Improving Care Transitions for Rhode Island Patients
|
|
|
- Linette Bryan
- 5 years ago
- Views:
Transcription

1 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator, Quality Partners of Rhode Island
2 Objectives Understand Care Transitions issue Consider the three readmission drivers Hear about the Rhode Island Safe Transitions Experience Learn about evidence-based interventions 2
3 Background Estimated $17 Billion in Medicare readmission 30-day FFS hospital readmission of 15-30% Several RCTs suggest that this can be reduced by 20-40% using various strategies Patient Activation Coleman: In-home coaching and phone f/u Jack: In-hospital computerized ed. and phone f/u Care management Naylor: Patient supported by transitional care nurse as primary care coordinator 3
4 Care Transitions Project Medicare-funded pilot 3 year pilot (09/08-08/11) Competitively funded 14 contracts nationwide Each based on various evidence-based research projects (independent approach) Cross-setting project Hospitals, home health, nursing homes, community physicians 4

5 Whatcom County, WA Care Transitions Project Greater Lansing Area, MI Western PA Evansville, IN Upper Capitol Region, NY Providence, RI North West Denver, CO Southwestern NJ Metro Atlanta East, GA Omaha, NE Baton Rouge, LA Miami-Dade, FL Harlingen, TX Tuscaloosa, AL
 * Altogether, 41 ZIP codes with: 7 hospitals 60 nursing homes 20 home health agencies ~375 physicians * * *Included in Target")
6 RI -Target Patients/Community The project targets 3 counties and patients (initially) with: Acute myocardial infarction (AMI) Congestive heart failure (CHF) Pulmonary processes (PNE+) * Altogether, 41 ZIP codes with: 7 hospitals 60 nursing homes 20 home health agencies ~375 physicians * * *Included in Target Community 6

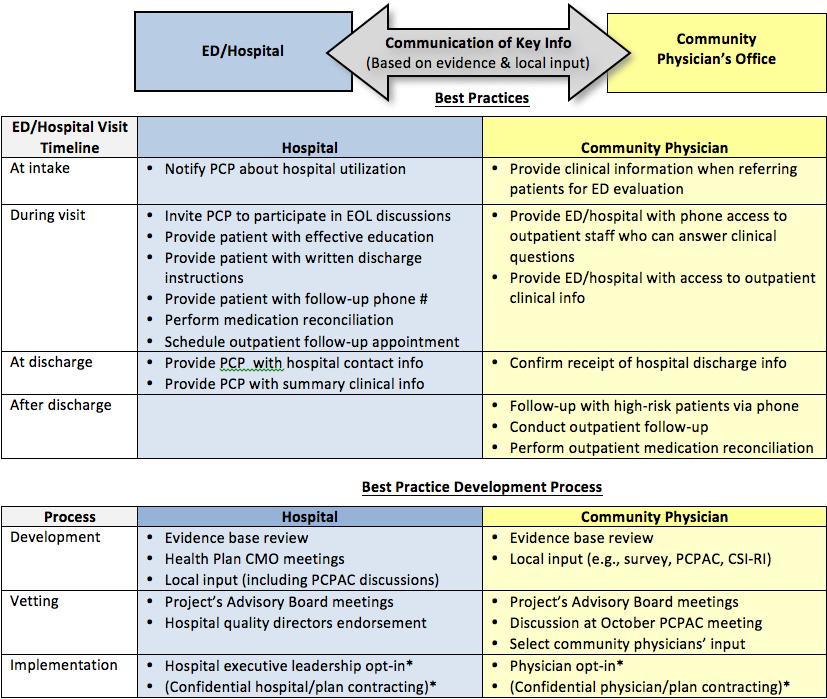
7 As a community, we defined our vision A healthcare system where discharged patients: understand their conditions and medications, know who to contact with questions (and when), and are supported by healthcare professionals who have access to the right information, at the right time. Over the past 2 ½ years, our transitions community and grown and RI has become a front runner in this journey 7
8 Project Goals Increase patient self-management Improve coordination of care Evidence-based practice Improved communication between providers Ultimately: Reduce 30-day re-hospitalization rates Improve post-discharge physician follow-up Enhance discharge-related outcomes (patient satisfaction) 1. Communication of information about medicines 2. Discharge information Our project s long-term goal: sustainability of proven interventions through cross-setting collaboration 8
9 Project Team s Initial Considerations How do we translate research to real-world conditions? What will work in our community? How can we affect outcomes quickly? How can we sustain change in the long-run? 9
10 HATCh Safe Transitions Model TM Advisory Board Best practices (e.g., hospital discharge) Economic models Business case (Long-term impact) Insurers C-Suites, Opinion Leaders Home Health Agencies Nursing Homes Systems interventions Tailored QI (each facility) Communities of practice: Within setting Across settings (Medium-term impact) Hospitals Patient/caregiver Physicians Patient interventions Coaching RED Education (Short term impact) 10

11 1. Low Patient (caregiver) activation Three Drivers 2. Lack of implemented standard and known processes 3. Inadequate communication 11
12 Team Considered the Existing Transitions Programs/Models Bridging Nursing Support / Transitional Care Model Transitional Care Nurses follow patients from the hospital into the home to provide services. Better Outcomes for Older Adults through Safe Transitions (BOOST) Toolkit for improving hospital discharge, including screening/assessment tools, discharge checklist, transition record, teachback process, risk-specific interventions and written discharge instructions. Best Practices Intervention Package (BPIP) Transitional Care Coordination Comprehensive manual for home health agency leadership and staff to identify tools and processes to improve patient transitions. Care Transitions Intervention Care transitions coaches support patients by providing specific tools and teaching self-management skills to ensure their needs are met during the transition from the acute care setting to home. Hospital to Home (H2H) National Quality Initiative Co-sponsored by the American College of Cardiology ( and the Institute for Healthcare Improvement ( H2H is an effort to improve the transition from inpatient to outpatient status for individuals hospitalized with cardiovascular disease. Interventions to Reduce Acute Care Transfers (INTERACT) Toolkit for SNF personnel to reduce avoidable hospital admission. Three types of tools: 1) communication; 2) clinical care paths; and 3) advance care planning. Re-Engineered Discharge (RED) Standardized discharge intervention; includes patient education, comprehensive discharge planning, post-discharge telephone reinforcement. Transforming Care at the Bedside (TCAB) Hospital intervention that includes four core elements: 1) enhanced admission assessment for post-discharge needs; 2) enhanced teaching and learning; 3) patient and family-centered handoff communication; and 4) early post-acute care followup.
13 Safe Transitions Project Provider Interventions Patient/Caregiver Activation CTI / RED Education Health Literacy Post Discharge Patient Call Back Programs Patient tools Zone tools CMS Discharge Checklist Pill boxes/ green bags Standard and Known Processes Standing Orders - Referral to SNF/ HH Follow-up Physician Appointments Palliative Care Counseling/Referrals Communication (within/across settings) CoC Form Audit/Feedback and Enhancements Multi-Disciplinary Rounding SBAR, Teach-back 13
14 A Closer Look at the Coleman: Patient Coaching The Care Transitions Intervention Coaches work 1:1 with hospitalized patients, following them for 30 days after discharge Two in-person visits (hospital and home/snf) Two phone calls RNs coach patients to ( Four Pillars ): 1. Use a personal health record (PHR) to self-manage 2. Perform medication reconciliation, or ask for help 3. Visit a physician for follow-up within seven days 4. Seek help for worsening red flags symptoms 14
15 CTI Key Lessons Patient activation appears to work among those who accept coaching This is not a clinical intervention coaches do not need to be nurses Our model also deployed social workers, a CNA, and a non-clinician The coach does not have to be owned by the hospital It may be a more effective intervention when deployed by a receiving provider in a way that it helps connect post-hospitalization care to PCP 15
16 What Else Works Preparing patients for Discharge - Day 1 Incorporating CTI s 4 pillars Educating using teach back method A Safe Discharge: Setting up for success Re-connecting with community resources Scheduling Follow-Up Visits Assisting with non-medical needs -The POINT Post discharge outreach
17 Incorporating Best Practices Hospitals and Community Physician Offices to start now working with Home Health Agencies and Nursing Homes
18 18
19 Wrap Up Q & A Session
20 Interested in learning more Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator, Quality Partners of Rhode Island
Outline. I. Overview of QIO Care Transitions. II. Analyses: patient trajectory III. Palliative and end-of-life care
 Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Home Health and Care Transitions. Objectives. The Care Transitions Theme: 9/28/2010
 Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor of Medicine, Brown University
 Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Meritage ACO Care Transitions: Coaching, Management, and Coordination
 Meritage ACO Care Transitions: Coaching, Management, and Coordination By Andrea Kmetz, RN https://www.psqh.com/analysis/aco-care-transitions-coaching-management-andcoordination/?highlight=wyjtzxjpdgfnzsjd#
Meritage ACO Care Transitions: Coaching, Management, and Coordination By Andrea Kmetz, RN https://www.psqh.com/analysis/aco-care-transitions-coaching-management-andcoordination/?highlight=wyjtzxjpdgfnzsjd#
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Care Transition Coach
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Care Transition Coach Marlene Seidel Butz Lehigh Valley Health Network, Marlene.Butz@lvhn.org Follow this and additional
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Care Transition Coach Marlene Seidel Butz Lehigh Valley Health Network, Marlene.Butz@lvhn.org Follow this and additional
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Care Continuum or Unconnected Silos
 Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Episode Payment Models:
 Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Housekeeping. Harmony Healthcare International, Inc.
 Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
INTERACT Webinar Series
 INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Sharing advanced INTERACT Success!
 Sharing advanced INTERACT Success! Developed by the following workgroup members: Irene Fleshner Pam Zanes William Thompson Laura Tubbs Judith Taubenheim Presentations by: Matt Tobalsky, LNHA Misti Valentino,
Sharing advanced INTERACT Success! Developed by the following workgroup members: Irene Fleshner Pam Zanes William Thompson Laura Tubbs Judith Taubenheim Presentations by: Matt Tobalsky, LNHA Misti Valentino,
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
West Valley and Central Valley Care Coordination Coalitions
 West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Ambulatory Care Management An Enhanced Care Coordination Program
 Ambulatory Care Management An Enhanced Care Coordination Program Carol Ecklund, RN, MN, AOCN Director of Medical Management May 21, 2014 TMIP Office Manager Webinar Objectives During this webinar you will
Ambulatory Care Management An Enhanced Care Coordination Program Carol Ecklund, RN, MN, AOCN Director of Medical Management May 21, 2014 TMIP Office Manager Webinar Objectives During this webinar you will
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
2016 Medical Home Summit. Reducing Hospital. Innovative Model of Care
 2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Readmission Prevention: A Community Collaborative Approach
 Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
M7: Improving Transitions and Reducing Avoidable Rehospitalizations. St. Luke s Hospital Member, Iowa Health System
 M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
National Committee for Quality Assurance
 National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
National Committee for Quality Assurance (NCQA) Private, independent non-profit health care quality oversight organization founded in 1990 MISSION To improve the quality of health care. VISION To transform
Improved Patient Engagement, Lower Readmissions with mhealth
 Improved Patient Engagement, Lower Readmissions with mhealth April 14, 2015 Mr. Richard Imbimbo, CFO Thompson Boyd, MD, FACHE, CHCQM, CPHIMS, CPHM DISCLAIMER: The views and opinions expressed in this presentation
Improved Patient Engagement, Lower Readmissions with mhealth April 14, 2015 Mr. Richard Imbimbo, CFO Thompson Boyd, MD, FACHE, CHCQM, CPHIMS, CPHM DISCLAIMER: The views and opinions expressed in this presentation
National Perspective No Wrong Door System. Administration for Community Living Center for Medicare and Medicaid Veterans Health Administration
 National Perspective No Wrong Door System Administration for Community Living Center for Medicare and Medicaid Veterans Health Administration Agenda National Perspective No Wrong Door System What is a
National Perspective No Wrong Door System Administration for Community Living Center for Medicare and Medicaid Veterans Health Administration Agenda National Perspective No Wrong Door System What is a
Medicaid Reform: The Opportunities for Home and Community Based Providers. All Rights Reserved
 Medicaid Reform: The Opportunities for Home and Community Based Providers ILS Background & Experience Care Management Company founded in 2001 Focuses on Duals, Medicaid ABD and Managing Medicaid Long term
Medicaid Reform: The Opportunities for Home and Community Based Providers ILS Background & Experience Care Management Company founded in 2001 Focuses on Duals, Medicaid ABD and Managing Medicaid Long term
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Medicaid Innovation Accelerator Project
 Medicaid Innovation Accelerator Project 2016-2017 Technical Expert Panel In-Person Meeting Community Integration Community-Based Long-Term Services and Supports Breakout Session April 18-19, 2017 Community
Medicaid Innovation Accelerator Project 2016-2017 Technical Expert Panel In-Person Meeting Community Integration Community-Based Long-Term Services and Supports Breakout Session April 18-19, 2017 Community
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan
 Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan July 2015 Inpatient hospitalizations account for 32 percent of the total $2.9 trillion spent on health care in the
Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan July 2015 Inpatient hospitalizations account for 32 percent of the total $2.9 trillion spent on health care in the
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses
 The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
The Metro Care Transitions Program (CCTP)
") The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
The National Quality Forum Quality Priorities and Home Care
 The National Quality Forum Quality Priorities and Home Care Lisa Hines, BSN, MS Managing Director, Membership & Council Services Objectives Awareness of The National Quality Forum The National Priority
The National Quality Forum Quality Priorities and Home Care Lisa Hines, BSN, MS Managing Director, Membership & Council Services Objectives Awareness of The National Quality Forum The National Priority
1/11/2016. The Metro Care Transitions Program (CCTP) OUR GOAL OUR HISTORY
 OUR GOAL OUR HISTORY") The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
The Metro Care Transitions Program (CCTP) OUR GOAL Build patient/caregiver confidence. Engage patients to take a more active role in self-management of chronic health conditions. Foster independence and
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Low Income Pool (LIP) Project Application Readmission Reduction Program at Memorial Regional Hospital
 Project Application Readmission Reduction Program at Memorial Regional Hospital") Low Income Pool (LIP) Project Application Readmission Reduction Program at Memorial Regional Hospital submitted by South Broward Hospital District, d/b/a Memorial Healthcare System July 31, 2012 Readmission
Low Income Pool (LIP) Project Application Readmission Reduction Program at Memorial Regional Hospital submitted by South Broward Hospital District, d/b/a Memorial Healthcare System July 31, 2012 Readmission
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Faculty Presenters. The Care Transitions Program. STAAR Initiative
 Session M13 These presenters have nothing to disclose 26th Annual National Forum on Quality Improvement in Health Care Minicourse: Reducing Avoidable Readmissions by Creating a More Patient-Centered Transition
Session M13 These presenters have nothing to disclose 26th Annual National Forum on Quality Improvement in Health Care Minicourse: Reducing Avoidable Readmissions by Creating a More Patient-Centered Transition