Care Transitions Partnerships that Work for Patients
|
|
|
- Egbert Maxwell
- 5 years ago
- Views:
Transcription


1 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator, Greenknoll Care and Rehabilitation Center WHAT S THE PROBLEM 1
2 Rising Health Care Costs Between 41.9 and 70% of MCR patients admitted to Hospital for care received services from an average of 10 or more physicians during their stay On average patients 65 and older with 2 or more chronic diseases see seven different physicians within one year and account for 95% of Medicare expenditures Discharges and Readmissions Nearly one in 5 discharges paid by Medicare Fee for Service is followed by another admission to a hospital within 30 days and 34% are readmitted within 90 days Half of those readmitted had not seen a physician since their discharge Unplanned readmissions cost Medicare over $18 Billion annually 2
3 System Of Care - Failures Practice in silos Poor communication Conflicting information Little knowledge or experience with other settings No standardized patient protocols across settings Primary physician out of information loop Competition limits sharing Lack of support for patient self management Self Management - Failures Patient and Family not active participants Unprepared to make their own decisions Overwhelmed Insufficient or conflicting information and support Non compliance High score on risk assessment 3

4 Transfer - Failures Communication Medication Reconciliation Medication Management Duplicative Meds Sub optimal Use Patient and Caregiver Confusion Lack of follow through on Referrals Missed or redundant MD appointments Not active in own care 4

5 Readmission Penalties 10 5
* Q1 12 by County 21.4 to 24.0 20.6 to 21.3 20.0 to 20.5 19.0 to 19.9 17.4 to 18.")

6 Medicare 30 Day Readmission Rate by State New Jersey 30-Day Readmission Rate by County (Q1 2012)* Q1 12 by County 21.4 to to to to to 18.9 *Source: This material was prepared by HQSI, under contract with CMS. These statistics are HQSI internal analysis of Medicare FFS claims for eligible beneficiaries discharged from NJ hospitals. 6
 Readmissions of Patients Discharged to SNFs (26.87%) Readmissions of Patients Discharged with Home Health Care (23.41%) Readmissions of Hospice Patients (2.")
7 New Jersey State Ranking on 30-Day Readmission Rates (2010)* 30-Day Readmission Rates (2010) All Readmissions (21.48%) Readmissions of Patients Discharged to Home without Home Health Care (17.88%) Readmissions of Patients Discharged to SNFs (26.87%) Readmissions of Patients Discharged with Home Health Care (23.41%) Readmissions of Hospice Patients (2.96%) State Ranking 50 out of out of out of out of out of 53 *Source: Post Acute Care Readmission Rankings as prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 13 7


8 How Can We Help Whose Responsibility is it? 8
9 Purposeful Partnerships Tools for group problem solving, decision making and action Dynamic groups vs time eaters Pool expertise, talents, energy and resources of members Compelling community problem Two main components Set aside personal agendas Come together to engage in public problem solving Goal of Collaboration Compelling reason for existing Bring together the right mix Represent multiple aspects of the problem Bring potential solutions Community Problem Solving 9
10 Purposeful Partnerships in the Community Interest 1. Is the collaboration focused on an issue you feel passionate about? 2. Are others in the group passionate about the issue? 3. Are you willing to commit your resources money, time, and talents so this can succeed? 4. Does the partnership/collaboration have the community s interest in mind? 5. Are the right people involved in the collaborative? 7 Keys for Sustaining Project Excellence Project Management Processes Organization Structure Project Management Tools Capable People Involvement and Communication Project Performance Management Leadership 10


11 Transitions in Care A set of actions designed to ensure the coordination and continuity of health care as patients transfer between different locations or different levels of care within the same location. T R A N S I T I O N S Home SAR ALF LTC Home Care Hospice Hospital 11
12 The Models - Red Boost Transitional Care Model Coleman Care Transitions Program Project Red Re-engineered Discharge Nurse Discharge Advocate Patient Education Comprehensive Discharge Planning Post-Discharge Telephone Reinforcement Follow up Appointments Individualized instruction booklet Pharmacist telephone follow-up 12


13 Components of RED Educate about diagnosis Make appointments for follow up Discuss test or study results Organize post discharge services Confirm the medication plan Reconcile the discharge plan Review what to do if problem arises Expedite sending D/C summary to physician Have patient explain in own words the plan Written D/C plan Telephone reinforcement 2-3 days post discharge Boost Better Outcomes, Older Adults Toolkit for hospital discharge Screening/Assessment Tool Discharge Checklist Transition Record Risk-specific interventions Written discharge instructions Improvement of information flow Identification of high risk patients Teach back Patient Education 13
14 BOOSTing Care Transitions TARGET Tool for identifying and addressing risk Universal checklist on discharge GAP general assessment of preparedness Transition Record (simpler version of PHR) Interventions (on discharge) Meds reconciled with preadmission meds Med use/side effects with teach back Action plan for management of symptoms Discharge communication provided post hospital providers Direct communication with PCP at discharge 72 hour phone contact post discharge Transitional Care Model Mary Naylor Multidisciplinary Comprehensive in hospital planning Transitional Care Nurse follows patient from hospital to home Streamline plan of care Interrupt patterns of emergency room use and re-hospitalization 14
15 Standard Protocol In Hospital Visits with Patients Comprehensive assessment of health status Defines priority needs and services Designs and Coordinates inpatient and follow-up care Home Visits with Patients Visit within hours post discharge 1 vs per week x 1 month then semi monthly until D/C Telephone calls on non visit weeks Plan for emergency care Nurse visit with Physician TCN accompanies patient on first visit post D/C Transition from Transitional Care Nurse Communicates with PCP Completes a transition summary for patient and physician Care Transitions - Coleman The Model Four Pillars Trained Transition Coach Hospital Visit Home Visit 3 Follow-up Phone Calls Med Management Med Reconciliation Personal Health Record MD Appt follow-up Red Flags 15

16 Pillar: Medication Self Management Patient Centered Record Follow-up Red Flags Goal Patient Knowledgeable about meds and has system Understands and manages a PHR Patient schedules and completes follow up MD visit Knowledgeable about indications that condition is worsening and how to respond Hospital Visit Discuss importance of knowing meds Explain PHR Recommend primary care provider follow-up visit Discuss symptoms and drug reactions Home Visit Reconcile pre and post hospital med list Review/update PHR Review D/C Summary Emphasize importance of FU visit Discuss symptoms side/effects meds Follow up Calls Answer any remaining Med Questions Discuss outcome of visit with PCP Provide advocacy in getting appt if necessary Reinforce when/if PCP should be called 16


17 Case Study Utilizing The Coleman Model 17

18 CARE A Collaborative Approach to Reach Patient Empowerment Community Partners: Community Visiting Nurse Association Somerset Medical Center Arbor Glen Continuing Care Community Bridgeway Care Center Green Knoll Care and Rehabilitation Center Greenbrook Manor Nursing and Rehabilitation Center Raritan Health & Extended Care Somerset Valley Rehabilitation & Nursing Center OBJECTIVES BUILD, FACILITATE AND MAINTAIN A COLLABORATIVE ENSURE SAFE AND EFFECTIVE DISCHARGES IMPROVE SEAMLESS DELIVERY OF CARE DEVELOP AND EMPLOY A CROSS INSTITUTIONAL MEDICATION RECONCILIATION FOR AND PROCESS PROMOTE PATIENT EMPOWERMENT AND SELF MANAGEMENT PROVIDE PATIENT AND FAMILY A VOICE IN THEIR CARE INCREASE PATIENT ABILITY TO SELF MANAGE CHRONIC ILLNESS ENSURE TRANSFER OF ADEQUATE AND COMPLETE PATIENT INFORMATION SHIFT PARADIGM FROM ACUTE CARE TO SUPPORTIVE AND HOLISTIC APPROACHES AT END OF LIFE ENSURE PHYSICIAN ALIGNMENT PROMOTE HEALTH TECHNOLOGY 18

19 PROGRAM BREAK DOWN BARRIERS TO CARE PATIENT EMPOWERMENT REDUCE HOSPITAL READMISSIONS TARGET POPULATION 55 OR OLDER SOMERSET AND MIDDLESEX COUNTIES DIABETES, CHF, COMORBIDITIES COMPLEX SOCIAL CIRCUMSTANCES WHILE ON SERVICE UP TO 1 YR COMMUNITY COLLABORATION HOSPITAL SUB ACUTE ASSISTED LIVING LONG TERM CARE HOMECARE HOSPICE COLEMAN MODEL ADVANCED PRACTICE NURSE/PATIENT COACH Enhancing Patient Outcomes Joint Quality Outcomes Collaboration among Healthcare providers Transitional care team State of the art technology Patient SELF MANAGEMENT Physician Interventions and parameters Coaching/Self Care Evidenced based guidelines Symptom Mgt. Medication Mgt. 19

20 Principles of Coleman Model Transition Coach and Personal Health Record central to patient empowerment and ability to self manage Improving patient or family members comfort with taking a more active role in their care Facilitates communication among providers, across settings and between patient/family and health care system Improve care transitions by providing patients with tools and support that promote knowledge and self management of their condition Goal of Care Independence Transition from role of patient to self-care management No ER visits No Hospitalizations No unscheduled home care visits Improved Quality of Life 20


21 Role of the Advanced Practice Nurse - Patient Focus Introduce patient/family to the program Provide patient support Promote patient education Role models behavior on how to play an active role Models and facilitates new behaviors and communication skills Helps patient with completion of Personal Health Record Review patient progress with four pillars Tailors content of visits/calls to needs and priorities of patient Four Basic Segments of activation or Self Management Competency Level 1 Level 2 Level 3 Level 4 Starting to take a role Individuals do not feel confident enough to play an active role in their own health % of the population Building knowledge and confidence Individuals lack confidence and an understanding of their health or recommended health regimen 20-30% of the population Taking Action Individuals have the key facts and are beginning to take action but may lack confidence and the skill to support their behaviors 30-40% of the population Maintaining Behaviors Individuals have adopted new behaviors but may not be able to maintain them in the face of stress or health crises 20-30% of the population Increasing level of Activation 21
22 Services, Tools and Assessments Patient Coach Risk Assessment Readiness to Change CTM Care Transition Measure Personal Health Diary (PHR) Personal Activation Assessment Red Flags/Heart Zones Universal Transfer Form Customized Education Scales Point Person at each Facility Transition Room/Experience Telemonitoring Chronic Care Management Outpatient Services Staff Education Support Groups Shared Data Drive Community Involvement Restaurants/MOW/Grocery Store My thoughts about changing my behaviors for this area: Readiness to change It is important for your healthcare team to know how ready you are to make changes to improve your health. This information can help you, your family and your healthcare team. Know how ready you are to change your behavior Talk with you about steps you can take to help you change your behavior Please take a few minutes to think about the following heart failure management areas. Then put an X in the box that best describes how you feel about making any changes for each behavior. Please give this complete form to your Nurse or Nurse Practitioner during your visit today. Heart Failure Management Areas: Weigh myself daily Take my medicine regularly Make healthy food choices I am thinking about it I am ready to start making some changes I recently started doing this I have already been doing this for the past six months or more Be physically active on a regular basis Keep my appointments Stop smoking Manage Stress Check my blood sugar if diabetic 22
23 Know Your Heart Failure Zones Zones Everyday Things to monitor Green Zone All Clear Yellow Zone Caution This is where we can make a difference with interventions Red Zone - Emergency CARE TRANSITIONS MEASURE (CTM-3) Patient Name: Date: 1. The hospital staff took my preferences and those of my family or caregiver into account in deciding what my health care needs would be when I left the hospital? 2. When I left the hospital, I had a good understanding of the things I was responsible for in managing my health. 3. When I left the hospital, I clearly understood the purpose for taking each of my medications. 23
24 Risk Assessment Problem High Risk medications (anticoagulants, insulin, digoxin, narcotics) Psychological (depression screen positive or h/o depression diagnosis) Principal diagnosis (cancer, stroke, DM, COPD, heart failure) Polypharmacy (5 or more routine meds) Poor health literacy (inability to do Teach Back) Patient support (absence of caregiver to assist with discharge and home care) Prior hospitalization (non-elective; in last 6 months) Palliative care (Would you be surprised if this patient died in the next year? Does this patient have an advanced or progressive serious illness?) Yes to either: Care Collaborative Chart Review Please complete and within 3 days of readmission. Name: Patient ID # : Age: Sex: M F English Primary Language: Spanish Other: Primary Diagnosis: Other Related Diagnosis: Hosp. Admit Date: Hosp. D/C Date: 30 Days: D/C to Sub-acute: Y N D/C to Home Care/Hospice: Y N D/C to Home No Services: Y N Hospital Readmit Date: D/C to Readmit: Readmission Diagnosis: Identified as High Risk for Readmission: Y N Fall Risk Polypharmacy Prior Hospitalization within 6 mths. Non English Speaking/English Second Language # Days From Symptoms Prior to Readmission: Related to CHF: Y N Related to Diabetes: Y N Patient seen by Physician Readmission: Prior to Y N U Sub-Acute/SNF: Seen by physician within 7 Y N U days of D/C: Seen by physician within 14 days of D/C: N U Home No Services: Pt saw physician within 7 days of D/C: Y N U Pt saw physician within 14 days of D/C: N U Homecare/Hospice: Pt saw physician within 7 days of D/C: Y N U Y Y N U Pt saw physician within 14 days of D/C: Y Patient Utilizing Health Record: Y N Patient Weighing Self Daily: Y N Patient Monitoring Blood Sugar: Y N Patient follows prescribed diet: N Y Patient follows Medication Regimen: Y N Patient record evidences understanding/teachback of Red flags: Y N Patient record evidences understanding/teachback of when to call Agency/MD: Y N Patient on high risk Meds: Y N Record evidences understanding/teachback of meds: Y N N/A Any changes in patient status reported to MD on same day: Y N Documented communication provided to all members of team in regard to patient status change: Y N Physician/Family requested/insisted on transfer: Y N Any interventions prior to transfer: Was this ACH preventable: 24

 Check for Edema - Measure Breath Sounds")
25 CHF Visit Protocol Vital Signs B/P, Pulse, Resp. Weigh patient on every visit encourage patient to weigh self daily. (Same time each day) Check for Edema - Measure Breath Sounds Heart Sounds SOB - observe SP02 Heart Zones Looking for changes from visit to visit 25
 EMERGENCY ROOM VISITS MD FOLLOWUP VISITS WITHIN 2 WEEKS OF DISCHARGE PERCENTAGE OF ELIGIBLE")
26 LISTEN TO YOUR NURSE! DATA POINTS TRANSITION SATISFACTION CTM3 REHOSPITALIZATION RATES (30,60,90 DAYS) EMERGENCY ROOM VISITS MD FOLLOWUP VISITS WITHIN 2 WEEKS OF DISCHARGE PERCENTAGE OF ELIGIBLE PATIENTS ENROLLING IN PROGRAM ADDITIONAL RISK DATA READINESS TO CHANGE SCORES FOLLOW UP PHONE CALLS AVERAGE LOS PATIENT ACTIVATION ASSESSMENT CLINICAL OUTCOMES 26
27 Collaboration Eight Partners Strong Weekly/Bi Weekly Meetings Open Forum for Discussion Understanding that Partnership development takes time Buy in from key organization stakeholders Community investment Partner Organizations WHY I M A PARTNER Mission Better Connection to Hospital Need to Participate Commitment to Service Strength in Numbers Serve same Patients WHAT IT DOES FOR ME Business Referrals Cost Containment Good Business Decision Quality Outcomes Standardization Patient Satisfaction Marketing Edge Remain on Cutting Edge Development ACO s Chance to get Published 27
28 Partners Role in System of Care Voice in design and implementation Development of policies and procedures Maintaining fidelity to model Fostering communication Designate point person at each facility Program support Liaison to Advanced Practice Nurse Educate staff Provide and update statistical data Monthly meetings for program and data review and evaluation Continuous program improvement System Support Educates staff on new model Champions program Supports change in practice Communicates progress between facilities Ensures fidelity to model In their facility Acts as liaison with physicians Oversees system of care 28
29 THE CARE MODEL Patient Admitted to SMC Better Choices Follow up Phone Calls if D/C home without services Chronic Care Program Telemed Outpatient Services ER Coor determines eligibility Risk Assessment APN visits in Hospital Med Rec Readiness to Learn Transition Utilizing Universal Transfer Form Patient D/C checklist Med Rec Facility Home Care Hospice APN Transition visit CTM-3 Med Rec Home Self Managed APN visits prior to and after any D/C or transfer Receives patient education booklet, personal health record 4 Pillars Education and response Patient Coaching Disease Education Continue 4 Pillars Disease Education Transition Room or Experience Pre D/C Transitions/Patient Empowerment Medication Self Management Educational Booklet Personal Health Record Coaching Patient Empowerment Transition Mgmt Medication Reconciliation Tool Teach Back Process Reduced medication errors or discrepancies Decreased Patient Complications Diet management Educational Booklet Nutritional Counseling Coaching Patient Empowerment Transition Mgmt Hospital Readmission Data Reduction in ED admissions for Diabetes /CHF and/or Complications of Weight Management Daily Weights Pt Responsibility PHR, Coaching Patient Empowerment Transition Mgmt Increased self care Knowledge of red flag Reduction in ED admissions for CHF B/S management Daily B/S monitor Pt Resp/PHR Coaching Patient Empowerment Transition Mgmt Increased self care Knowledge of red flag Reduction in ED admissions for Diabetes Increased understanding of risk factors Coaching Role Playing Patient Empowerment Transition Mgmt Pt Empowerment Increased self resp for health care Reduced avoidable ED visits and Hospital Readmissions Decreased adverse events 29
30 Transitions/Patient Empowerment Improved patient satisfaction CTM-3 Patient Empowerment Transition Mgmt Press Ganey/Other format Improved Patient Satisfaction Improved perception of quality of life Increased ability to manage own health Patient Empowerment Transition Mgmt Increased skill among health care workers Improved Community Health More active participation in transitions Provide caregiver with tools and support Patient Empowerment Transition Mgmt Provide caregiver with tools and support Improvement in care transitions Patient able to communicate needs effectively Personal Health Record Continuity of care plan across providers and settings Patient Empowerment Transition Mgmt Enhanced ability of health technology to promote information exchange across care settings Improved Communication Structure Increased self responsibility and understanding of health care Empowerment Support Groups Coaching Follow up MD Patient Empowerment Transition Mgmt Follow Up MD visit Reduced avoidable ED visits and Hospital Readmissions Decreased adverse events Tracking and Sharing Tools and Activities Teach-Back Process Medication Discrepancy Tool Excel Spread Sheet for Data Tracking/Move to Access Determined What, When, Who and How Determined two alternatives for Data Sharing Chart Review Worksheet for Readmissions Set Monthly Meetings for Data Review Developed Goals, and System, Patient and Community Level Outcomes and Developed Methods to Capture Data Set Education Strategy Constructed Communication Strategy Diagnostic Tool for Evaluating Group Function 30



31 Health Status Medical Center Statistics Sept 2011 CFH Re-Admissions 2010 (March-October) 31

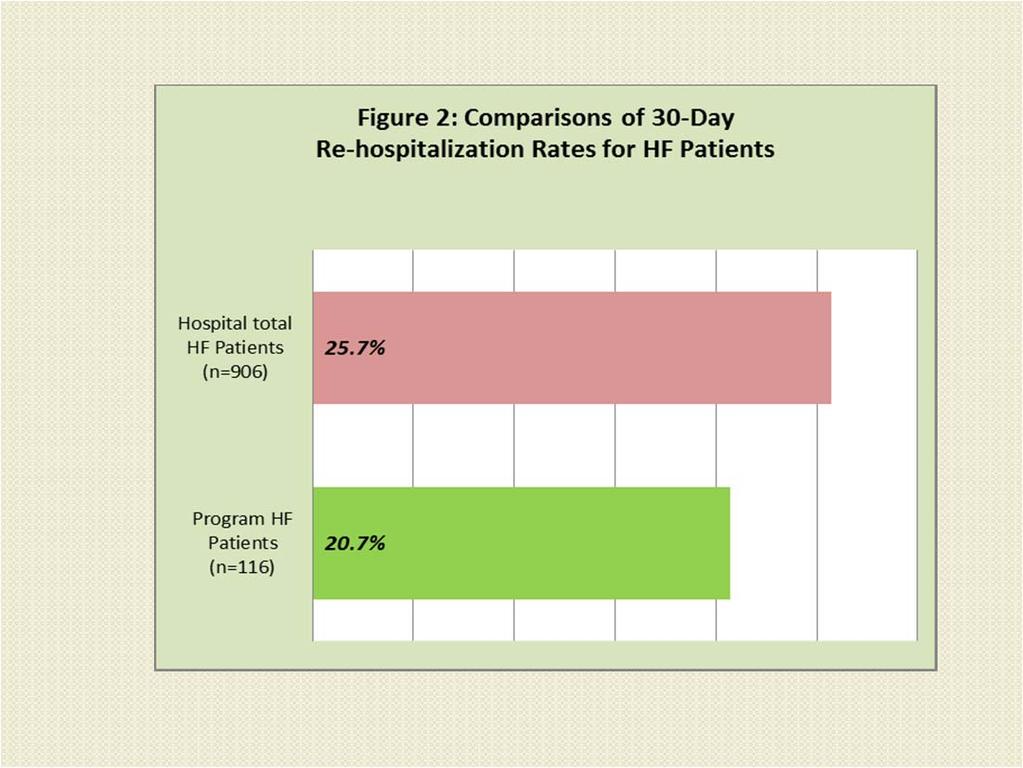
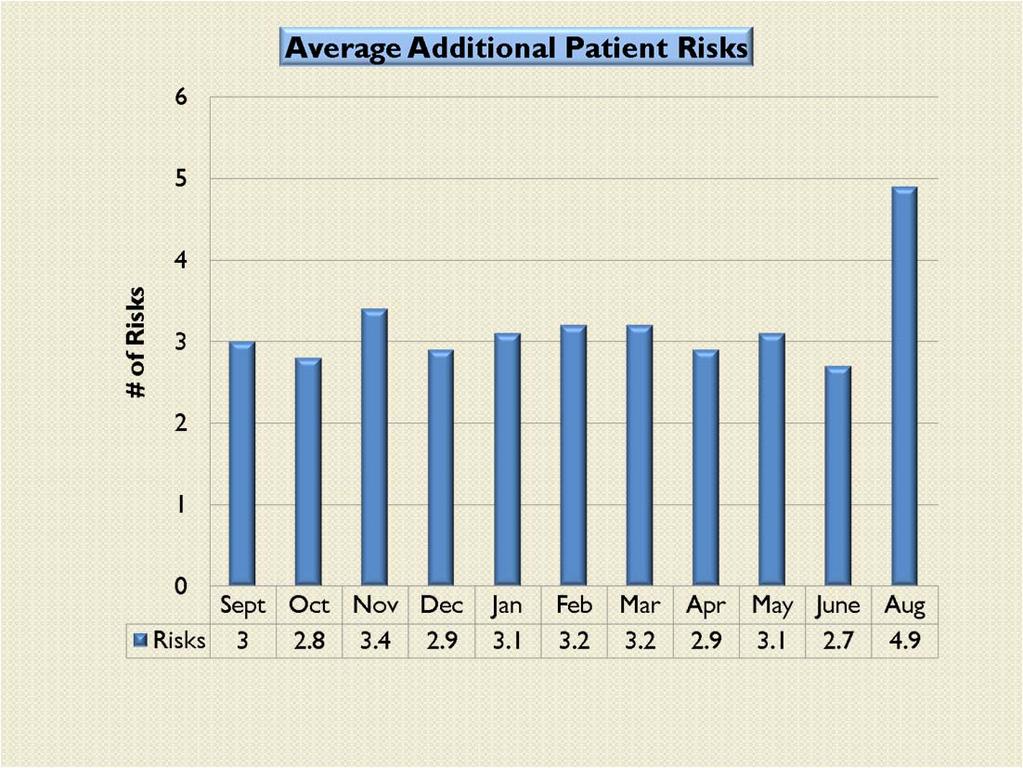
32 OUTCOMES One Year of Program Data 32
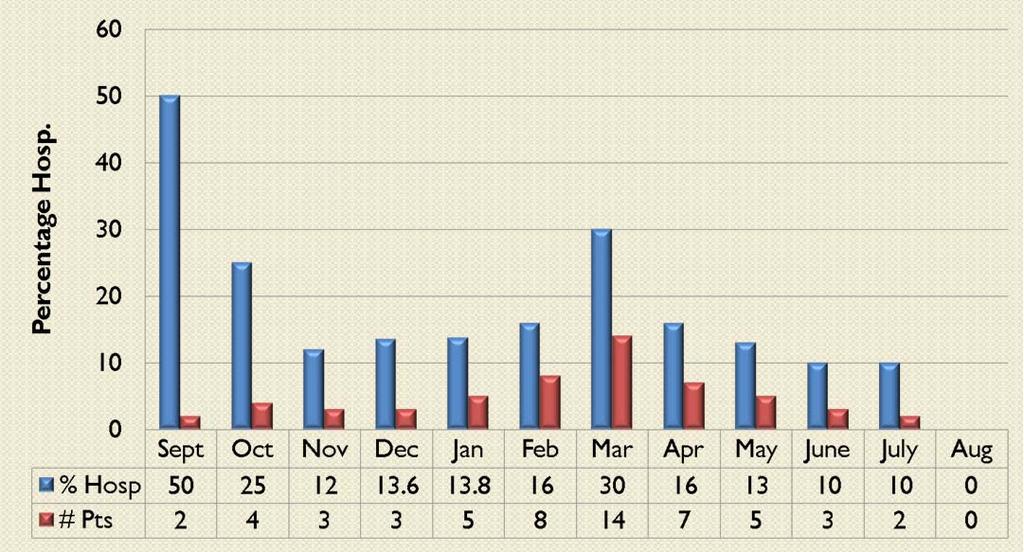

33 30 Day Hospitalization Data March Trends 33

34 Reasons for March Readmissions GI Bleed Fever, Shortness of Breath Anemia Sepsis COPD Hypoglycemia Seizures CHF Urinary Tract Infection Respiratory distress 34

35 35


36 Table 4. Physician Follow up Visit among Program Patients # patients with follow up % patients with follow up Hospital Discharge Month # of patients 7 Day 14 Day 30 Day 7 Day 14 Day 30 Day Sep Oct Nov Dec Jan Feb Mar Total Readmission Rates for Program Participants 30/60/90 Days 36
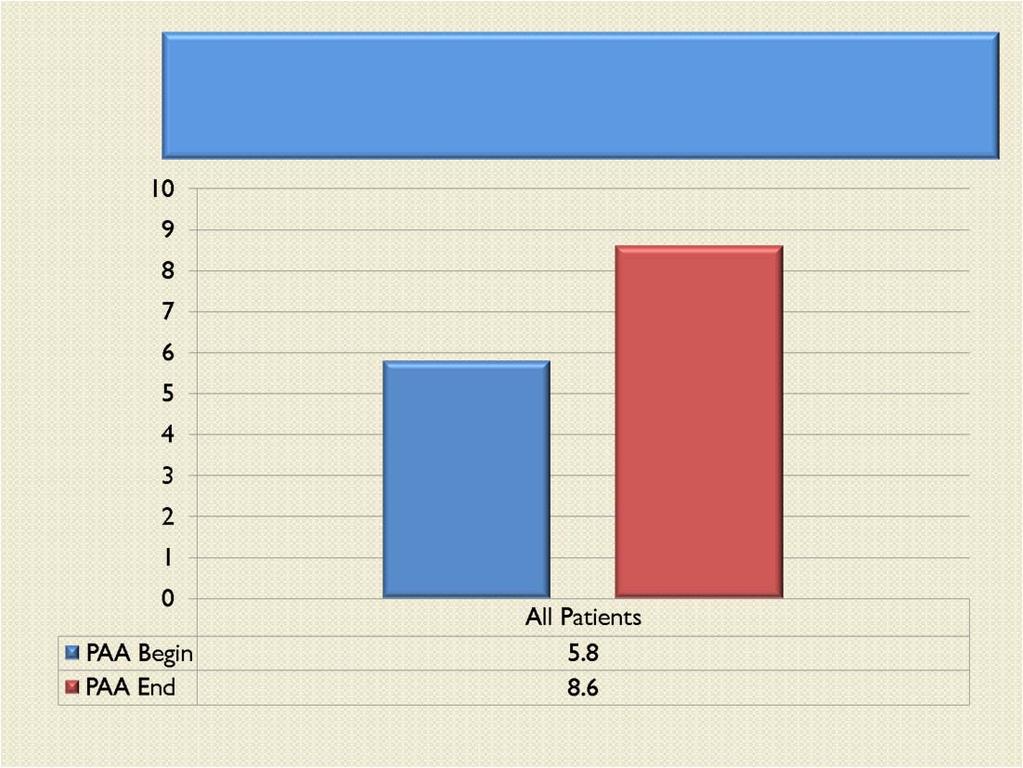
37 Patient Activation Assessment 37


38 CTM 3 SCORES 9/12/11 4/30/12 Length of stay 38
39 Accomplishments Patient Education Customized CHF Booklets Diabetic Booklets Hiring of APN within 45 days Patient Scales Customized Personal Health Diary Staff Education Physician Education Community Education Diabetes/CHF Diabetes Education Modules Shared Data Drive Universal Transfer Form Practice Tip Sheets Medication Availability/Facilities Coleman Training Partner Collaboration Monthly Meetings Good Attendance Roundtable Discussions Standardized Protocols Standardized Education Improved Patient Care Improved Documentation Best Practices Standardized Data Collection Collaboration HQSI Community Presentations Reduction in Re-hospitalizations Progress towards Objectives BUILD, FACILITATE AND MAINTAIN A COLLABORATIVE ENSURE SAFE AND EFFECTIVE DISCHARGES IMPROVE SEAMLESS DELIVERY OF CARE DEVELOP AND EMPLOY A CROSS INSTITUTIONAL MEDICATION RECONCILIATION FORM AND PROCESS PROMOTE PATIENT EMPOWERMENT AND SELF MANAGEMENT PROVIDE PATIENT AND FAMILY A VOICE IN THEIR CARE INCREASE PATIENT ABILITY TO SELF MANAGE CHRONIC ILLNESS ENSURE TRANSFER OF ADEQUATE AND COMPLETE PATIENT INFORMATION SHIFT PARADIGM FROM ACUTE CARE TO SUPPORTIVE AND HOLISTIC APPROACHES AT END OF LIFE ENSURE PHYSICIAN ALIGNMENT PROMOTE HEALTH TECHNOLOGY 39
40 Challenges Change from the outside in Multiple partners Follow through Same message Same Processes and Protocols Data Collection Monitor up to 1 year Excel Access Changing Data Challenges Patient Identification Cerner Tabs Physician Buy In Increased Competition with Other Programs Medication Reconciliation Partnering with Community Organizations Maintaining the Momentum Effecting and Sustaining Change 40
41 Over Time Demonstrate program success through measurable results Support continuous quality improvement Build finance model to identify needs to sustain activity Support change to a patient centered care system Patient Coach as the change agent over time becomes train the trainer so that everyone knows and is comfortable with the coaching model Multiplication effect proven program utilized by all 8 partners increasing the positive impact we are able to make for the populations we are serving and the organizations Where to Start Join or Initiate a group Identify high risk patients for re-hospitalization Historical Current Data and CMS Initiatives Start discussions on admission and discharge processes Look at best practices and evidence based models Determine what will work for the group and get started small is okay 41
42 42
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses
 The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Complex Care Management Protocols and Procedures
 Complex Care Management Protocols and Procedures December 2014 Version 3.0 1 Table of Contents I. Complex Care Management Program Staff Roles and Responsibilities... 4 II. Complex Care Management Program
Complex Care Management Protocols and Procedures December 2014 Version 3.0 1 Table of Contents I. Complex Care Management Program Staff Roles and Responsibilities... 4 II. Complex Care Management Program
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
At EmblemHealth, we believe in helping people stay healthy, get well and live better.
 At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
Roundtable on Health Literacy Institute of Medicine 17 March 2014
 Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Discharge Information
 Discharge Information Yes, patients were given information about what to do during their recovery Vikki Choate, MSN, RN, CCM, RN-BC, CPHQ Nashville, TN May 14-15, 2013 Learning Objectives At the end of
Discharge Information Yes, patients were given information about what to do during their recovery Vikki Choate, MSN, RN, CCM, RN-BC, CPHQ Nashville, TN May 14-15, 2013 Learning Objectives At the end of
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Improving Patient Outcomes through Quality Transitions
 Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Improving Patient Outcomes through Quality Transitions Founded in 1892, Union Hospital began as a 20 bed facility and has grown into a 380 bed not-for-profit hospital Union Hospital is a Regional Referral
Exacerbation of Condition. VNAA Best Practice for Home Health
 Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Ambulatory Care Management An Enhanced Care Coordination Program
 Ambulatory Care Management An Enhanced Care Coordination Program Carol Ecklund, RN, MN, AOCN Director of Medical Management May 21, 2014 TMIP Office Manager Webinar Objectives During this webinar you will
Ambulatory Care Management An Enhanced Care Coordination Program Carol Ecklund, RN, MN, AOCN Director of Medical Management May 21, 2014 TMIP Office Manager Webinar Objectives During this webinar you will
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State ( )
") RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Implementation Guide: Critical Interventions in the First/Second Visit. VNAA Best Practice for Home Health
 Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Oxford Condition Management Programs:
 Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services
 Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM
 ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Question Patient #1 Patient #2 Patient #3 Patient #4 Patient #5 Number of days between the last discharge and this readmission date?
 Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
Worksheet A: Chart Reviews of Patients Who Were Readmitted Conduct chart reviews of the last five readmitted patients. Reviewers should be physicians or nurses from the hospital and community settings.
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
DELTA CARE CHANGING LIVES. A CARE TRANSITION PROGRAM of EPHRAIM MCDOWELL HEALTH DR. JOAN HALTOM, PHARM.D, FKSHP GAIL SHEARER, BSN, MBA,CCM
 DELTA CARE CHANGING LIVES A CARE TRANSITION PROGRAM of EPHRAIM MCDOWELL HEALTH DR. JOAN HALTOM, PHARM.D, FKSHP GAIL SHEARER, BSN, MBA,CCM DELTA CARE Delta Care is an Innovative approach to transitioning
DELTA CARE CHANGING LIVES A CARE TRANSITION PROGRAM of EPHRAIM MCDOWELL HEALTH DR. JOAN HALTOM, PHARM.D, FKSHP GAIL SHEARER, BSN, MBA,CCM DELTA CARE Delta Care is an Innovative approach to transitioning
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able