Improving Care Transitions: Creating Your Evidence-Based Approach
|
|
|
- Scarlett Anderson
- 6 years ago
- Views:
Transcription


1 Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor UCSF Dept. of Family and Community Medicine Elizabeth Davis, MD Medical Director of Care Coordination, San Francisco Health Network Primary Care San Francisco General Hospital Assistant Clinical Professor UCSF Dept. of General Internal Medicine

2 Disclosures

3 Outline Readmissions vs Care Transitions Quality Improvement Drivers Connecting the Best Case Models Our Work in Progress Current Understanding and Vision
4 Readmission Basics In 2011: 3.3 million 30 day readmissions among adults in US Medicare national average 18% COPD 17-25% Myocardial Infarction 20% Pneumonia 18% Heart Failure 25% Medicare cost: $15 to $17 billion per year SFGH all cause readmission rate : 12.6%
5 Readmissions: A Complicated Metric Definition: is 30 days an appropriate timeframe? Data: no comprehensive source, easier to get subgroup data Universal access leads to increased utilization (esp. among lower SES) Risk adjustment: similar % s between systems if control for patient characteristics Preventable? 23-30% readmissions appear to be avoidable No national consensus on preventability or approach
6 Can readmissions be prevented? Goals: Identify patients at high risk of re-hospitalization and target specific interventions to mitigate potential adverse events Reduce 30 day readmission rates Improve patient satisfaction scores and H CAHPS scores related to discharge Improve flow of information between hospital and outpatient physicians and providers Improve communication between providers and patients Optimize discharge processes Funding: >$2 million, via institutional, grant, federal and insurancebased funding Results to date: Decreased readmissions by 13% (Absolute reduction = 2%: 14.7% to 12.7%)
7 Should readmissions be a focus?? Effect on morbidity & mortality Eg. COPD readmission = independent mortality predictor (OR 1.85) Other studies (eg. Krumholz, JAMA 2013) have found little to no correlation Lost income & time in community Likely a negative psychosocial impact Hospital acquired risk ~10% risk of HAC/unnecessary inpatient day Krumholz JAMA 2013
8 But wait Hot off the presses!!!
9 Readmissions as an accountability measure: Patient and health systemcentered benefit can be achieved through improved transitions of care. Adapted from Health Policy blog of Ashish Jha MD, Harvard School of Public Health

10 National Drivers of Care Transitions QI CMS penalty up to 3% of yearly hospital reimbursement HCAHPS Patient Satisfaction Community SFHP P4P bonus to PCMH s Hospital/Individual Optimal, patient-centered care

11 From Reducing Readmissions, produced by US DHHS, Partnership for Patients
12 External Guidelines & Regulatory Requirement Biomedical Mental Health Food Security/ Nutrition Comprehensive Patient Care Health- Related Behaviors Housing and Domestic Safety Issues of Cognition & Capacity Family Systems


13 Hospital Community Key Components of Ideal Transitions of Care K. Oza MPH, adapted from Burke et al JHM 2013


14 10 Building Blocks of High Performing Primary Care Bodenheimer et al (2014)

15 San Francisco Health Network San Francisco s only complete care system Primary care for all ages Dentistry Emergency & trauma treatment Medical & surgical specialties Diagnostic testing Skilled nursing & rehabilitation Behavioral health
16 San Francisco General Hospital and San Francisco s public hospital Devoted to care of the city s most vulnerable residents Sole provider of trauma and psychiatric emergency services in SF Serves over 100,000 patients per year 16,000+ admissions/year 20% of the city s inpatient care Trauma Center Average LOS adult inpatients is 5 days
17 Readmissions at SFGH SFGH All Cause 30-Day Readmission Rate Q1-13 Q2-13 Q3-13 Q4-13 Q1-14 Q2-14 Q3-14 Q4-14 Top 5 Discharge APR- DRG SFGH 30-Day Readm Rate (%) Goal (10.6%) SFGH 30-Day Readmit Rate (%, n) Repatriation program begins COPD* 25.8% (78) 20.8% Heart Failure* 24.8% (103) 20.0% Renal Failure 24.7% (44) 19.1% Sepsis 13.6% (67) 16.6% Cellulitis 11.3% (55) 10.2% AEH Public Hospitals 30-Day Readmit Rate 64% of readmitted patients have Medi-Cal coverage. 60% of readmitted patients have mental illness. 28% of readmitted patients have a substance use diagnosis. 16% of readmitted patients are homeless. 28% of readmitted patients are not empaneled with a PCP. 33% of readmissions occur within 7 days of discharge. 326 individuals accounted for 1734 hospitalizations & 764 readmissions (47% of all readmits). Data analysis by K. Oza MPH (SFGH Care Transitions Taskforce)
18 Team-Based Complex Care Planning


19 Morning multidisciplinary rounds on the UCSF Family Medicine Inpatient Service.

20


21 Brief, structured format for MD:nursing huddle and provider:patient discussion.
22 Cross-System Communication and Care Coordination

23 San Francisco Health Network J H Homeless and MCAH


24 Pharmacy Interventions and Medication Reconciliation
25 Vision for SFHN Primary Care Improve the health of the patients we serve Ensure excellent patient experience Sustainable Patient- and Family- Centered Care Optimize access, operations, and costeffectiveness Build a foundation of a healthy, engaged, and sustained primary care workforce
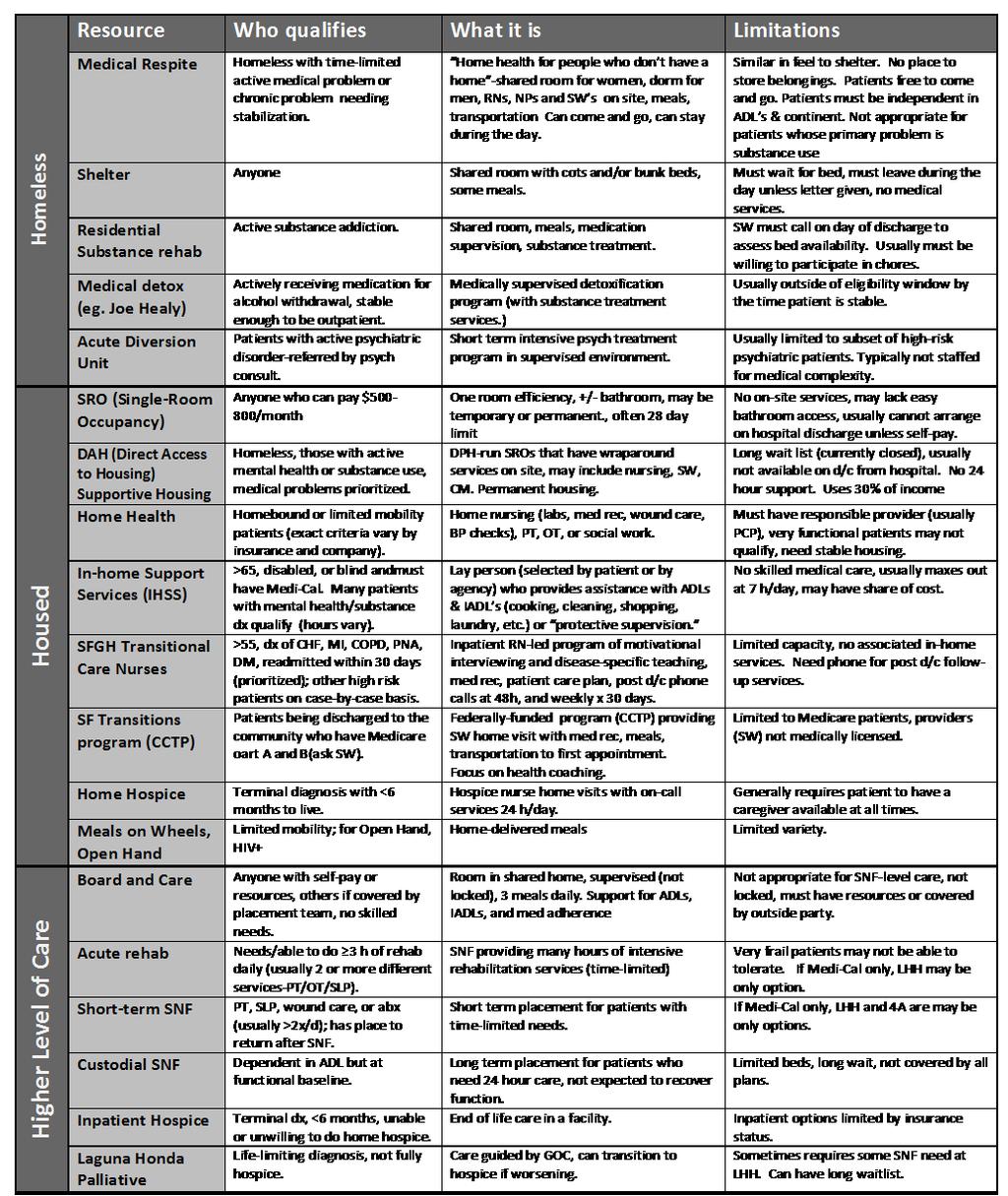
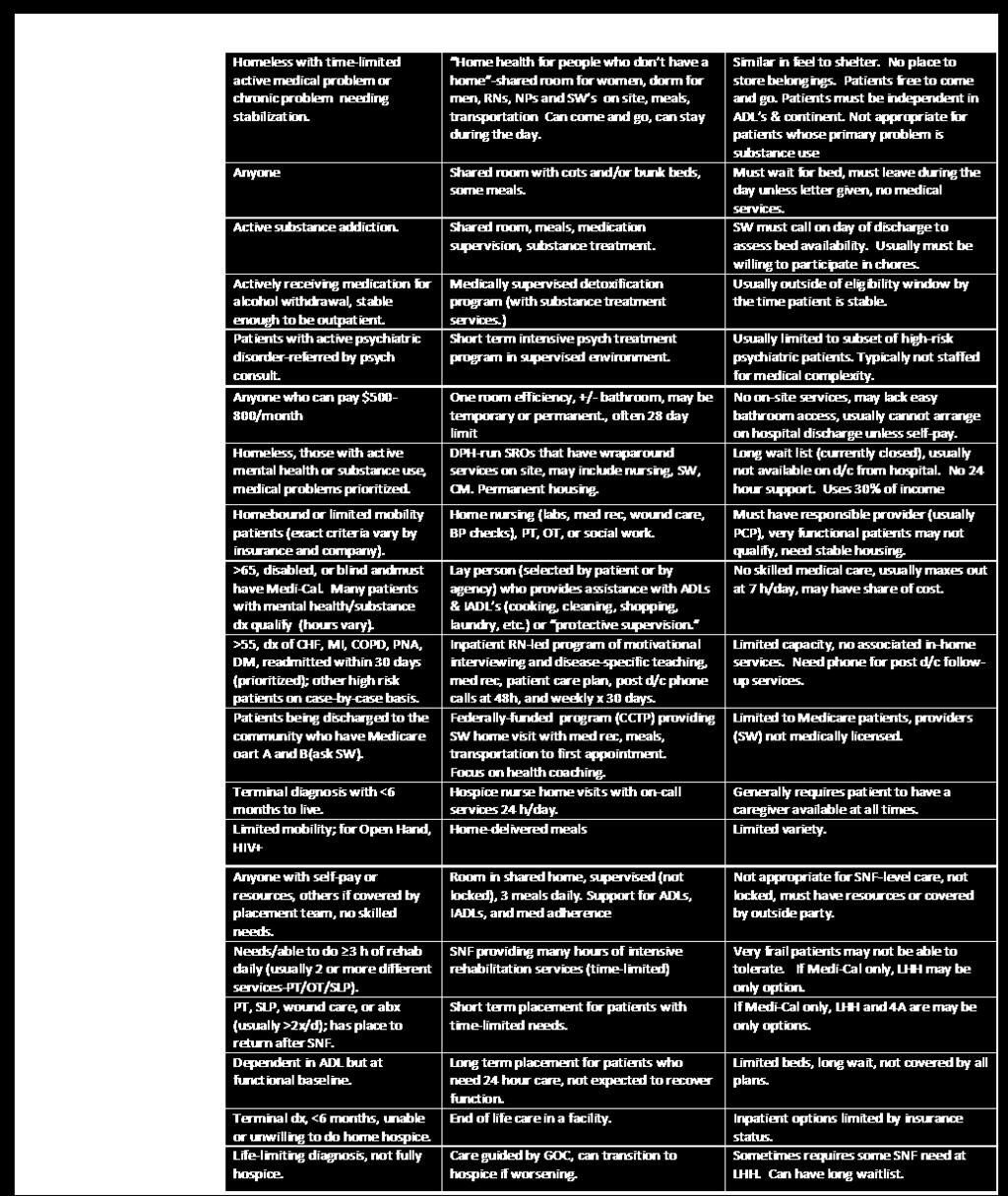
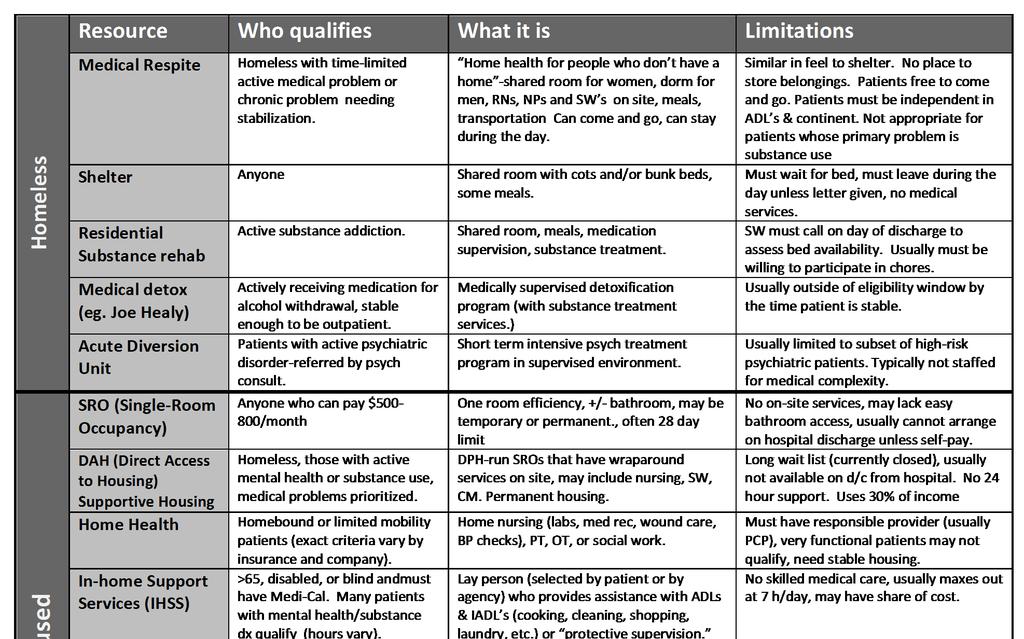
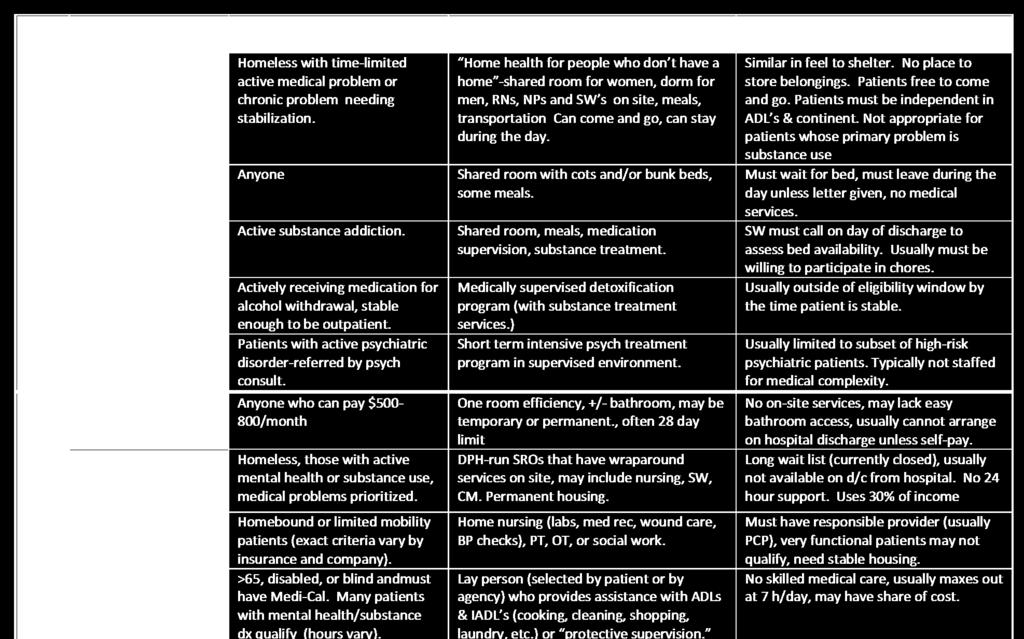
26 Improving Post-discharge care Standardization of post-discharge visits Timing Team based care Metrics for each health center Monthly rates of follow up within 7 days of d/c Readmission rates Services for high risk patients, such as case management, home health services, supportive housing, Bridge clinic, Respite, caregiver support
 Office 4F53 Office Phone 415-206-8651 / Fax 415-206-6135 HOSPITAL")
27 Dear Dr. Chase, Team Oriented Care Transition UCSF Family Medicine Inpatient Service San Francisco General Hospital Building 5 (Main Hospital) Office 4F53 Office Phone / Fax HOSPITAL ADMISSION NOTICE Communication of information Your patient Jane Smith MRN was admitted for COPD exacerbation. At admission, we found that she had run out of her inhalers and did not have any refills. She has been smoking cocaine every 2-3 days. She had hypercapnic respiratory failure in the SFGH ED and required urgent BiPAP. We plan to treat with steroids, bronchodilators, evaluate for pneumonia and provide cocaine cessation resources. We estimate that the patient will be discharged on: 5/1/2015 Follow-up appointments Primary care follow-up please reply with date and time for a visit within 7 days after the expected discharge date. Primary care clinic pharmacist/medication reconciliation visit should be scheduled for medication literacy teaching. Specialty clinic follow-up - please schedule appointment after the expected discharge date and reply with date and time: 1. Better breathing class Indication for referral: COPD 2. COPD NP Clinic Indication for referral: COPD Ambulatory & Community Referrals To communicate with us, please (1) reply to this and/or (2) page (before 7:30AM or after noon) using the table below. Sincerely, The FMIS team Bundled, -based care transitions communication.

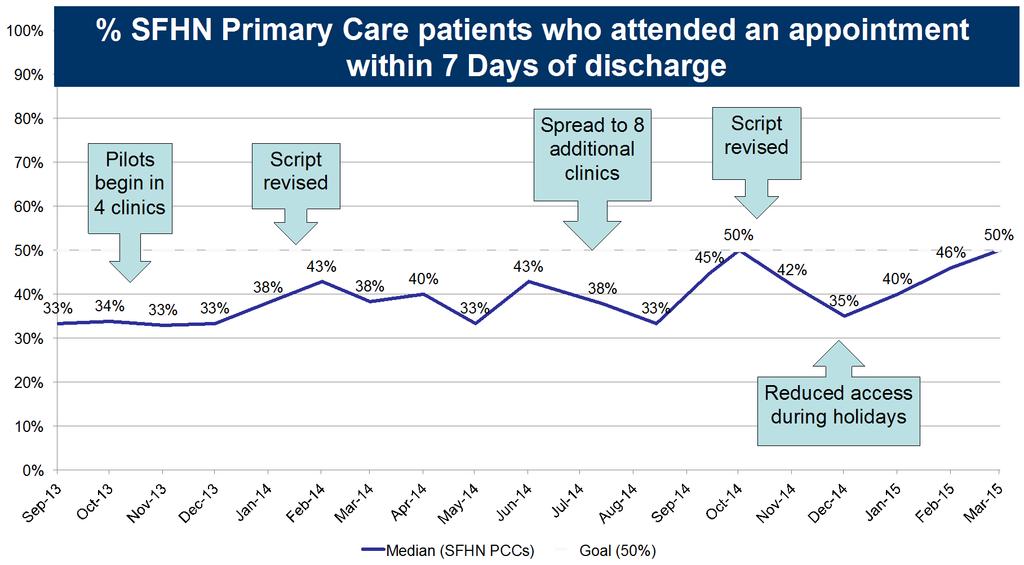
28 Family Medicine Inpatient Service (FMIS) vs all other SFGH Adult inpatient Services - Patients Attending Any Follow-Up Within 7 Days of DIscharge 70% 60% 50% 48% 51% 56% 55% 51% 52% 52% 40% 30% 20% 39% 34% 36% 36% 36% 32% 27% 27% 39% 35% 38% 43% 41% 44% 47% 48% 45% 10% FMIS Attended % SFHN Incentive Goal All Other SFGH Services Attended %

29 Post-discharge phone calls Call within 72 hrs of discharge HW, MA, or RN Scripted Appts Meds Red flags Primary care access

30 Complex Care Management
31 Patient Education and Supported Self-Management





32 SFGH Transitional Care Nursing Program Catheryn Williams RN Tip Tam RN Richard Santana RN Tami Lenhoff PharmD Spanish language self-management guide produced by the UCSF Center for Vulnerable Populations, 2007


33 Medication Instructions with Polyglot s Meducation TM 5 th to 8 th grade reading level Uses universal medication scheduling language & pictograms Can be translated into 18 different languages

34 Multilingual Heart Failure Education

35 Business Cards and Warmline



36 Building a Community of Support
37 Data Capture, Analysis and Metrics

38 SFGH Care Transitions Taskforce: a multidisciplinary QI workgroup aligning initiatives across continuum of care within and outside of SFGH and SFHN.

39 Care Transitions Discharge Worklist
40
41
42 SFGH 30-Day All-Cause Readmission Rate 30-Day Readmissions: SF Health Network (All clinic average)
43 Current Understanding Readmissions are complex & costly for patients and health systems Outcomes involve a diverse set of contributing factors, variable by patient, health system and community No consensus on exact definition of readmission or prevention Bigger win is to improve transitions of care Engage stakeholders, create high functioning teams, connect through efficient EBM processes, track & distribute data
44 Big Picture Goals 1. Team-oriented, standard-work approach for care transitions from hospital to community critical to align hospital and primary care. 2. Reduce total readmissions by 15-20% (the preventable component)




45 With thanks to the Moore Foundation, the SF General Hospital Foundation, the SFGH Care Transitions Taskforce, & our partners from SFGH and SFHN.
46 References Almagro P et al. Mortality After Hospitalization for COPD. Chest, 2002: 121(5): Balaban RB et al. A Patient Navigator Intervention to Reduce Hospital Readmissions among High-Risk Safety-Net Patients: A Randomized Controlled Trial. J Gen Intern Med Jul;30(7): Bodenheimer T et al. The 10 Building Blocks of High Performing Primary Care. Annals of Family Medicine Vol 12(2): Mar/Apr Burke RE et al. Contribution of Psychiatric Illness and Substance Abuse to 30-Day Readmission Risk. J Hosp Med Vol 8(8): Chen C et al. Readmission Penalties and Health Insurance Expansion: A Dispatch from Massachusetts. J Hosp Med: 2014 Nov 9(11). Hansen LO et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization J Hosp Med: 2013 Aug 8 (8). Horwitz L. The Insurance-Readmission Paradox: Why Increasing Insurance Coverage May Not Reduce Hospital-Level Readmission Rates. J Hosp Med: 2014 Nov 9(11). Jackson C et al. Timeliness of outpatient follow-up: an evidence-based approach for planning after hospital discharge. Ann Fam Med Mar;13(2):
47 Even More References Krumholz HM et al. Relationship Between Hospital Readmission and Mortality Rates for Patients Hospitalized With Acute Myocardial Infarction, Heart Failure, or Pneumonia. JAMA. 2013;309(6): Lavenberg J et al. Assessing Preventability in the Quest to Reduce Hospital Readmissions. J Hosp Med: 2014 Sept 9(9). Lindquist, LA et al. Primary Care Physician Communication at Hospital Discharge Reduces Medication Discrepancies. J Hosp Med Vol 8(12): Schnell K et al. The prevalence of clinically relevant comorbid conditions in patients with physician-diagnosed COPD: a crosssectional study using data from NHANES BMC Pulm Med Jul 9;12:26. Walsh C et al. Provider to provider electronic communication in the era of meaningful use: a review of the evidence. J Hosp Med Vol 8(10): An Ounce of Evidence -- Health Policy. Blog by Ashish Jha MD, Harvard Scholl of Public Health Hospitals Have High Rates Of Overall Readmissions, New Medicare Data Show:
 www.bu.")
48 Web Resources Institute for Healthcare Improvement America s Essential Hospitals Society for Hospital Medicine BOOST ProjectRED (Re-Engineered Discharge)


49 More Web Resources US Dept of Health and Human Services Partnership for Patients Hospital Consumer Assessment of Healthcare Providers and Systems Agency for Healthcare Research and Quality San Francisco Health Network
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager A HEALTHIER WORLD THROUGH BOLD INNOVATION
 Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
Over the past decade, team-based models of care have become
 INSIGHTS Email-Based Care Transitions to Improve Patient Outcomes and Provider Work Experience in a Safety-Net Health System JACK CHASE, MD, FAAFP, FHM; KARISHMA OZA, MPH; AND SETH GOLDMAN, MD ABSTRACT
INSIGHTS Email-Based Care Transitions to Improve Patient Outcomes and Provider Work Experience in a Safety-Net Health System JACK CHASE, MD, FAAFP, FHM; KARISHMA OZA, MPH; AND SETH GOLDMAN, MD ABSTRACT
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Version 1.0 (posted Aug ) Aaron L. Leppin. Background. Introduction
 Aaron L. Leppin. Background. Introduction") Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
UCSF Transitional Care Program. Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016
 UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
thequalitypost in this issue Get Out of Your Comfort Zone Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone
 thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Medication Error Reporting Program (MERP) Update. April 2010 *********************************************
 Update. April 2010 *********************************************") Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
Aurora will expand its geographic coverage within Wisconsin to achieve its mission to: Aurora Health Care 1991 Strategic Plan
 Objectives To describe the 20-year evolution of Aurora Medical Group within Aurora Health Care To identify the cultural characteristics necessary to improve patient access from the patient s perspective
Objectives To describe the 20-year evolution of Aurora Medical Group within Aurora Health Care To identify the cultural characteristics necessary to improve patient access from the patient s perspective
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER
 SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER 1 WHY IS SAN FRANCISCO GENERAL HOSPITAL IMPORTANT? and Trauma Center (SFGH) is a licensed general acute care hospital which is owned and operated by the
SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER 1 WHY IS SAN FRANCISCO GENERAL HOSPITAL IMPORTANT? and Trauma Center (SFGH) is a licensed general acute care hospital which is owned and operated by the
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Neighborhoods, resources and capacity to improve
 Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers
 Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Inpatient to Outpatient Transitions: Admissions, Discharges & Transfers Care Coordination Matters 15 th Annual Case Management Conference November 10, 2015 Christopher Kim, MD, MBA, SFHM Associate Medical
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Readmissions Moving beyond blame to fill the patient needs. Jackie Conrad RN, MBA, RCC Cynosure Health
 Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Care Coordination What Matters
 Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Center for Community Health Navigation at NewYork-Presbyterian Hospital
 Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
1. PROMOTE PATIENT SAFETY.
 SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
SAN FRANCISCO GENERAL HOSPITAL MEDICAL CENTER GOALS & ACCOMPLISHMENTS FISCAL YEAR 2006-2007 1. PROMOTE PATIENT SAFETY. Implemented medication reconciliation processes and procedures for admitted patients.
Presentation Summary
 SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER ANNUAL REPORT Fiscal Year 2011-2012 1 Presentation Summary SFGH Strategic Plan Update Environment of Care Report Approval Requested Provision of Care Policy
SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER ANNUAL REPORT Fiscal Year 2011-2012 1 Presentation Summary SFGH Strategic Plan Update Environment of Care Report Approval Requested Provision of Care Policy
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
New pharmacy practice opportunity: Enhancement of the transitions of care process
 New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
New pharmacy practice opportunity: Enhancement of the transitions of care process EMMA GORMAN, PHARMD CLINICAL ASSISTANT PROFESSOR DEPARTMENT OF PHARMACY PRACTICE D YOUVILLE SCHOOL OF PHARMACY BUFFALO,
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future
 Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future Arnold Epstein MSU 2018 Health Care Policy Conference April 6, 2018 The Good Ole Days 2 Per Capita National Healthcare
Delivery System Reform The ACA and Beyond: Challenges Strategies Successes Failures Future Arnold Epstein MSU 2018 Health Care Policy Conference April 6, 2018 The Good Ole Days 2 Per Capita National Healthcare
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Facilitating Teamwork Improves the Quality of Inpatient Care
 Facilitating Teamwork Improves the Quality of Inpatient Care Graham McMahon MD MMSc, Ellen Clemence RN MSN & ITU Team; Depts. of Medicine and Nursing, Brigham and Women s Hospital & Harvard Medical School,
Facilitating Teamwork Improves the Quality of Inpatient Care Graham McMahon MD MMSc, Ellen Clemence RN MSN & ITU Team; Depts. of Medicine and Nursing, Brigham and Women s Hospital & Harvard Medical School,
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Improving the Health of Our Patients and Our Communities:
 Jason Jones, PhD Executive Director Kaiser Permanente, Southern California Patti Harvey, RN, MPH, CPHQ Senior Vice President Kaiser Permanente, Southern California Improving the Health of Our Patients
Jason Jones, PhD Executive Director Kaiser Permanente, Southern California Patti Harvey, RN, MPH, CPHQ Senior Vice President Kaiser Permanente, Southern California Improving the Health of Our Patients
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Issue Brief. Redefining Frequent Emergency Department Users
 Issue Brief Volume 1, Issue 1, April 2014 Redefining Frequent Emergency Department Users Abstract Frequent ED users are perceived to be a costly population that often abuse or misuse ED services due to
Issue Brief Volume 1, Issue 1, April 2014 Redefining Frequent Emergency Department Users Abstract Frequent ED users are perceived to be a costly population that often abuse or misuse ED services due to
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Title. SF Health Network Telephone Communication Program. Subtitle. Antenor Arenas Director, Centralized Call Center
 SF Health Network Telephone Communication Program December 15, 2015 Antenor Arenas Director, Centralized Call Center Title Anna Robert, RN, DrPH Director of Care Coordination Subtitle 1 Overview Organizational
SF Health Network Telephone Communication Program December 15, 2015 Antenor Arenas Director, Centralized Call Center Title Anna Robert, RN, DrPH Director of Care Coordination Subtitle 1 Overview Organizational
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
San Francisco Whole Person Care California Medi-Cal 2020 Waiver Initiative
 San Francisco Whole Person Care California Medi-Cal 2020 Waiver Initiative Update April 3, 2018 Health Commission Maria X Martinez, Director Whole Person Care Barry Zevin, MD, Medical Director Street Medicine
San Francisco Whole Person Care California Medi-Cal 2020 Waiver Initiative Update April 3, 2018 Health Commission Maria X Martinez, Director Whole Person Care Barry Zevin, MD, Medical Director Street Medicine
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE. By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012
 PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
1. March RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 13.8%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
January 4, Via Electronic Mail to file code CMS-3317-P
 701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
701 Pennsylvania Ave., NW, Suite 800 Washington, DC 20004-2654 Tel: 202 783 8700 Fax: 202 783 8750 www.advamed.org Via Electronic Mail to file code CMS-3317-P Andrew M. Slavitt Acting Administrator Centers
2015 Quality Improvement Work Plan Summary
 2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
2015 Quality Improvement Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Transitional Care and Preventing Readmissions in San Francisco
 Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center San Francisco Transitional Care Program Carrie
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated