hagland Northeast Georgia Physicians Group (NGPG), based in Gainesville, Georgia, a suburb of
September 21, 2013 Managing Population Health in Northeast Georgia: One Medical Group's Experience By Mark Hagland Northeast Georgia Physicians Group (NGPG), based in Gainesville, Georgia, a suburb of
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Benefits are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
Patient-centered care - from buzz word to meaningful reality. Current Health Care System
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care
 Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Strategies to Support the Integration of Behavioral Health and Primary Care: What Have We Learned Thus Far?
 COMMENTARY Strategies to Support the Integration of Behavioral Health and Primary Care: What Have We Learned Thus Far? W. Perry Dickinson, MD The articles in this supplement contain a wealth of practical
COMMENTARY Strategies to Support the Integration of Behavioral Health and Primary Care: What Have We Learned Thus Far? W. Perry Dickinson, MD The articles in this supplement contain a wealth of practical
Models of Accountable Care
 Models of Accountable Care Medical Home, Episodes and ACOs Making it work Elliott Fisher, MD, MPH Director, Population Health and Policy The Dartmouth Institute for Health Policy and Clinical Practice
Models of Accountable Care Medical Home, Episodes and ACOs Making it work Elliott Fisher, MD, MPH Director, Population Health and Policy The Dartmouth Institute for Health Policy and Clinical Practice
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
NCQA WHITE PAPER. NCQA Accreditation of Accountable Care Organizations. Better Quality. Lower Cost. Coordinated Care
 NCQA Accreditation of Accountable Care Organizations Better Quality. Lower Cost. Coordinated Care. NCQA WHITE PAPER NCQA Accreditation of Accountable Care Organizations Accountable Care Organizations (ACO)
NCQA Accreditation of Accountable Care Organizations Better Quality. Lower Cost. Coordinated Care. NCQA WHITE PAPER NCQA Accreditation of Accountable Care Organizations Accountable Care Organizations (ACO)
Collaboration between Medical Homes and Urgent Care Clinics
 Collaboration between Medical Homes and Urgent Care Clinics 03.24.15 THE VISION Our company vision is to have a world in which: CITYMD MAKES EVERYONE BETTER. TODAY AND TOMORROW. EVERYWHERE. Patients Providers
Collaboration between Medical Homes and Urgent Care Clinics 03.24.15 THE VISION Our company vision is to have a world in which: CITYMD MAKES EVERYONE BETTER. TODAY AND TOMORROW. EVERYWHERE. Patients Providers
Requirements Document for the Blue Quality Physician Program sm Criteria Effective 08/03/2015
 All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
Draft Covered California Delivery Reform Contract Provisions Comments Welcome and Encouraged
 TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
New Models of Care- Looking at PCMH & Telehealth
 New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
New Models of Care- Looking at PCMH & Telehealth Paula Block, RN, BSN, Clinical Process Improvement Manager Montana Primary Care Association pblock@mtpca.org or 406.442.2750, ext. 1003 Agenda What is PCMH?
meaningful reality Katie Coleman, MSPH
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
Building the Oncology Medical Home. Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc.
 Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
Building the Oncology Medical Home Susan Tofani, MS, Director Network and Payer Relations, Oncology Management Services, Inc. Quality, Performance Improvement, Certification / Recognition Keep the doors
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH
 What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure
 The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure Marci Nielsen, PhD, MPH Executive Director Amy Gibson, MS, RN Chief Operating Officer Patient-Centered
The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure Marci Nielsen, PhD, MPH Executive Director Amy Gibson, MS, RN Chief Operating Officer Patient-Centered
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Models for Patient-centered Cancer Care
 Models for Patient-centered Cancer Care Ed Wagner, MD, MPH Cancer Research Network CRN Cancer Communication Research Center Supported by: Division of Cancer Control and Population Sciences, NCI Four Perspectives
Models for Patient-centered Cancer Care Ed Wagner, MD, MPH Cancer Research Network CRN Cancer Communication Research Center Supported by: Division of Cancer Control and Population Sciences, NCI Four Perspectives
Where Do We Go From Here? The Value of Sustaining Practice Transformation
 Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
Where Do We Go From Here? The Value of Sustaining Practice Transformation MASSACHUSETTS LEAGUE OF COMMUNITY HEALTH CENTERS ANNUAL CLINICAL CONFERENCE November 19, 2013 Nicole Van Borkulo, MEd Senior Consultant
Hudson Headwaters Journey to Patient Centered Medical Home Recognition
 Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
Hudson Headwaters Journey to Patient Centered Medical Home Recognition Cyndi Nassivera-Cordes, VP Clinical Quality February 9, 2012 R4 1 Initial Steps Identify PCMH Project Leader Educate Yourself Determine
2018 SUMMARY OF BENEFITS
 2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Group Medicare Advantage (PPO) H2001-827 Group Name: North Carolina State Health Plan for Teachers and State Employees Group Numbers: 12309,
2018 SUMMARY OF BENEFITS Overview of your plan UnitedHealthcare Group Medicare Advantage (PPO) H2001-827 Group Name: North Carolina State Health Plan for Teachers and State Employees Group Numbers: 12309,
Shana Scott, JD, MPH, Health Systems Team Lead Tuesday, October 3, 2017
 Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Connecticut SIM: Enabling Accountable Care and Accountable Communities
 Connecticut SIM: Enabling Accountable Care and Accountable Communities SIM SYMPOSIUM FROM ACCOUNTABLE CARE TO ACCOUNTABLE COMMUNITIES: HOW CONNECTICUT S STATE INNOVATION MODEL INITIATIVE IS DRIVING REFORM
Connecticut SIM: Enabling Accountable Care and Accountable Communities SIM SYMPOSIUM FROM ACCOUNTABLE CARE TO ACCOUNTABLE COMMUNITIES: HOW CONNECTICUT S STATE INNOVATION MODEL INITIATIVE IS DRIVING REFORM
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination
 Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Anthem BlueCross and BlueShield HMO
 Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: NCQA (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product
Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: NCQA (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product
MAKING PROGRESS, SEEING RESULTS
 MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
MAKING PROGRESS, SEEING RESULTS VALUE-BASED CARE REPORT HUMANA.COM/VALUEBASEDCARE Y0040_GCHK4DYEN 1117 Accepted 2 Americans are sick and getting sicker, with millions of us living with chronic conditions
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Alternative Payment Models- Recipes For Success
 Alternative Payment Models- Recipes For Success Elizabeth Lange, MD, PCMH-Kids Michael Magill, MD, Department of Family and Preventative Medicine-University of Utah Kevin Schendel, MD Timothy Willox, MD,
Alternative Payment Models- Recipes For Success Elizabeth Lange, MD, PCMH-Kids Michael Magill, MD, Department of Family and Preventative Medicine-University of Utah Kevin Schendel, MD Timothy Willox, MD,
Transforming to Value: One Way Forward
 Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
GUIDELINES FOR ADVERTISING AND MARKETING RECOGNITION PROGRAMS. Table of Contents
 GUIDELINES FOR ADVERTISING AND MARKETING RECOGNITION PROGRAMS Table of Contents INTRODUCTION 2 USE OF RECOGNITION SEALS 2 APPROVED QUOTE 6 RECOMMENDED LANGUAGE 7 PROGRAM-SPECIFIC INFORMATION 8 HEART/STROKE
GUIDELINES FOR ADVERTISING AND MARKETING RECOGNITION PROGRAMS Table of Contents INTRODUCTION 2 USE OF RECOGNITION SEALS 2 APPROVED QUOTE 6 RECOMMENDED LANGUAGE 7 PROGRAM-SPECIFIC INFORMATION 8 HEART/STROKE
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition