Patient Activation Using Technology- Supported Navigators
|
|
|
- Nicholas Barton
- 6 years ago
- Views:
Transcription


1 Patient Activation Using Technology- Supported Navigators March 2, PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC
2 Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting Fees
3 Agenda/Introduction 1.Review of STEPS Value 2.Role of Technology and Navigators in Improving Health Outcomes A.Supporting Research B.Technology C.Role of Navigator 3.Navigator in Health Care Settings A.Home Health Care B.Physician Office (CCM) C.Hospital Case Management D.Call Centers 4.STEPS Outcomes
4 Learning Objectives 1. Identify components of a technology-enabled program for community residing older adults 2. Identify advantages of synthesis of High-tech, High touch approach to technology use in health care 3. State impact of technology supported navigators on outcomes of: rehospitalization, ER usage, patient satisfaction and patient activation
5 An Introduction of How Benefits Were Realized for the Value of Health IT Patient Employee Payer Self Care Goals Medications HIPAA Compliant Targeted Health Education Interventions Patient Activation Cost Rehospitalizations ER Usage Ease of CCM Compliance


6 Reimbursement model is changing OLD WAY Fee for Service Model NEW WAY Value-Based Model Episodic interaction Stand alone plans of care No requirement for psychosocial assessment Little accountability for quality or cost Patient initiated interactions Duplicate tests, activities, tasks Accountability Bundled Payments Chronic Care Management Reimbursement. Chronic disease driven interactions Recognition of Social Determinants of Health Inter-visit coaching/contact Post-visit follow up Comprehensive Plan of Care development & management Technology adoption Data collection & assessment Outcome-based reimbursement
7 Social Determinants of Health Those non-medical issues that make a diagnosis or treatment difficult for patients. Healthcare barriers can be due to: Socioeconomic conditions Health Literacy Logistical issues (access to care) Language or culture The healthcare system itself!

8 Why????




9 Collaborative Platform Care Navigators Combining High-tech + High-touch HIPAA-compliant extension to existing EHR Trained patient advisors address non-clinical issues
10 Components of a High-Tech System Ease of Use-Patient Centric Compatibility with existing Health IT programs Accessible across the health care continuum: Acute & Post Health Facility-Navigator- Patient-Family One True Source Meets Requirements of Chronic Care Management Cost Effective
11 Technology Platform
12 High Touch - Role of Navigator Gunn et al (2014) identified a nine principle framework for the role of the navigator: Individual Level Principles Eliminating Barriers to Timely Care Providing patient-centric care Integrate fragmented system Navigate across disconnected system Program Level Principles Program cost effectiveness Level of skill is defined Clear scope of role System is coordinated Willis et al (2013) identified additional skills : Community Resource identification Patient Empowerment Ethics and Professional Conduct Cultural Competency
13 Navigator Curriculum Module 1 Introduction/Job Description HIPAA Module 2 Orientation to MyKinergy Module 3 Chronic Illness: A Lifestyle Disease/Adult Education Module 4 Communication Module 5 Medications Module 6 Mental Health/ Neurologic Diseases Module 7 Red Flags Escalation Policies Module 8 Working with Families Module 9 Professional Relationships Module 10 Customer Service Module 11 Review of Specific Chronic Diseases Module 12 Use of PAM Module 13 Role of Navigator in Various Settings Module 14 How Do We Measure Success? Additional Requirements: Final Exam, 12 Hours on-the-job supervision, including monitored phone calls
14 Current Supporting Research


15 Certified Navigator role in Readmissions Reduction Recent study highlights ROI opportunity: 1,531 patients worked with a care navigator 3.16% were readmitted 4% decrease in Medicare readmissions totaling $29,702 in savings over 6 months 5% decrease in private pay readmissions totaling $127,102 in savings over 6 months Reference: Fay, et al, 2014 Lay Navigator delivers positive ROI in 3 months with Medicare and private pay patients who have known challenges with care plan compliance.
16 Use of Care Guides in achieving patient identified health goals 230 patients receiving telephone follow up with a care guide along with usual care in a weight management program. (Adams et al, 2013) Estimated cost was $286 per patient per year. Patient s with care guides achieved more goals than usual care patients (82.6% vs. 79.1%) reduced unmet goals by 30.1% compared with 12.6% for usual care patients; improved meeting several individual goals, including not using tobacco. Significant improvements in patient satisfaction scores healthier eating habits improved quality of life more success with goal attainment
17 Additional Research Supporting Effectiveness of Navigator Use of navigators has been demonstrated to: Decrease rehospitalizations (Fay & McLaughlin, 2014; NOHA 2012; Balderson & Safavi, 2013), Decrease cancelled and missed appointments (Fay & McLaughlin, 2014; NE Ohio Center for Health Affairs, 2012; Balderson & Safavi, 2013; CHA,2012). Disease specific interventions with significant findings with Navigators include: Improve control of heart failure management (Smith et al, 2008) Improved control of diabetes through measurement of A1C levels when a navigator is added to usual care (Wilson et al, 2013) Decrease in delay of treatment of breast cancer (Hoffman, et al, 2013)
18 Areas Utilizing Lay Health Navigators Certified Home Health Agencies Physician Office with CCM (Chronic Care Management) Call Centers Hospital Case Management
19 Demonstrated Uses in Certified Home Health Support case managers in meeting non-medical issues that impact health status (Social Determinants of Health) Communicate patient outcomes quickly to referral sources Focused programs on areas of patient satisfaction needing improvement via targeted intervention programs by navigators Immediate feedback of patient concerns so they are immediately resolved, increasing overall patient satisfaction
20
21
22 Areas of Focus Condition and Symptom Management (Red Flags) Medication Adherence Diet and Nutrition Physical Activity Stress and Coping Smoking Cessation
23 Home Health Care/Hospice Added Advantages Ability to maintain patient contact with health care provider to assure possible reimbursement for the next 10 years expectation of hospital admissions, readmissions. Differentiate organization from competitors due to enhanced services. Positive impact on HHCAHPS scores for Patient Satisfaction. Identify patient usage of other providers-hospitals, home care, physician through data collection. Decreased off-hour and ER visits for hospice patient
24 New Medicare rules mean new opportunities for physicians Certified Navigator Role in Medicare Chronic Care New CMS Chronic Care Management Rules Physician reimbursement ~ $42.60 per patient per month CMS estimates $130,000 -$190,000 annually per physician in new revenue generation 2+ chronic conditions CPT code Acknowledges Effectiveness of non Face-to-Face Care 20 minutes non face to face time/patient/month Delivered by care team with oversight by physician Care plan coordination among health care team, patient and family Specific patient identified goals and addressing of psycho-social issues (SDH) Requires the use of technology Provides concierge-type service
25 Role of a Navigator in Chronic Care Management (CCM) Identify qualified patients Written consent during face to face meeting Create comprehensive care plan Physical, mental, cognitive, functional, psychosocial, environmental Structured data from certified EHR 24 x 7 accessibility by entire patient care team Scope of Service Monitor and update comprehensive plan of care Medication reconciliation Communication with patient and family caregivers (24 x 7 secure accessibility) Oversee patient self-management Care team communication & coordination (specialist, home health, community) Arrange for community services = Navigator s can provide Manage care transitions and provide follow-up care Ensure preventative care services Document CCM activities by team member
26 Medication Interview Guides patient through creation of a comprehensive medication list Meds listed by condition Patient is prompted as to how to think about what they use.
27 Goals of Medication Interview 1. Assure client has all medications prescribed, understands when and how to take them. 2. Assists client in obtaining clarification of medication discrepancies by reporting to health care provider. 2. Reviews medication list with client to see if client has all of the medications listed and know which to take that day. 3. Problem solves with client to resolve common barriers to medication adherence: a) Obtaining Rx from MD b) Obtaining medication from pharmacy c) Knows when to take it. d) Is physically able to get medication out of container and take? e) Remembers when to take medication 4. Keeps medication list as One True Source by updating as appropriate.
28
29 Efficient way to grow practice and increase revenue Earn revenue of $139K+ annually per physician in your practice Strong ROI Minimal up-front fees Turnkey solutions available Reimbursement Opportunity for One Physician Number of physicians 1 Patient panel size (per physician) 2,000 % # Medicare patients 22% 440 Eligible for % 272 Per Patient Reimbursement/Mo $42.60 Reimbursement Opportunity Monthly gross revenue $11,587 Annual gross revenue $139,046

30 Improved Appointment Metrics in MD offices Pre/Post Use of Navigators
 Use of escalation policies to direct calls to appropriate level of staff Patients are better able to self-manage with")
31 Call Centers Identify and resolve non-medical issues with lower cost staff. Large % of calls are non-medical in nature (Social Determinants of Health) Use of escalation policies to direct calls to appropriate level of staff Patients are better able to self-manage with improved activation, comfort in asking questions More frequent contacts cost effective in preventing escalations/increase patient loyalty. Allow current staff to manage a greater volume of high-risk patients. Facilitate communication among patient, providers, caregivers and family. Used in support and education of family caregivers
32 Hospital Case Management
 Nearly two-thirds of the hospitalizations were due to unintentional drug overdoses from insulins oral")
33 Statistics 88.3% of emergency hospital admissions of older adults caused by adverse drug events (NEHI, 2012) Nearly two-thirds of the hospitalizations were due to unintentional drug overdoses from insulins oral antiplatelet agents, oral hypoglycemic A review of 55 observational studies found: Up to 40% of the time. medication information was missing from discharge Patients with medication discrepancies had a 30-day hospital readmission rate of 143% compared with 6.1% for patients without a medication discrepancy.

34 Navigators Post-Discharge Clarify discharge instructions and ensure care plan understanding. Ensure follow-up activities are scheduled. Provide coaching and modeling of positive health behaviors. Assure med schedule is understood and prescriptions are filled. Identify barriers or condition change and escalate.
35 High Tech/High Touch Approach Patients are better able to self-manage. Allow current staff to manage a greater volume of high-risk patients. (RPI) Measure impact on avoidable readmissions. Improve HCAPHS care transitions scores. Increase patient loyalty. Facilitate communication among patient, providers, caregivers and family.


36 Discharge Checklist for Family QUICKLY ACCESS IMPORTANT PATIENT INFO DISCHARGE INSTRUCTIONS CAN BE ATTACHED WALKS FAMILY CAREGIVER THROUGH QUESTIONS THEY NEED TO ASK PRIOR TO DISCHARGE
37 Patient Testimony to Support Navigator Intervention

38 An Introduction of How Benefits Were Realized for the Value of Health IT Patient Employee Payer Self Care Goals Medications HIPAA Compliant Targeted Health Education Interventions Patient Activation Cost Rehospitalizations ER Usage Ease of CCM Compliance
39 STEPS: Satisfaction Graphics Patient Payer Employee Satisfaction Employee Satisfaction Positive comments from Case Managers
40 STEPS: Treatment/Clinical Self-Care Goals Achieved Medication Adherence

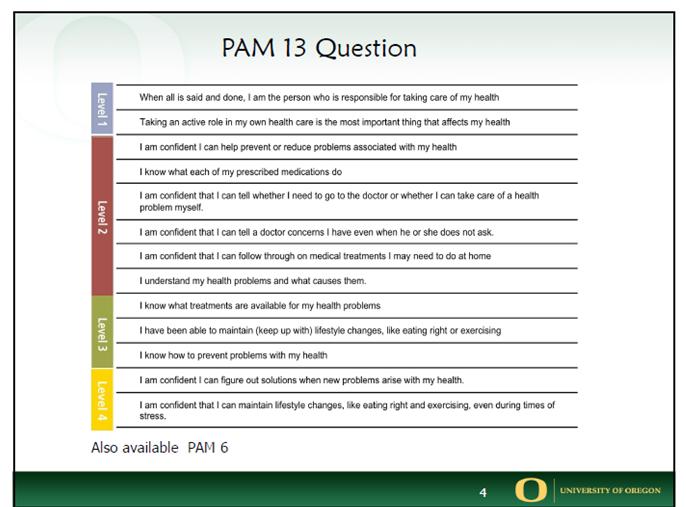
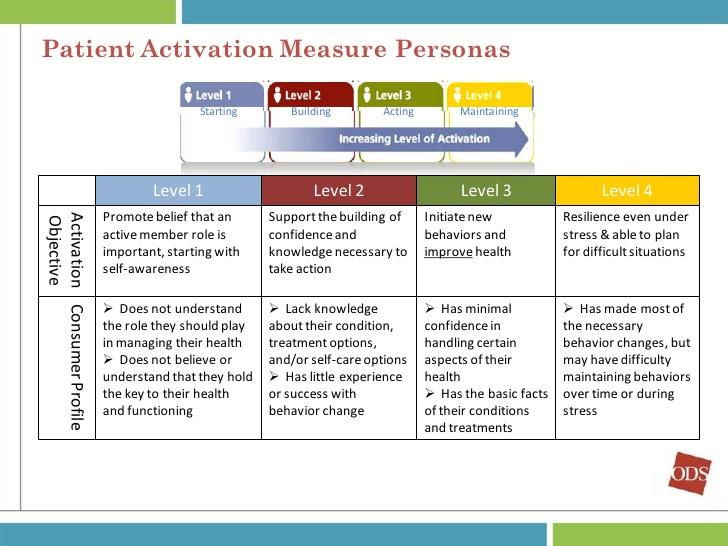
41 STEPS: Patient Engagement & Population Management Patient Activation Scores

42 STEPS: Savings ROI CCM Compliance ER Usage Rehospitalization
43 References Adams, S. et al (2013). Patient satisfaction and perceived success with a telephonic health coaching program. Preventing Chronic Disease: Public Health Research, Practice and Policy. Accessed on line November 2014 at Balderson, D & Safavi, K. (2013).How Patient Navigation Can Cut Costs and Save Lives accessed on line November, 2014 at Center for Health Affairs.(CHA), (2012). Emerging field of patient navigation: A Golden opportunity to improve health care. Accessed on line at: ewsreleases/~/media/a92355f0a6e140f1a13493bc3c349cab.ash x Fay, S. & McLaughlin, M. (2014). The Navigator in the community acute care hospital. CMSA Conference, Cleveland Ohio, accessed November, 2014 at Gunn, C. et al (2014). An Assessment of patient navigator activities in breast cancer patient navigation programs using a nine-principle framework. Health Services Research, 49(5),
44 References cont Hoffman, H. et al. (2013) Patient Navigation Significantly Reduces Delays in Breast Cancer Diagnosis in the District of Columbia. J, Epidemiol Biomarkers & Prev. 21: Hibbard, J. H., Stockard, J., Mahoney, E. R., & Tusler, M. (2004). Development of the Patient Activation Measure (PAM): Conceptualizing and Measuring Activation in Patients and Consumers. Health Services Research, 39(4 Pt 1), Morisky, D. E., Ang, A., Krousel-Wood, M., & Ward, H. J. (2008). Predictive Validity of A Medication Adherence Measure in an Outpatient Setting. Journal of Clinical Hypertension (Greenwich, Conn.), 10(5), NEHI (2013). Improving Medication adherence and reducing hospital admissions. Accessed on line at Willis, M. et al (2013). Development of a framework for patient navigation: Delineating roles across navigator types. Journal of Oncology and Navigation and Survivorship, 4(6), Wilson, F.P. & Caputo, D. (2013) ADA: Targeted Phone Calls May Help Control Diabetes. Hearings at ADA Annual Meeting.
45 6756 Old McLean Village Drive Suite 200 McLean, VA Office: Merrily Evdokimoff, RN, PhD Clinical Leader Cell: Gail Embt, MBA CEO Cell:
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Implementation Guide: Critical Interventions in the First/Second Visit. VNAA Best Practice for Home Health
 Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
The Care Transitions Intervention
 The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
The Care Transitions Intervention Kimberly Irby, MPH Colorado Foundation for Medical Care www.cfmc.org/integratingcare Acknowledgments: Objectives To provide an overview of the Care Transitions Intervention
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
Chronic Care Management
 Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
Chronic Care Management Increase Practice Revenue, While Increasing Patient Care Presented by Steven Kress CEO, Renova PCA Introduction Mr. Kress is a founding Member and Serves on the Board of Directors
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
Specialty Pharmacy: What You Need To Know. William Pong, Pharm.D., MBA
 Specialty Pharmacy: What You Need To Know William Pong, Pharm.D., MBA DISCLOSURE I have no actual or potential conflict of interest in relation to this program/ presentation OBJECTIVEs Navigating the landscape
Specialty Pharmacy: What You Need To Know William Pong, Pharm.D., MBA DISCLOSURE I have no actual or potential conflict of interest in relation to this program/ presentation OBJECTIVEs Navigating the landscape
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Chronic Care Management Coding Guidelines Effective January 1, 2017
 Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Readmissions Moving beyond blame to fill the patient needs. Jackie Conrad RN, MBA, RCC Cynosure Health
 Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Patient Navigators Skills they bring, what they do, where they work and the value they add for practices and patients
 Patient Navigators Skills they bring, what they do, where they work and the value they add for practices and patients Wanda Ali-Matlock, RN, BS, MBA, FAACM, PCMH CCE Senior Consultant Aleece Caron,PhD
Patient Navigators Skills they bring, what they do, where they work and the value they add for practices and patients Wanda Ali-Matlock, RN, BS, MBA, FAACM, PCMH CCE Senior Consultant Aleece Caron,PhD
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Administrators. Medical Directors. 61% The negative impact on our hospital-based program s. 44% We will need to consider the most appropriate or most
 2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH
 What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Chronic Care Management INFORMATION RESOURCE
 Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
Oncology Home Care: A Strategy for Growth & Improved Clinical Performance. Our Story. What s So Special About Specialty Care?
 Oncology Home Care: A Strategy for Growth & Improved Clinical Performance Bringing the best of oncology care home Our Story Oncology Care Home Health Specialists, Inc. started in 1989 in Newark, Delaware.
Oncology Home Care: A Strategy for Growth & Improved Clinical Performance Bringing the best of oncology care home Our Story Oncology Care Home Health Specialists, Inc. started in 1989 in Newark, Delaware.
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Exacerbation of Condition. VNAA Best Practice for Home Health
 Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
Exacerbation of Condition VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model. ACO Congress November 5, 2013 Charles Kennedy
 Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE
 INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Care Coordination in a no discharge system
 Care Coordination in a no discharge system Barry Bittman, MD Estes Park Institute Let s begin with a basic question. Who should be responsible? How can we align physicians with our hospital? Can we continue
Care Coordination in a no discharge system Barry Bittman, MD Estes Park Institute Let s begin with a basic question. Who should be responsible? How can we align physicians with our hospital? Can we continue
Standard #1: Internal Structure
 Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
Standard #1: Internal Structure
 Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
History of Patient Navigation 8/26/17. Cancer Navigation September 26, Agenda
 Cancer Navigation September 26, 2017 Eric T. Kimchi, MD, MBA Medical Director, Ellis Fischel Cancer Center Agenda History of Patient Navigation Principles of Patient Navigation UAB Experience EFCC Initiative
Cancer Navigation September 26, 2017 Eric T. Kimchi, MD, MBA Medical Director, Ellis Fischel Cancer Center Agenda History of Patient Navigation Principles of Patient Navigation UAB Experience EFCC Initiative
E-nabling Disease Management through IT The Next Generation of DM services
 E-nabling Disease Management through IT The Next Generation of DM services The Disease Management Colloquium Jefferson Medical College, Philadelphia, PA June 27-30, 2004 Thomas G. Lundquist, MD, MMM Executive
E-nabling Disease Management through IT The Next Generation of DM services The Disease Management Colloquium Jefferson Medical College, Philadelphia, PA June 27-30, 2004 Thomas G. Lundquist, MD, MMM Executive
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
Using Patient Activation to Transition Patients from Hospital to Home
 Using Patient Activation to Transition Patients from Hospital to Home May 2014 Mary McLaughlin Davis DNP MSN APRN ACNS-BC CCM Lakewood Hospital Cleveland Clinic Background Stroke affects an estimated 795,000
Using Patient Activation to Transition Patients from Hospital to Home May 2014 Mary McLaughlin Davis DNP MSN APRN ACNS-BC CCM Lakewood Hospital Cleveland Clinic Background Stroke affects an estimated 795,000
Metabolic & Bariatric Surgery. Nate Sann, MSN, FNP-BC
 Telemedicine in Metabolic & Bariatric Surgery Nate Sann, MSN, FNP-BC Disclosures: Apollo Endosurgery Faculty Member Exam Med Consultant Long term follow-up in Metabolic & Bariatric Surgery Obesity is a
Telemedicine in Metabolic & Bariatric Surgery Nate Sann, MSN, FNP-BC Disclosures: Apollo Endosurgery Faculty Member Exam Med Consultant Long term follow-up in Metabolic & Bariatric Surgery Obesity is a
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Chapter 2. At a glance. What is health coaching? How is health coaching defined?
 Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
Jody Hereford, BSN, MS Clinical Programs Consultant Iowa Chronic Care Consortium
 Jody Hereford, BSN, MS Clinical Programs Consultant Iowa Chronic Care Consortium 1. The role(s) of a health coach 2. Lessons from the field 3. Conclusions and strategies for action No outcome, no income.
Jody Hereford, BSN, MS Clinical Programs Consultant Iowa Chronic Care Consortium 1. The role(s) of a health coach 2. Lessons from the field 3. Conclusions and strategies for action No outcome, no income.
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Maternity Management. The best part? These are available to you at no additional cost. Intro
 Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Pharmacists Improve Care Through Team Collaboration
 Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Billing for Pharmacist Collaborative Patient Care Services
 3/9/15 SCSHP 15 Annual Meeting Disclosure Billing for Pharmacist Collaborative Patient Care Services Bob Davis, PharmD, FAPhA Professor, Kennedy Pharmacy Innovation Center, University of South Carolina
3/9/15 SCSHP 15 Annual Meeting Disclosure Billing for Pharmacist Collaborative Patient Care Services Bob Davis, PharmD, FAPhA Professor, Kennedy Pharmacy Innovation Center, University of South Carolina
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
UPMC Health Plan. Value Based Insurance Design (VBID) Spark Your Health
 Spark Your Health") UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
UPMC Health Plan Value Based Insurance Design (VBID) Spark Your Health Value Based Insurance Design (VBID) Spark Your Health Medicare Advantage Summit April 6, 2017 Helene Weinraub 1 The statements contained
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Patient and Family Caregiver Interview Tool
 Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Transforming Clinical Practices Initiative
 Transforming Clinical Practices Initiative Overview CMS through its Center for Medicare & Medicaid Innovation is launching its Transforming Clinical Practices Initiative (TCPI), which over a four-year
Transforming Clinical Practices Initiative Overview CMS through its Center for Medicare & Medicaid Innovation is launching its Transforming Clinical Practices Initiative (TCPI), which over a four-year
Oxford Condition Management Programs:
 Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
Technology Fundamentals for Realizing ACO Success
 Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
EVOLENT HEALTH, LLC. Asthma Program Description 2017
 EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
MEDICATION THERAPY MANAGEMENT. MemberChoice FORMULARY MANAGEMENT MEDICATION THERAPY MANAGEMENT (MTM) SPECIALTY DRUG MANAGEMENT
 SPECIALTY DRUG MANAGEMENT") MemberChoice FORMULARY MANAGEMENT MEDICATION THERAPY MANAGEMENT (MTM) SPECIALTY DRUG MANAGEMENT MEDICATION THERAPY MANAGEMENT Medication Therapy Management 1 $ 290 Billion Wasted in avoidable costs due
MemberChoice FORMULARY MANAGEMENT MEDICATION THERAPY MANAGEMENT (MTM) SPECIALTY DRUG MANAGEMENT MEDICATION THERAPY MANAGEMENT Medication Therapy Management 1 $ 290 Billion Wasted in avoidable costs due