Reducing Readmission Case Stories Discussion of Successes
|
|
|
- Rosalyn Quinn
- 5 years ago
- Views:
Transcription

1 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids Iowa Peg Bradke RN, MA Vice President, Post Acute Care UnityPoint Health St. Luke s

2 University of California, San Francisco 2 Mission: The reason that we exist is Caring, Healing, Teaching, and Discovery Top 10 Hospitals (US World and News past 13 yrs) 722 licensed beds; 28,000 admissions, New UCSF Mission Bay Hospitals Benioff Children s Hospital Betty Irene Moore Woman s Hospital Bakar Cancer Hospital Ron Conway Family Gateway Medical Building

3 The Cross Continuum Team 3 Multidisciplinary cross continuum team it takes a village; Family caregivers, nurses, physicians, senior leadership, case managers, social workers, dieticians, pharmacists, nurse practitioners, home care team, palliative care, Care Support team, chaplains, managers, community partners, SNF liaisons, outpatient clinic liaisons, community clinics liaisons, and more
4 The Cross Continuum Team 4 Excellence in Transitions of Care ETOC Workgroups Hospital wide readmission projects Data review and management Highlights on progress on projects/programs Inpatient and outpatient programs Senior leadership participation Office of Population Health





5 Cross Continuum Teams UCSF Housecalls UCSF Care Support UCSF-Hastings Medical Legal Partnership for Seniors UCSF Center for Geriatrics Care UCSF Bridges
6 St. Luke s Hospital - UnityPoint Health System Private hospital Cedar Rapids, Iowa Affiliate in the UnityPoint Health System Licensed for 500 Beds with more than 17,000 admissions Truven Top 100 Hospital 5 years; Heart Hospital - 3 years Iowa Recognition for Performance Excellence Gold Award Joint Commission Disease-Specific Recertifications in Stroke ( ), Heart Failure ( ), Total Joint ( ) and Palliative Care ( ). Society of Chest Pain Center Chest Pain Certification (2010, 2013) Magnet Re-designation 2014 Mayo Clinic Care Network 2014
7 CCT Transition to Home Our mission: To give the healthcare we d like our loved ones to receive Meets monthly Reviews readmissions for each month related to core diagnosis to assess causes and opportunities for improvement Reviews process and outcome measures Continually testing and improving, aggregating the experiences of patients, families and caregivers Each site/level of care reports on testing occurring in their area
8 Transition to Home Team Members Inpatient Nursing Units Manager Care Managers Palliative Care Home Care Respiratory Care Emergency Dept. Case Management CardioPulm. Rehab. Pharmacy Nurse Practitioners UnityPoint Clinics Reps Critical Access Hospital Community SNF s Hospitalist Rounding Nurses Outpatient Social Services Inpatient Social Services Performance Improvement
9 Several Subgroups Report into the Larger Transition to Home Team Data Management Patient Education Processes Home Care SNF/Nursing Facilities Work Processes Physician Clinic Processes Case Management/Social Work/Care Coordination Several members of the Transition to Home team are members of the hospital ACO and Population Health Management work. Information is bidirectional between these teams.
10 Program Overview 10
11 Overview of the Process Standardized evidence-based care through order sets. Patient Education/Teaching: Utilizing Universal Health Literacy Concepts Enhanced teaching materials Teach back Utilization of whiteboard to individualize patient s plan of care and communicate to team. Bedside Report Transition to Home Huddles
12 Continuum of Care (Cont d) Touch points post discharge: Home Care - care coordination visit 24 to 48 hours post discharge on high-risk patients Physician Clinic follow-up appointment made prior to discharge for 3-7 days after Work closely with PCP offices on Transitional Code (TCM) and Patient Centered Medical Home Standardized tool for transfer of information to nursing facilities for next level of care. Telehealth monitor available through Home Care Emergency Department Consistent Care Program Advanced Medical Team Outpatient Social Worker Palliative Care Program
13 The Foundation Monthly Heart Failure Grant Meetings with Multidisciplinary Team Comprehensive Patient Education Care coordination Implemented IHI Evidence Based Interventions Development of Data Collection System Patient Advisory Group, Heart Healthy classes on unit Palliative Care Collaboration Staff trained on Teach Back & HF Education Patient stories shared to drive change Focus on Continuum of Care - Communication and Collaboration

14 Patient Interventions Patient Identification- Daily Chart Reviews Extensive Patient and Family education Referrals: Inpatient and Outpatient Follow-up Appointments Within 7 days for primary HF, COPD, PNA,AMI Heart Failure Clinic NPs visits for high risk patients Outpatient programs for high risk patients Follow-up calls Increased with automation to 5/month Medication Reconciliation- Pharmacist consult Discharge Summaries- within 48 hours Hand off Communication to Outpatient providers Care at Home Programs High Risk patients
 Geriatric Transitions, Consultation, and Comprehensive Care (GeriTraCCC) started UC Care Support at Home MD House Calls for High Risk HF Patients (Aug 2010) Advanced Heart Failure")
15 Outpatient Focus Collaboration with Outpatient Providers Skilled Nursing Facilities, Home Care Agencies, Primary Care Physicians, and Cardiologists Virtual Team to connect providers (in/outpatient) Geriatric Transitions, Consultation, and Comprehensive Care (GeriTraCCC) started UC Care Support at Home MD House Calls for High Risk HF Patients (Aug 2010) Advanced Heart Failure Clinic; High Risk pts- NP follow up In-services for staff, home care, skilled nursing staff Hospital wide projects to standardize and improve discharge process and readmission projects
16 Assessment 16

17 UCSF MDR Improvements 17 Quieter space New team monthly- welcome and orientation Clear expectations for all members Readmission discussions What can we do differently? Address level of support needed Risk discussed

18 Readmission Interviews 18 Gain perspective of patient and family caregivers Reach out to inpatient and outpatient providers Notification of # of admissions in past year, 30 and 90 day readmits, and possible factors Low health literacy Lack of support Medication challenges Transportation challenges Assessments: Cognitive, depression, functional, motivation



19 The Patient Story to share and learn from 19
20 Enhanced Assessment During Admission Assessment, the patient and family are asked, Who would you like to have present when we provide your discharge information? Medication reconciliation: Dedicated Admission Center RN s complete home medication list and prepare an appropriate list for physician to address. Readmission Interviews
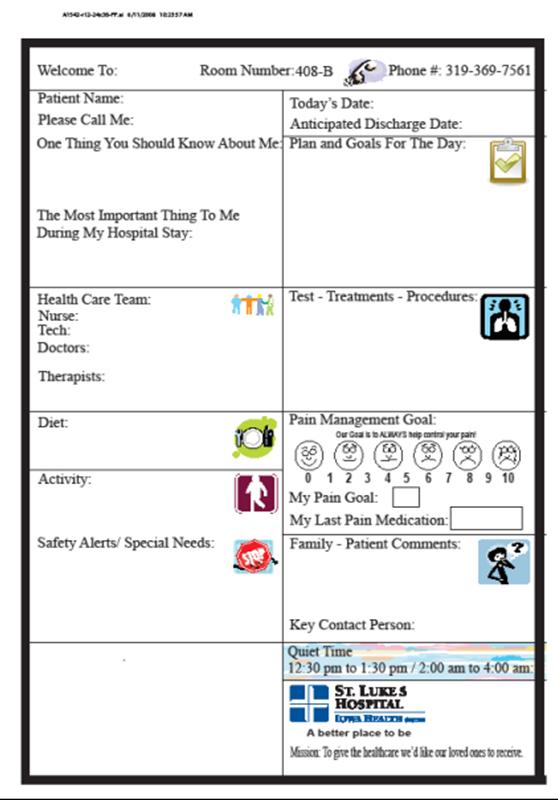
21 Whiteboard
22 Multidisplinary Rounds Bedside shift report To involve patient and family caregivers as partners in care Daily discharge huddles Identification of patient/family needs/concerns Daily goals are reviewed Available support for patient: need for Palliative Care Referral Educational needs Identification of home care needs/other levels of care Nurse sensitive indicators: fall risk, skin issues
23 Patient Education/Teach Back 23
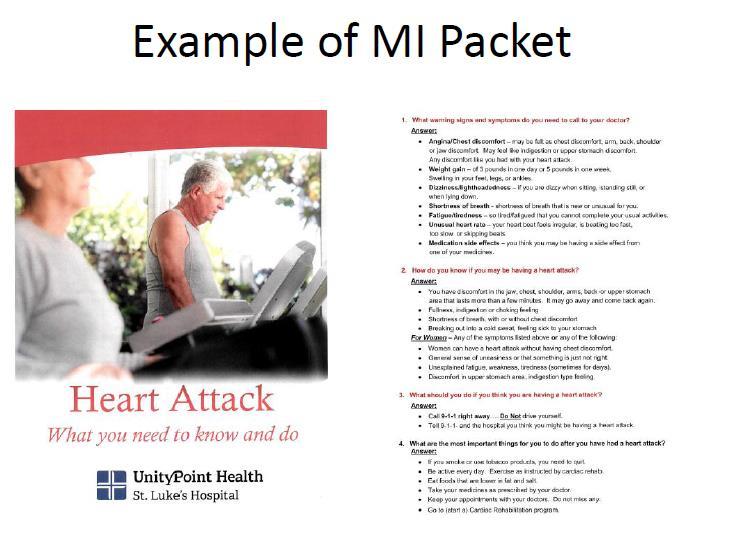
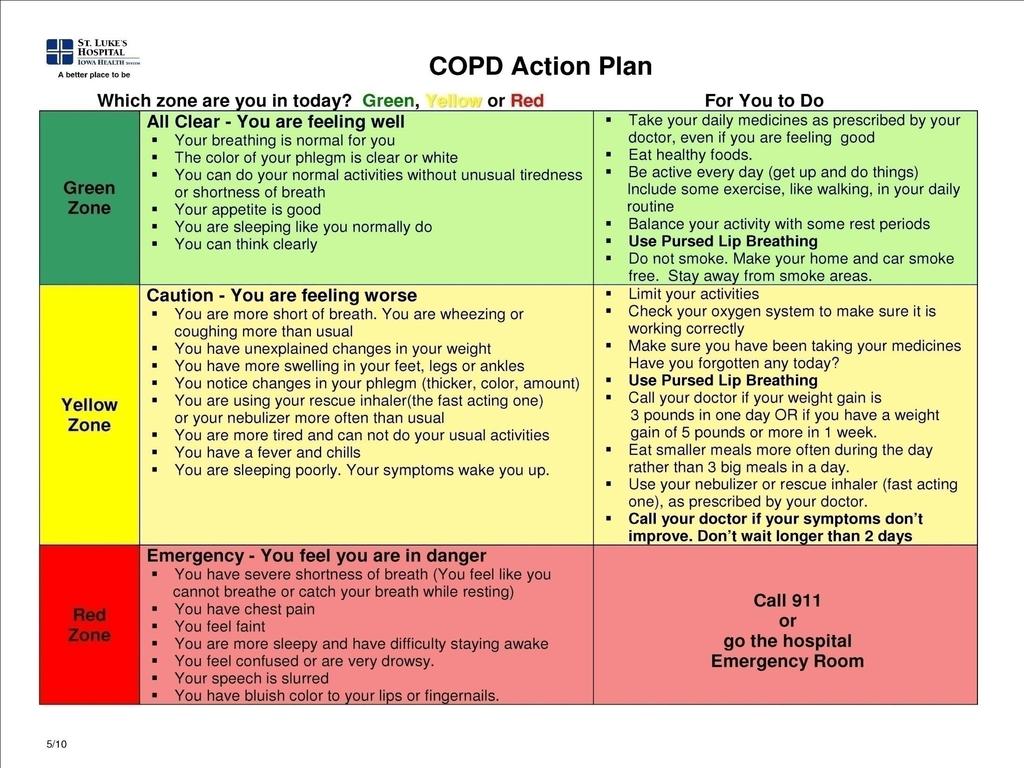
24 Enhanced Teaching and Learning Same materials are used across the continuum: in the hospital, with home care, long-term care settings and the clinics. Short, succinct patient/family education packet Teach Back questions part of packet Patient teaching flowsheets close the loop to help staff nurses address Teach Back and assure the documentation and use of Teach back.
25

26 Example: MI 2nd page with TB questions
27 27

28 Example from EPIC Patient Teaching Flowsheet
29 Teach Back Utilized with Discharge Instructions Can you show me on these instructions: How you find your doctors office appointment? What other tests you have scheduled and when? Is there anything on these instructions that could be difficult for you to do? Have we missed anything? Who will you call if you have questions?
30 Discharge SmartPhrase
31

32 Patient Education Teach Back Technique- WORKS Health Literacy principles Multiple languages- use of interpreters Input from patients and family caregivers Same materials and technique across the Continuum of Care Educate patient regarding diagnosis, self care management, and importance of follow up Lesson Learned: Listen before we teach. Ask open-ended questions Goal for Patient: Take action when you notice a change in your health
33 Real-Time Handover 33

34 Real-Time Handover Communications Warm Hand-overs to Skilled Nursing Facilities, Home care agencies, outpatient clinics, and providers -notifications to inpatient team, case manager, consultants, HF clinic, home care RNs, SNF and PCP on admission Creates a Virtual Care Team Time consuming but valuable Unites the entire team working on transition of care Importance of Home Care referrals Medication reconciliation Focus on self management skills
35 to Team on Admission: Dear Medical Team, We wanted to let you know that we are following Mr. XXXXXXXXXXX in the Heart Failure / Transitional Care Program. We are very familiar with this high risk patient from previous admissions (5 th in past 4 months). We have provided education, initiated palliative care consults, and coordinated services in the past. We would like to provide as much support as possible for the patient and family. Recommendations: 1.Bridges Program- MD home visits 2.UC RN home care 3.Pharmacist consult for discharge medications 4.Follow up appointment within 7 days 5.Goals of care discussion/palliative care consult The goal of this program is to provide our Medicare patients and families with as much information and support as possible to enable them to safely manage their care during this vulnerable post hospitalization period, and to prevent avoidable 30 day readmissions. We will be following patients with primary heart failure, COPD, PNA, and AMI. We will be sharing information through tracking of the readmissions to identify trends and to learn from. The focus of the program is as follows; In-house consults when indicated dietary, pharmacist, palliative care Goals of care conversations initiated ( by the team or PCS) for all patients admitted 3 times within a year RN/PT home care visits whenever deemed appropriate Follow up appointments scheduled within 7 days for primary heart failure patients and 14 days for all others at time of discharge Follow up calls through the UCSF discharge phone call program and by the transitional care program for patients identified as high risk for readmissions Please let us know if there is anything that we might do to assist and thank you for the great care that you provide our patients!
36 Real-Time Handover Communications Interagency standardized transfer form Warm handover Communication Work with Clinic and the TCM code ARNP s assigned to Post Acute Facilities to oversee care management Transition Feedback opportunities
37 Support Programs 37
38 Support Programs Consistent Care Program (EDCCP) Patients who had Emergency Room visits >12 times in previous 12 months. Care Plan is developed by a team coordinated by an assigned Social Worker. Communication tool provides data specific to patient s medical Hx. and current medical needs, and Goals of Care for when patients presents again. Advance Medical Team High Risk patients assigned a Care Navigator to work with them across the continuum. Team includes resource for Outpatient Social Work and Pharmacy consult for medication management.
39 Support Programs 39 Heart Failure Clinics MD/NP home visits programs Outpatient Palliative Care program Health Care Navigators ACO case managers Discharge phone calls program


40 UCSF Automated Calls Program Goal: All patients receive a discharge phone call- 80% Currently: ED, Neuro, Medicine, Ortho, Cardiac Disease Management Heart Failure, COPD, AMI Specific calls promotes accountability 4-6 additional calls over 30 days


41 Post Discharge Automated Call Program

42 HealtheHeart Study Nurse Avatar Molly Heart Failure management Calls recorded by Heart Failure Coordinators Weights, B/P, Heart Rate Promotes self care management Inpatient Survey- patients 65+ positive feedback

43 UCSF Palliative Care Program 43
44 Palliative Care Palliative care proven to improve symptoms, quality of life, satisfaction, and patient and family outcomes 25% of our Heart Failure patients die within one year Up to one- half of deaths with Heart Failure are due to Sudden Death Palliative care prompts patients to think about all their options in the future and to start the important discussions for making plans Standard- consult on 3rd Readmission /Year New this year, PC MD on Heart Failure Service Increased palliative care options in outpatient setting- expansion Pantilat and Steimle JAMA 2004;291: Wright et al. JAMA 2008;300: Morrison J Palliat Med 2005;8:S79-87

45 The Goals of Care Conversation: When you think about the future what do you hope for? When you think about what lies ahead, what worries you most? How do you approach these decisions in your family? Sit and listen Wait full 2 minutes without a word Steve Pantilat, MD Director of the UCSF Palliative Care Program
46 Results 46
47 47

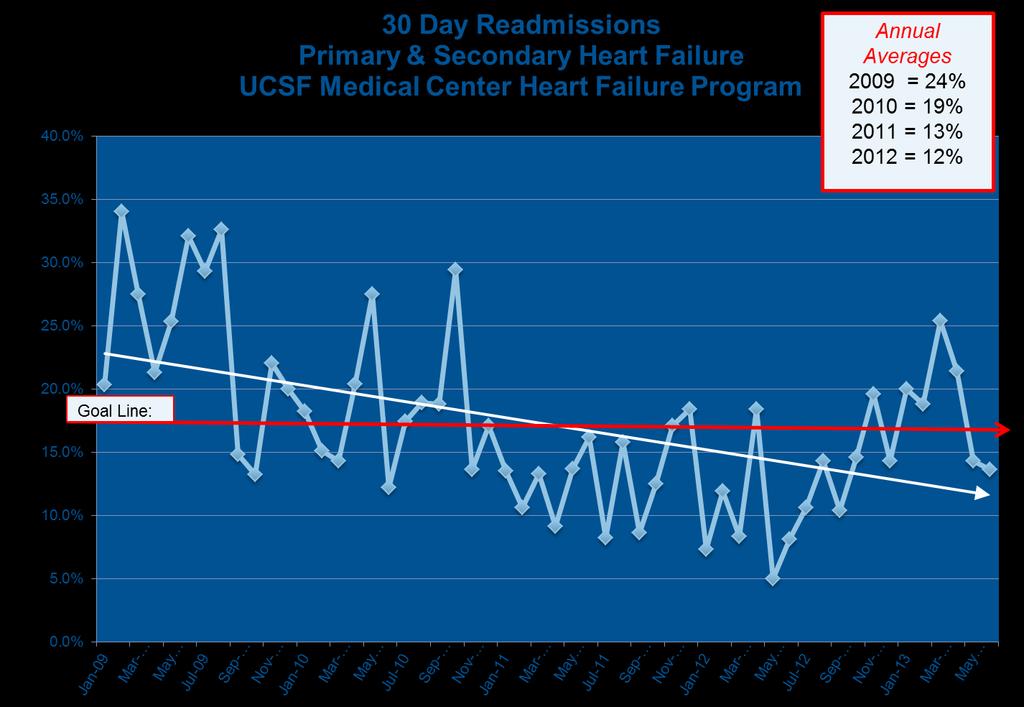
48 Medicare FFS 30 day Readmissions 48 Index 67 readmit 16 Index 40 readmit 8 FY 2012 FY 2013 FY 2014 FY 2015 YTD AMI 12.3% 15.8% 13.6% 20% CHF 22.3% 17.0% 18.4% 16.6% COPD 17.5% 13.5% 16.2% 23.9% PNA 18.1% 13.3% 14.6% 6.9% HF 75% of patients in Transitions Program

49 UCSF Readmission Dashboard
50 Results
51

52 HCAHPS RESULTS DISCHARGE INFORMATION (% Yes) The following questions make up this composite measure: #19 During hospital stay, did doctors, nurses or other hospital staff talk about whether you would have the help you needed when you left the hospital? #20 - During hospital stay, did you get the information in writing about what symptoms or health problems to look out for after you left the hospital?
53 Lessons Learned 53
54 Lessons Learned Importance of engaged executive leaders and physicians. Patients and families help transform care in profound ways. The patient and family home environment must be understood. Involving frontline staff in the changes helps them understand why they are important and grows ownership by engaging them in redesign.
55 Lessons Learned (cont) The role of Information Technology in the process should be addressed simultaneously with the work. Ongoing monitoring of Process and Outcome Measures is important to hardwiring best practices. Using patient stories unleashes energy and participation that becomes evident in process and outcome results. The power of relationship building and collaboration of the cross-continuum team builds new ideas to work and removes many of the silos in the care.
56 Lessons Learned Collaboration with IHI extremely valuable Dedicated Heart Failure/Disease Management Program Coordinators - accountable, reliable processes Willingness to test, trial, and change interventions Make efforts to move outside of silos Senior Leadership and Champions necessary Cohesive, committed multidisciplinary cross continuum teams
57 Lessons Learned Palliative Care Team Collaboration Home Care collaboration and referrals Outpatient program & Community Partners essential Results are not immediate takes time to show improvement Teach Back works focus on Health Literacy Technology great potential Here to stay Power of the patient story to learn from and drive change
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
REDUCING READMISSIONS
 REDUCING READMISSIONS UnityPoint Health - St. Luke s Hospital Cedar Rapids, Iowa IHI National Forum December 2014 - Orlando, Florida ST. LUKE S HOSPITAL UNITYPOINT HEALTH SYSTEM Private hospital Cedar
REDUCING READMISSIONS UnityPoint Health - St. Luke s Hospital Cedar Rapids, Iowa IHI National Forum December 2014 - Orlando, Florida ST. LUKE S HOSPITAL UNITYPOINT HEALTH SYSTEM Private hospital Cedar
M7: Improving Transitions and Reducing Avoidable Rehospitalizations. St. Luke s Hospital Member, Iowa Health System
 M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
UCSF Transitional Care Program. Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016
 UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
IHI S APPROACH TO REDUCING REHOSPITALIZATIONS IN THE STAAR INITIATIVE: OVERVIEW
 Session M1 This presenter has nothing to disclose IHI S APPROACH TO REDUCING REHOSPITALIZATIONS IN THE STAAR INITIATIVE: OVERVIEW Pat Rutherford, RN, MS, Vice President, Institute for Healthcare Improvement,
Session M1 This presenter has nothing to disclose IHI S APPROACH TO REDUCING REHOSPITALIZATIONS IN THE STAAR INITIATIVE: OVERVIEW Pat Rutherford, RN, MS, Vice President, Institute for Healthcare Improvement,
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Enhanced Assessment for Post Hospital Needs
 These presenters have nothing to disclose Enhanced Assessment for Post Hospital Needs Maureen Carroll September 28, 2015 Session Objectives Participants will be able to: Identify failures in current processes
These presenters have nothing to disclose Enhanced Assessment for Post Hospital Needs Maureen Carroll September 28, 2015 Session Objectives Participants will be able to: Identify failures in current processes
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
Readmission Prevention: A Community Collaborative Approach
 Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4
 Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 1. Expedition Coordinator
 Thursday, June 6, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 1 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 6, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 1 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Transforming Outcomes through Implementation of a Nurse Practitioner Hospitalist Service. About Long Beach, CA. About Memorial Care
 Transforming Outcomes through Implementation of a Nurse Practitioner Hospitalist Service Judy Fix, MSN, CNO Megan Liego, DNP, ACNP-BC About Long Beach, CA Located in South Los Angeles County Seventh largest
Transforming Outcomes through Implementation of a Nurse Practitioner Hospitalist Service Judy Fix, MSN, CNO Megan Liego, DNP, ACNP-BC About Long Beach, CA Located in South Los Angeles County Seventh largest
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Baystate Medical Center
 Baystate Medical Center STAAR Collaborative February 2 & 3 2011 680 bed tertiary care referral center ( ~1M) Flagship of Baystate Health 42 k admissions/year Annual surgical volume: 29,043 Western Campus
Baystate Medical Center STAAR Collaborative February 2 & 3 2011 680 bed tertiary care referral center ( ~1M) Flagship of Baystate Health 42 k admissions/year Annual surgical volume: 29,043 Western Campus
Redesigning the Role of the RN in Case Management: Impact on HCAHPS and Readmission Rates Session C093. Mercy Health System 09/10/15
 Redesigning the Role of the RN in Case Management: Impact on HCAHPS and Readmission Rates Session C093 2015 ANCC National Magnet Conference Friday October 9th 2015 8:00 a.m. Debra Potempa MSN, RN, NEA
Redesigning the Role of the RN in Case Management: Impact on HCAHPS and Readmission Rates Session C093 2015 ANCC National Magnet Conference Friday October 9th 2015 8:00 a.m. Debra Potempa MSN, RN, NEA
Impacting Key Hospital Performance Metrics Through Leveraging a Hospitalist Program Becker s Hospital Review April 14, 2018
 Impacting Key Hospital Performance Metrics Through Leveraging a Hospitalist Program Becker s Hospital Review April 14, 2018 Carle Foundation Hospital Lynne Barnes, Chief Operating Officer Dr. Saad Adoni,
Impacting Key Hospital Performance Metrics Through Leveraging a Hospitalist Program Becker s Hospital Review April 14, 2018 Carle Foundation Hospital Lynne Barnes, Chief Operating Officer Dr. Saad Adoni,
Emerging Strategies for Improving Hospital Medicine
 Emerging Strategies for Improving Hospital Medicine Improving efficiency, patient safety, metrics and satisfaction Improving communication among the patient s community of caregivers Your Presenters Francisco
Emerging Strategies for Improving Hospital Medicine Improving efficiency, patient safety, metrics and satisfaction Improving communication among the patient s community of caregivers Your Presenters Francisco
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Involving Patients and Families to Improve Care Transitions
 Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
Involving Patients and Families to Improve Care Transitions Julius Yang, MD, PhD Director of Inpatient Quality Sarah Moravick, MBA QI Project Manager 1 Overview of Today s Discussion 1. BIDMC s burning
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Outside the Box: A. Social Service Model of Community-based Palliative Care. Seniors At Home A division of Jewish Family and Children s Services
 Outside the Box: A Social Service Model of Community-based Palliative Care Seniors At Home A division of Services J. Redwing Keyssar, RN, BA, Author Director, Palliative Care and Nursing Services 1 The
Outside the Box: A Social Service Model of Community-based Palliative Care Seniors At Home A division of Services J. Redwing Keyssar, RN, BA, Author Director, Palliative Care and Nursing Services 1 The
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
An Integrated Approach to Heart Failure Care. Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN
 An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
ASPIRE to Knockout Pneumonia Readmissions Webinar #1. Amy Boutwell, MD, MPP March 1, 2018
 ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Improving Care Transitions: Creating Your Evidence-Based Approach
 Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
Improving Care Transitions: Creating Your Evidence-Based Approach Jack Chase, MD Director of Operations, UCSF Family Medicine Inpatient Service San Francisco General Hospital Assistant Clinical Professor
Heart Failure Education Consider Health Literacy
 Heart Failure Education Consider Health Literacy Sandy Hall RN BSN Heart Failure Case Manager Mercy Medical Center Des Moines, IA August 2012 What does this mean to you? Cardiac diet 1 Is it this? Low
Heart Failure Education Consider Health Literacy Sandy Hall RN BSN Heart Failure Case Manager Mercy Medical Center Des Moines, IA August 2012 What does this mean to you? Cardiac diet 1 Is it this? Low
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager A HEALTHIER WORLD THROUGH BOLD INNOVATION
 Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
ASPIRE to Reduce Readmissions
 ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia. Webinar #3 Post-Acute Care Readmissions September 8, 2016
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Program Development. Completion of Gap Analysis. Review of Data. Multi-disciplinary team
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Organization. Hospital to SNF Communication. Care Coordination Goals. Chasing the Perfect Handoff The Missing Link to Interoperability 7/18/2016
 Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Organization Chasing the Perfect Handoff The Missing Link to Interoperability Annette Brown, BSN, RN Director, Clinical Informatics Eisenhower Medical Center abrown@emc.org Not for profit, academic, community
Improvements in Care-Transitions: A Case Study of St. Luke s Hospital
 [CASE STUDY] January 18, 2012 Improvements in Care-Transitions: A Case Study of St. Luke s Hospital Prepared for the Centers for Medicare and Medicaid Services 2012 The Brookings Institution Foreword The
[CASE STUDY] January 18, 2012 Improvements in Care-Transitions: A Case Study of St. Luke s Hospital Prepared for the Centers for Medicare and Medicaid Services 2012 The Brookings Institution Foreword The
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
2017 Edition. MIPS Guide. The rule is in and Medicare physician payments are changing. What does that mean for you?
 2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
WHEN THINGS ARE CHANGING FAST
 The Home Health Challenge PLAN, POSITION, PARTNER Presented by: Tim Ashe MSN, MBA Partner Fazzi Associates, Inc. tashe@fazzi.com WHEN THINGS ARE CHANGING FAST Not Paying Attention to the Changes and Not
The Home Health Challenge PLAN, POSITION, PARTNER Presented by: Tim Ashe MSN, MBA Partner Fazzi Associates, Inc. tashe@fazzi.com WHEN THINGS ARE CHANGING FAST Not Paying Attention to the Changes and Not
NoCVA Preventing Avoidable Readmissions. Moving Beyond the Basics March 27, 2014
 NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure
 Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide