How to Improve the Discharge Process. Michelle Mourad, MD Ryan Greysen, MD
|
|
|
- Antony Allen
- 6 years ago
- Views:
Transcription
1 How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD



2 Who are we? Why are we here?


3 I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like us are passionate about improving the discharge process.
4 Discharging patients: It s complicated
5 And lots of things can go wrong Med rec? Insurance check? RN transcribing error Poor health literacy Pending tests? No point of contact after discharge No appointment No PMD communication No D/c summary
6 Workshop goals and overview Part 1: tackling discharge issues (in a broken system) Part 2: Best practices around discharge Part 3: Making quality discharge a reality

7 You re right. I m smiling, but I m scared inside. Lets start with something Uh Michelle, simpler. this sounds pretty complicated. Are you sure we can improve this?
8 How to Draw a Pig? Michelle Mourad, MD Ryan Greysen, MD
9 Drawing a Pig 1) Draw the side profile of a pig, centered on the page. 2) Make sure the pig's head is facing left. 3) The pig should be drawn large enough so that a piece of it is in every box EXCEPT the top right. 4) You have 2 minutes to draw your pig. 5) Look up when you are done.
10 Compare pigs!


11 Lets try that again Look up when you are finished
12 Compare Pigs!
13 Third time is the charm! Look up when you are finished

14 Lessons from Pig #1: Left on your own, every pig (or discharge) is different. Sure, it s quick to draw your own pig, but guiding improvements is a challenge.

15 Lessons from Pig #2: It s hard to follow instructions when you don t know what your goal or end product is. It takes to much time and makes standardization hard.

16 Lessons from Pig #3: Knowing the end product helps in following directions and everyone produces consistent quality pigs!
17 Drawing a Pig = Discharging a Patient You can t expect everyone to automatically follow all best practices without cues Provide instructions, examples and make the process easier

18 FIX IT!!




19

20 Workshop goals and overview Part 1: What do we know about readmissions? Part 2: Best practices around Discharge Part 3: Making Best Practices a Reality
21 Break Out Session Your first task: What should be standard for every discharge? With your table make a 5-item checklist to standardize every discharge You have 20 minutes

22 What s on your list? 1. Evidence 2. Best practice 3. What we re doing at UCSF 4. What are you doing?

23 MEDICATION RECONCILIATION
24 Medication Reconciliation: Evidence 15-30% of patients have med discrepancies during hospitalization Age, high-risk meds, and polypharmacy are risk factors Patients with med discrepancies twice as likely to be readmitted Coleman EA, et al. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med Gleason KM, al. Results of the Medications at Transitions and Clinical Handoffs (MATCH)study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010
25 Medication Reconciliation: Best Practices Confirm admission med list with PCP or pill bottles if possible Discharge pharmacy consult for high-risk meds or polypharmcy Careful documentation of med reconciliation including stop meds in patient instructions and discharge summary Ensure access to meds at discharge

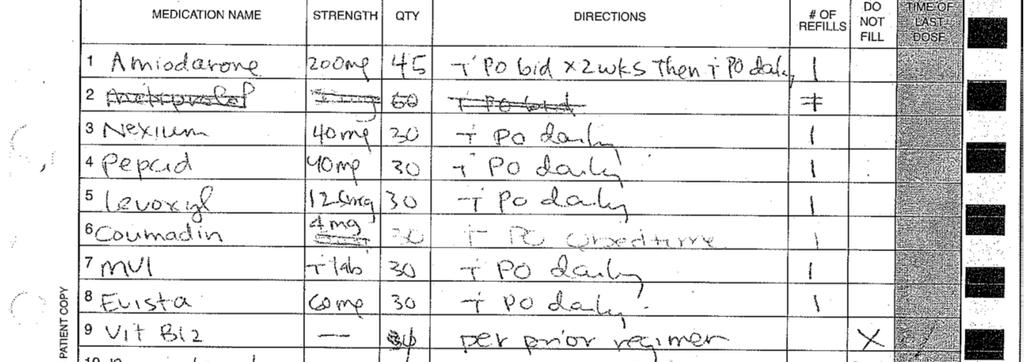
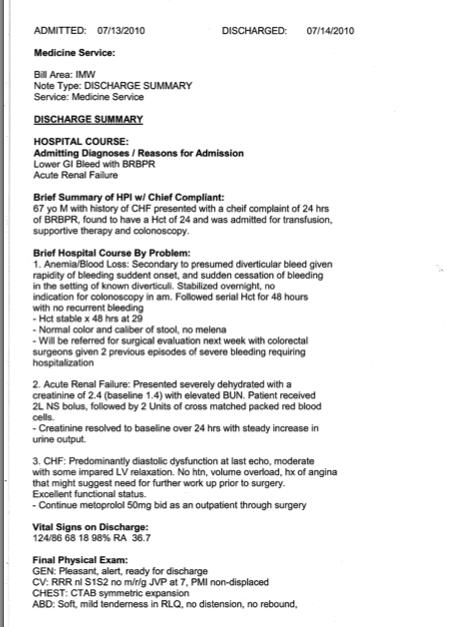
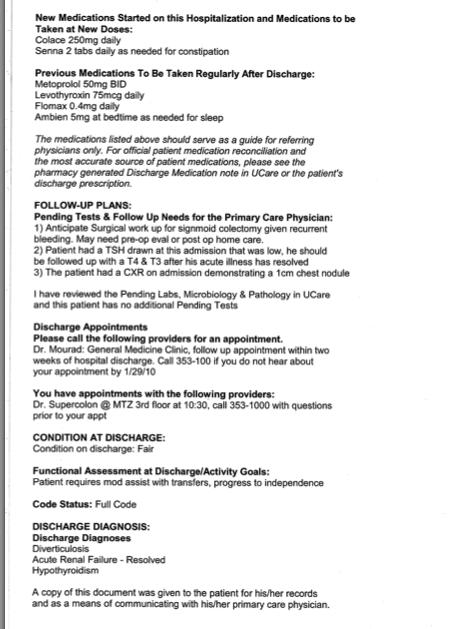
26 Do TRUE Medication reconciliation for Stopped, Started, Continued Medications in the Dishcarge Summary

27 MEDICATION TEACHING



28 Medication Teaching Evidence Multiple Articles cite improvements in when trained pharmacists do discharge teaching. Unfortunately Pharmacists are a limited resource at many institutions


29 Medication Teaching The Evidence High Risk meds are High risk!
30 High Risk Meds List PHARMACY CONSULT Anticoagulant medications (enoxaparin, coumadin, etc.) Any injected medication (insulin, enoxaparin, neupogen, epoetin, etc.) Changes to long-acting opiate regimens (fentanyl patch, MS Contin, Kadian, etc.) Antibiotics needing prior authorization (i.e. linezolid, cefpodoxime, PO vanco, etc.) Patients admitted with a drug related complication Any other questions, concerns, or special needs you may have for patients at discharge
31
32 Medication Education
33
34
35 PCP COMMUNICATION
36 PCP Communication Evidence 75% of discharge summaries NOT available at time of first follow-up appointment with PCP 24% caused limitations to PCP clinical plan One study found a trend to increased readmissions if a discharge summary was missing PCPs unaware of 62% of the pending test results after discharge 37% were considered actionable Kripilani et al, Journal of Hospital Medicine, 2007
37 PCP Communication Best Practice Make PCP info easy for inpatient providers to find Talk to your admissions department about automating communication on admission Involve PCPs early Consider setting the bar for the discharge summary within 24 hrs Communicate the discharge diagnosis, medications, results of procedures, pending test results, follow-up arrangements, and suggested next steps. Within 1 week, a detailed discharge summary should have been received.
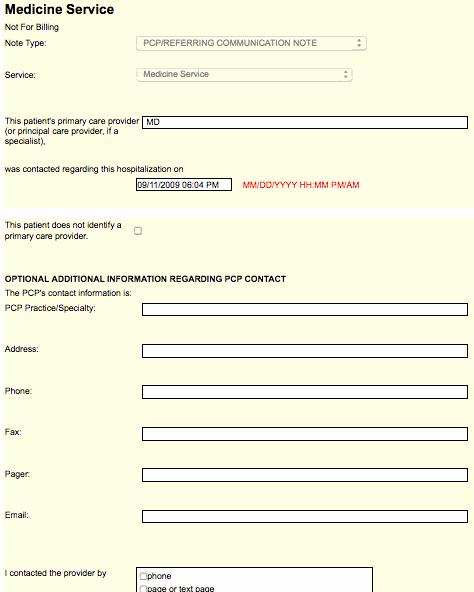
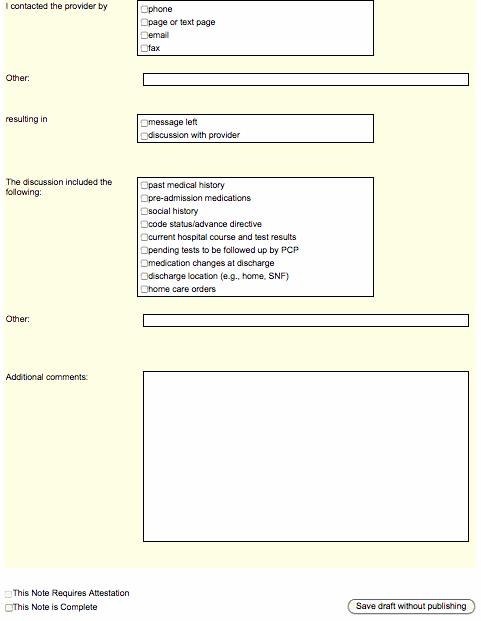
38 PCP Communication Note

39 Dictated discharge summaries
40 e-discharge summaries
41 Changing the culture Timely Discharge Summary Average days to completion % 80% 60% 40% 20% 0% Percent done on discharge Average Time to Intern Signature Completed by intern on the day of discharge


42 FOLLOW UP PLANS Wave goodbye!


43 Follow Up Appointments Evidence Evidence for two week follow up appointments
44 Follow Up Appointments Best Practice Follow up within 2 weeks from hospital discharge for General Medicine Follow up within 7 days for patients with CHF Follow up within 30 days for SNF patients Audit and feedback of appointment rates can change behavior: see if your EMR can track this! Consider follow-up phone calls by discharge coordinator (RN/NP role)
45 Follow up appointments Can we make a slide about our PCP follow up rates (as referenced in last slide can improve with audits/feedback!)

46 Follow Up with patients Creating a post-discharge hotline to the nurses station or an admin, can be a good first step to understand post discharge issues

47 Follow Up Phone Calls Some evidence these decrease readmissions Some evidence for increased patient satisfaction A good opportunity to check what patients understood from discharge instructions


48 Data from Follow Up Calls Able to fill all prescriptions 76% No new meds 11% No Insurance Financial Burden 13% Unable to fill some or all prescriptions 13% Drug Store issue (no stock, wrong meds,) 13% Patient awaiting Insurance approval 12% Patient had not attempted to fill prescription 42% Pharmacy closed at time of discharge - 6%

49 PATIENT EDUCATION

50 Patient Education Evidence Nurses spend an average of 8 minutes on discharge Less than half of patients understand their discharge diagnosis, medications, etc.
51 Patient Education Best Practice Reason for Admission Findings from Hospital Stay Discharge Diagnoses Instructions for Self-Care/Symptom Management at home Follow up Plans Pending test Use Teachback!
52 Teachback Explain discharge instructions to patient Assess Recall & Comprehension: Ask Patient to Demonstrate Reassess Recall & Comprehension: Ask patient to Demonstrate Clarify & Tailor the Instructions
53 Old Form
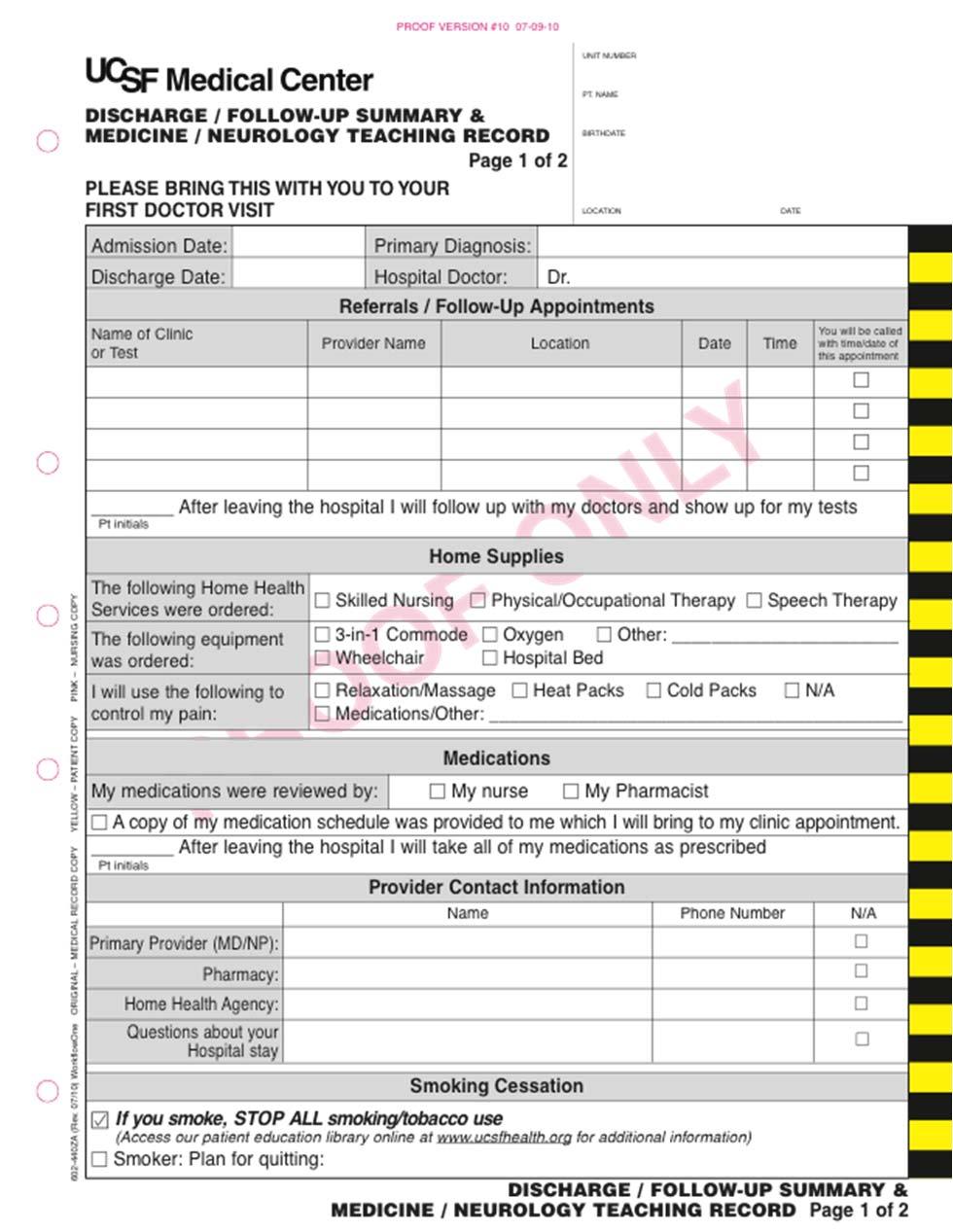
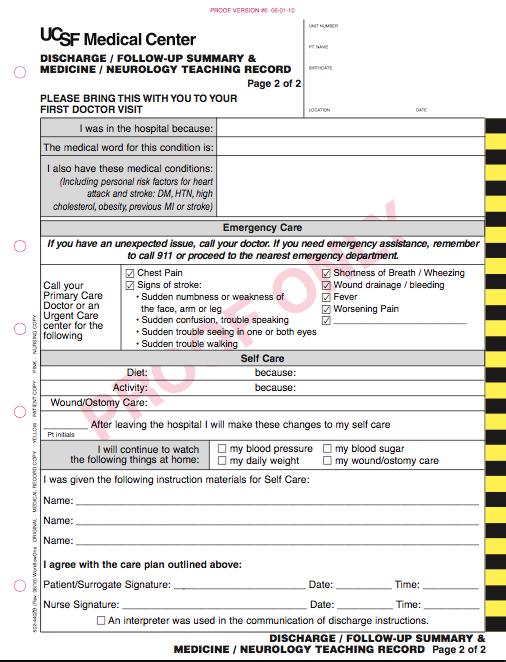
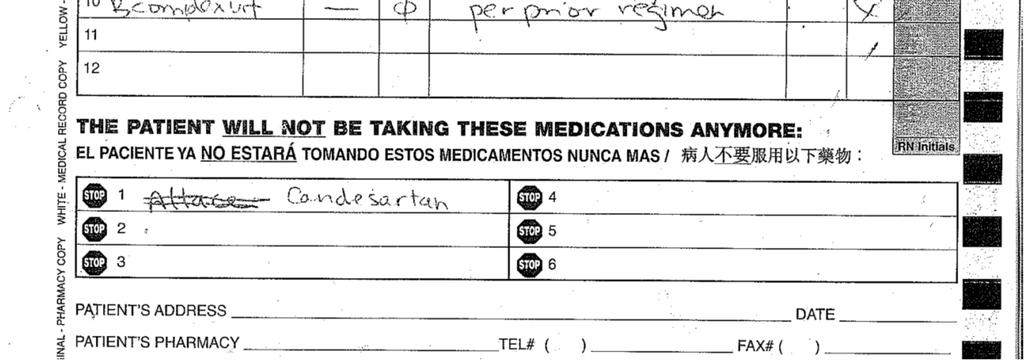
54 New Form

55 What do patients go home with? PATIENT BELONGINGS NAME: ROOM:
56

57 COMMUNICATION WITH NURSES Does this exist?
58 Communication with Nurses Evidence No studies on effects of MD-RN communication on quality of discharge or readmission BUT RNs more likely than MDs to cite poor communication as reason for delays in discharge 30% of observed hospitalists did not communicate with nurse verbally at all during admission MD-RN agreement on plans for medication changes was 59% overall Minicello, Auerback, Wachter. Caregiver Perceptions of the Reasons for Delayed Hospital Discharge. Effective Clinical Practice Rothberg et al. The Relationship Between Time Spent Communicating and Communication Outcomes on a Hospital Medicine Service. JGIM. 2011

59 Communication with Nurses Best Practice Discharge Time Out Discharge diagnosis Follow-up plans Need for education/training prior to discharge Necessary paperwork completed Anticipated time of discharge.
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Sample Communication Plan for a Hospitalist Program
 A P P E N D I X E Sample Communication Plan for a Hospitalist Program COMMUNICATION WITH PRIMARY CARE PHYSICIANS At Admission The emergency department (ED) physician speaks with the referring primary care
A P P E N D I X E Sample Communication Plan for a Hospitalist Program COMMUNICATION WITH PRIMARY CARE PHYSICIANS At Admission The emergency department (ED) physician speaks with the referring primary care
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility
 Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility Cynthia Williams, B.S.Pharm, FASHP Vice President/Chief Pharmacy Officer Riverside Health System, Newport
Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility Cynthia Williams, B.S.Pharm, FASHP Vice President/Chief Pharmacy Officer Riverside Health System, Newport
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Roundtable on Health Literacy Institute of Medicine 17 March 2014
 Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
Electronic Medication Reconciliation and Depart Process Overview Nursing Deck
 Electronic Medication Reconciliation and Depart Process Overview Nursing Deck Revised: 8/16/2011 1 Introduction To achieve the highest standard of care that our system aspires to, as well as to meet the
Electronic Medication Reconciliation and Depart Process Overview Nursing Deck Revised: 8/16/2011 1 Introduction To achieve the highest standard of care that our system aspires to, as well as to meet the
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
University of Michigan Health System Program and Operations Analysis. Analysis of Problem Summary List and Medication Reconciliation Final Report
 University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
University of Michigan Health System Program and Operations Analysis Analysis of Problem Summary List and Medication Reconciliation Final Report To: John Clark, PharmD, MS, University of Michigan Health
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Poor admission medication reconciliation can follow
 Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Master the Skills of Successful Patient Medication Education
 Master the Skills of Successful Patient Medication Education 0 1 Communication about Medication The Medication Education Imperative To deliver a World Class Patient Experience --- To Every Patient, Every
Master the Skills of Successful Patient Medication Education 0 1 Communication about Medication The Medication Education Imperative To deliver a World Class Patient Experience --- To Every Patient, Every
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Optimizing pharmaceutical care via Health Information Technology:
 Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Medication Reconciliation for Older Adults Transitioning from. Long-Term Care to Home. Allison (Leverett) Kackman
 Kackman") Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
Medication Reconciliation for Older Adults Transitioning from Long-Term Care to Home By Allison (Leverett) Kackman Washington State University Spokane. Riverpoint campus Ubrary P.O. Box 1495 Spokane, WA
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Objectives THE BASICS AND USING TECHNICIANS 3/22/2017
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Pharmacy Technicians: Improving Patient Care through Medication Reconciliation
 Pharmacy Technicians: Improving Patient Care through Medication Reconciliation Disclosure I, Holly Katayama, have no financial relationships to disclose. Objectives Describe how to fully utilize pharmacy
Pharmacy Technicians: Improving Patient Care through Medication Reconciliation Disclosure I, Holly Katayama, have no financial relationships to disclose. Objectives Describe how to fully utilize pharmacy
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Medication Reconciliation
 Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Society of General Internal Medicine May 7 th, 2011 Session G
 Society of General Internal Medicine May 7 th, 2011 Session G Introductions o Gregory M. Bump, MD bumpgm@upmc.edu o Caridad A. Hernandez, MD hernandezca@upmc.edu o Efren C. Manjarrez, MD Emanjarrez@med.miami.edu
Society of General Internal Medicine May 7 th, 2011 Session G Introductions o Gregory M. Bump, MD bumpgm@upmc.edu o Caridad A. Hernandez, MD hernandezca@upmc.edu o Efren C. Manjarrez, MD Emanjarrez@med.miami.edu
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
Transition of Care Model for Inpatient & Observation Units
 V.2 Transition of Care Model for Inpatient & Observation Units TRANSITION OF CARE PROGRAM FOR INPATIENTS & OBSERVATION UNITS (TOC) SCC PROJECT MANAGEMENT OFFICE TOC MODEL FOR INPATIENT & OBSERVATION UNITS
V.2 Transition of Care Model for Inpatient & Observation Units TRANSITION OF CARE PROGRAM FOR INPATIENTS & OBSERVATION UNITS (TOC) SCC PROJECT MANAGEMENT OFFICE TOC MODEL FOR INPATIENT & OBSERVATION UNITS
The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD
 The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD Presented by: Mary Jane Fellers, RN, BSN, MBA Senior Director, UM & Care Coordination OhioHealth Columbus, Ohio Replace text box
The Role & Challenges of Hospital Care Coordination in a POP HEALTH WORLD Presented by: Mary Jane Fellers, RN, BSN, MBA Senior Director, UM & Care Coordination OhioHealth Columbus, Ohio Replace text box
A Pharmacist Network for Integrated Medication Management in the Medical Home
 A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
Pharmacists Role in Care Transitions
 Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy
 Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
2017 Edition. MIPS Guide. The rule is in and Medicare physician payments are changing. What does that mean for you?
 2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Admission Medication History and Reconciliation Documentation. Froedtert Hospital, Milwaukee WI
 Overview of Medication History and Reconciliation Process 2 Overview of Icons Used in the Medication History 2 and Reconciliation Process The Admission Navigator 3 SureScripts Medication Reconciliation
Overview of Medication History and Reconciliation Process 2 Overview of Icons Used in the Medication History 2 and Reconciliation Process The Admission Navigator 3 SureScripts Medication Reconciliation
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
DUKE GENERAL MEDICINE SENIOR RESIDENT ORIENTATION
 Department of Medicine Hospital Medicine Program 2012-2013 DUKE GENERAL MEDICINE SENIOR RESIDENT ORIENTATION Your responsibilities and goals as the supervising resident on the Duke General Medicine Service
Department of Medicine Hospital Medicine Program 2012-2013 DUKE GENERAL MEDICINE SENIOR RESIDENT ORIENTATION Your responsibilities and goals as the supervising resident on the Duke General Medicine Service
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
A Stepwise Approach to Quality Improvement. Michelle Mourad, MD Director of Quality and Safety, Division of Hospital Medicine UCSF Medical Center
 A Stepwise Approach to Quality Improvement Michelle Mourad, MD Director of Quality and Safety, Division of Hospital Medicine UCSF Medical Center Why do we fail to do simple things that improve care? Hand
A Stepwise Approach to Quality Improvement Michelle Mourad, MD Director of Quality and Safety, Division of Hospital Medicine UCSF Medical Center Why do we fail to do simple things that improve care? Hand
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Transitions of Care: Vital to Quality Patient Care. Erica Shaver, MD WVU GME Orientation June 2017
 Transitions of Care: Vital to Quality Patient Care Erica Shaver, MD WVU GME Orientation June 2017 Goals of Session Define transition of care What makes for a good or bad handoff? ACGME expectations WVU
Transitions of Care: Vital to Quality Patient Care Erica Shaver, MD WVU GME Orientation June 2017 Goals of Session Define transition of care What makes for a good or bad handoff? ACGME expectations WVU
Readmission Reduction and the ACO
 Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
Key Words: Transitions of care, care coordination, medication management, drug therapy problem
 Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Admission from ED and PowerPlans (Order Sets)
") Admission from ED and PowerPlans (Order Sets) 7 17 12 Admission from the ED (Initiate PowerPlan) 1. Ensure patient is ready for Orders: i.e. In Virtual Bed (Loc: ED & a number) Ready Not Ready Must order
Admission from ED and PowerPlans (Order Sets) 7 17 12 Admission from the ED (Initiate PowerPlan) 1. Ensure patient is ready for Orders: i.e. In Virtual Bed (Loc: ED & a number) Ready Not Ready Must order
Preventing Avoidable Readmissions Together: Improving Discharge Summaries. R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC
 Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Preventing Avoidable Readmissions Together: Improving Discharge Summaries R. Neal Axon, MD, MSCR Assistant Professor of Medicine MUSC Today s Objectives Identify elements of a complete discharge summary
Adapting Practice to Keep Pace with Changes in Health Care. Change in Health Care. Professional Responsibilities?
 Accountable Care Innovations: Leading Medication Management Across the Continuum Adapting Practice to Keep Pace with Changes in Health Care Rick Couldry, M.S., FASHP University of Kansas Hospital Kansas
Accountable Care Innovations: Leading Medication Management Across the Continuum Adapting Practice to Keep Pace with Changes in Health Care Rick Couldry, M.S., FASHP University of Kansas Hospital Kansas
Reducing Hospital Re-Admissions with Telemedicine & Medication Reconciliation The prescription for improved patient outcomes
 Reducing Hospital Re-Admissions with Telemedicine & Medication Reconciliation The prescription for improved patient outcomes Download the presentation at RxConcile.com or asaging.org Who we are Chad Worz
Reducing Hospital Re-Admissions with Telemedicine & Medication Reconciliation The prescription for improved patient outcomes Download the presentation at RxConcile.com or asaging.org Who we are Chad Worz
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Introduction. Singapore and its Quality and Patient Safety Position. Singapore 2004: Top 5 Key Risk Factors. High Body Mass
 Introduction Singapore and its Quality and Patient Safety Position Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking (7.4%; 28,000)
Introduction Singapore and its Quality and Patient Safety Position Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking (7.4%; 28,000)
Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007
 Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007 Introduction During 2007, CT BHP partnered with family members and providers to address the
Treatment Improvement Initiative: Improved Planning for Youths being Discharged from Inpatient Care CT BHP 2007 Introduction During 2007, CT BHP partnered with family members and providers to address the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Marshall Digital Scholar. Marshall University. Brittany Snodgrass. Charles K. Babcock Marshall University,
 Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
Reducing Readmissions in Practice
 Reducing Readmissions in Practice Oregon Association of Hospitals and Health Systems Tualatin, Oregon Feb. 24, 2017 Matt Schreiber: Disclosures I am supported by Oregon State Hospital Association for my
Reducing Readmissions in Practice Oregon Association of Hospitals and Health Systems Tualatin, Oregon Feb. 24, 2017 Matt Schreiber: Disclosures I am supported by Oregon State Hospital Association for my
Pharmacy Medication Reconciliation Workflow Emergency Department
 Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
The Park at Allens Creek Suite Allens Creek Road Rochester, NY 14618
 The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
The Park at Allens Creek Suite 100 132 Allens Creek Road Rochester, NY 14618 Phone: (585) 473-7573 Fax: (585) 473-7641 www.mcms.org mcms@mcms.org Monroe County Medical Society Quality Collaborative Community
Patient and Family Caregiver Interview Tool
 Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Transition from Hospital to Home: Importance of Medication Education and Reconciliation
 Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
Question Patient #1 Patient #2 Patient #3 Patient #4 Patient #5 Number of days between the last discharge and this readmission date?
 Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Safe & Sound: How to Prevent Medication Mishaps. A Family Caregiver Healthcare Education Program. A Who What Where Why When Tool Kit
 Safe & Sound: How to Prevent Medication Mishaps A Family Caregiver Healthcare Education Program A Who What Where Why When Tool Kit National Family Caregivers Association www.thefamilycaregiver.org 800/896-3650
Safe & Sound: How to Prevent Medication Mishaps A Family Caregiver Healthcare Education Program A Who What Where Why When Tool Kit National Family Caregivers Association www.thefamilycaregiver.org 800/896-3650
Improving Sign-Outs in Hospital Medicine
 Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
Who s s on What? Latest Experience with the Framework Challenges and Successes. November 29, Margaret Colquhoun Project Leader ISMP Canada
 Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Medication Reconciliation - Inpatient
 Page 1 of 8 Home Previous Page Print Medication Reconciliation - Inpatient Administrative Policies & Procedures Document Number: MHC-ADMIN-02-1280 v6 Document Owner: Donna Ciufo, DNP, RN Date Last Updated:
Page 1 of 8 Home Previous Page Print Medication Reconciliation - Inpatient Administrative Policies & Procedures Document Number: MHC-ADMIN-02-1280 v6 Document Owner: Donna Ciufo, DNP, RN Date Last Updated: