CareTrek : Nebraska s Journey to Safe Care Transitions
|
|
|
- Shavonne Hall
- 5 years ago
- Views:
Transcription



1 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement Organization for Nebraska, under contract with the Centers for Medicare & Medicaid Services (CMS), a federal agency of the U.S. Department of Health and Human Services. The contents do not necessarily reflect CMS policy. 9SOW-NE-CT-133/0211
2 Welcome CIMRO of Nebraska Overview of Care Transitions CareTrek Evidence-Based Interventions CareTrek Implementation of Evidence-Based Interventions 2
3 CIMRO of Nebraska Medicare Quality Improvement Organization for Nebraska Work under contract with CMS Work with healthcare providers to improve the quality of care delivered to people with Medicare 3
4 CIMRO of Nebraska CMS 9 th Scope of Work (9SOW) includes care transitions 14 QIOs were selected through a competitive process Nebraska s community: Omaha metro area Goal: improve healthcare transitions with the specific aim to reduce rehospitalizations Innovative and cutting-edge work 4

5 CMS Care Transitions Projects 5
6 Definition of a Care Transition Moving a person from one level of care to another Examples include: Hospital to home Hospital to skilled nursing facility Skilled nursing facility to home health care Home health care to hospital Poor care transitions lead to rehospitalizations 6
7 Rehospitalization is an Expensive Issue For the patient, family and Medicare Preliminary 2007 Medicare data analysis finds 1 of 5 beneficiaries are rehospitalized within 30 days of discharge from a hospital 7
8 Affordable Care Act Contains language regarding adjustment of payments to hospitals with high rates of potentially preventable Medicare readmissions for AMI/HF/PNE 8
9 The Ideal Rehospitalization Rate? Not all rehospitalizations are avoidable, but many could be avoided Heart failure, pneumonia, COPD, Acute MI are readmission leaders CABG, PTCA, other vascular procedures lead surgical conditions Nationally, 76% of readmissions are potentially avoidable - MedPAC Report to Congress,

10 National Attention to Readmissions 10
11 National Attention to Readmissions Just under 25% of hospital discharges to SNF are readmitted within 30 days Cost to Medicare in 2006 over $4 billion 11
12 Discharge Destination of Initial Hospitalization Home 58% Skilled Nursing Facility 22% Home Health 14% 12
13 CareTrek Nebraska s care transitions project The goal is to improve safety in care transitions for Medicare beneficiaries living in Douglas and Sarpy counties Bringing together providers from PPS hospitals, SNF, home health and community support services 13
14 CareTrek Overview Reduce hospital readmissions by improving transitions of care Interventions are evidence-based All beneficiaries discharged from seven full service hospitals in Douglas and Sarpy Counties 14
15 CIMRO of Nebraska s Role in CareTrek Identify the gaps in transition process Determine the root cause of the gap Determine the result of the gap Bring together groups to work on improving the gaps between sender and receiver Help to identify evidence-based interventions Measure the results 15
16 Evidence-Based Interventions Program or Toolkit Coleman Model of Coaching Transitional Care Model Better Outcomes for Older Adults through Safe Transitions Best Practices Intervention Package Interventions to Reduce Acute Care Transfers (INTERACT) Transforming Care at the Bedside Project RED (Reengineered Discharge) 16
17 Evidence-Based Interventions Cross-Setting Care Standardization Enhanced information at discharge Follow-up care established at discharge Medication management Plan of Care Telemedicine Telephone Follow-up Palliative Care 17
18 Evidence-Based Interventions Patient, Family and Caregiver Support Education Coaching Personal Health Record Community Supports 18
19 CareTrek Community Learning Groups 1. Hospital to SNF- Standard communication patterns 2. Hospital to Home Health Medication list management 3. Hospital Discharge Standardize and enhance discharge process 4. AHRQ/QIO Mini-Collaborative Medication Reconciliation 5. Coleman Model Care Coaching 6. Senior Leadership and Community Involvement 7. Caregiver education 19
20 Community Learning Groups: Cross Setting Communication and Medication Reconciliation Jennifer Geisert, RN, BSN Quality Improvement Advisor CIMRO of Nebraska
21 Community Learning Groups Care Transition: Key participants Sender Receiver Patient How is information communicated? Timely? User friendly? Complete? Available? 21
22 Cross Setting Group: Communication One hospital and four SNFs Participating staff includes nurse case manager, social worker, director of nursing, nurse unit manager and admission nurse 22
23 Identified Gaps Gaps in known & standard processes of transfer of patient Ambulance transfer availability, differing transfer forms and medication lists, no contact information from sender Gaps in transfer of information - leading to omissions in care EMR access, hospital discharge summary 23
24 Interventions Transition Mapping: Structured exchange visits between the hospital staff and the nursing staff to map the patient transfer process 24
25 Interventions (Continued) Health Information Technology (HIT): Identified a gap between the information provided by the hospital and the SNF ability to obtain this information Additional SNF staff were trained to use the system and access the information 25
26 Interventions (Continued) Chart Audits: SNF collecting readmission data, including reasons for medical instability & transfer to the hospital 26
27 Instructions for Using Transfer Tracking Tool Resident Identifier: Enter information that will not make the resident easily identifiable to others, but will help the facility to identify each resident (do not use resident name, social security number, Medicare number, date of birth) Admission Date: Enter the date the resident was admitted to the facility Medical Instability: Enter signs & symptoms or medical conditions that prompted the transfer to the hospital Reason for Hospital Transfer: Enter the factors that led to the decision to transfer the resident to the hospital 27
28 Tracking Tool.continued Date Transferred to Hospital: Enter the date the resident was transferred to the hospital Efforts to handle situation without transfer: Enter the interventions/efforts that were tried in the facility prior to the transfer Time of transfer: Enter the time of day the resident was transferred to the hospital 28
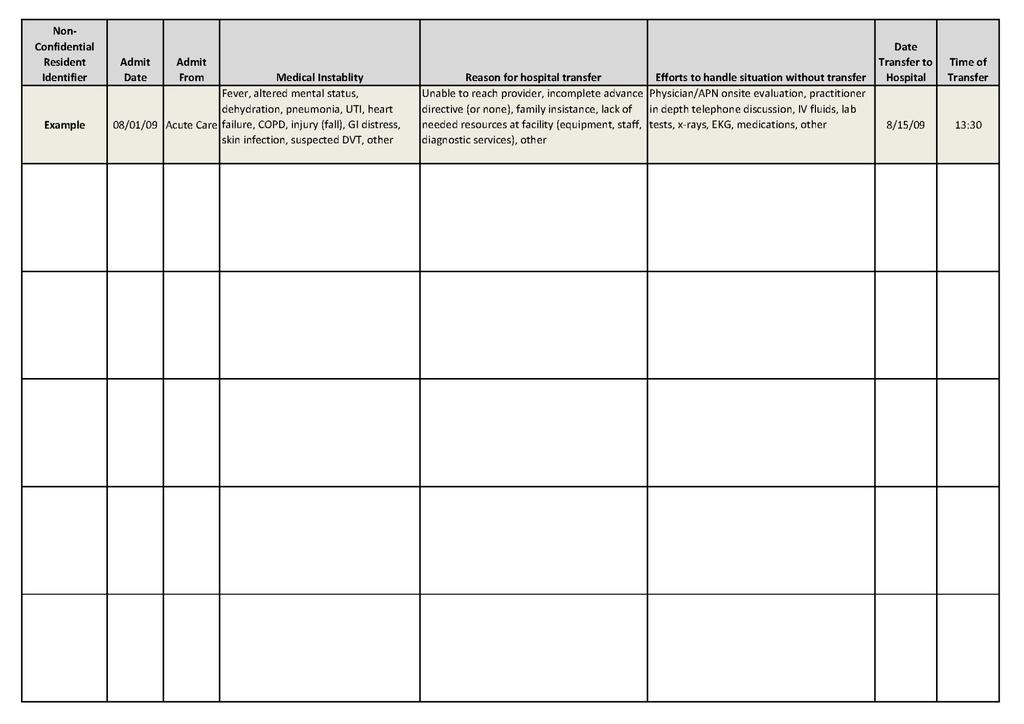
29 29
30 Identified Medical Instability September - October Chest Pain 3% Pain 8% Abnormal Lab 6% Respiratory Issues 21% Edema 1% Change in Vital Signs 17% Change in Mental Status 12% Availability of Services 17% GI Complaints 15% 30
31 Interventions (continued) Nurse-to-Nurse call: Communication implemented to provide handover information in a known and standard way 31
32 Interventions (continued) Educational Learning Sessions: The goal of the learning sessions is to improve communication skills and clinical competencies 32
33 Educational Learning Sessions cont Training focused on SBAR ( Situation- Background-Assessment-Recommendation) tools, management of diabetes, dyspnea, heart failure and the INTERACT II tool 33
34 INTERACT II: Interventions to Reduce Acute-Care Transfers INTERACT II: SBAR Situation, Background, Assessment, Recommendation Early Warning Tool: Stop and Watch Transfer Checklist Resident Transfer Form Transfer Form Quality Improvement tool Clinical Care Paths Change in Condition Cards Advanced Care Planning Tools 34
35 Educational Learning Sessions cont d Diabetes, CHF, Dyspnea and COPD Recorded WebEx Sessions: x 35
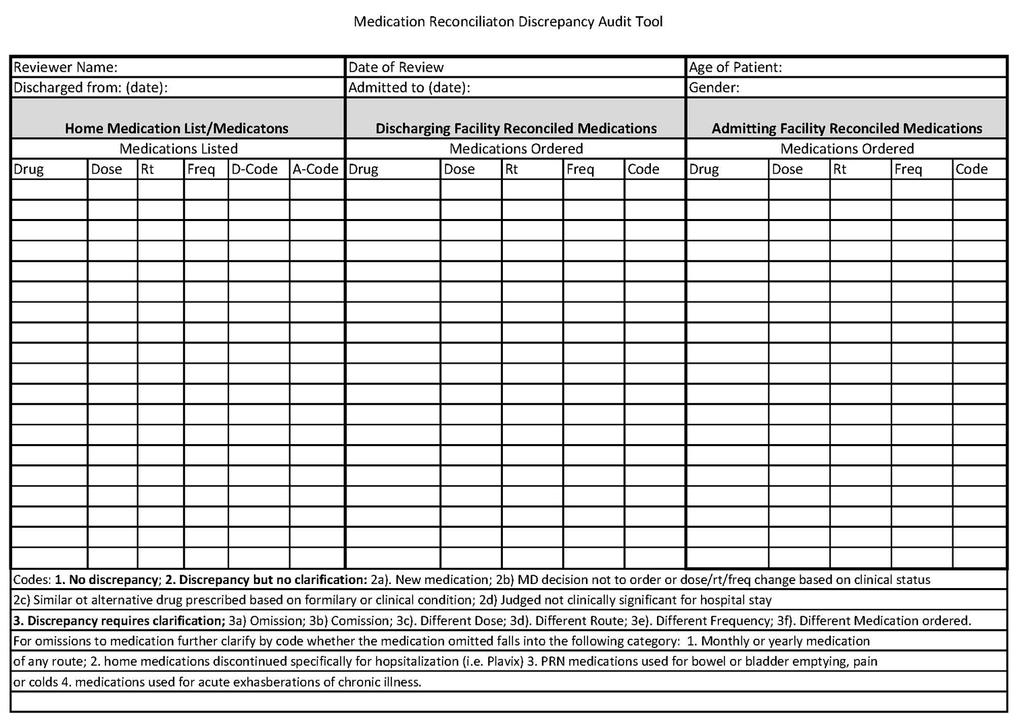
36 Community Learning Group: Medication Reconciliation National Patient Safety Goal #8: Accurately and completely reconcile medications across the continuum of care A process to compare the patient s current medications with those being ordered Communicate the reconciled list of medications to the next provider of services and the patient/caregiver 36
37 The Issue: Medication Reconciliation Coleman, Smith et al s (2005) study on Posthospital Medication Discrepancies found the 30- day re-hospitalization rate for patients with identified medication discrepancies on discharge was 14.3% and for those patients without a medication discrepancy, the rate was 6.1% 37
38 Medication Reconciliation Community Learning Group The group performed a mapping process that identified that SNFs were getting up to 7 different medication lists at transfer It was hard to identify which list was the most accurate and up-to-date. Multiple lists complicated the transfer and lead to errors in medication reconciliation 38
39 One True List Concept of the One True List was established The One True List was identified by the hospital and communicated to the SNF The One True List decreased the amount of medication discrepancies CIMRO of Nebraska produced a One True List toolkit as a resource 39
40 40
41 Models for Transitions of Care Paula Sitzman, RN, BSN Quality Improvement Advisor CIMRO of Nebraska
42 Models for Transitions of Care Care Transitions Intervention (CTI): (Dr. Eric Coleman) Re-Engineered Discharge (Project RED): Jack Transitional Care Model (CTM): (Mary Naylor) Transforming Care at the Bedside (TCAB): Institute for Healthcare Improvement (IHI) Project BOOST Home Health Quality Improvement (HHQI) Campaign 42
43 Care Transition Intervention (CTI) Care Transition Intervention Coleman Model Patient empowerment through patient activation Four pillars Medication self-management, Personal Health Record (PHR), MD follow-up, knowledge of red flags Transition Coach 30 days 43
44 Re-Engineered Hospital Discharge (Project RED) Discharge Advocate - APRN Eleven discrete, mutually-reinforcing components After Hospital Care Plan (AHCP) Pharmacist phone follow-up post discharge Phone reinforcement of AHCP 44
45 Discharge Advocate Educate patient Make f/u appointments Inform pt of tests Organized post-dc services Confirm medication plan Reconcile DC plan Review steps if problem arises DC summary to post DC providers Assess pt knowledge Give pt written AHCP Pharmacist phone reinforcement of DC plan & problem solve with pt 2-3 days post DC 45
46 Project RED One Omaha hospital implemented Initiated on the Telemetry Unit & focused on heart failure patients Spread to other hospital units 46
47 Transforming Care at the Bedside (TCAB) - IHI Guide focuses on Heart Failure Can be adapted to improve the DC process for all patients 47
48 TCAB Creating an Ideal Transition Home Enhanced admission assessment for postdischarge needs Enhanced teaching and learning Patient & family-centered handoff communication Post-acute care follow-up 48
49 Enhanced Admission Assessment for Post-Discharge Needs Include family caregivers and community providers as partners in assessment, DC planning & needs at home Reconcile medications upon admission Initiate plan of care based on assessment 49
50 Enhanced Teaching and Learning Identify the learner(s) on admission Redesign the patient education to improve patient and family caregiver understanding of self-care Use teach-back daily in the hospital and during follow-up phone calls 50
51 Patient and Family-Centered Communication Reconcile medications for discharge Provide customized, real-time information to the next provider that: Accompanies patient to next provider, or Is transmitted to the physician at time of discharge 51
52 Post-Acute Care Follow-up High-risk patients: Prior to DC, schedule a face-toface follow-up visit to occur within 48 hours of DC Moderate-risk patients: Prior to DC, schedule a follow-up phone call within 48 hours and schedule a physician office visit within 5 days 52
53 Transitional Care Model (TCM) Transitional Care Nurse APRN Comprehensive in-hospital planning Coordination and continuity of care Ongoing communication, education and support Post-hospital follow-up for 2 months 53
54 Transitional Care Nurse In-hospital assessment and development POC Coordination of care Regular home visit and telephone support for 2 months post-discharge Patient and caregiver education and support Nurse and physician collaboration 54
55 Transitional Care Model Participants Improvement in post-hospital discharge health outcomes Enhanced patient and family caregiver satisfaction Avoidance of re-hospitalization for primary and comorbid conditions Reduction in healthcare costs 55
56 Project BOOST BOOST Better Outcomes for Older adults through Safe Transitions Reduce 30-day readmissions Improve patient satisfaction Improve information between providers Identify high-risk patients & interventions Improve patient / family preparation for DC 56
57 Home Health Quality Improvement National Campaign (HHQI) Best Practice Intervention Packages: Reducing Acute Care Hospitalization (ACH) Medication Management Fall Prevention Cross Setting I Care Transitions across settings Cross Setting II Chronic Care Cross Setting III Medical Homes 57
58 Community Learning Group Home Health Agencies and Hospitals Gaps in information transfer leading to medication delays & errors Reconciled medication lists Sender/receiver communication 58
59 Community Learning Group One Hospital & four SNFs Lack of complete DC information in known & standard format that is understandable for postacute setting Collaboration to determine what was needed by SNF electronically generated transfer information 59
60 CareTrek Continues Share the successes of the community Promote & facilitate the One True List within the community CareTrek listserv Education Research palliative care best practices & share info CareTrek Toolkit Care Transitions fellows 60
61 Intervention References Colorado Foundation for Medical Care Care Transitions Intervention Project RED Project BOOST _CareTransitions/CT_Home.cfm 61
62 Intervention References cont d Transforming Care at the Bedside ngcareatthebedside.htm Transitional Care Model INTERACT II HHQI National Campaign 62
63 Contact Information CIMRO of Nebraska 1230 O Street, Suite 120 Lincoln, Nebraska P: F:
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Home Health and Care Transitions. Objectives. The Care Transitions Theme: 9/28/2010
 Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4
 Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Outline. I. Overview of QIO Care Transitions. II. Analyses: patient trajectory III. Palliative and end-of-life care
 Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
Wednesday May 19, 2010 Tom Ventura, MS, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract with the
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
February 27, Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models
 1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Home Health Infection Prevention Toolkit
 Home Health Infection Prevention Toolkit Paula Sitzman, RN, BSN Great Plains Quality Innovation Network Judy Riggert, RN, MS Visiting Nurse Association of the Midlands Map Great Plains Quality Innovation
Home Health Infection Prevention Toolkit Paula Sitzman, RN, BSN Great Plains Quality Innovation Network Judy Riggert, RN, MS Visiting Nurse Association of the Midlands Map Great Plains Quality Innovation
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Housekeeping. Harmony Healthcare International, Inc.
 Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Care Continuum or Unconnected Silos
 Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Reducing Avoidable Readmissions Within 30 Days of Discharge
 Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Reducing Avoidable Readmissions Within 30 Days of Discharge What We Know About Hospital Readmissions Approximately 20% of Medicare hospital discharges are followed by readmission within 30 days. 90% of
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
Improving Patient Safety Across Michigan and Illinois Designing Your Readmission Reduction Approach February 17, 2016 Agenda Peer to Peer Learning Network/Improvement Poster (Illinois) Designing your Readmissions
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Project RED (ReEngineering Discharge)
") Project RED (ReEngineering Discharge) Karla Weng, MPH, CPHQ RARE Networking Webinar September 29, 2011 HealthPartners Institute for Medical Education is accredited by the Accreditation Council for Continuing
Project RED (ReEngineering Discharge) Karla Weng, MPH, CPHQ RARE Networking Webinar September 29, 2011 HealthPartners Institute for Medical Education is accredited by the Accreditation Council for Continuing
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Faculty Presenters. The Care Transitions Program. STAAR Initiative
 Session M13 These presenters have nothing to disclose 26th Annual National Forum on Quality Improvement in Health Care Minicourse: Reducing Avoidable Readmissions by Creating a More Patient-Centered Transition
Session M13 These presenters have nothing to disclose 26th Annual National Forum on Quality Improvement in Health Care Minicourse: Reducing Avoidable Readmissions by Creating a More Patient-Centered Transition
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 1. Expedition Coordinator
 Thursday, June 6, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 1 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 6, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 1 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Lost in Transition. Definition. Objectives 9/22/2014
 Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Lost in Transition Eliza Borzadek, RN, Pharm.D., BCPS Idaho State University eliza@fmed.isu.edu ISHP Annual Fall Conference: September 26-28, 2014 Objectives 1. Describe the background and history of transitions
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
The Community based Care Transitions Program (CCTP)
") The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
MediServe. More than 25 Years Serving the Rehab and Respiratory Communities
 MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
How-to Guide: Improving Transitions from the Hospital to the Clinical Office Practice to Reduce Avoidable Rehospitalizations
 How-to Guide: Improving Transitions from the Hospital to the Clinical Office Practice to Reduce Support for the How-to Guide was provided by a grant from The Commonwealth Fund. Copyright 2012 Institute
How-to Guide: Improving Transitions from the Hospital to the Clinical Office Practice to Reduce Support for the How-to Guide was provided by a grant from The Commonwealth Fund. Copyright 2012 Institute
Roundtable on Health Literacy Institute of Medicine 17 March 2014
 Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
Project RED: Reengineering the Discharge Process Roundtable on Health Literacy Institute of Medicine 17 March 2014 Michael Paasche-Orlow MD, MA, MPH Associate Professor of Medicine Boston University School
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Use of Health Information Technology to Reduce Health Risk
 Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Use of Health Information Technology to Reduce Health Risk Sandra M. Foote Senior Advisor, Chronic Care Improvement Centers for Medicare & Medicaid Services September 9, 2005 The MHS Challenge Develop
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan
 Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan July 2015 Inpatient hospitalizations account for 32 percent of the total $2.9 trillion spent on health care in the
Acute Care Readmission Reduction Initiatives: An Update on Major Programs in Michigan July 2015 Inpatient hospitalizations account for 32 percent of the total $2.9 trillion spent on health care in the
An Innovative Approach to Identifying and Communicating Change of Condition
 An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
Reducing Readmissions: Care Transitions Toolkit
 Reducing Readmissions: Care Transitions Toolkit 2 nd Edition: February 26, 2014 Right Care at the Right Time in the Right Setting 1 P a g e Washington State Hospital Association - Partnership for Patients
Reducing Readmissions: Care Transitions Toolkit 2 nd Edition: February 26, 2014 Right Care at the Right Time in the Right Setting 1 P a g e Washington State Hospital Association - Partnership for Patients
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
 Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees") Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations. Aetna s Compassionate Care SM Program
 Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
Caring for Patients with Advanced and Serious Illnesses: Changing Medical Practice and Patient Expectations Aetna s Compassionate Care SM Program Our chief want in life is somebody who shall make us do
UCSF Transitional Care Program. Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016
 UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
Reducing Potentially Avoidable Hospitalizations of Nursing Home Residents
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Home Health Agencies & Reducing Readmissions. presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights
 Home Health Agencies & Reducing Readmissions presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights Objectives Describe the benefits of collaborating and utilizing
Home Health Agencies & Reducing Readmissions presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights Objectives Describe the benefits of collaborating and utilizing
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
improvement program to Electronic Health variety of reasons, experts suggest that up to
 Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Reducing Hospital Readmissions March/2017 The readmission rate for patients discharged to a skilled nursing facility is 25% within 30 days1. What can senior care providers do to reduce these hospital readmissions?
Continuing Education Disclosures
 Supporting CHF Patients in the Home Setting through a Comprehensive Community Approach Diane Schuh, RN, BSN Aurora Sheboygan Memorial Medical Center September 26, 2017 Continuing Education Disclosures
Supporting CHF Patients in the Home Setting through a Comprehensive Community Approach Diane Schuh, RN, BSN Aurora Sheboygan Memorial Medical Center September 26, 2017 Continuing Education Disclosures
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives