Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
|
|
|
- Martha Montgomery
- 5 years ago
- Views:
Transcription

1 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety
2 Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated with the increased focus on patient re hospitalization, particularly related to the transition from hospital to home List various predictors to assist in the identification of patients who can benefit from post acute care Recap strategies that have been utilized to promote successful, safe transitions for patients from the hospital to their homes without resulting re hospitalizations
3 Consensus National Attention Institute of Medicine (IOM) report, To Err is Human 2001 IOM report, Crossing the Quality Chasm 2007, 2008 MedPAC reports highlight avoidable rehospitalizations; recommend data reporting and payment reform May 2008 National Quality Forum (NQF) endorsed 5 outcome measures for care transitions Aug 2008 CMS launched Care Transitions contracts in 14 communities; 9 th SOW Nov 2008 National Priorities Partnership (NPP) identified care coordination as one of six national priorities; stressed need for increased communication
4 Consensus National Attention April 2009 New England Journal of Medicine article (Jencks, Coleman, Williams) Fall 2009 CMS releases hospital specific readmission rates for AMI/Pneumonia/HF 2009 States and providers actively engaged in efforts to reduce re hospitalization and improve care coordination 2010 Enactment of the Patient Protection and Accountability Care Act (PPACA) aka Affordable Care Act th Scope of Work Care Integrations
5 Why is readmission reduction a priority? The 2009 study of the 2004 Medicare population by Dr. Jencks was published in the NEJM Findings: 19.6% were readmitted within 30 days 34% were readmitted within 90 days. 50% of those readmitted had not seen their PCP Average LOS for the rehospitalized patient was 0.6 days longer Hospital readmissions have been identified as an important outcome measure for assessing performance of the health care system New England Journal of Medicine Re hospitalizations among Patients in the Medicare Fee for Service Program, Jencks, Williams, Coleman; April 2009
6 Hospital Utilization In 2011, more than 7 million Medicare beneficiaries experienced 12.4 million inpatient hospitalizations This equals approximately 2.5 million re hospitalizations during 2011 (30 day Rehospitalization Rate = 20%) Older adults are hospitalized for fall-related injuries 5 times more often than they are for injuries from other causes Medicare Payment Advisory Committee (MedPAC). Report to the Congress: Medicare Payment Policy Washington, DC: March 2012 Medicare Payment Advisory Committee (MedPAC). Report to the Congress: Medicare Payment Policy Washington, DC: March 2011:Chapter 8 pp
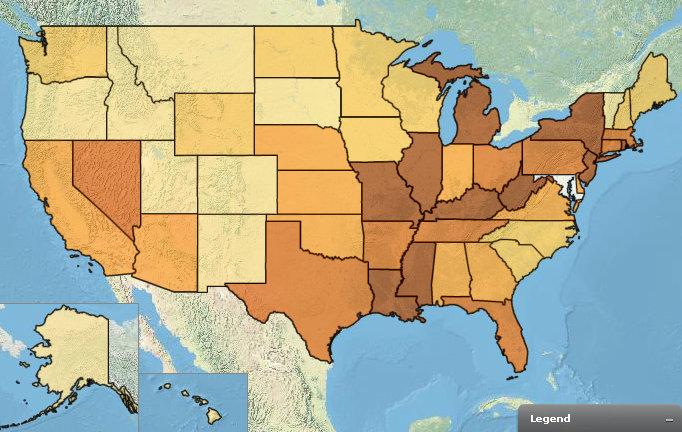
7 Rate* of Nonfatal, Medically Consulted Fall Injury Episodes, by Age Group National Health Interview Survey, United States, 2010 * Per 1,000 population. Annualized rates of injury episodes for which a health-care professional was contacted either in person or by telephone for advice or treatment. An injury episode refers to a traumatic event in which the person experienced one or more injuries from an external cause. Estimates are based on household interviews of a sample of the civilian, non-institutionalized population. 95% confidence interval. Adams PF, Martinez ME, Vickerie JL, Kirzinger WK. Summary health statistics for the U.S. population: National Health Interview Survey, Vital Health Stat 2011;10(251).
8 Rehospitalizations are.. Rehospitalizations are Frequent 30 day Re admission rates (2008) One in five Medicare patients (19%), One in four Medicaid patients (24%) SNF & Nursing Home patients (24%), Greater than one in ten privately insured patients (12%) Wier LM, Barrett M, Steiner C, Jiang J. All cause readmissions by payer and age, Healthcare cost and Utilization Project. AHRQ. Statistical Brief #115, June 2011.
9 Rehospitalizations are.. Variable (2009)


10 Rehospitalizations are.. Costly Medicare Spending (Billions) 10 Jencks, S., Williams, M., Coleman, E. Rehospitalizations among Patients in the Medicare Fee for Service Program. NEJM April 2009, 360(14), Medicare Payment Advisory Committee (MedPAC). Report to the Congress: Medicare Payment Policy Washington, DC: March 2011:Chapter 8 pp
11 Rehospitalizations are.. Potentially avoidable In 2008, one out ten hospital stays were potentially preventable 3.9% acute conditions 6.2% chronic conditions 60 % patients > 65 Actionable for improvement Greater than 30% reduction of 30 day readmission rates have been realized from research and quality improvement initiatives Care Transition Programs Coleman, Naylor, STAAR, RED, BOOST Stranges, E., Stocks, C. Potentially Preventable Hospitalizations for Acute and Chronic Conditions, Healthcare cost and Utilization Project. AHRQ. Statistical Brief #99. November National Transitions of Care Coalition. Improving Transitions of Care. September 2010

12 Factors leading to Hospital Readmission Bisognano M & A Boutwell. Improving Transitions to Reduce Readmissions. Frontiers of Health Service Management (3): 6
13 What can the Hospital do to help prevent an unplanned hospitalization? Appropriate referral for home care Enhanced client / family education & coaching on self management Written discharge instructions (with health literacy) Accurate medication reconciliation Facilitate timely post acute follow up Educate patients to know who to call for an issue Improve communication to the next level of care Boutwell A. Promising Approaches to Reduce ReHospitalizations. Institute for Healthcare Improvement (IHI) 2009 National Transitions of Care Coalition. Improving Transitions of Care. September 2010
14 Institute for Healthcare Improvement recommends: Appropriate referral for home care Boutwell, A. Promising Approaches to Reduce Rehospitalizations. Institute for Healthcare Improvement. 2009
15 Who is a Potential Home Health Care Patient? Age / Gender 77 year old, female (64%) Income level over half are below $21,780 / year Health status Support Referral greater than four (4) diagnoses 90% had medication changes 61% are physically de conditioned 42% have urinary incontinence 39% have skin integrity problems (wounds) 50% have no primary care giver 35% come from inpatient facilities Caffrey C, et al. Home Health Care and Discharged Hospice Care Patients: United States, CDC, National Health Statistics Reports. Number 38, April 27, Medicare Payment Advisory Committee (MedPAC). Report to the Congress: Medicare Payment Policy Washington, DC: March 2011:Chapter 8 pp
16 Predictors for Referral to Post Acute Care Indicator Major walking restrictions More likely to refer: 6.5 x Who had no or intermittent help available Self rated health as fair poor Self rated health as good Remained in the hospital longer Multiple of co morbidities Higher depression scores 3.0 x 4.0 x 3.1 x 1.2 x 1.2 x 1.1 x Bowles KH, Holmes JA, Ratcliffe SA, et al. Factors Identified by Experts to Support Decision Making for Post Acute Referral. Nurs Res ; 58(2):
17 Predictors for Referral to Post Acute Care Indicator Major walking restrictions Who had no or intermittent help available Self rated health as fair poor Self rated health as good Remained in the hospital longer Multiple of co morbidities Higher depression scores More likely to refer: 6.5 x 3.0 x 4.0 x 3.1 x 1.2 x 1.2 x 1.1 x **Multiple medications / med changes Bowles KH, Holmes JA, Ratcliffe SA, et al. Factors Identified by Experts to Support Decision Making for Post Acute Referral. Nurs Res ; 58(2):
18 Medication Management/Reconciliation Medication adverse events 30% of patients one medication discrepancy D/C from the hospital One in five patients D/C to home experience an adverse event within 3 weeks of discharge 60% medication related and could have been avoided Medication errors harm an estimated 1.5 million people per year at a cost of $3.5 billion annually 18


19 Reduce Hospitalizations: A National Study to Reduce Avoidable Hospitalizations through Home Care
20 Delta Study Top 5 Strategies to Reduce Unplanned Hospitalizations 1. Fall Prevention 94.9% 2. Agency Awareness, Culture & Support 92.5% 3. Front Loading 89.0% 4. Medication Management 78.8% Hour Availability/Response System 78.5% Delta Health Technologies, LLC, Fazzi Associates, Inc. The Delta Study to Reduce Hospitalizations: A National Study to Reduce Avoidable Hospitalizations through Home Care.. January 2012
21 Findings Practices used by most successful and least successful agencies were nearly identical in frequency of use of the strategy They use the same strategies the same percentage of the time What distinguished successful agencies from unsuccessful agencies was not the strategy but, rather, how the strategy was implemented How not What Delta Health Technologies, LLC, Fazzi Associates, Inc. The Delta Study to Reduce Hospitalizations: A National Study to Reduce Avoidable Hospitalizations through Home Care.. January 2012
22 What can a Home Health Agency do to keep clients safe? Step 1 Step 2 Step 3 Step 4 Step 5 Assess & Identify who is at Risk Plan and implement appropriate interventions Develop patient Self Management skills Medication Reconciliation and Management Communicate and Coordinate
23 Risk Assessments Hospitalization Risk Assessment Fall Risk Assessment Emotional Risk (Depression) Assessment Pressure Ulcer Risk Assessment Diabetic Foot Assessment

24 Hospitalization Risk Assessment



25 OCS Predictive Risk Assessment Based on OASIS SOC responses Reported in 5 levels High, Moderate, Low Risk Drivers Important to discuss at SOC case conference with clinician Focus on drivers of risk
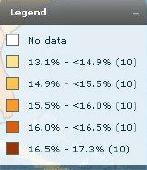
26 OASIS C Fall Assessment CMS Requirement: A multi factor falls risk assessment must include at least one standardized tool that has been validated as effective in identifying falls risk in community dwelling elders, and which includes a standard response scale. TUG Timed Up and Go Functional Reach
27

28 Self Management Skills Zone Tool for Fall Risk
29 Home Safety PlanTM

30 Degrees of Integration IOM (Institute of Medicine) Primary Care and Public Health: Exploring Integration to Improve Population Health. Washington, DC: The National Academies Press.

31 Self Management is a Partnership

32 Client Activation 32 Hibbard, J. Development of the Patient Activation Measure. Health Services Research 39:4, Part I, August 2004

33 Activation can be developed
 Health Tracking Household")
34 Patient Activation Center for Studying Health System Change (HSC) Health Tracking Household Survey 2007

35 Key program components Timely admission (24 hour Start of Care) Identification of ACH risk at start of care Interdisciplinary focus SN, PT, OT, ST, RD, MSW, HHA Individualized plan of care Client/Caregiver Education Frequent contact Home visit and/or phone call daily for first 7 14 days after start of care Specialized support tools

36 Holistic Approach American Physical Therapy Association, 2012










37 Eliminate medication discrepancies Improve communication among healthcare providers Improve timeliness of medical follow up Improve patient education Decrease deficiencies in health literacy 37
38 Thank you Deborah Perian, RN MHA CPHQ Regulatory & Quality Affairs BAYADA Home Health Care 38
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Connecting Therapy to Outcome and Process Measures: Moving from Concept to Reality
 Connecting Therapy to Outcome and Process Measures: Moving from Concept to Reality Presented By: Cindy Krafft MS PT Director of Rehabilitation Consulting Services President Home Health Section APTA August
Connecting Therapy to Outcome and Process Measures: Moving from Concept to Reality Presented By: Cindy Krafft MS PT Director of Rehabilitation Consulting Services President Home Health Section APTA August
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
A Tool for Maximizing Quality in Your Organization
 OASIS C: A Tool for Maximizing Quality in Your Organization Debbie Costello RN BSN MSM Director of Quality & Safety Caritas Home Care Session Outline Events leading to change in OASIS C Progress in home
OASIS C: A Tool for Maximizing Quality in Your Organization Debbie Costello RN BSN MSM Director of Quality & Safety Caritas Home Care Session Outline Events leading to change in OASIS C Progress in home
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations
 Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations Cindy Sun, MSN, RN Objectives At the conclusion of this session, the participant will be able to: Access
Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations Cindy Sun, MSN, RN Objectives At the conclusion of this session, the participant will be able to: Access
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Emerging Issues in Post Acute Care Trends
 Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
MediServe. More than 25 Years Serving the Rehab and Respiratory Communities
 MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
Accountable Care in Infusion Nursing. Hudson Health Plan. Mission Statement. for all people. INS National Academy of Infusion Therapy
 Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Outcome Based Case Conference
 Outcome Based Case Conference Are You On the Train or On the Tracks? Michelle Funk, RN BS, COS C 15 years RN 13 years Home Health Clinician Case Manager Program Coordinator Supervisor QA Coordinator Special
Outcome Based Case Conference Are You On the Train or On the Tracks? Michelle Funk, RN BS, COS C 15 years RN 13 years Home Health Clinician Case Manager Program Coordinator Supervisor QA Coordinator Special
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Basic Training: Home Health Edition. OASIS and Outcomes. April 2, 2013
 Basic Training: Home Health Edition OASIS and Outcomes April 2, 2013 Presented by: Rhonda Will, RN, BS, COS-C, BCHH-C, Assistant Director of the Competency Institute, Fazzi Associates, Inc. 243 King Street,
Basic Training: Home Health Edition OASIS and Outcomes April 2, 2013 Presented by: Rhonda Will, RN, BS, COS-C, BCHH-C, Assistant Director of the Competency Institute, Fazzi Associates, Inc. 243 King Street,
Care Coordination in the New CoP s. Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017
 Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
NDNQI Rhythms in Quality 2010 Data Use Conference
 NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
January 4, Via Electronic Mail to file code CMS-3317-P
 701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Measure Applications Partnership (MAP)
") Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule
 Calendar Year (CY) 2013 Final Rule") Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Last updated 11/13/12 Contact: Advocacy@apta.org Medicare Home Health Prospective Payment System (HHPPS) Calendar Year (CY) 2013 Final Rule Introduction COMPREHENSIVE SUMMARY On November 2, 2012, the Centers
Pave Your Path: How to Improve-Will, Ideas and Execution
 Pave Your Path This presenter has nothing to disclose Pave Your Path: How to Improve-Will, Ideas and Execution Cory Sevin, RN, MSN, NP Director, IHI Kate Bones, MSW Director, IHI February 19, 2013 Organization
Pave Your Path This presenter has nothing to disclose Pave Your Path: How to Improve-Will, Ideas and Execution Cory Sevin, RN, MSN, NP Director, IHI Kate Bones, MSW Director, IHI February 19, 2013 Organization
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Medical Home as a Platform for Population Health
 Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
CMS Proposed Home Health Claims-Based Rehospitalization and Emergency Department Use Quality Measures
 July 15, 2013 Acumen, LLC 500 Airport Blvd., Suite 365 Burlingame, CA 94010 RE: CMS Proposed Home Health Claims-Based Rehospitalization and Emergency Department Use Quality Measures To Whom It May Concern:
July 15, 2013 Acumen, LLC 500 Airport Blvd., Suite 365 Burlingame, CA 94010 RE: CMS Proposed Home Health Claims-Based Rehospitalization and Emergency Department Use Quality Measures To Whom It May Concern:
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
POST-ACUTE CARE Savings for Medicare Advantage Plans
 POST-ACUTE CARE Savings for Medicare Advantage Plans TABLE OF CONTENTS Homing In: The Roles of Care Management and Network Management...3 Care Management Opportunities...3 Identify the Most Efficient Care
POST-ACUTE CARE Savings for Medicare Advantage Plans TABLE OF CONTENTS Homing In: The Roles of Care Management and Network Management...3 Care Management Opportunities...3 Identify the Most Efficient Care
Implementation Guide: Critical Interventions in the First/Second Visit. VNAA Best Practice for Home Health
 Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
August 25, Dear Acting Administrator Slavitt:
 August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
Transitional Care and Preventing Readmissions in San Francisco
 Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs. Laura J. Dunlap, RN
 William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs Laura J. Dunlap, RN Background Research Questions Methods Results for North Carolina Results for Specific Counties
William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs Laura J. Dunlap, RN Background Research Questions Methods Results for North Carolina Results for Specific Counties
PPS Therapy. Medicare 2/28/ year Home Health clinician/contractor. 30 years Geriatric Rehab. Home Health consultant, author, speaker
 PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
PPS Therapy Changes 30 year Home Health clinician/contractor 30 years Geriatric Rehab Home Health consultant, author, speaker Progressive programming/clinical delivery Progressive management systems Home
The Reality of Health Care Reform: Accountable Care, Bundled Payments and Opportunities for Innovation
 The Reality of Health Care Reform: Accountable Care, Bundled Payments and Opportunities for Innovation May 11, 2010 Douglas A. Hastings Chair, Epstein Becker & Green, P.C. Member, Board on Health Care
The Reality of Health Care Reform: Accountable Care, Bundled Payments and Opportunities for Innovation May 11, 2010 Douglas A. Hastings Chair, Epstein Becker & Green, P.C. Member, Board on Health Care
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
PPS: The Big Picture
 PPS: The Big Picture Fall Conference, 2012 Presented by Karen Vance, OTR Supervising Consultant BKD, LLP Colorado Springs, Colorado kvance@bkd.com PPS: The Big Picture Industrial Revolution Urbanization
PPS: The Big Picture Fall Conference, 2012 Presented by Karen Vance, OTR Supervising Consultant BKD, LLP Colorado Springs, Colorado kvance@bkd.com PPS: The Big Picture Industrial Revolution Urbanization
Key points. Home Care agency structures. Introduction to Physical Therapy in the Home Care Setting. Home care industry
 Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
Introduction to Physical Therapy in the Home Care Setting Home Health Section of APTA Key points Home care industry Client populations Prospective Payment System (PPS) Physical therapy services Assessment
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses
 The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
The Promise of Care Coordination: Models That Decrease Hospitalizations and Improve Outcomes for Beneficiaries with Chronic Illnesses August 5, 2009 Center for Health Care Strategies Webinar Randall Brown,
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC. Month Day Year / / Month Day Year
 / / UHHC. Month Day Year / / Month Day Year") Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
 Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees") Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Medicare Part A Update
 Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
Medicare Part A Update Jennifer Bogenrief, JD Manager, Regulatory Affairs AOTA AOTA Specialty Conference: Effective Documentation Friday, September 12, 2014 1 Topics Medicare Therapy Documentation Requirements
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings.
 Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination
: Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination") Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Measure #46 (NQF 0097): Medication Reconciliation Post-Discharge National Quality Strategy Domain: Communication and Care Coordination 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: