Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility
|
|
|
- Ferdinand Simpson
- 5 years ago
- Views:
Transcription
1 Optimizing Patient Outcomes at the Transition of Care: From Inpatient to Skilled Nursing Facility Cynthia Williams, B.S.Pharm, FASHP Vice President/Chief Pharmacy Officer Riverside Health System, Newport News VA Katherine Koehl, Pharm D, BCPS, BSNSP System Director, Clinical Pharmacy Services PGY1 Residency Director Riverside Health System, Newport News VA
2 Disclosure Neither speaker has any relevant conflicts of interest to disclose
3 Learning Objectives Describe the difference in care transition needs from acute care to skilled nursing versus acute care to home List elements of best practice models demonstrated to improve transitions from acute care to skilled nursing facilities (SNF) Discuss potential medication safety risks with poor transition planning between acute and skilled nursing
4 Today s Agenda Transitions of care: background and challenges Acute to Post-acute toolkits Acute to Post-acute care practice models 4

5 Riverside Health System Overview


6 Riverside Health System Integrated Health Delivery Network Located in Southeastern Virginia





7 3 divisions Acute Care Services 45% 30% 25% 5 acute care hospitals 754 beds 3 specialty hospitals 222 beds Riverside Medical Group Medical home model 110 practices 565+ providers 35 specialties Lifelong Health 10 nursing homes 943 beds 4 PACE centers Helping 650 nursing home eligible participants stay in their homes In home health Home Health Home enabling technology House calls System Overview

8 Practice Reflection Question In your organization, how does the readmission rate from skilled nursing facilities compare with that of those discharged home? A. Higher B. Lower C. Not sure
9 Why are care transitions important? Adverse events and avoidable complications can occur due to poor communication and coordination among caregivers, health care professional, and the patient during care transitions 1 The quality of communication between the hospital and the nursing home is horrendous 2 1. American Medical Directors Association. Transitions of Care in the Long-Term Care Continuum Clinical Practice Guideline. Columbia, MD: AMDA Covinsky K The difficult transition between the hospital and nursing home, viewed 23 September 2015,
10 Challenges Frail, elderly population Increasing patient acuity in SNF Specialization of physician roles PCP Hospitalist/Specialist SNFist/LTC Medical Director Failure to understand needs of transitions partner Lack of integrated electronic health record between care settings
11 Background More than 5M individuals transition from hospitals to skilled nursing facilities annually Nurses in SNFs play primary role in receiving and initiating care Little work has been done on transitions from acute to SNF The primary processes at the receiving end must be better understood King BJ, Gilmore-Gykovskyi AL, Roiland RA et al. The Consequences of Poor Communications During Transitions from Hospital to Skilled Nursing Facility: A Qualitative Study. J Am Geriatr Soc. 2013; 61:
12 Background SNF nurses rely heavily on written hospital discharge communication Inadequacies include: Problems with medication orders Lack of opioid prescriptions for pain Little psychosocial or functional history Inaccurate information on current health status King BJ, Gilmore-Bykovskyi AL, Roiland RA et al. The Consequences of Poor Communications During Transitions from Hospital to Skilled Nursing Facility: A Qualitative Study. J Am Geriatr Soc. 2013; 61:
13 Missing/incomplete Conflicting Inaccurate Seeking, Reviewing, Gathering, Reconciling Working blindly Using caution Discovering inaccurate information Development of Plan of Care Poor Quality Hospital Discharge Info Implementation of Plan of Care Patient care delays Staff stress, frustration Increased workload Increased risk of readmission Increased risk of negative patient outcome Increased resident/ family dissatisfaction Negative SNF facility image/star rating
14 Key Elements to Ensure a Safe Care Transition Patient-centered care Effective communication Consistent discussion and documentation of end-of-life care preferences Education of patient and family about the reasons for transfer Consideration of the patient s individual preferences Prompt and consistent medication reconciliation AMDA. Improving Care Transitions Between the Nursing Facility and the Acute-Care Hospital Settings. March 2010
15 Communication at Transition of Care Recent literature has noted Inadequacies of hospital discharge summaries not mentioning 1 Outstanding lab tests Post-discharge testing Failure to identify a PCP or receiving physician 2 11% of discharge letters and 25% of discharge summaries never reaching PCP 1. Were MC, Li X, Kesterson J, et al. Adequacy of hospital discharge summaries in documenting tests with pending results and outpatient follow-up providers. J Gen Intern Med 2009; 24(9): Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer between hospital-based and primary care physicians: Implications for patient safety and continuity of care. JAMA 2007; 297(8):
16 Medication Reconciliation Medication changes from hospital admission to hospital discharge Approx. ½ of regularly used home medications were discontinued 1 Over 1/3 of omissions were considered to have the potential to cause moderate or severe discomfort or clinical deterioration Adverse drug events attributable to medication changes occurred in 20% of transfers between nursing homes and acute care hospitals 2,3 1. Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: Prevalence and contributing factors. Arch Intern Med 2005; 165(16): Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med 2003; 138(3): Boockvar K, Fishman E, Kyriacou CK, et al. Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med 2004; 164(5):
17 Care Transition Models: Acute to Post-Acute
18 SHM Post-Acute Care Transitions Toolkit Resources to help optimize transitions of care process between acute care and post-acute care Based on principles of quality improvement Interventions derived from Evidence-based medicine Experiences of institutional experts Includes Resources Innovations Innovation/Implementation_Toolkit/pact/Overview _PACT.aspx?hkey=dea3da3c db-a00f-89f07f accessed September 23, 2015.
19 SHM Post-Acute Care Transitions Toolkit Acquire cross-setting, institutional support for project Understand local post-acute care environment Development of cross-setting multidisciplinary team Focus on improved quality of care transitions at their organization Development of specific aims or goals (measurable, achievable) Standardize intervention pathway and protocols across settings Engaging patients and families Development of comprehensive education programs Innovation/Implementation_Toolkit/pact/Overview_PACT.aspx?hkey=dea3da3c db-a00f-89f07f accessed September 23, 2015.
20 SHM Post-Acute Care Transitions Toolkit Measure and Analyze Problem Identification Tools Tracking Performance Case and clinical level data Process and Outcome metrics Compliance with initiative protocols Readmission rates, including disease specific ED visit rates Mortality rates General nursing home quality measures ACO measures Innovation/Implemntation_Toolkit/pact/Overview_PAC T.aspx?hkey=dea3da3c db-a00f-89f07f accessed September 23, 2015.
21 SHM Post-Acute Care Transitions Toolkit Developing Interventions Discharge Documentation Post-discharge follow-up Medication Reconciliation SHM MARQUIS initiative Nursing Warm Handoff Physician Warm Handoff Innovation/Implementation_Toolkit/pact/Overvi ew_pact.aspx?hkey=dea3da3c db-a00f-89f07f accessed September 23, 2015.
22 SHM Post-Acute Care Transitions Toolkit Discharge Documentation Discharge checklist Medical records Transfer instructions/orders for next setting Including disease specific order sets Universal transfer forms/data sheets Contact information Schedule II-V prescriptions and hard to obtain specialty medications Health care directives (POLST) Transfer/discharge summary Innovation/Implementation_Toolkit/pact/Overvi ew_pact.aspx?hkey=dea3da3c db-a00f-89f07f accessed September 23, 2015.
23 Practice Model: Vanderbilt University CMS IMPACT grant (Improved Post-Acute Care Transitions) Transition intervention for Medicare patients transferring to 1 of 23 PAC in Nashville area Interdisciplinary Nurse transitions advocate meeting Includes patient, family, acute care and PAC Transfer-oriented medication reconciliation by clinical pharmacist Myers AP, Neal EB, Mixon AS. May Post-Acute Care Transitions: Time for Improvements, viewed 23 September 2015, ViewArticle.aspx?d_id=50&a_id=27515&ses=ogst
24 Practice Model: Vanderbilt University Clinical Pharmacist Role Reconcile transfer orders at discharge Create a medication management plan (MMP) for PAC providers. Includes Pre-hospital medications Medications to be ordered at the PAC facility Indications for each medications Over age 65, review of age inappropriate medications (Beers, high ACB risk) Last administration time for medications in acute care Side-by-side comparison allows for quick review of medications throughout the continuum of care Myers AP, Neal EB, Mixon AS. May Post-Acute Care Transitions: Time for Improvements, viewed 23 September 2015,
25 Practice Model: Vanderbilt University Focus on high risk medications Warfarin orders include: Indication for therapy and INR goal at least 3 days of INR history and plan for follow-up dosage history Target INR: Duration of Therapy: indefinite 2 days before discharge Day before discharge INR Warfarin given (mg) Held Held 2mg Day of discharge Myers AP, Neal EB, Mixon AS. May Post-Acute Care Transitions: Time for Improvements, viewed 23 September 2015, st
26 Practice Model: Vanderbilt University Focus on high risk medications Insulin Include blood glucose readings All scheduled and correction insulin administered Diuretics Daily serum creatinine Daily weight Prospective medication plan for other drugs as needed Titration schedules, monitoring plans, stop dates, warnings for patient specific problems Myers AP, Neal EB, Mixon AS. May Post-Acute Care Transitions: Time for Improvements, viewed 23 September 2015, st
27 Practice Model: Cedars-Sinai Enhanced Care Program Cedars-Sinai delivers care transitions services to 8 SNFs in their market Resulted in 25% reduction in 30-day readmissions Includes Nurse-practitioner led transitions Medication reconciliation Boudreau E. 4 March How Cedars-Sinai Made SNFs Its Readmission Partner. Viewed 23 September 2015,
28 Practice Model: Cedars-Sinai Nurse-practitioner led transitions Acts as lead liaison, communicating with SNF attending physician Inpatient care team Visit to patient in SNF within 24 hours of transition, then 1-2 times/week as needed Inter-Facility Transfer Report Inpatient notes and key pieces of hand-off information Boudreau E. 4 March How Cedars-Sinai Made SNFs Its Readmission Partner. Viewed 23 September 2015,
29 Practice Model: Cedars-Sinai Don t underestimate the value of medication reconciliation One of the largest problems was that there wasn t a single, clean medication list. [The SNFs] sometimes received multiple lists with different medication on them, and the SNF nurses had to try and reconcile them. Rita Shane, PharmD, FASHP, FSCHP Chief Pharmacy Officer Cedars-Sinai Medical Center Boudreau E. 4 March How Cedars-Sinai Made SNFs Its Readmission Partner. Viewed 23 September 2015,
30 Practice Model: Cedars-Sinai Medication Reconciliation Within hours of SNF admission, SNF admission medication list sent to Cedars-Sinai pharmacy department Pharmacist Reconciles SNF med list with acute discharge med list Clinically evaluates reconciled list Communicates issues to NP liaison Identification and correction of drug errors in 50% of participating patients Boudreau E. 4 March How Cedars-Sinai Made SNFs Its Readmission Partner. Viewed 23 September 2015,

31 Practice Model: Riverside Resident Pilot ToC Pharmacist RRMC Expansion Establish the model Define program metrics Sustain resident program Expand to additional clinical area Add ToC to all facility clinical areas Include all RHS post-acute facilities
32 Riverside: Phase I Transitions of Care Pharmacist Pilot Initial focus on Riverside acute care to Riverside SNF Engagement of multidisciplinary team from sending and receiving facilities Providers Care Management Nursing Pharmacy
33 Riverside: Phase I Development of standardized checklist Prior to day of discharge Home medication list validated IV to PO conversions Auto-substitutions identified Discuss anticipated discharge medications with provider Obtain hard copy prescriptions CII-V Compare anticipated medications to SNF stat box contents Initiate discharge medication reconciliation in pending status
34 Riverside: Phase 1 Development of standardized checklist Day of discharge Review/validate discharge med rec Coordinate with discharging nurse to administer any medications needed within 2 hours post transfer Focus on pain medication and antimicrobials Ensure any medications needed within 4 hours of transition located in facility stat box Completion of transition of care note/warm handoff Entry of PAC orders into SNF EHR as pending for receiving provider review
35 Riverside: Phase 1 Transition of Care Note Pain Management (Document PSR and pain regimen administration over past 24 hours) Diabetes Mellitus (Document BG, SSI requirements and basal insulin regimen over past 24 hours) Duration of Therapy & Indication (Antibiotics, anticoagulants) Warfarin INR Trend (Document last 3 INR and corresponding doses) Initial Supply (Document if any unit of use items have been sent with patient)
36 Riverside: Phase 1 Pilot design Focus on patients identified for transition from largest RHS acute to largest RHS SNF List provided through e discharge portal Staffed M F First 4 weeks: entire hospital focus Only focused on care transitions Week 5 forward: focus on single unit Role includes all pharmaceutical care functions plus care transitions
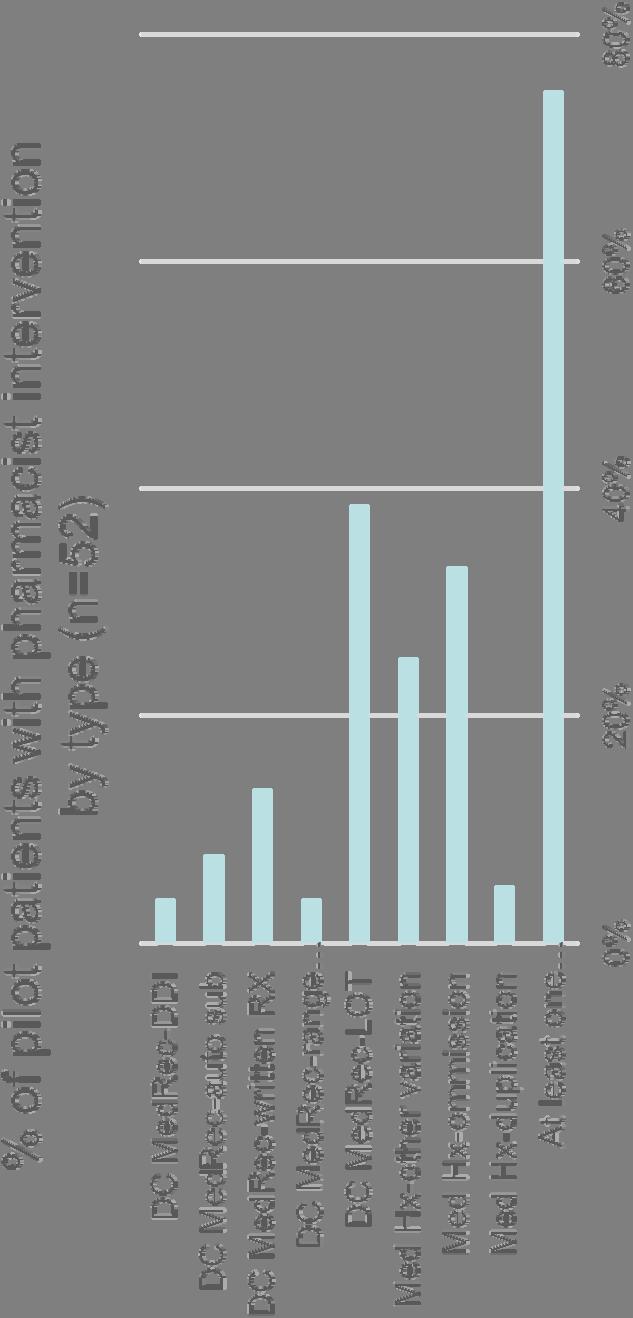
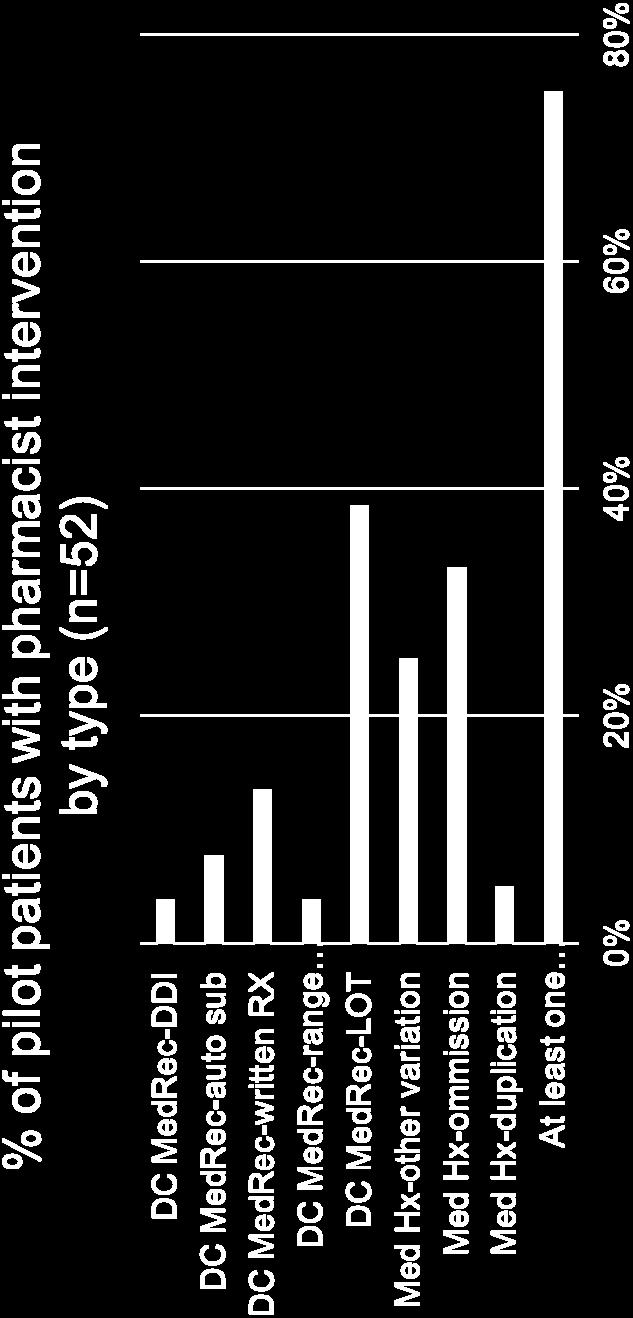
37 Riverside: Phase 1
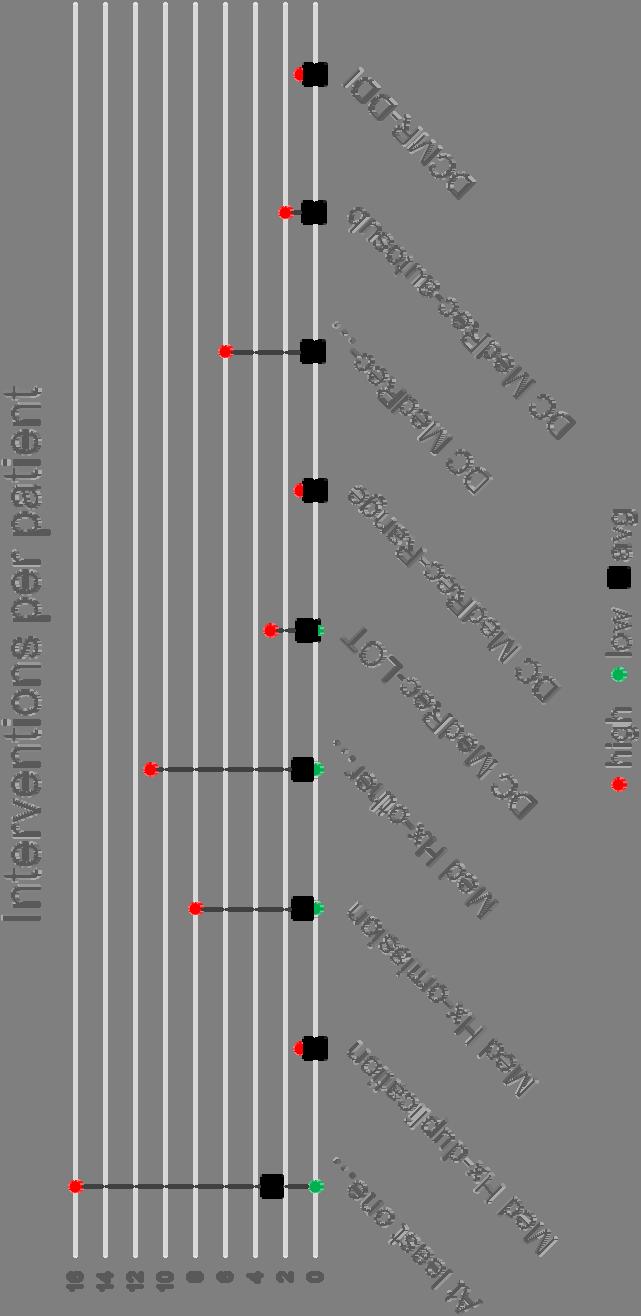
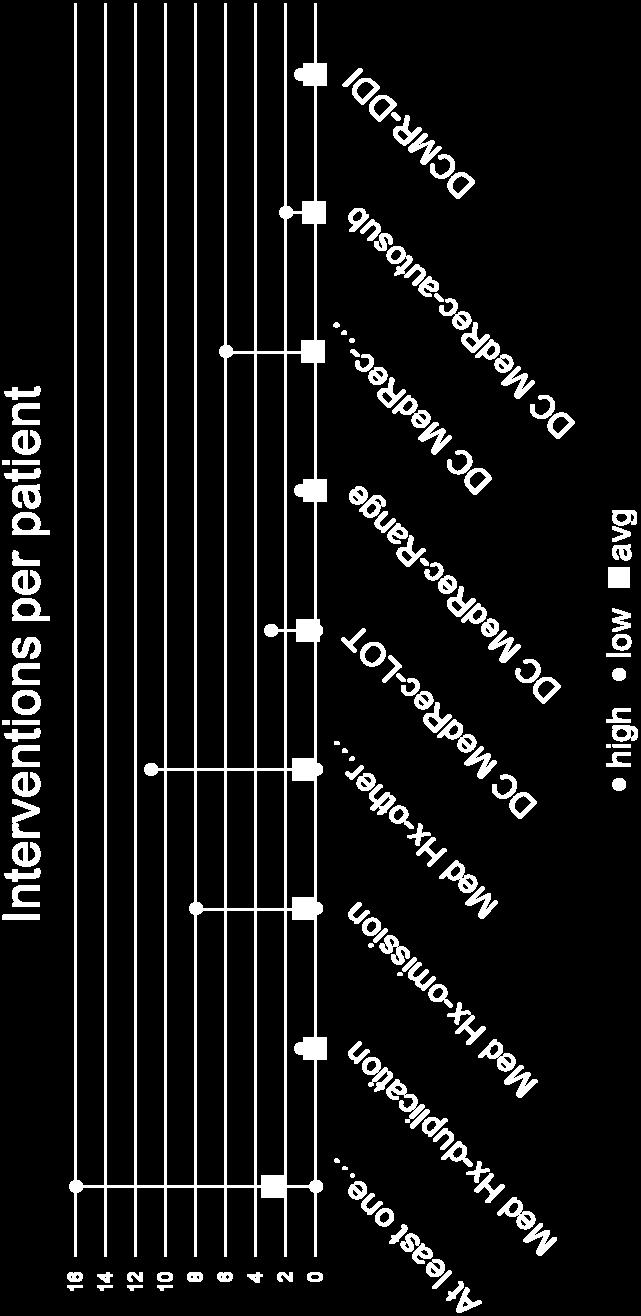
38 Riverside: Phase 1
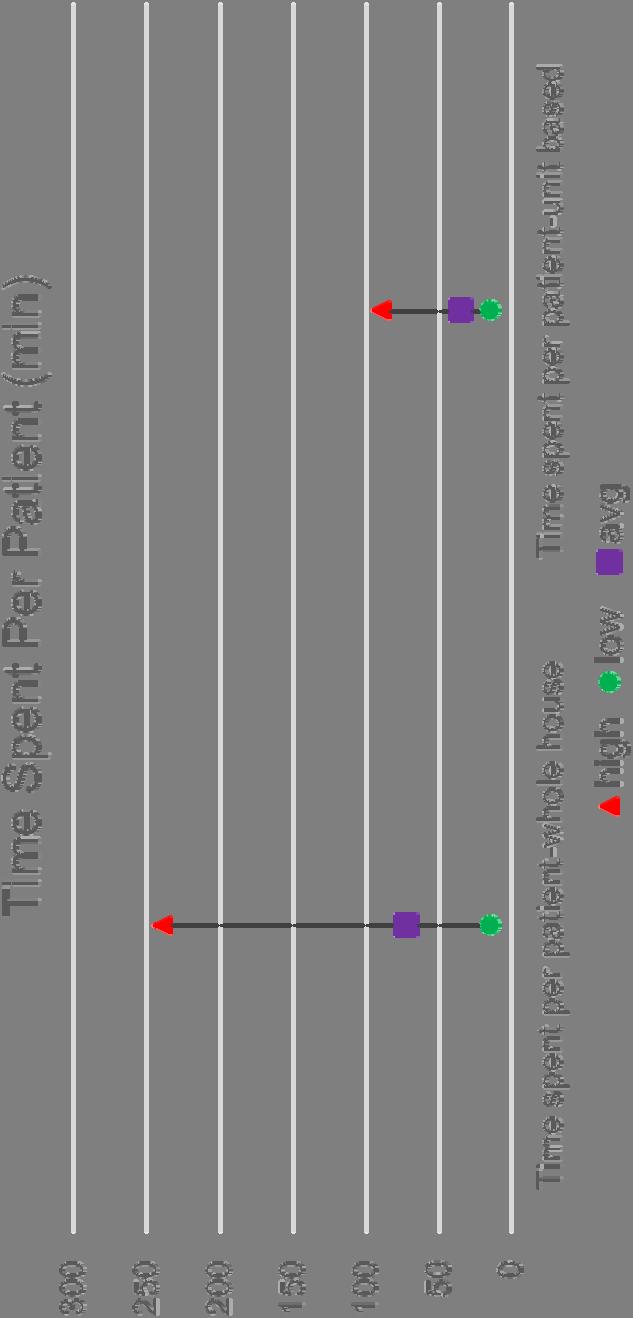
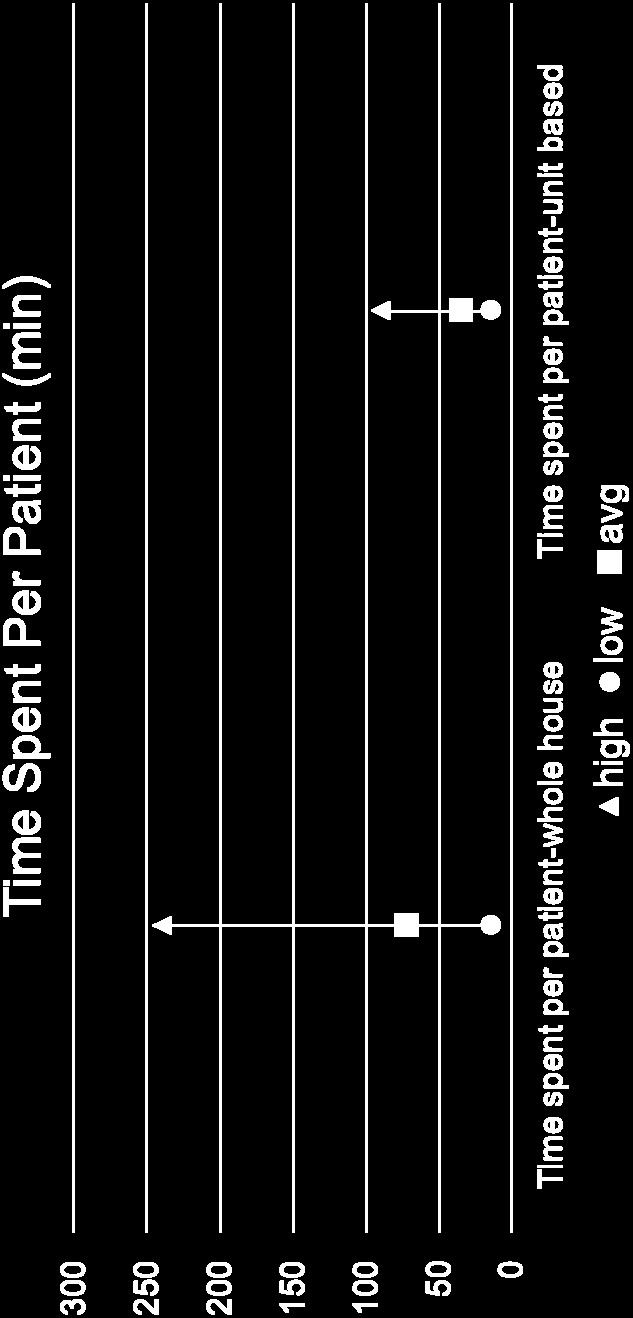
39 Riverside: Phase 1
40 Riverside: Phase 1 Additional results Enhanced provider and staff satisfaction at SNF Decreased time to availability of medications 14.6% readmission rate pilot versus 16.3% all patients (pilot hospital to pilot SNF) Lessons learned Need better method to identify patients for intervention Education of providers may remove workload some from pharmacist Incorporating into workflow of clinical teams more efficient than dedicated TOC pharmacist Activity peaks on Friday, so may need additional resources
41 Riverside: Phase 2 Established the Transitions of Care pharmacist as a permanent position Assigned one unit of clinical coverage Responsible for ToC activities for other units to one SNF Pharmacists gained efficiency over time ToC pharmacist added 15 more patients to clinical load Added ToC activities to another established clinical team
42 Riverside: Phase 3 Challenged to expand transitions of care service to all RHS post acute facilities with no additional staff Critically evaluated each clinical team Average daily patient load Patient length of stay Medical Complexity Consult volume (TPNs, kinetics, etc) Number of daily RHS post acute transitions Renamed Transitions of Care pharmacist to Medical/Surgical Team Emphasized that ToC responsibilities belong to everyone
43 Riverside: Phase 3 Changed the patient coverage map to balance clinical and transitions workload Created a buddy system to help with high volumes or timing issues Paired pharmacists are never in rounds at the same time Leverage relationship with pilot SNF physician champion Helped establish contacts at other facilities Spoke at RRMC provider committees to promote the transitions program and educate on transfer needs
44 Riverside: Phase 3 Next Steps Maintain program through electronic medical record (EMR) transition Use efficiencies gained through common EMR to add transition services to non RHS facilities Improve tracking of pharmacist time and intervention impact using tools in new EMR
45 Key Takeaways Resident projects are a great way to pilot new clinical services Utilize data to determine what model works for your organization Create a mechanism to support pharmacists Balance ToC with other clinical activities Post-acute provider champion is key Helps to educate and create demand Tell your story, share your success
46 Post-Acute Care Transition Resources Society of Hospital Medicine: Post-Acute Care Transitions Toolkit State Action on Avoidable Rehospitalizations (STARR) Program Pages/default.aspx Interventions to Reduce Acute Care Transitions (INTERACT) Minnesota Reducing Avoidable Readmissions Effectively (RARE) National Transitions of Care Coalition
47 Questions/Comments
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Key Words: Transitions of care, care coordination, medication management, drug therapy problem
 Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
How to Improve the Discharge Process. Michelle Mourad, MD Ryan Greysen, MD
 How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Pharmacists Role in Care Transitions
 Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Optimizing pharmaceutical care via Health Information Technology:
 Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy
 Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center Asst. Dean, Clinical Pharmacy, UCSF School of Pharmacy Describe the transformation of health-systems in response to
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Poor admission medication reconciliation can follow
 Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Shaping the Workforce of Tomorrow: Preparing Technicians for Advanced Roles
 Shaping the Workforce of Tomorrow: Preparing Technicians for Advanced Roles ASHLEE MATTINGLY, PHARMD, BCPS & SARAH LAWRENCE, PHARMD, MA, BCGP Speaker Contact Ashlee Mattingly, PharmD, BCPS Lab Pharmacist
Shaping the Workforce of Tomorrow: Preparing Technicians for Advanced Roles ASHLEE MATTINGLY, PHARMD, BCPS & SARAH LAWRENCE, PHARMD, MA, BCGP Speaker Contact Ashlee Mattingly, PharmD, BCPS Lab Pharmacist
Disclosures. Objectives. Leveraging and Developing Your Team for Optimal Outcomes. None
 Leveraging and Developing Your Team for Optimal Outcomes Michelle W. McCarthy, PharmD, FASHP Coordinator, Pharmacy Education and Graduate Programs Charlottesville, VA November 6, 2017 Disclosures None
Leveraging and Developing Your Team for Optimal Outcomes Michelle W. McCarthy, PharmD, FASHP Coordinator, Pharmacy Education and Graduate Programs Charlottesville, VA November 6, 2017 Disclosures None
Monday, October 24, :15 a.m. to 10:45 a.m. Great Halls 1 & 2
 Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
Expanding Pharmacy Impact: Transitional Care Management and Chronic Care Management Activity Number: 0217-0000-16-1118-L04-P 1.50 hours of CPE credit; Activity Type: A Knowledge-Based Activity Monday,
PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE
 PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE RAJEEV KUMAR MD FACP CHIEF MEDICAL OFFICER SYMBRIA OBJECTIVES Identify elements of key literature that describes post-hospital
PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE RAJEEV KUMAR MD FACP CHIEF MEDICAL OFFICER SYMBRIA OBJECTIVES Identify elements of key literature that describes post-hospital
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Implementation of Clinical Services at Various Institutions
 Implementation of Clinical Services at Various Institutions Niki Carver, Pharm.D., UAMS Medical Center Shannon Hays, Pharm.D., White Co Medical Melanie Claborn, Pharm.D., Veterans Healthcare System of
Implementation of Clinical Services at Various Institutions Niki Carver, Pharm.D., UAMS Medical Center Shannon Hays, Pharm.D., White Co Medical Melanie Claborn, Pharm.D., Veterans Healthcare System of
Background and Methodology
 Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting
 Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Disclosures. Learning Objectives 4/26/2017. Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic
 Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Disclosure. SwedishAmerican Hospital A Division of UW Health. Learning Objectives. Medication History. Medication History 2/2/2017
 Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
A Pharmacist Network for Integrated Medication Management in the Medical Home
 A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
ROTATION DESCRIPTION FORM PGY1
 ROTATION DESCRIPTION FORM PGY1 Rotation Title Medicine Intensive Care Unit (MICU) Level of Learner PY4 PGY1 PGY2 Preceptor(s) Stacy Campbell-Bright, Brian Murray Preceptor Contact Stacy.Campbell-Bright@unchealth.unc.edu;
ROTATION DESCRIPTION FORM PGY1 Rotation Title Medicine Intensive Care Unit (MICU) Level of Learner PY4 PGY1 PGY2 Preceptor(s) Stacy Campbell-Bright, Brian Murray Preceptor Contact Stacy.Campbell-Bright@unchealth.unc.edu;
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Marshall Digital Scholar. Marshall University. Brittany Snodgrass. Charles K. Babcock Marshall University,
 Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Marshall University Marshall Digital Scholar Pharmacy Practice & Administration Faculty Research 2013 The impact of a community pharmacist conducted comprehensive medication review (CMR) on 30-day re-admission
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Is the Discharge Information Received by PCP from Hospitals Adequate to Ensure the Continuity of Patients Care?
 Is the Discharge Information Received by PCP from Hospitals Adequate to Ensure the Continuity of Patients Care? Research Project By Suzette Bartosh, Deepa Khadka, Uchechi Okani, Abena Sarhene and Sukhraj
Is the Discharge Information Received by PCP from Hospitals Adequate to Ensure the Continuity of Patients Care? Research Project By Suzette Bartosh, Deepa Khadka, Uchechi Okani, Abena Sarhene and Sukhraj
Novel combined patient instruction and discharge summary tool improves timeliness of documentation and outpatient provider satisfaction
 701053SMO0010.1177/2050312117701053SAGE Open MedicineGilliam et al. research-article2017 Original Article SAGE Open Medicine Novel combined patient instruction and discharge summary tool improves timeliness
701053SMO0010.1177/2050312117701053SAGE Open MedicineGilliam et al. research-article2017 Original Article SAGE Open Medicine Novel combined patient instruction and discharge summary tool improves timeliness
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project
 Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Best Practices for Safety & Care Coordination
 Best Practices for Safety & Care Coordination Thursday, February 23, 2016 Nicole Skyer-Brandwene MS, RPh, BCPS, CCP Adverse Drug Events Network Task Lead Andrew Miller, MD, MPH Care Coordination Network
Best Practices for Safety & Care Coordination Thursday, February 23, 2016 Nicole Skyer-Brandwene MS, RPh, BCPS, CCP Adverse Drug Events Network Task Lead Andrew Miller, MD, MPH Care Coordination Network
Vanita K. Pindolia, PharmD Vice President, Ambulatory Clinical Pharmacy Program. Detroit, Michigan
 PCMH Best Practices Vanita K. Pindolia, PharmD Vice President, Ambulatory Clinical Pharmacy Program Henry Ford dhealth lthsystem Detroit, Michigan Faculty Disclosure The faculty reported the following
PCMH Best Practices Vanita K. Pindolia, PharmD Vice President, Ambulatory Clinical Pharmacy Program Henry Ford dhealth lthsystem Detroit, Michigan Faculty Disclosure The faculty reported the following
Home Assessments Resulting in a Positive Effect on Outcome Score Cards
 Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
2017 ASHP Proposed Policies: To Approve or Not to Approve, That is the Question. Disclosures. Learning Objectives 3/16/2017
 2017 ASHP Proposed Policies: To Approve or Not to Approve, That is the Question Nicole Allcock, PharmD, BCPS, FASHP Noelle RM Chapman, PharmD, BCPS, FASHP Joel Hennenfent, PharmD, MBA, BCPS, FASHP Jen
2017 ASHP Proposed Policies: To Approve or Not to Approve, That is the Question Nicole Allcock, PharmD, BCPS, FASHP Noelle RM Chapman, PharmD, BCPS, FASHP Joel Hennenfent, PharmD, MBA, BCPS, FASHP Jen
Medication Reconciliation
 Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Medication Adherence
 Medication Adherence Robert DiGregorio, PharmD, FNAP, BCACP Professor (Long Island University) Sr. Director, Pharmacy & Pharmacotherapy Services (TBHC) Chief, Pharmacotherapy Department of Internal Medicine
Medication Adherence Robert DiGregorio, PharmD, FNAP, BCACP Professor (Long Island University) Sr. Director, Pharmacy & Pharmacotherapy Services (TBHC) Chief, Pharmacotherapy Department of Internal Medicine
Impact of an Innovative ADC System on Medication Administration
 Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service
 Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Heart Failure Nurse Practitioner Role Development and Proposal. Anita M. Wilson, BSN, RN. ACNP, DNP Student Creighton University
 1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
1 Heart Failure Nurse Practitioner Role Development and Proposal Anita M. Wilson, BSN, RN ACNP, DNP Student Creighton University PO Box 21 Kingsley, IA 51028 abwilson@frontiernet.net 712-490-8347 Mary
Improving Clinical Outcomes
 Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, :00 5:00 PM
 ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
4/9/2013. Best Practice Initiative: Inpatient Anticoagulation Stewardship. Dorcas Letting reports no relevant financial relationships
 Disclosure Best Practice Initiative: Inpatient Anticoagulation Stewardship Dorcas Letting reports no relevant financial relationships Dorcas Letting-Mangira, Pharm.D Pharmacotherapist, Internal Medicine
Disclosure Best Practice Initiative: Inpatient Anticoagulation Stewardship Dorcas Letting reports no relevant financial relationships Dorcas Letting-Mangira, Pharm.D Pharmacotherapist, Internal Medicine
Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6,
 Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6, 2009 Conference Purpose The purpose of the conference
Society of Hospital Medicine Medication Reconciliation: A Team Approach A Multi-disciplinary Conference AHRQ Sponsored Chicago, Illinois - March 6, 2009 Conference Purpose The purpose of the conference
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Adapting Practice to Keep Pace with Changes in Health Care. Change in Health Care. Professional Responsibilities?
 Accountable Care Innovations: Leading Medication Management Across the Continuum Adapting Practice to Keep Pace with Changes in Health Care Rick Couldry, M.S., FASHP University of Kansas Hospital Kansas
Accountable Care Innovations: Leading Medication Management Across the Continuum Adapting Practice to Keep Pace with Changes in Health Care Rick Couldry, M.S., FASHP University of Kansas Hospital Kansas
Pharmacy Technicians: Improving Patient Care through Medication Reconciliation
 Pharmacy Technicians: Improving Patient Care through Medication Reconciliation Disclosure I, Holly Katayama, have no financial relationships to disclose. Objectives Describe how to fully utilize pharmacy
Pharmacy Technicians: Improving Patient Care through Medication Reconciliation Disclosure I, Holly Katayama, have no financial relationships to disclose. Objectives Describe how to fully utilize pharmacy
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge
 Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
Pharmacy Technicians and Interns: Charting New Territory
 Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
MEDICATION THERAPY MANAGEMENT. MemberChoice FORMULARY MANAGEMENT MEDICATION THERAPY MANAGEMENT (MTM) SPECIALTY DRUG MANAGEMENT
 SPECIALTY DRUG MANAGEMENT") MemberChoice FORMULARY MANAGEMENT MEDICATION THERAPY MANAGEMENT (MTM) SPECIALTY DRUG MANAGEMENT MEDICATION THERAPY MANAGEMENT Medication Therapy Management 1 $ 290 Billion Wasted in avoidable costs due
MemberChoice FORMULARY MANAGEMENT MEDICATION THERAPY MANAGEMENT (MTM) SPECIALTY DRUG MANAGEMENT MEDICATION THERAPY MANAGEMENT Medication Therapy Management 1 $ 290 Billion Wasted in avoidable costs due
8/28/2018. Presentation agenda CURRENT STATE OF THE POST ACUTE PROVIDER SECTOR. Impact of The Medical Director in Preserving Your Future
 Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Importance of Clinical Leadership in Pharmacy
 Importance of Clinical Leadership in Pharmacy Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center, Los Angeles Assistant Dean, Clinical Pharmacy UCSF School of Pharmacy
Importance of Clinical Leadership in Pharmacy Rita Shane, Pharm.D., FASHP, FCSHP Chief Pharmacy Officer Cedars-Sinai Medical Center, Los Angeles Assistant Dean, Clinical Pharmacy UCSF School of Pharmacy
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW
 CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Pharmacy Services Providing Value In An Accountable Care Organization
 Presentation Outline Pharmacy Services Providing Value In An Accountable Care Organization The Fairview i Experience Pamela Phelps, Pharm.D., FASHP Director, Clinical Pharmacy Services Fairview Health
Presentation Outline Pharmacy Services Providing Value In An Accountable Care Organization The Fairview i Experience Pamela Phelps, Pharm.D., FASHP Director, Clinical Pharmacy Services Fairview Health
REPORT OF THE COUNCIL ON MEDICAL SERVICE
 REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
REPORT OF THE COUNCIL ON MEDICAL SERVICE CMS Report -I- Subject: Presented by: Referred to: Hospital Discharge Communications Peter S. Lund, MD, Chair Reference Committee J (Candace E. Keller, MD, Chair)
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
Caring in the Carolinas 11/5/2016
 The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest
The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest