Health Care Reform s BOOST to Reducing Readmissions
|
|
|
- Nancy Anderson
- 6 years ago
- Views:
Transcription

1 Health Care Reform s BOOST to Reducing Readmissions Mark V. Williams, MD, FHM Professor & Chief, Division of Hospital Medicine Principal Investigator, Project BOOST Why the Focus on Care Transitions? n Significant number of readmissions n 1 out of 5 Medicare patients, many preventable readmissions n Significant harm: n 1 out of 5 of patients have an Adverse Event after discharge n Regulatory Pressures n PPACA contains penalties for hospitals with excess readmissions 1

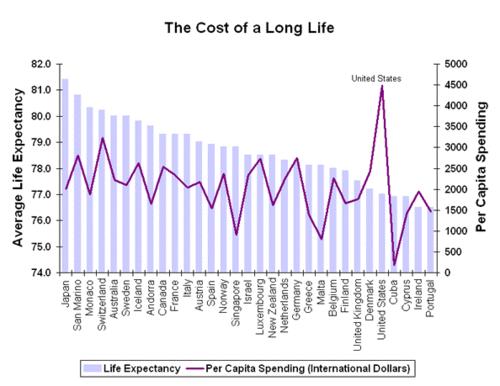
2 Objectives n Describe how we got here n Demonstrate variability in rates of rehospitalization n Outline key healthcare reform legislation components n Review options to BOOST the hospital discharge transition Health Care Costs Rising Faster than CPI 2


3 BIG piece of the $3.5 Trillion Government Pie Nation s Health Care Dollar 2010 n CMS - 48 cents of every dollar received by hospitals n 28 cents of every dollar spent on physicians services 3

4 4


5 June 2007 MedPAC Report n Medicare pays for ALL admissions regardless n Initial stay or readmission for same condition n 17.6% of admissions result in re-admissions within 30 days (6% in 7 days) n = $15 billion in spending n Future n Public Disclosure of readmission rates n Lower case payments for readmissions HospitalCompare.hhs.gov 5

6 1 in 5 Medicare patients rehospitalized in 30 days Half never saw outpatient doc 70% of surgical readmissions chronic medical conditions Costs $17.4 billion Rates of Rehospitalization within 30 Days after Hospital Discharge Jencks S, Williams MV, Coleman EA. N Engl J Med 2009;360:


7 Health Affairs 2010; 29:57-64 Harlan M. Krumholz, MD, SM research group n Observational study of 6,955,461 Medicare FFS hospitalizations for HF; 1993 and 2006, with 30-day f/u. n Mean age = 80 n 52% Htn, 38% DM, 37% COPD n LOS 8.8 days down to 6.3 n Discharges to SNF increased from 13% to 20% n Discharge to home decreased from 74% to 67% n 30 day readmission increased from 17.2% to 20.1% n Post-discharge mortality increased from 4.3% to 6.4% n In-hospital mortality declined from 8.5% to 4.3% n 30-day mortality declined from 12.8% to 10.7% 7
8 A Problem for a long time n Rosenthal, J. M. and D. B. Miller "Providers have failed to work for continuity." Hospitals 53(10): n Continuity of patient care between different health care settings has been advocated for nearly 20 years, but little has been done to affect it. The study described here emphasizes the current lack of effort by health care providers in hospitals and nursing homes to find a workable solution. Eric Coleman, MD, MPH n Director, Care Transitions Program University of Colorado Denver n Reducing readmissions jumps off the page as an area where we could see enormous savings in national health expenditures. n We re pretty good at identifying who s at risk of readmission, but it s harder to say who s at modifiable risk. 8
9 Reform It s here! n H.R. 3590, the Patient Protection and Affordable Care Act n H.R the Health Care and Education Reconciliation Act n Paying for quality instead of quantity n Demonstration projects Donald Berwick, MD, MPP Administrator for CMS n High quality health care does not necessarily mean the most expensive health care. n CMS aims to become a leader in health care improvement and reward delivery of value in health care. 9
10 Quality ver$us Quantity As Congress debates health care, some policy experts say no meaningful improvement can be made without changing the payment system so medical centers have more financial incentive to help people stay out of the hospital. Reducing Readmissions = Reducing Revenue? n Asthma Prevention Program at Children s Hospital of Boston n 62% reduction in ER visits n 82% reduction in hospitalizations n $1300 cost savings per child over 2 years n ROI of 1.46 n Savings to society and insurers n Hospital loses revenue and pays for program 10
11 Affordable Care Act and Reducing Readmissions KK 3025 Beginning in FY 2011 Community - Based Care Transitions Program For Period FY AHRQ funding for projects related to QI research and technical assistance. Topics identified include reducing readmissions. March 2012 Program for eligible hospitals to improve their readmission rates through Patient Safety Organizations Beginning in FY 2013 Hospitals with higher than expected readmissions rates will experience decreased payments for Medicare discharges Section 3025 of ACA n Hospital Readmissions Reduction Program Financial penalties on hospitals for excess readmissions vs. expected n All DRG payment amounts in hospitals with excess readmission are reduced by a factor determined by the level of excess, preventable readmissions n HF, AMI, Pneumonia; Effective FY2013 n Excess = ratio of actual to expected (risk-adj) n Reduction of up to 1%, 2%, 3% first 3 years n $7.1 billion in savings over 10 years 11
12 Hospital Discharge - currently Random events connected to highly variable actions with only a remote possibility of meeting implied expectations. Roger Resar, MD Agent of Tremendous Change and Global Innovation Seeker Luther Midelfort Mayo Health System Senior Fellow, IHI Dangers of Discharge 19% of patients had a post discharge AE - 1/3 preventable and 1/3 ameliorable Ann Intern Med 2003; Vol % of patients had a post discharge AE - 28% preventable and 22% ameliorable CMAJ 2004;170(3) 12
13 Dangers of Discharge n 1095 of 2644 (41%) inpatients discharged with test result pending n (9.4%) potentially required action n - Survey of MDs involved: almost 2/3 unaware of results n - Of these: 37% actionable and 13% urgent Ann Intern Med 2005;143(2):121-8 Dangers of Discharge Arch Intern Med. 2007;167: n ¼ of discharged patients require additional outpatient work-ups n > 1/3 not completed n Increased time to post-discharge f/u associated with lack of work-up completion n Availability of discharge summary increased likelihood of work-up being done 13

14 Medication Reconciliation JGIM 2010 n n n n 21 minute Pharmacist interviews 36% order errors n ½ required increased monitoring or intervention n 10% harmful 49% omission error, 30% wrong dose; 11% frequency Elderly and larger # of meds increased risk Medication List protective to avoid errors Hospitalist to PCP n Info transfer and communication deficits at hospital discharge are common n Direct communication 3-20% n Discharge summary availability at 1 st postdischarge appt 12-34%; 51-77% at 4 weeks n Discharge summaries often lack info n Dx test results (33-63%), hospital course (7-22%), discharge meds (2-40%), pending test results (65%) n Follow-up plans (2-43%), Counseling (90-92%) Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW JAMA 2007;297:


15 Discharge Summary J Gen Intern Med 2009;24: Discharge summaries are grossly inadequate at documenting both tests with pending results and appropriate f/u providers. Principles l Accountability l Responsibility l Coordination of Care l Family Involvement l Communication l Timeliness l National standards and metrics 15
16 Post discharge - follow-up by RN or MD l Naylor et al: RN visit post d/c for geriatric medical patients *decreased rehospitalizations* Ø 10% vs. 23% (p = 6 wks Ø N/S by 12 weeks l Anderson et al: MD visit post d/c for stroke decreased rehospitalizations Ø 26% vs. 6 months Who would pay for this? Ann Intern Med 1994;120(12): Stroke 2000;31: l Randomized 363 patients age > 65 l Comprehensive discharge planning and home follow-up with APNs l ~70% completion rate l Readmissions at 24 weeks 20% vs 37% Ø Reduced multiple readmissions 6.2% vs 14.5% Ø Prolonged time to first readmission Ø Medicare reimbursements cut in half 16
17 Arch Intern Med 2006;166: l Elderly patients transitioning to SNF/home l Randomized: Intervention group paired with Transition Coach vs. standard care l Empowerment and education: 4 pillars Ø Facilitate self management/adherence Ø Maintain a personal health record Ø Timely follow-up Ø Knowledge and management of complications l Education during hospitalization Ø including meds and med reconciliation l Phone calls and personal visits by TC post discharge l N=750 Arch Intern Med 2006;166: Results Rehospitalization Interv Cont P(adj) OR (95%CI) Within 30d ( ) Within 90d* ( ) Within 180d* ( ) *Also significantly improved for Rehospitalization for same diagnosis as index admission. Costs($) Interv Cont Unadj Log Transformed At 30d At 90d At 180d
:894-900 l Swedish ward-based pharmacists l")

18 Pharmacists Work! Arch Intern Med. 2009;169(9): l Swedish ward-based pharmacists l 16% reduction in hospital visits l 47% reduction in ER visits l Drug-related readmissions reduced 80% l Intervention group cost < control 18
19 Project RED l RCT of 749 hospitalized adults l Intervention Ø Nurse Discharge Advocate l F/U appt, Medication Reconciliation l Patient education Ø Individualized instruction booklet Ø Pharmacist call 2-4 days post-discharge l Review medications l Limitations Ø Urban, academic, safety net hospital Project RED Outcomes Intervention (n = 370) Control (n = 368) ER Visits* 16.5% 24.5% Rehospitalization** 15% 21% PCP f/u in 30 days* 62% 44% Prepared for Discharge* 65% 55% *p < 0.05 **p = 0.09 Mean age = 50 Mean LOS = 2.6 to 2.8 days Exclusions: Admitted from SNF Discharged to SNF 19


20 Low-cost Intervention JGIM 2008 l user-friendly Patient Discharge Form l Telephone outreach from a nurse postdischarge l Improved outpatient follow-up l Reduced ER visits and rehospitalizations from historical controls 1. Med Rec by PharmD 2. RN Care Coordinator D/C Planning 3. Phone Follow-up 4. PHR, Supplemental Discharge Form l Reduced ER visits, Reduced Readmission 20

21 Project BOOST Improving Hospital Care Transitions Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST Tina Budnitz, MPH Project Director, Project BOOST June 1, 2011 Project BOOST California HealthCare Foundation The John A. Hartford Foundation 21

22 Advisory Board Chair: Eric Coleman, MD, MPH Co-Chair & PI: Mark Williams, MD with organizational representatives from: Social work Case management Clinical pharmacy Geriatric medicine Geriatric nursing Health IT Blue Cross/Blue Shield United Health Health systems NQF AHRQ TJC CMS National Consumer s League Other content experts 22
23 Key Components BOOST Tools & Intervention Available for free at: Project Management tools Clinical Tools: Comprehensive risk assessment on admission 8Ps Risk specific interventions during stay & at discharge Patient centered discharge process Teachback, F/U appt scheduled prior to discharge Standardized PCP communication 72 hour follow-up call for high risk patients Mentored Implementation Longitudinal coaching throughout planning and implementation Ongoing educational opportunities BOOST Community/Collaborative TARGET Assessment Tool - The 8Ps Tool for Addressing Risk: a Geriatric Evaluation for Transitions TARGET Assessment Tool - The 8Ps Tool for Addressing Risk: a Geriatric Evaluation for Transitions Prior hospitalization Problem medications Psychological Principal diagnosis Polypharmacy Poor health literacy Patient support Palliative care Risk Specific Checklist GAP: General Assessment of Preparedness 23
24 The General Assessment of Preparedness: The GAP Caregivers and social support circle for patient Functional status evaluation completed Cognitive status assessed Abuse/neglect Substance abuse Advanced care planning addressed and documented On Admission Functional status Cognitive status Access to meds Responsible party for ensuring med adherence prepared Home preparation for patient s arrival Financial resources for care needs Transportation home Access (e.g. keys) to home Nearing Discharge l Understanding of dx, treatment, prognosis, followup and postdischarge warning S/S (using Teach Back) l Transportation to initial follow-up At Discharge 24
25 Discharge Patient Education Tool DIAGNOSIS I had to stay in the hospital because: The medical word for this condition is: I also have these medical conditions: TESTS DPET While I was in the hospital I had these tests: which showed: TREATMENT While I was in the hospital I was treated with: The purpose of this treatment was: FOLLOW-UP APPOINTMENTS After leaving the hospital, I will follow up with my doctors. (initials) Primary Care Doctor: Phone Number: DATE:,, 200 TIME: : m Specialist Doctor: Phone Number: DATE:,, 200 TIME: : m FOLLOW-UP TESTS After leaving the hospital, I will show up for my tests. (initials) LOCATION DATE TIME TESTS,, 200 : m Call your Primary Care Doctor for the following: Warning signs 1) 4) LIFE STYLE CHANGES After leaving the hospital, I will make these changes in my activity and diet. (initials) Activity:, because Diet:, because 25
26 Schillinger D et al. Closing the loop: physician communication... Arch Intern Med. 2003;163: Teach Back Life-Cycle Project BOOST Planning Training & Preparation Analyze processes Institutional Support Assemble Team Baseline Data 2 Day Training Intervention Toolkit Teach-back Training Peer-learning Project Planning Mentor reviewed action plan Implementation Redesign care processes Staff education Tailor tools Develop policies, procedures, order sets Evaluation Plan Individualized Mentoring Intervention Implement intervention Keep stakeholders informed Monitor core elements Surveillance Analyze data Adjust intervention components Report to stakeholders Spread gains Training 6-9 months 9-12 months 26
27 Mentored Implementation Secret Sauce for Project BOOST Target hospitalists at sites QI effector arm Mentor conference calls with hospital QI team follow-up Mentor experienced physician with QI expertise Beyond BOOST Some patients need more attention and support beyond the foundation provided by Project BOOST Frail elderly patients with multiple medical problems, multiple medications and potentially multiple social issues 27
28 References Balaban RB, Weissman JS, Samuel PA, Woolhander S. Redefining and redesigning hospital discharge to enhance patient care: a randomized controlled study. J Gen Intern Med 23(8): Coleman EA, Berenson RA. Lost in transition: challenges and opportunities for improving the quality of transitional care. Annals of Internal Medicine. Oct ;141(7): Coleman EA, Parry C, Chalmers S, Min S-J. The care transitions intervention: results of a randomized controlled trial. Archives of Internal Medicine. Sep ;166(17): Coleman EA, Smith JD, Raha D, Min S-j. Posthospital medication discrepancies: prevalence and contributing factors. Archives of Internal Medicine. Sep ;165(16): Dedhia P, Kravet S, Bulger J, Hinson T, Sriharan A, Kolodner K, Wright S, Howell E. A quality improvement intervention to facilitate the transition of older adults from three hospitals back to their homes. J Am Geriatr Soc 2009;57: Forster A, Clark H, Menard A, et al. Adverse events among medical patients after discharge from hospital. CMAJ. 2004;170: Forster A, Murff H, Peterson J, Gandhi T, Bates D. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(161-7). Forster AJ. Can you prevent adverse drug events after hospital discharge? CMAJ Canadian Medical Association Journal. Mar ;174(7): Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital.[see comment]. Annals of Internal Medicine. Feb ;138(3): Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients--development of a discharge checklist for hospitalists. Journal of Hospital Medicine. Nov 2006;1(6): References Jack BW, Chetty VK, Anthony D, Greenwald JL, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med 2009:150: Koehler BE, Richter KM, Youngblood L, Cohen BA, Prengler ID, Cheng D, Masica AL. Reduction of 30-day postdischarge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. JHM Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. Feb ;297(8): Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies: Volume 7 Care Coordination, Structured Abstract. Publication No. 04(07) , June Agency for Healthcare Research and Quality, Rockville, MD. Manning DM, Tammel KJ, Blegen RN, et al. In-room display of day and time patient is anticipated to leave hospital: a "discharge appointment". Journal of Hospital Medicine. Jan 2007;2(1): Moore C, McGinn T, Halm E. Tying up loose ends: discharging patients with unresolved medical issues. Arch Intern Med. 2007;167: Pantilat SZ, Lindenauer PK, Katz PP, Wachter RM. Primary care physician attitudes regarding communication with hospitalists. American Journal of Medicine. 2001;111 (9B):15S-20S. 28
29 References Parry C, Kramer HM, Coleman EA. A qualitative exploration of a patient-centered coaching intervention to improve care transitions in chronically ill older adults. Home Health Care Services Quarterly. 2006;25(3-4): Poon E, Gandhi T, Sequist T, Murff H, Karson A, Bates D. "I wish I had seen this test result earlier!": dissatisfaction with test result management systems in primary care. Archives of Internal Medicine. 2004;164: Roy C, Poon E, Karson A, et al. Patient safety concerns arising from test results that return after hospital discharge. Annals of Internal Medicine. 2005;143: Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Archives of Internal Medicine. Mar ;166(5): Shepperd S, Parkes J, McClaren J, Phillips C. Discharge planning from hospital to home.[update of Cochrane Database Syst Rev. 2000;(4):CD000313; PMID: ]. Cochrane Database of Systematic Reviews. 2004(1):CD van Walraven C, Mamdani M, Fang J, Austin P. Continuity of care and patient outcomes after hospital discharge. Journal of General Internal Medicine. 2004;19: Weiss ME, Piacentine LB, Lokken L, et al. Perceived readiness for hospital discharge in adult medical-surgical patients. Clinical Nurse Specialist. Jan-Feb 2007;21(1):
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
IMPROVING INPATIENT TO OUTPATIENT TRANSITION FOR GENERAL MEDICINE CLINIC PATIENTS
 IMPROVING INPATIENT TO OUTPATIENT TRANSITION FOR GENERAL MEDICINE CLINIC PATIENTS JULIE GILBREATH, MD, FACP; RAMON GALLEGOS, RN; PATRICIA REYES 8/2016-1/2017 1 THE TEAM CSE Participants: Julie Gilbreath,
IMPROVING INPATIENT TO OUTPATIENT TRANSITION FOR GENERAL MEDICINE CLINIC PATIENTS JULIE GILBREATH, MD, FACP; RAMON GALLEGOS, RN; PATRICIA REYES 8/2016-1/2017 1 THE TEAM CSE Participants: Julie Gilbreath,
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Adverse Drug Events and Readmissions: The Global Picture
 Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE. Measure Information Form
 Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Set: CMS Readmission Measures Set Measure ID #: READM-30-HWR Measure Information Form Performance Measure Name:
Last Updated: Version 4.3 NQF-ENDORSED VOLUNTARY CONSENSUS STANDARD FOR HOSPITAL CARE Measure Set: CMS Readmission Measures Set Measure ID #: READM-30-HWR Measure Information Form Performance Measure Name:
Poor admission medication reconciliation can follow
 Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
FREQUENTLY ASKED QUESTIONS (FAQs)
") FREQUENTLY ASKED QUESTIONS (FAQs) 2013 Voluntary Hospital Public Reporting of PCI Readmission Rationale for the Percutaneous Coronary Intervention (PCI) Readmission Measure... 3 1. Why measure readmissions
FREQUENTLY ASKED QUESTIONS (FAQs) 2013 Voluntary Hospital Public Reporting of PCI Readmission Rationale for the Percutaneous Coronary Intervention (PCI) Readmission Measure... 3 1. Why measure readmissions
Pharmacists Role in Care Transitions
 Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Heart Failure Nurse Practitioner Role Development and Proposal. Anita M. Wilson, BSN, RN. ACNP, DNP Student Creighton University
 1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Transitions of Care Project BOOST
 Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility
 Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility Cynthia Williams, B.S.Pharm, FASHP Vice President/Chief Pharmacy Officer Riverside Health System, Newport
Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility Cynthia Williams, B.S.Pharm, FASHP Vice President/Chief Pharmacy Officer Riverside Health System, Newport
Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan
 Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan July 2015 Inpatient hospitalizations account for 32 percent of the total $2.9 trillion spent on health care in the
Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan July 2015 Inpatient hospitalizations account for 32 percent of the total $2.9 trillion spent on health care in the
Version 1.0 (posted Aug ) Aaron L. Leppin. Background. Introduction
 Aaron L. Leppin. Background. Introduction") Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
Evidence Summary for the Care Transitions Program
 Social Programs That Work Review Evidence Summary for the Care Transitions Program HIGHLIGHTS: PROGRAM: The Care Transitions Program is a low-cost hospital discharge planning and home follow-up program
Social Programs That Work Review Evidence Summary for the Care Transitions Program HIGHLIGHTS: PROGRAM: The Care Transitions Program is a low-cost hospital discharge planning and home follow-up program
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Key Words: Transitions of care, care coordination, medication management, drug therapy problem
 Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
De.3 If included in a composite, please identify the composite measure (title and NQF number if endorsed):
:") NATIONAL QUALITY FORUM Measure Submission and Evaluation Worksheet 5.0 This form contains the information submitted by measure developers/stewards, organized according to NQF s measure evaluation criteria
NATIONAL QUALITY FORUM Measure Submission and Evaluation Worksheet 5.0 This form contains the information submitted by measure developers/stewards, organized according to NQF s measure evaluation criteria
How to Improve the Discharge Process. Michelle Mourad, MD Ryan Greysen, MD
 How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP
 Can Nurse Staffing Levels Improve Hospital Readmissions Performance? By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP Presentation Outline Overview of Readmissions Reduction Program Study Significance
Can Nurse Staffing Levels Improve Hospital Readmissions Performance? By Julie Berez Mentor: Matthew McHugh PhD JD, MPH, RN, CRNP Presentation Outline Overview of Readmissions Reduction Program Study Significance
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6,
 Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6, 2009 Conference Purpose The purpose of the conference
Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6, 2009 Conference Purpose The purpose of the conference
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Accepted Manuscript. Hospitalists, Medical Education, and US Health Care Costs,
 Accepted Manuscript Hospitalists, Medical Education, and US Health Care Costs, James E. Dalen MD, MPH, ScD (hon), Kenneth J Ryan MD, Anna L Waterbrook MD, Joseph S Alpert MD PII: S0002-9343(18)30503-5
Accepted Manuscript Hospitalists, Medical Education, and US Health Care Costs, James E. Dalen MD, MPH, ScD (hon), Kenneth J Ryan MD, Anna L Waterbrook MD, Joseph S Alpert MD PII: S0002-9343(18)30503-5
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE. By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012
 PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
REPORT OF THE COUNCIL ON MEDICAL SERVICE
 REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
Project Boost implementation guide
 Project Boost implementation guide Second Edition Editors: Chase Coffey, MD, MS Jeff Greenwald, MD, SFHM Tina Budnitz, MPH Mark V. Williams, MD, FACP, MHM Copyright 2013 by Society of Hospital Medicine.
Project Boost implementation guide Second Edition Editors: Chase Coffey, MD, MS Jeff Greenwald, MD, SFHM Tina Budnitz, MPH Mark V. Williams, MD, FACP, MHM Copyright 2013 by Society of Hospital Medicine.
Improving Care Transitions: Creating Your Evidence-Based Approach
 Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD
 Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Follow-up Telephone Contact following Discharge from Long-Term Acute Care Hospitals
 Eastern Kentucky University Encompass Doctor of Nursing Practice Capstone Projects Baccalaureate and Graduate Nursing 2016 Follow-up Telephone Contact following Discharge from Long-Term Acute Care Hospitals
Eastern Kentucky University Encompass Doctor of Nursing Practice Capstone Projects Baccalaureate and Graduate Nursing 2016 Follow-up Telephone Contact following Discharge from Long-Term Acute Care Hospitals
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Marshall Digital Scholar. Marshall University. Brittany Snodgrass. Charles K. Babcock Marshall University,
 Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
MediServe. More than 25 Years Serving the Rehab and Respiratory Communities
 MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Healthy Hearts Northwest : A 2 x 2 Randomized Factorial Trial to Build Quality Improvement Capacity in Primary Care
 Healthy Hearts Northwest : A 2 x 2 Randomized Factorial Trial to Build Quality Improvement Capacity in Primary Care April 7, 2017 Michael Parchman, MD, MPH This project is supported by grant number R18HS023908
Healthy Hearts Northwest : A 2 x 2 Randomized Factorial Trial to Build Quality Improvement Capacity in Primary Care April 7, 2017 Michael Parchman, MD, MPH This project is supported by grant number R18HS023908
Click to edit Master title style
 Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Medication Reconciliation as a Patient Safety Practice During Transitions of Care
 Medication Reconciliation as a Patient Safety Practice During Transitions of Care Janice L. Kwan, MD, MPH, FRCPC Division of General Internal Medicine Mount Sinai Hospital, University of Toronto Recorded
Medication Reconciliation as a Patient Safety Practice During Transitions of Care Janice L. Kwan, MD, MPH, FRCPC Division of General Internal Medicine Mount Sinai Hospital, University of Toronto Recorded
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
A Structured Workshop to Improve the Quality of Resident Discharge Summaries
 A Structured Workshop to Improve the Quality of Resident Discharge Summaries Jaideep S. Talwalkar, MD Jason R. Ouellette, MD Shawnette Alston, MD Gregory K. Buller, MD Daniel Cottrell, MD Thomas Genese,
A Structured Workshop to Improve the Quality of Resident Discharge Summaries Jaideep S. Talwalkar, MD Jason R. Ouellette, MD Shawnette Alston, MD Gregory K. Buller, MD Daniel Cottrell, MD Thomas Genese,
Emerging Issues in Post Acute Care Trends
 Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Faculty Presenters. The Care Transitions Program. STAAR Initiative
 Session M13 These presenters have nothing to disclose 26th Annual National Forum on Quality Improvement in Health Care Minicourse: Reducing Avoidable Readmissions by Creating a More Patient-Centered Transition
Session M13 These presenters have nothing to disclose 26th Annual National Forum on Quality Improvement in Health Care Minicourse: Reducing Avoidable Readmissions by Creating a More Patient-Centered Transition
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Improving patient discharge process using electronic medication input tool and on-line guide to arranging follow-ups
 BMJ Quality Improvement Reports 2013; u756.w711 doi: 10.1136/bmjquality.u756.w711 Improving patient discharge process using electronic medication input tool and on-line guide to arranging follow-ups Rory
BMJ Quality Improvement Reports 2013; u756.w711 doi: 10.1136/bmjquality.u756.w711 Improving patient discharge process using electronic medication input tool and on-line guide to arranging follow-ups Rory
Medication Management: Is It in Your Toolbox?
 Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
Improving Transitional Care by Involving Family Caregivers: The TC-QuIC Collaborative
 Improving Transitional Care by Involving Family Caregivers: The TC-QuIC Collaborative Carol Levine Director, Families and Health Care Project United Hospital Fund N3C/New York Academy of Medicine American
Improving Transitional Care by Involving Family Caregivers: The TC-QuIC Collaborative Carol Levine Director, Families and Health Care Project United Hospital Fund N3C/New York Academy of Medicine American
The Hospital Discharge: A Review of a High Risk Care Transition With Highlights of a Reengineered Discharge Process
 ORIGINAL ARTICLE The Hospital Discharge: A Review of a High Risk Care Transition With Highlights of a Reengineered Discharge Process Jeffrey L. Greenwald, MD,* Charles R. Denham, MD,Þ and Brian W. Jack,
ORIGINAL ARTICLE The Hospital Discharge: A Review of a High Risk Care Transition With Highlights of a Reengineered Discharge Process Jeffrey L. Greenwald, MD,* Charles R. Denham, MD,Þ and Brian W. Jack,
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
SAFE PRACTICE 15: DISCHARGE SYSTEMS
 Safe Practices for Better Healthcare 2010 Update SAFE PRACTICE 15: DISCHARGE SYSTEMS The Objective Ensure that effective transfer of clinical information to the patient and ambulatory clinical providers
Safe Practices for Better Healthcare 2010 Update SAFE PRACTICE 15: DISCHARGE SYSTEMS The Objective Ensure that effective transfer of clinical information to the patient and ambulatory clinical providers
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: