Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services
|
|
|
- Barry Wilson
- 5 years ago
- Views:
Transcription

1 Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical Officer Brookdale Senior Living
2 Learning Objectives Following this presentation, the participant will: 1. Understand the paradigm changes taking place in the American health system 2. Recognize the importance of post-acute care (PAC) providers in achieving quality care transitions and reducing avoidable hospital readmissions 3. Be able to define the triple aim of CMS to improve the quality of health care for older adults. 4. Understand the various innovative care models for improving care transitions, with particular attention to INTERACT 2
3 Speaker Disclosure Dr. O Neil is a full-time employee and shareholder of Brookdale Senior Living. 3
4 Disclaimer Re: CMS Health Care Innovations Award The project described was supported by Grant Number 1C1CMS from the Department of Health and Human Services, Centers for Medicare & Medicaid Services. The contents of this presentation are solely the responsibility of the author and do not necessarily represent the official views of the U.S. Department of Health and Human Services or any of its agencies. 4

5 Geriatrics is a TEAM Sport! It s a lot easier if we pull together! 5
6 Evolution of Accountable Care Year Milestones 2010 Affordable Care Act (ACA) enacted 2011 Center for Medicare Innovation Medicare Shared Savings Program 2012 Hospital readmission penalties Independence at Home Demonstration 2013 Bundled Payment Pilots New Medicare Tax Passive income Tax Excise tax on medical devices 2014 Health benefits exchanges Individual, employer mandate Independent Payment Advisory Board begins submitting recommendations 2015 Payment adjustments for hospital-acquired conditions 2016 Individual, employer penalties rise 2018 Excise tax on Cadillac health plans Courtesy: Advisory Board Company 6
7 Payment Reform Goal: tying 30% of traditional Medicare payments to quality or value through alternative payment models, such as Accountable Care Organizations (ACOs) or Bundled Payment arrangements by the end of 2016 Tying 50% of payments to these models by the end of HHS also set a goal of tying 85% of all traditional Medicare payments to quality or value by 2016 and 90% by 2018 through programs such as the Hospital Value Based Purchasing and the Hospital Readmissions Reduction Programs. First time in the history of the Medicare program that HHS has set explicit goals for alternative payment models and value-based payments. 7


8 Complex Patients Spurring Medicare Cost Growth Courtesy: Advisory Board Company 8

9 Prioritizing Population Health Interventions Courtesy: Advisory Board Company 9
10 Triple Aim of CMS Better health of populations Better care for individuals while lowering the percapita costs of care over time Improve the care experience 10
11 CMS Innovation Center The Innovation Center was established in 2011 Purpose: to test innovative payment and service delivery models to reduce program expenditures while preserving or enhancing the quality of care for those who receive Medicare, Medicaid, or Children s Health Insurance Program (CHIP) benefits. 11


12 12 Bundled Payments Drive Delivery System Integration Fee for Service Environment Individual Payments Reinforce Siloed Care Delivery Bundled Payment Environment Lump Sum Payments Drive Integration through Shared Accountability Payer Payer Physician Services Hospital Services Post Acute Services Physician Services Hospital Services Post Acute Services 12 Source: Health Care Advisory Board interviews and analysis.
13 New Paradigm Reimbursement will no longer be based on volume of services Based on performance metrics: Avoidable readmissions Disease quality metrics Health outcomes Patient and family satisfaction 13

14 Update on Accountable Care Organizations 14 Where the Medicare ACOs Are Courtesy: Advisory Board Company Source: Centers for Medicare and Medicaid Services; Health Care Advisory Board interviews and analysis.
15 Transitional Care Transitional care is defined as a set of actions designed to ensure the coordination and continuity of health care as patients transfer between different locations or different levels of care within the same location. Source: AGS Position Statement,
16 Communication The single biggest problem with communication is the illusion that it has taken place. -George Bernard Shaw 16
17 Why Focus on Care Transitions? 20% of Medicare beneficiaries readmitted within 30 days Negative physical, emotional, psychological impact Costs Medicare billions of dollars 1 $26 billion annually $17.5 billion on in-patient spending Avoidable hospitalizations/readmissions a key strategy 25-42% of readmissions are avoidable 2 1. Jordan Rau. Medicare Revises Hospitals Readmissions Penalties, Kaiser Health News. Oct. 2, Long-Term Quality Alliance. Improving Care Transitions: how quality improvement organizations and innovative communities can work together to reduce hospitalizations among at-risk populations. June
18 CMS Special Study in Georgia Expert Ratings of Potentially Avoidable Hospitalizations Based review of 200 hospitalizations from 20 NHs Was the Hospitalization Avoidable? Definitely/Probably YES Definitely/Probably NO Medicare A 69% 31% Other 65% 35% HIGH Hospitalization Rate Homes LOW Hospitalization Rate Homes 75% 25% 59% 41% TOTAL 68% 32% Ouslander et al: J Amer Ger Soc 58: ,
19 Major Problem Areas Acute change in condition Care transitions Medication management AMDA Conference,
20 Poor Transitions and ADEs ADEs are responsible for 5% to 28% of acute geriatric hospital admissions ADEs incidence: 26/1000 hospital beds In nursing homes, $1.33 spent on ADEs for every $1.00 spent on medications 350,000 ADEs in NHs each year Annual cost of ADEs in NHs is $7.6 billion 20
21 Impact on Hospitals More than 2000 hospitals have received readmission penalties Penalties: >$280 million Reputation Penalty : Hospital Compare website 21
22 Ineffective Transitions Wrong treatment Delay in diagnosis Severe adverse events Patient complaints Litigation Increased healthcare costs Increased length of stay Source: Australian Council for Safety and Quality in Health Care. Clinical hand-over and Patient Safety literature Review Report. March
23 Hospital Challenges Lack of control over PAC setting Gathering data on quality metrics and outcomes Collaboration with PAC providers that address hospital needs Limiting PAC networks to quality providers 23

24 CEO/CFO 78 million boomers turning 65 Where are my margins? CV procedures, hip/knee replacements Margins on frail older adults with unplanned hospitalizations flat or negative Rx: Keep my beds for the high-margin cases and find alternative quality locations for others CMO: The hospital can be a dangerous place for an older adult (e.g., delirium, HAIs, falls, pressure ulcers) 24
25 Post-Acute Care 40% of Medicare beneficiaries admitted to postacute and long-term care settings Skilled nursing, assisted living, and home care become critical to reducing re-hospitalizations Need to build collaborative relationships in the communities we serve Need to empower patients AND families 25
26 Co-Opetition Co-Opetition = Cooperation + Competition 26
27 Spotlight on Transitions Government: Quality Improvement Organization 9 th Scope of Work Joint Commission: including care transitions in accreditation requirements and in 2009 Patient Safety Goals ASIM: Step Up to the Plate Alliance safe, effective, patient-centered, timely, efficient, equitable service AGS: Position statement on care transitions AMA: passed a resolution submitted by AMDA Society of Hospital Medicine: Project BOOST AMDA: Created a Clinical Practice Guideline National Transitions of Care Coalition 27

28 Communication The single biggest problem with communication is the illusion that it has taken place. -George Bernard Shaw 28

29 Conceptual Model Source: National Transitions of Care Coalition 29
30 Overview of Transition Programs BOOST (Better Outcomes for Older Adults Through Safe Transitions) Project RED (Re-Engineered Discharge) Enhanced hospital discharge planning Care Transition Program Transition coach Trained volunteers Empowered patients and caregivers POLST (or MOLST ) (Physician (or Medical) Orders For life Sustaining Treatment) Advance care planning INTERACT is One of Several Evidence-Based Care Transitions Interventions High Quality Care Transitions for Older Adults & Caregivers Bridge Model Social Worker coordinating Aging Resource Center Services at hospital discharge Transitional Care Model APN coordinates care during and after discharge Home, SNF, and clinic visits INTERACT (Interventions to Reduce Acute Care Transfers) Communication Tools, Care Paths, Advance Care Planning Tools, and QI tools for nursing homes and SNFs 30 Slide used with permission of Dr. Joseph Ouslander
31 Overview of the INTERACT Quality Improvement Program Can help safely reduce hospital transfers by: 1. Preventing conditions from becoming severe enough to require hospitalization through early identification and assessment of changes in resident condition 2. Managing some conditions in the NH without transfer when this is feasible and safe 3. Improving advance care planning and the use of palliative care plans when appropriate as an alternative to hospitalization for some residents 31
32 INTERACT: A Quality Improvement Program Improvement Program Quality Improvement Tools Communication Tools Decision Support Tools Advance Care Planning Tools 32

33 Checklists 33

34 34 Stop and Watch

35 Interacting with Hospitals The NH to Hospital Transfer Form has two pages. The first page has information that ED physicians and nurses identified as essential to make decisions about the resident Consistent and clear clinical terms are used 35

36 Interacting with Hospitals The NH to Hospital Transfer Form has two pages. The second page has additional information that will be helpful to inpatient teams, and can be sent within 24 hours if the resident is admitted. 36
37 Interacting with Hospitals This Transfer Checklist can be printed or taped onto an envelope, and is meant to compliment the Transfer Form by indicating which documents are included with the Form 37


38 INTERACT Decision Support Tools: Change in Condition File Cards and Care Paths INTERACT Care Paths Acute Mental Status Change Change in Behavior: New or Worsening Behavioral Symptoms Dehydration Fever GI Symptoms nausea, vomiting, diarrhea Shortness of Breath Symptoms of CHF Symptoms of Lower Respiratory Illness Symptoms of UTI 38
39 Change in Condition File Cards The INTERACT Change in Condition File Cards are meant to be visible and sit next to the phone for quick reference 39

40 Interacting with Hospitals Information Transfer From the Hospital The Hospital to Post- Acute Care Transfer Form highlights Critical Time Sensitive Information But, there is no substitute for a warm handoff. 40
41 CMS Health Innovation Challenge Grant 3 Year Grant - Awarded July 1, 2012 to University of North Texas Health Science Center in partnership with Brookdale Goal: to revise and implement INTERACT Program in skilled nursing, assisted living, and home care settings 67 Brookdale Communities in Tampa Bay, Jacksonville, Dallas/Ft. Worth, Houston, Austin, San Antonio, Kansas City, and Denver Program to be shared and disseminated Expected savings of more than $9 million 41
42 SNF 30-Day Readmission Rate
43 SNF Hospitalization Rate: CMS Claims

44 Cost of Care: Skilled Nursing
45 INTERACT-AL and INTERACT-HH Now available at Include: Communication Tools Quality Improvement Tools Decision Support Tools Advance Care Planning Tools 45
46 Case History Madelyn O, 84 year old Past history: hypertension, atrial fibrillation, CHF Med: lisinopril, HCTZ, digoxin, warfarin Falls, fractures left hip Undergoes surgical repair Transferred to rehab. Warfarin held for prolonged INR
47 The Revolving Door After 2 week stay in rehab, transferred to assisted living Arrives with transfer papers, no discharge summary Med list does not include warfarin 1 week later, has sudden left-sided weakness and is transferred back to the hospital with an acute stroke. QUESTION: Was this preventable or not?
48 Assisted Living Landscape Fastest growing segment of elder care Over 31,000 ALFs 971,900 beds Acuity level has increased* 86% need assistance with taking meds 72% with bathing 57% with dressing 41% with toileting 36% with transferring 23% with eating *Source: National Center for Health Statistics,
49 INTERACT Assisted Living Version 1.0 Tools ng These are a modification of the INTERACT Quality Improvement Program 3.0 Tools based on feedback from an Assisted Living Facility (ALF) usability pilot-testing program. The majority of ALF participants reported usability of the tools and experts in ALF care provided suggestions for improving the tools for use in every day care of residents Florida Atlantic University
50 Do you think this INTERACT AL is a useful tool? Percentage of respondents agreeing that the tool is useful Percentage of respondents agreeing that the tool is useful For Communication Between AL and Hospital Communication Tools SBAR Communication Form and Progress Note for RN/LPN/LVNs in AL/HH SBAR Communication Form and Progress Note for Caregiver in AL/HH Medication Reconciliation Worksheet for Post Hospital Care 70% 53% 47% Assisted Living Capabilities List 69% AL to Hospital Transfer Form 61% AL to Hospital Transfer Data List 48% AL Acute Care Transfer Checklist 53% Hospital To Post Acute Care Transfer Form 47% Stop and Watch Early Warning Tool 88% Hospital To Post Acute Care Data List 37% Final Assisted Living Pilot Site Ratings (N=33*) Response rate varies from participants 50


51 ADVANCE CARE PLANNING 51
52 Pilot Sites Conclusions ALF tools are rated as very useful Highest ranked tools are Communication tools (SBAR and Stop and Watch) Decision support and Advance Care Planning tools were well received ALFs with Electronic records were more likely to complain the INTERACT forms duplicate work Staff indicated improvements but admitted it was work to implement Many pilot sites used communication forms but did not enact QI process for full use of all tools 52
53 INTERACT Implementation 53
54 Assisted Living: Hospitalization Rate 54

55 AL Hospitalization Rate: CMS Claims 55
56 56 Emergency Room Transfer Rates

57 Engaging Hospitals 1. Create a list of all hospitals your facility sends patients to/or receives patients from. 2. Identify the readmissions champion for each hospital. 3. Host or join a cross-continuum or Community Care Transitions Working Group or Coalition. 4. State your facility s goals to reduce avoidable hospital transfers, admissions, and readmissions, and link that to the hospitals goals in readmission reduction. 5. Describe the set of quality improvements underway in your facility through INTERACT and other initiatives. 6. Ask the hospital to be an active partner in your INTERACT improvements. 57
58 Engaging With Hospitals: V=Q+S $ Identify your champions and co-champions Share your capabilities Demonstrate your value with data Participate on transition teams and coalitions Determine projects to pursue Hardwire continuous quality improvement structure 58
59 Ensure Leadership Buy-in Create a feeling of urgency Build your team Have a clear vision Communicate for buy-in Empower action Create short-term wins Don t let up Make changes stick Source: Kotter JP, Leading Change 59
60 Impact: Acute and PAC Providers Strategic planning Identifies opportunities for synergistic alliances Increases care coordination with hospitals and communities Positions the PAC provider to be a viable hospital partner Aligns internal operations with ACA and hospital Initiatives 60
61 Project Impact: Medicare Population Assist organizations in the development of processes that: Improve clinical post-acute care outcomes for Medicare population Decreases risk of inappropriate hospital readmissions and ER transfers Improves continuity of care from acute to post-acute care Reduce cost and health care expenditures through increased efficiency and operational capacity Provides methods to hold post-acute care and long-term care providers accountable for performance 61
62 Project Impact: Public Health Addresses Accountable Care Act and Triple Aim Guidelines to: Improve Patient Experience Improve Quality of Healthcare Decrease Medical Cost Reduces: Silos in Healthcare Healthcare Expenditures Medical Errors Increases Internal and External Accountability for PAC and LTC Providers Develops Relationships between Public Health and Senior Long-Term Healthcare Providers 62
63 What We Have Learned Importance of Leadership & Communication Role of Champions/Co-Champions is critical Sustaining gains & training new staff Integrating QI/tools into the culture Opportunities with staff turnover Family/Caregiver education on INTERACT is important Advanced Care Planning discussions make a difference Involve all staff in quality improvement Critical role of the Transition Teams 63
64 Resources National Transitions of Care Coalition: Institute for Healthcare Improvement: INTERACT QI Program: Care Transitions Program SM, University of Colorado (Eric Coleman, MD): American Medical Director Association: Transitions of Care Clinical Practice Guideline at 64

65 Alone we can do so little; together we can do so much. Helen Keller 65

66 Questions? 66
INTERACT for Assisted Living
 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
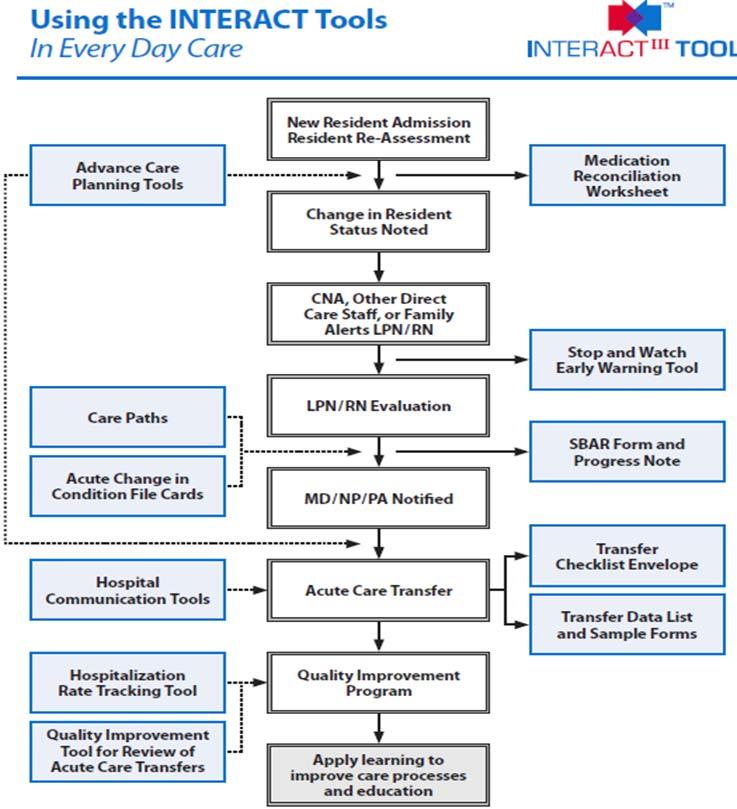
Tools Use Suggested Formats. All facility staff Provides a visual depiction of INTERACT in daily practice
 INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Reducing Potentially Avoidable Hospitalizations of Nursing Home Residents
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
February 27, Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models
 1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT
 04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Care Alignment Strategy Management & Operations Track Tuesday, July 29, 4:45 5:45 pm
 Post-Acute Care Alignment Strategy Management & Operations Track Tuesday, July 29, 4:45 5:45 pm Lisa Lyons Executive Director St. Josephs John Knox John M. Hehn, Jr. Executive Director Florida Presbyterian
Post-Acute Care Alignment Strategy Management & Operations Track Tuesday, July 29, 4:45 5:45 pm Lisa Lyons Executive Director St. Josephs John Knox John M. Hehn, Jr. Executive Director Florida Presbyterian
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Readmission Prevention: A Community Collaborative Approach
 Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative
 Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
Preventing Unplanned Acute Care Admissions A Nursing Home Quality Initiative UPMC Senior Communities Skilled Nursing Facilities UPMC Senior Communities: Who are We? 5 Skilled Nursing Facilities 5 Personal
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
Unlock the keys to success in the future: Clinical targets for care programming control
 MISSOURI ALLIANCE HOME CARE (MAHC) Unlock the keys to success in the future: Clinical targets for care programming control Kimberly McCormick RN/BSN 22 year Home Health Clinician 22 years in Home Health
MISSOURI ALLIANCE HOME CARE (MAHC) Unlock the keys to success in the future: Clinical targets for care programming control Kimberly McCormick RN/BSN 22 year Home Health Clinician 22 years in Home Health
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Postacute care (PAC) cost variation explains a large part
 cost variation explains a large part") INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
Emerging Issues in Post Acute Care Trends
 Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
Presentation Objectives
 Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
Using Quality Data to Market to Referral Sources BUSINESS OF HEALTHCARE
 Using Quality Data to Market to Referral Sources Cindy Mason Change as a Matter of Survival BUSINESS OF HEALTHCARE 2 National Transformation of Healthcare the Affordable Care Act provides CMS the flexibility
Using Quality Data to Market to Referral Sources Cindy Mason Change as a Matter of Survival BUSINESS OF HEALTHCARE 2 National Transformation of Healthcare the Affordable Care Act provides CMS the flexibility
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Presented by: Darren Swenson, MD Director of Medical Affairs, IPC of Nevada, Inc. March 30, 2010
 Presented by: Darren Swenson, MD Director of Medical Affairs, IPC of Nevada, Inc. March 30, 2010 Healthcare reform Costs: +$15 billion Medicare alone Increasing number of readmissions 18.2% (2000) to 23.5%
Presented by: Darren Swenson, MD Director of Medical Affairs, IPC of Nevada, Inc. March 30, 2010 Healthcare reform Costs: +$15 billion Medicare alone Increasing number of readmissions 18.2% (2000) to 23.5%
Session Objectives. The Triple Aim & Beyond- Partnering with Payers- Increasing Trust, Building Infrastructure, & Rethinking Partnerships 3/18/2016
 Orlando, Florida The Triple Aim & Beyond- Partnering with Payers- Increasing Trust, Building Infrastructure, & Rethinking Partnerships Iva Tatum, RN CCM CLNC Manager of Case Management Community Care Managed
Orlando, Florida The Triple Aim & Beyond- Partnering with Payers- Increasing Trust, Building Infrastructure, & Rethinking Partnerships Iva Tatum, RN CCM CLNC Manager of Case Management Community Care Managed
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
The Center for Medicare & Medicaid Innovations: Programs & Initiatives
 The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
The Center for Medicare & Medicaid Innovations: Programs & Initiatives Rob Stone, Esq. American Health Lawyers Association Institute on Medicare & Medicaid Payment Issues March 30-April 1, 2012 CMMI Mission
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Using Quality Data to Market to Referral Sources. Kim Hicks
 Using Quality Data to Market to Referral Sources Kim Hicks Change as a Matter of Survival BUSINESS OF HEALTHCARE 3 What s Happening here? It costs Medicare about $26 billion a year, with about $17 billion
Using Quality Data to Market to Referral Sources Kim Hicks Change as a Matter of Survival BUSINESS OF HEALTHCARE 3 What s Happening here? It costs Medicare about $26 billion a year, with about $17 billion
OPTIMISTIC 8/13/2014. Outline OBJECTIVES
 OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings.
 Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Succeeding in Value-Based Care CareConnect Journey
 Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
Succeeding in Value-Based Care CareConnect Journey Donna Mueller VP Network Development dmueller@infinityrehab.com 360-201-2703 Jake Arrastia VP Strategy Development & Innovation jrarrastia@infinityrehab.com
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
QUALITY AND COMPLIANCE
 2015 HCCA SOUTHEAST CONFERENCE JANUARY 23, 2015 QUALITY AND COMPLIANCE Katie Fink Donna Lewis Susan Walberg Presenters Katie Fink Senior Counsel Office of Counsel to the Inspector General U.S. Department
2015 HCCA SOUTHEAST CONFERENCE JANUARY 23, 2015 QUALITY AND COMPLIANCE Katie Fink Donna Lewis Susan Walberg Presenters Katie Fink Senior Counsel Office of Counsel to the Inspector General U.S. Department
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home. Your thoughts
 Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Objectives. Assisted Living. O 2 : Opportunities & Outcomes in Assisted Living. Presented by: Chief Clinical Officer
 O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
Readmission Reduction and the ACO
 Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Readmission Reduction and the ACO Jeffrey E. Epstein, MD Medical Director Atlantic Health System Morristown Medical Center Morristown, NJ 07960 JeffreyEpsteinMD@gmail.co m Morristown Medical Center Why
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
PHCA Webinar January 30, Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq.
 PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
PHCA Webinar January 30, 2014 Latsha Davis & McKenna, P.C. Kimber L. Latsha, Esq. 1 2 Intended to: Encourage the development of ACOs in Medicare Promotes accountability for a patient population and coordinates
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR
 CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS
 BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
BUILDING BRIDGES: SUCCESSFUL TRANSITIONS FROM HOSPITAL TO HOME FOR OLDER ADULTS Senior s Month Education 2013 Sponsored by Regional Geriatric Program central (RGPc) Committee for the Enhancement of Elder
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
8/28/2018. Presentation agenda CURRENT STATE OF THE POST ACUTE PROVIDER SECTOR. Impact of The Medical Director in Preserving Your Future
 Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Value-Based Reimbursements are Here: Are you Ready?
 Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Housekeeping. Harmony Healthcare International, Inc.
 Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Tackling Avoidable Readmission through Care Transition: PART I HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Diane Buckley, BSN, RN, RAC-CT Director
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
QUALITY MEASURES WHAT S ON THE HORIZON
 QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QUALITY MEASURES WHAT S ON THE HORIZON The Hospice Quality Reporting Program (HQRP) November 2013 Plan for the Day Discuss the implementation of the Hospice Item Set (HIS) Discuss the implementation of
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
What s Inside? Sidebars DID YOU KNOW? Hospital Outcome of Care Measures National Averages
 Roughly 40% of Medicare beneficiaries leaving the hospital are discharged to a post-acute setting, where the risk for rehospitalization begins, and the role of the skilled and assisted living facility
Roughly 40% of Medicare beneficiaries leaving the hospital are discharged to a post-acute setting, where the risk for rehospitalization begins, and the role of the skilled and assisted living facility
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system