Exacerbation of Condition. VNAA Best Practice for Home Health
|
|
|
- Shanon Merritt
- 6 years ago
- Views:
Transcription

1 Exacerbation of Condition VNAA Best Practice for Home Health
2 Learning Objectives The participant will be able to: Discuss two reasons why it is important to help a patient identify changes in their condition Identify two tools available to help patients/caregivers manage changes in their diseases Identify three steps that are helpful in initiating a Red Flag intervention in home health 2
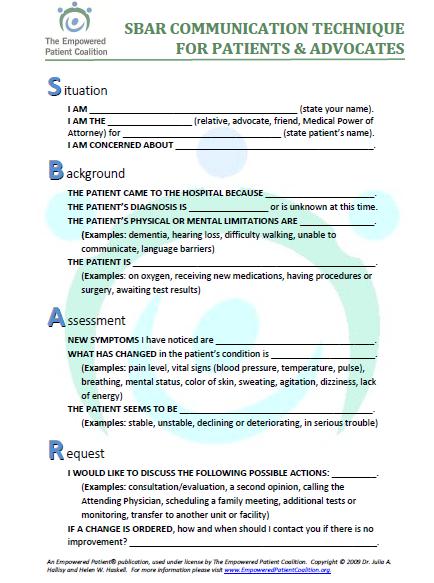
3 Why is this important? Key to prevention o Coleman s Care Transition Intervention SM Essential part of self-management Part of comprehensive plan of care o Teach back o Health literacy-sbar for patients/families 3
4 Research to support importance of managing exacerbation of condition or red flags Evdokimoff, M., (2011) found that implementation of the Four Pillars of the Coleman Care Transitions Model resulted in a 12 percentage point decrease over a 12 month time period. (Red Flags is one of the interventions) Coleman, et.al., (2006) found in a randomized control study that those patients who received the Four Pillars through encouraging patients/caregivers to assert a more active role and fostering care coordination through the use of the personal health record and visits and calls by transitional coach had significantly lower readmission rate than the control group at 30 and 90 days. 4
5 WHAT S OUT THERE? 5
6 6

7 Acute-Care-Hospitalizatio.aspx 7

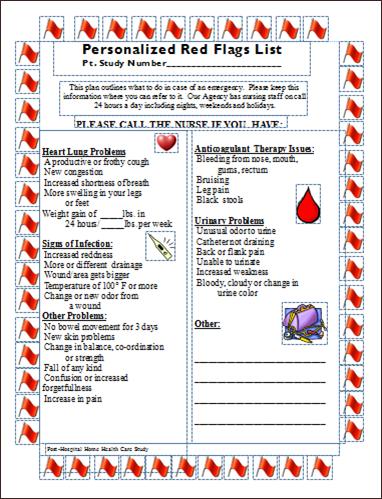
8 Stoplight tools 8

9 Emergency care plan 9

10 SBAR for staff 10
11 How to create a useful red flag intervention Make it easy to do the right thing! Embed in your processes Provide all necessary tools Plan for and measure success 11
12 Make it easy to do the right thing! Embed red flags in admission packet Make part of personal health record Place disease-specific teaching tools into the admission packet 12
13 Barriers to implementation Inconsistent processes Lack of training materials Staff reluctance Patient reluctance Limited health literacy 13
14 Embed in your processes Staff input- those closest to the issue What s in it for me? Do I have to? Recruit champions Use best practices, gold standards Identify measurements of success Provide education Don t go for perfection as the goal 14
15 Create a process map (sample) Review Med List with Patient/Family Understanding (Slide 10) All consistent Discrepancies Noted Provide updated list to patient (agency policy, include in PHR if utilized) Clinically Significant-Contact MD within 1 calendar day Other Issues to Resolve Able to reach MD and resolve Unable to reach MD Unable to Obtain Meds Patient/Family Contact other MD associated with pt. Lack of Money Agency Policy: Program in place Social Work Referral Emergency Funds available in community Contact Hospitalist/DC MD Contact MD Director of Home Care Agency Cannot Physically Obtain Meds Taxi voucher to have delivered Use of pharmacy that delivers Community Programs Program with hospital to send home with x days supply 15

16 Sample process map 16
17 Process map/helpful hints 1. Start with patient in mind 2. Identify ROI actions 3. Include not only direct provider of action, but any dept. or individual that has contact with desired outcome, any barriers, supplies needed 4. Include all hand-offs 5. Inputs must be included 6. Who are the decision makers, what do people need to do their jobs? 7. What is your goal and how will you measure it? 8. Accept variations in agency 17
18 Provide all necessary tools Tools for staff: Hospital discharge information Red flags document Access to disease-specific information Zone tools and spotlight forms Emergency care plan 18
19 Staff reluctance Collect success stories early in testing Tape record patient testimony (with permission) Provide current research Provide access to benchmarking tools: Home Health Compare Agency software company HHQI Incorporate in competency and evaluations 19
20 Provide all Necessary Tools Tools for Patient/care partner Red flags document Applicable health literacy appropriate teaching guides/booklets Zone tools and spotlight forms SBAR for patient/family Emergency plan 20
21 Health literacy Understands Red Flags-appropriate reading level How to Access Appropriate Assistance Who to Call When to Call What information to give-sbar 21
22 22
23 Clinician role Emergency plan Include parameters in orders If gains lbs in days, increase Lasix to 60mg x 3 days If pain is not relieved to a 4 or below, add (pain medication) If BS is above 250, provide additional 3 units regular insulin Use teach back to assure understanding-who and when to call Post in obvious place (refrigerator) - Family, home health aide can use Provide place for recording vs, weight, BS (calendar, vital sign record; telehealth) Share plans with patient/family Assurance calling you will not necessarily result in trip to ER Reinforce plan when call 23

24 Plan and measure for success Small tests of change: PDSA 24
25 Plan Assemble your team State aim of your test Predict what you expect to happen Develop change action 25
26 26
27 Do Carry out your plan Identify barriers, unexpected findings Analyze data Start small: 1 nurse, 1 patient 27
28 Study Study your findings: Were they what you expected? What did you learn? 28
29 Act Make change plans based on what you learned Plan next do : increase numbers involved 29
30 Where would you start? What is my aim/desired outcome? Where are your champions? Where most likely to meet success? Who else is interested in this? How will I measure success? 30
31 Measurement Percent of patients who have symptom exacerbation/red flags document completed (choose which document for review in patient chart) Review could be of Red Flags Worksheet, Emergency Plan or Zone Tools/Spotlight Tools 31
Implementation Guide: Critical Interventions in the First/Second Visit. VNAA Best Practice for Home Health
 Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Pave Your Path: Improvement Science & Helpful Techniques
 Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Meeting Proposed Home Health Conditions of Participation by Applying Integrated Care Management Tools and Competencies
 Meeting Proposed Home Health Conditions of Participation by Applying Integrated Care Management Tools and Competencies Beth Hennessey, BSN, MSN Paula Suter, RN, BSN, MA Sutter Center for Integrated Care
Meeting Proposed Home Health Conditions of Participation by Applying Integrated Care Management Tools and Competencies Beth Hennessey, BSN, MSN Paula Suter, RN, BSN, MA Sutter Center for Integrated Care
Care Transition Coach
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Care Transition Coach Marlene Seidel Butz Lehigh Valley Health Network, Marlene.Butz@lvhn.org Follow this and additional
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Care Transition Coach Marlene Seidel Butz Lehigh Valley Health Network, Marlene.Butz@lvhn.org Follow this and additional
Care Transitions Partnerships that Work for Patients
 Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
Care Transitions Partnerships that Work for Patients Alyce Brophy, President/CEO, Community Visiting Nurse Association Alyssa Kizun, Director, Care Management, Somerset Medical Center Stacey Wilbur, Administrator,
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Tools Use Suggested Formats. All facility staff Provides a visual depiction of INTERACT in daily practice
 INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
4/26/2017. I ll Do It My Way, Thank You Performance Improvement Strategies for Home Care. Session Objectives. Session Agenda
 I ll Do It My Way, Thank You Performance Improvement Strategies for Home Care Barbara Katz, RN, MSN President, BK Health Care Consulting, LLC www.bkhealthconsulting.com Session Objectives Explain the role
I ll Do It My Way, Thank You Performance Improvement Strategies for Home Care Barbara Katz, RN, MSN President, BK Health Care Consulting, LLC www.bkhealthconsulting.com Session Objectives Explain the role
Putting the Patient at the Center of Care
 CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CMMI Innovation Advisor Paula Suter, Sutter Care at Home: Putting the Patient at the Center of Care Paula Suter, of Sutter Care at Home, joins the Alliance for a discussion of her work with the Center
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Improving Transitions to Home & Community- Based Care Settings
 This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
This presenter has nothing to disclose. Improving Transitions to Home & Community- Based Care Settings Eric Coleman September 29, 2015 Session Objectives Participants will be able to: Describe the role
Improving Care Transitions for Rhode Island Patients
 Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
Improving Care Transitions for Rhode Island Patients Nelia Odom, RN, BSN, MBA, MHA Senior Program Coordinator, Quality Partners of Rhode Island Deborah Correia Morales, MSW Senior Program Coordinator,
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Care Continuum or Unconnected Silos
 Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE
 CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES
 VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES Care Initiation: Critical Interventions VNAA Best Practice for Hospice and Palliative Care The first few days following a patient s admission to
VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES Care Initiation: Critical Interventions VNAA Best Practice for Hospice and Palliative Care The first few days following a patient s admission to
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Advance Care Planning: Goals of Care - Calgary Zone
 Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients
 Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
Solution Title: Population Health: A Paradigm Shift in how we care for Behavioral Health Patients Overview of Project A drive to Population Health and changes in reimbursement have prompted the need to
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings.
 Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Person-Centered Models for Assuring Quality and Safety During Transitions Across Care Settings. Written Testimony to the United States Senate Special Committee on Aging Senator Herb Kohl, Chair Hearing
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Care Initiation: Crisis Management
 VNAA Blueprint for Excellence Pathway to Best Practices Care Initiation: Crisis Management VNAA Best Practice for Hospice and Palliative Care: End of Life This presentation addresses crisis management
VNAA Blueprint for Excellence Pathway to Best Practices Care Initiation: Crisis Management VNAA Best Practice for Hospice and Palliative Care: End of Life This presentation addresses crisis management
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing
 Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing Course Description, Student Learning Outcomes and Competencies, Clinical Evaluation Tool, and Clinical Activities
Merced College Registered Nursing 34: Advanced Medical/Surgical Nursing and Pediatric Nursing Course Description, Student Learning Outcomes and Competencies, Clinical Evaluation Tool, and Clinical Activities
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
M7: Improving Transitions and Reducing Avoidable Rehospitalizations. St. Luke s Hospital Member, Iowa Health System
 M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
M7: Improving Transitions and Reducing Avoidable Rehospitalizations Peg M. Bradke, RN, MA St. Luke s Hospital, Cedar Rapids, Iowa This presenter has nothing to disclose. St. Luke s Hospital Member, Iowa
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
FY 2016 PERFORMANCE PLAN
 Program Purpose PERFORMANCE PLAN ADSD Amy Vennett x1714 Program Information Improve and then maintain the health status of adults with multiple chronic illnesses and/or disabilities so they successfully
Program Purpose PERFORMANCE PLAN ADSD Amy Vennett x1714 Program Information Improve and then maintain the health status of adults with multiple chronic illnesses and/or disabilities so they successfully
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System
 Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Digital Transformation of MOLST: Getting Started and Ensuring Sustainability
 Digital Transformation of MOLST: Getting Started and Ensuring Sustainability Speakers Patricia Bomba, MD, MACP Vice President and Medical Director, Geriatrics, Excellus BlueCross BlueShield Chair, MOLST
Digital Transformation of MOLST: Getting Started and Ensuring Sustainability Speakers Patricia Bomba, MD, MACP Vice President and Medical Director, Geriatrics, Excellus BlueCross BlueShield Chair, MOLST
5/1/2017 THE BEST DEFENSE IS A GOOD OFFENSE OBJECTIVES. Preparing for a Home Health Medicare Recertification Survey
 THE BEST DEFENSE IS A GOOD OFFENSE Preparing for a Home Health Medicare Recertification Survey OBJECTIVES To gain an understanding how the Medicare Conditions of Participation (CoPs), the individual G-tags,
THE BEST DEFENSE IS A GOOD OFFENSE Preparing for a Home Health Medicare Recertification Survey OBJECTIVES To gain an understanding how the Medicare Conditions of Participation (CoPs), the individual G-tags,
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
The Colorado ALTO Project
 Using Alternatives to Opioids (ALTOs) in Hospital Emergency Departments PRE-LAUNCH CHECKLIST Based on the 2017 Opioid Prescribing & Treatment Guidelines Colorado ALTO Project Champion Sets the direction
Using Alternatives to Opioids (ALTOs) in Hospital Emergency Departments PRE-LAUNCH CHECKLIST Based on the 2017 Opioid Prescribing & Treatment Guidelines Colorado ALTO Project Champion Sets the direction
SELF-REPORTING TOOL: Procedural Areas
 Page 1 of 7 SELF-REPORTING TOOL: Procedural Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses patient safety needs
Page 1 of 7 SELF-REPORTING TOOL: Procedural Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses patient safety needs
Community Counseling Centers, Inc. & North Country Health Care
 Community Counseling Centers, Inc. & North Country Health Care Holbrook & Show Low Navajo County Communities 9/28/11 The CCC multi-faceted approach to an integrated health program with North Country Health
Community Counseling Centers, Inc. & North Country Health Care Holbrook & Show Low Navajo County Communities 9/28/11 The CCC multi-faceted approach to an integrated health program with North Country Health
A Pilot Study in Performance Improvement CME: Using an Electronic Health Record for Guided Self Assessment and Learning
 A Pilot Study in Performance Improvement CME: Using an Electronic Health Record for Guided Self Assessment and Learning Joseph L. Seltzer, MD Jeanne G. Cole, MS Nothing to disclose Timely Administration
A Pilot Study in Performance Improvement CME: Using an Electronic Health Record for Guided Self Assessment and Learning Joseph L. Seltzer, MD Jeanne G. Cole, MS Nothing to disclose Timely Administration
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
SELF-REPORTING TOOL: Procedural Areas
 Page 1 of 6 SELF-REPORTING TOOL: Procedural Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses patient safety needs
Page 1 of 6 SELF-REPORTING TOOL: Procedural Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses patient safety needs
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure
 Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
SELF-REPORTING TOOL: Outpatient Areas
 Outpatient Self Report Page 1 of 7 SELF-REPORTING TOOL: Outpatient Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses
Outpatient Self Report Page 1 of 7 SELF-REPORTING TOOL: Outpatient Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB)
") AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB) HAZLETON GENERAL HOSPITAL HAZLETON, PENNSYLVANIA PRESENTERS:
AN OVERVIEW of TARGET HF: QUALIFYING for the HONOR ROLL and a DETAILED FOCUS on MEDICATION COMPLIANCE (ACE/ARB, ADLOSTERONE ANTAGONIST, and EBBB) HAZLETON GENERAL HOSPITAL HAZLETON, PENNSYLVANIA PRESENTERS:
10/27/10. Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch. pulmonary edema. sodium intake & daily weights
 Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch pulmonary edema sodium intake & daily weights 1 What makes her at risk for readmission? Why didn t she listen to her doctors about her salt intake? Did
Quality Improvement/PBLI in Residency Using Continuity Clinic as the Site- APPD Workshop 10
 Quality Improvement/PBLI in Residency Using Continuity Clinic as the Site- APPD Workshop 10 Mary Kay Kuzma, Raj Donthi and John D Mahan, Nationwide Children s Hospital Columbus, Ohio ACGME Competency Practice
Quality Improvement/PBLI in Residency Using Continuity Clinic as the Site- APPD Workshop 10 Mary Kay Kuzma, Raj Donthi and John D Mahan, Nationwide Children s Hospital Columbus, Ohio ACGME Competency Practice
Hospice Discharges. Legacy Hospice
 Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
5/3/2017. QAPI Quality and Compliance HOSPICE. Hospice Quality Reporting Program QAPI & HQRP: DIFFERENCES AND SIMILARITIES
 QAPI Quality and Compliance HOSPICE Katie Wehri, CHPC Director of Operations Consulting Healthcare Provider Solutions Kwehri@healthcareprovidersolutions.com QAPI & HQRP: DIFFERENCES AND SIMILARITIES Hospice
QAPI Quality and Compliance HOSPICE Katie Wehri, CHPC Director of Operations Consulting Healthcare Provider Solutions Kwehri@healthcareprovidersolutions.com QAPI & HQRP: DIFFERENCES AND SIMILARITIES Hospice
ACTIVITY DISCLAIMER DISCLOSURE. Learning Objectives. Tools for Improving Access and Continuity. Tools to improve access and continuity
 ACTIVITY DISCLAIMER Tools for Improving Access and Continuity Jean Antonucci, MD The material presented here is being made available by the American Academy of Family Physicians for educational purposes
ACTIVITY DISCLAIMER Tools for Improving Access and Continuity Jean Antonucci, MD The material presented here is being made available by the American Academy of Family Physicians for educational purposes
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
SELF-REPORTING TOOL: Outpatient Areas
 LPN Outpatient Self Report Page 1 of 8 SELF-REPORTING TOOL: Outpatient Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses
LPN Outpatient Self Report Page 1 of 8 SELF-REPORTING TOOL: Outpatient Areas Subject s Name: Evaluator s Name: Requires Evaluation Descriptors (Quality & ) for reference PLANNING & MANAGING CARE 1. Addresses
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 2/27/2013 2010, American Heart Association 2 1
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 2/27/2013 2010, American Heart Association 2 1
Partnering with Patients in Medication Safety
 Partnering with Patients in Medication Safety February 6 th, 2018 PPC 2018 Alice Watt, RPh. B.Sc (Pharm) ISMP Canada ISMP Canada 1 Presenter Disclosure Presenter s Name: Alice Watt I have no current or
Partnering with Patients in Medication Safety February 6 th, 2018 PPC 2018 Alice Watt, RPh. B.Sc (Pharm) ISMP Canada ISMP Canada 1 Presenter Disclosure Presenter s Name: Alice Watt I have no current or
Clinical Safety & Effectiveness Cohort # 8
 Clinical Safety & Effectiveness Cohort # 8 1 IMPROVING THE TIMELINESS OF PARACENTESIS: IMPACT OF A PROCEDURE TEAM DATE Educating for Quality Improvement & Patient Safety FINANCIAL DISCLOSURE Patricia Wathen,
Clinical Safety & Effectiveness Cohort # 8 1 IMPROVING THE TIMELINESS OF PARACENTESIS: IMPACT OF A PROCEDURE TEAM DATE Educating for Quality Improvement & Patient Safety FINANCIAL DISCLOSURE Patricia Wathen,
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now!
 Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
Adopting Standardized Definitions The Future of Data Collection and Benchmarking in Alternate Site Infusion Must Start Now! Connie Sullivan, RPh Infusion Director, Heartland IV Care Lyons, CO CE Credit
SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS?
 Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Who are we? Why are we here? SO YOU WANT TO IMPROVE THE DISCHARGE PROCESS? Michelle Mourad MD Arpana Vidyarthi Ellen Kynoch Oh Betty Why Betty? pulmonary edema sodium intake & daily weights What makes
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TeamSTEPPSCM. Strategies & Tools to Enhance Performance and Patient Safety
 TeamSTEPPSCM Strategies & Tools to Enhance Performance and Patient Safety Agency for Healthcare Research and Quality Advancing Exce fence in Health Care www.ahrq.gov TeamSTEPPS Team Competency Outcomes
TeamSTEPPSCM Strategies & Tools to Enhance Performance and Patient Safety Agency for Healthcare Research and Quality Advancing Exce fence in Health Care www.ahrq.gov TeamSTEPPS Team Competency Outcomes
10/12/2011. Hospital Admissions. Length of stay. Patient and caregiver knowledge Patient empowerment
 How the Transition Coach Model is employed at United Memorial Medical Center Amy Snyder RN Since our program started at United Memorial Medical Center 2009 21 Home Visits 2010 60 Home Visits 2011 51 Home
How the Transition Coach Model is employed at United Memorial Medical Center Amy Snyder RN Since our program started at United Memorial Medical Center 2009 21 Home Visits 2010 60 Home Visits 2011 51 Home
3/30/2015. Objectives. Rationale for QAPI. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 2 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP, CDE
 Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP, CDE Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP,
Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP, CDE Integrating the LLM / JCPP-PPCP Seena Haines, PharmD, BCACP,