4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
|
|
|
- Raymond Greene
- 5 years ago
- Views:
Transcription


1 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS. This handout is intended for use by this audience only. Please do not distribute. After the presentation the learner will be able to: 1. Describe the role of nursing home leaders on cross-continuum teams Explain how a QAPI program such as INTERACT, when fully implemented, may lead to reduced avoidable hospitalizations, improved quality of care and quality of life Discuss how use of the Advancing Excellence hospitalization quality measure can help an organization to meet the intent of the Affordable Care Act (ACA) nursing home QAPI provision 1





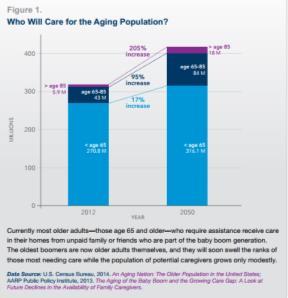
2 How can we transform our communities so that people have a choice about how and where they age? How can we ensure quality of life during transitions for the most vulnerable older adults and their caregivers? Health and Well-being Model Deeper dive into the issue: Who are all these old people and where did they come from????? 2


3 3





4 4



5 The demand for direct-care workforce is set to increase by 48% over the next decade This demand and lack of retention could lead to a shortage Turnover and issues with access create particular problems during care transitions 5

 Lack of")


6 Specifically: lack of affordable and accessible housing, transportation, nutrition programs (meals on wheels) Lack of behavioral/mental health services Need for personal attendant service/additional service hours Need to acquire independent living skills prior to transition Many others 6


7 What tools and systems will you use to understand your data and make meaningful changes based on that data? How will you excite your staff around using data? Advancing Excellence Hospitalization Tool Preferences for Everyday Living Inventory (PELI) Consistent assignment tool Having the same caregivers makes a difference! Staff stability High turnover may lead to ineffective transitions. It may also put facility at risk of deficiency citations on surveys, risk of more complaints from residents, families 7
 Early data showed cost savings of about $5,000 per patient in frail older adults with CHF Care management whatever it takes 8")
8 Care Transitions Model Four pillars Dynamic, person-centered record Medical self-management Follow up Red flags Care management (coaching model) CTM-3 measure Transitional Care Model Uses APRNs with high risk populations (e.g., CHF, dementia, SMI) Early data showed cost savings of about $5,000 per patient in frail older adults with CHF Care management whatever it takes 8
.")
9 The INTERACT Quality Improvement Program A Practical Approach To Safely Reducing Rehospitalizations Thanks to Laurie Herndon, APRN-BC, GNP The INTERACT Program and Tools were initially developed by Joseph G. Ouslander, MD and Mary Perloe, MS, GNP at the Georgia Medical Care Foundation with the support of a contract from the Centers for Medicare & Medicaid Services (CMS). The current version of the INTERACT Program was developed by members of the INTERACT interdisciplinary team under the leadership of Dr. Joseph G. Ouslander, M.D. with input from many direct care providers and national experts in projects based at Florida Atlantic University (FAU) supported by The Commonwealth Fund. INTERACT Strategies 1. Prevent conditions from becoming severe enough to require hospitalization through early identification and evaluation of changes in resident condition 2. Manage some conditions without transfer when this is feasible and safe 3. Improve advance care planning and the use of palliative care plans when appropriate as an alternative to hospitalization for some residents 4. Improve documentation and communication within LTC facilities and programs, and between LTC and acute care 9

 Medicare SNF Rehospitalizations: Implications for Medicare")



10 Rehospitalizations of SNF Residents are Common and Costly 1 in 4 patients admitted to a SNF are re-admitted to the hospital within 30 days at a cost of $4.3 billion Source: Mor, et al. (2010) Medicare SNF Rehospitalizations: Implications for Medicare Payment Reform, Health Affairs. Why Does This Matter? Hospitalization At the beauty salon At risk for complications Delirium Polypharmacy Falls Incontinence and catheter use Hospital acquired infections Immobility, de-conditioning, pressure ulcers Some Hospitalizations and Readmissions are Avoidable Several studies suggest that a substantial percent of hospital transfers, admissions, and readmissions are unnecessary and can be prevented 30 10
.")

11 Background: Many Are Avoidable Subjects: The population of interest is a cohort of long-stay NH residents. Data are from the Nursing Home Stay file, a sample of residents in 10% of certified NHs in the United States ( ). Results: Three fifths of hospitalizations were potentially avoidable and the majority was for infections, injuries, and congestive heart failure. Medical Care: August Volume 51 - Issue 8 - p doi: /MLR.0b013e bff Changes in Medicare and Health Care Financing are Changing Incentives Pay-for-Performance ( P4P ) No payment for certain complications; disincentives for avoidable hospitalizations Bundling of payments for episodes of care Accountable Care Organizations that include hospitals, physicians, home health agencies, and SNFs that are responsible for the care of a defined group of patients State Duals Programs and Medicaid Managed Care Other models e.g. most recent CMS contracts for reducing unnecessary hospitalizations of long-stay NH residents The Bottom Line Collaboration among hospitals and community-based providers is essential for improving transitions between care settings and keeping discharged patients out of the hospital. Fostering partnerships among providers, payers, and health plans can help identify causes of avoidable rehospitalizations and align programs and resources to address them A. E. Boutwell, M. B. Johnson, P. Rutherford et al., "An Early Look at a Four-State Initiative to Reduce Avoidable Hospital Readmissions," Health Affairs, July (7):
12 Quality Improvement Tools Communication Tools Decision Support Tools Advance Care Planning Tools CMS Pilot Study Results 1. Tools and implementation strategies were pilot tested in 3 Georgia NHs with relatively high hospitalization rates 2. Tools were acceptable to staff 3. Significant reduction in hospitalizations 4. Significant reduction in transfers rated as avoidable by an expert panel Ouslander et al: J Amer Med Dir Assoc 9: , 2009 Implementation Model in the Commonwealth Fund Grant Collaborative On site training (part of one day) Facility-based champion Collaborative phone calls with up to 10 facility champions twice monthly facilitated by an experienced nurse practitioner Availability for telephone and consults Completion and faxing of QI Review Tools 12


 3.")
 4.01 3.")
 3.")
13 Commonwealth Fund Project Results Facilities Mean Hospitalization Rate per 1000 resident days Mean Change Relative Reduction in All- Cause Hospitalizations Pre intervention During Intervention p value All INTERACT facilities (N = 25) % Engaged facilities (N = 17) % Not engaged facilities (N = 8) % Ouslander et al, J Am Geriatr Soc 59: ,





14 How many transfers from your nursing home? When do they occur? How many days since admit? Ah ha moments Online version Root Cause Analysis: The Rest of the Story Demographics What happened Contributing factors Attempts to manage in SNF Avoidable? Staff thoughts about this Opportunities for improvement Cross continuum review of cases Enhanced Nursing Assessment Builds on early recognition Standard approach MD/NP response Warm hand over How might this complement disease management? 14





15 Communication Tools Across Settings Nursing Home Capabilities Checklist Medication Reconciliation Worksheet Transfer forms both directions Data lists both directions Can use as platform to start discussion about which elements nurses will use for warm hand off Returned Unopened Poor Communication=Poor Outcomes Decision Support Tools 15





16 Decision Support Tools For the SNF: one unit For the hospital: one SNF For HH/AL: one case For surveyors: one conversation For all: one CC meeting The Important Role of Your Facility Team Facility Leaders: Improving Relationships Direct Care Staff: Improving Quality of Care 16
.")
17 Connect across provider types within each community Take the initiative don t wait for an invitation Use existing resources Hospital Engagement Networks (HENs) State Coalitions to Improve Dementia Care Quality Improvement Networks (QINs, formerly QIOs). National Nursing Home Quality Care Collaborative (NNHQCC) change package Advancing Excellence Local Area Networks for Excellence (LANEs) Create the change you want to see! Model the attitudes and behaviors you would like to see in your staff Be visible Send a clear, consistent message about your organization s philosophy around transitions Ask questions ( what do you need from me? What is most broken what needs to be fixed first? How can we be the best at getting better? ) Help staff embrace measuring improvement Take action but don t try to do everything all at once. Start with small steps but keep going! Facility Leaders Be prepared Initiate contact Know your data Share your story Know what tools, data, information you want to share Set date for next meeting 17



18 Lots of interest in this form Bring it with you Offer to update regularly Be sure you can do what you say you can It is not about the forms: It is about the relationship Enhancing the relationship by using the Warm Hand Over The Warm Hand Over The Power of One One SNF nurse One hospital nurse One meeting One trial How did it go? Modify Try again Spread Results Are Shared Cross Continuum Meeting Frontline work intersects with work of leadership= improved care 18


19 Person-centered Nurse led APRN supported Evidence is building Scalable Initiative to Reduce Avoidable Hospitalizations of Nursing Facility Residents 4 year initiative 15 partner facilities required, with average census >100 residents Focus is long stay, dual eligible residents Funded through the CMS Innovation Center and Medicare-Medicaid Coordination Office Approximately $100 million for 7 projects IU Geriatrics Optimizing Patient Transfers, Impacting Medical Quality, and Improving Symptoms: Transforming Institutional Care $13.4 million over 4 years 19 partner facilities (~2000 residents) Independents, regional and national chains represented Greg Sachs & Kathleen Unroe Project Directors 19
20 Reduction in avoidable hospitalizations of long stay nursing home residents through: improving medical care, enhancing transitional care and access to palliative care RNs are embedded in each facility to lead delivery of the intervention, supported in managing residents by NPs who cover a group of facilities Unroe et al, JAGS 2014 RNs (18) placed at each facility to lead delivery of the intervention, supported in managing residents by NPs (6) who cover a group of facilities 2 RN managers (one with 50% and one 25% managerial time) IU Geriatrics Dedicated to one building Full-time Monday-Friday Quality Improvement champion Mentorship in clinical assessment for facility staff Liaison to the NP IU Geriatrics 20
21 Acute Change in Condition INTERACT implementation; mentoring and coaching Support NPs identify patients; communication Advance Care Planning 2-3 patients per week Collaborative Care Reviews gather information Quality Improvement transfer root cause analyses; integrate into the QI facility efforts IU Geriatrics Cover 4-5 facilities Available 10am-6pm Monday-Friday; 8-12 on weekends Ability to see residents with a change in status or identified by RN as needing evaluation discussing with PCP Resident, family, staff education IU Geriatrics Acute change in condition Transition Visits Collaborative Care Reviews Support RN in education efforts IU Geriatrics 21
 Wall mounted")
, light level, noise level")
, weight, BP, SaO2 Drs.")
22 IU Geriatrics Wrist worn devices physical activity (time, distance, calories, steps), sleep quality, temperature, galvanic skin response, heart rate, heart rate variability ) Wall mounted sensors motion, activity level, inferred behaviors, nicotine in air, etc. Smart phone Location, orientation, distance, voice quality (mood), light level, noise level Others clothing (ECG, respiration, ), tatoos (blood glucose), contact switches, computer interactions (cognitive measures), weight, BP, SaO2 Drs. Holly Jimison & Misha Pavel Home health based on unobtrusive, continuous monitoring 22



23 Pavel et al., IEEE Special Issue, in press 67 Activity Monitoring in the Home Sensor Events Private Home Bedroom Bathroom Living Rm Front Door Kitchen Hayes et al., Hayes, ORCATECH 2007 In 2013, 15.5 million caregivers provided over 17.7 billion hours of unpaid care Valued at more than $220 billion The vast majority of caregivers are women Caregivers had over 9.3 billion in additional health care costs of their own 60% of caregivers rate the emotional stress of caregiving as high or very high; more than 1/3 report symptoms of depression 23






24 Most care provided in the community by family members or others Some through state Medicaid waiver programs ( money follows the person, community first and others) Only about 5% of older adults (about 1.5 million people) live in nursing homes So what are some of the clinical and social issues that could benefit from innovation? Respite, falls, incontinence, self-care/selfmanagement, exercise, cognitive games, medication management The future is now. Payment reform is driving change. Acute care hospitals are very interested in what is going on in post-acute care and are asking about care coordination and programs for care transitions Inform your local hospitals and other partners and help develop a dynamic working relationship Be the leaders in innovation! 24



25 Photo: Alex Tenappel 25
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT
 Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Avoidable Hospitalizations INTERACT, PACE, RA+IT Richard G. Stefanacci, DO, MGH, MBA, AGSF, CMD Thomas Jefferson University Jefferson School of Population Health Chief Medical Officer The Access
Reducing Potentially Avoidable Hospitalizations of Nursing Home Residents
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Florida Atlantic University Assistant Dean for
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN 2015-2016 UCSF Presidential Chair Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
A Journey from Evidence to Impact
 1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
1 TRANSITIONAL CARE MODEL A Journey from Evidence to Impact Mary D. Naylor, Ph.D., RN Marian S. Ware Professor in Gerontology Director, NewCourtland Center for Transitions and Health University of Pennsylvania
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR
 CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
An Innovative Approach to Identifying and Communicating Change of Condition
 An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
An Innovative Approach to Identifying and Communicating Change of Condition Introduction to INTERACT II Presenters Cathy Lipton, Senior Medical Director, Evercare, cathy_lipton@uhc.com Pam O Rourke, VP
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
February 27, Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models
 1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
1 February 27, 2014 Mobilizing Skilled Nursing Facilities to Reduce Avoidable Rehospitalization: New Imperatives and New Models 2 Having Audio Issues? If you experience any disruptions or other issues
Postacute care (PAC) cost variation explains a large part
 cost variation explains a large part") INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Long-Term Care Program
 Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
Long-Term Care Program Long-Term Care Program p.1 Program Overview Nurses Improving Care for Healthysystem Elders (NICHE) is a nursing education and consultation program designed to improve geriatric
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services
 Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Spreading INTERACT Practices Across the Continuum Through Skilled Nursing, Assisted Living, Home Health and Homes With Services Kevin W. O Neil MD, FACP, CMD Internal Medicine and Geriatrics Chief Medical
Presentation Objectives
 Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
Quality Improvement and Value-Based Purchasing (VBP) How your QI program can prepare you for transformation Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality
OPTIMISTIC 8/13/2014. Outline OBJECTIVES
 OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
OPTIMISTIC An Approach to Increasing Quality of Life for Long Term Care Residents Presented by Noadiah Malott RN,MSN,ACNP-BC Project NP School of Medicine Department of Medicine Division of General Internal
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound
 Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
Palliative Care in the Skilled Nursing Facility Setting: Opportunities Abound Date: February 1, 2017 Jennifer Judson, Project Lead: Palliative Care Jennifer Hodge, HIIN Quality Specialist 1/18/2017 2 Objectives
INTERACT for Assisted Living
 INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
INTERACT for Assisted Living Part 1 NYSHFA/NYSCAL 2014 Fall Conference & Trade Show LuAnne Leistner MS, RN, BC, NE, BC, CALN Director Clinical Services- Assisted Living/Brookdale November 20, 2014 1 Bio/Disclosures
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Why Develop Some Local Management of Services for Frail Elderly Persons?
 12:30 1:30 PM Managing and Measuring 1 Why Develop Some Local Management of Services for Frail Elderly Persons? 1. Local entities could integrate social supports and health care 2. Local entities could
12:30 1:30 PM Managing and Measuring 1 Why Develop Some Local Management of Services for Frail Elderly Persons? 1. Local entities could integrate social supports and health care 2. Local entities could
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 13, a top Medicare official testified that while readmission rates had remained steady for the past five years at
Thank You for Joining!
 Thank You for Joining! Learning Series 2: Improving Dementia Care New England Nursing Home Quality Care Collaborative Webinar Will Begin Shortly. Call-In Number: (888) 895-6448 Access Code: 5196001 2/10/2016
Thank You for Joining! Learning Series 2: Improving Dementia Care New England Nursing Home Quality Care Collaborative Webinar Will Begin Shortly. Call-In Number: (888) 895-6448 Access Code: 5196001 2/10/2016
THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT
 April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
April 13, 2018 The Misadventures of the Recently-Discharged Older Adult THE MISADVENTURES OF THE RECENTLY-DISCHARGED OLDER ADULT Robert E. Burke MD, MS April 13, 2018 I have no conflicts of interest to
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Presentation Objectives
 Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Creating Connections: Use of HIT to Link Nursing Homes into the Care Continuum
 Creating Connections: Use of HIT to Link Nursing Homes into the Care Continuum Mary Jane Koren, M.D., M.P.H. Vice President, Delivery System Reform The Commonwealth Fund Grantmakers in Aging Annual Conference
Creating Connections: Use of HIT to Link Nursing Homes into the Care Continuum Mary Jane Koren, M.D., M.P.H. Vice President, Delivery System Reform The Commonwealth Fund Grantmakers in Aging Annual Conference
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
NDNQI Rhythms in Quality 2010 Data Use Conference
 NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
Measure Applications Partnership (MAP)
") Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling. Speaker: Thomas Martin November 2014
 Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Accountable Care in Infusion Nursing. Hudson Health Plan. Mission Statement. for all people. INS National Academy of Infusion Therapy
 Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
with Food, Nutrition, and Dining
 by Brenda Richardson, MA, RDN, LD, CD, FAND 1 HOUR CE CBDM Approved Reducing Hospital Admissions with Food, Nutrition, and Dining NUTRITION CONNECTION FOOD, NUTRITION, AND DINING ARE INTEGRAL COMPONENTS
by Brenda Richardson, MA, RDN, LD, CD, FAND 1 HOUR CE CBDM Approved Reducing Hospital Admissions with Food, Nutrition, and Dining NUTRITION CONNECTION FOOD, NUTRITION, AND DINING ARE INTEGRAL COMPONENTS
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #53 Assess and Educate to Prevent Rehospitalizations Thursday, August 8 10:00 to 11:30 a.m. Regency 1 Upon
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
The Role of Pharmacy in Alternative Payment Models
 The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
New Opportunities for Case Management Leadership in our Changing Environment
 New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017
 NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
10/22/2015. QIO Program Restructures. QIO Program Restructures ANHA Activities/Social Services Convention Person-Centered Care
 2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Pay-for-Performance. GNYHA Engineering Quality Improvement
 Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS
 PROVIDERS") Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS Navigation To Start the training, please press Function + F5 To advance through each slide use the icon located at the
Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS Navigation To Start the training, please press Function + F5 To advance through each slide use the icon located at the
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
OneCare Model of Care
 OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
Checklist: What Can My Organization Do?
 Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Defining and Driving Value: Provider and Payer Perspectives
 Defining and Driving Value: Provider and Payer Perspectives NAHC Financial Managers Meeting June 2013 Serving the Midcoast of Maine in Knox Waldo Lincoln Counties 1 Who we are... Medicare Certified & State
Defining and Driving Value: Provider and Payer Perspectives NAHC Financial Managers Meeting June 2013 Serving the Midcoast of Maine in Knox Waldo Lincoln Counties 1 Who we are... Medicare Certified & State
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
Agenda. ACMA A Strong Base
 New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
Florida Health Care Association 2013 Annual Conference
 Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
Florida Health Care Association 2013 Annual Conference The Westin Diplomat Resort & Spa Session #51 Navigating Health Care Reform: Creating a Road Map for Success Thursday, August 8 8:15 to 9:45 a.m. Regency
The Coalition of Geriatric Nursing Organizations
 - The Coalition of Geriatric Nursing Organizations Representing 28,700 Nurses American Academy of Nursing (AAN) Expert Panel on Aging American Assisted Living Nurses Association (AALNA) American Association
- The Coalition of Geriatric Nursing Organizations Representing 28,700 Nurses American Academy of Nursing (AAN) Expert Panel on Aging American Assisted Living Nurses Association (AALNA) American Association
Person-Centered Accountable Care
 Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care
 Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Nursing Home Labor Market Issues. Testimony for the Institute of Medicine Committee on the Future of Health Care Workforce for Older Americans
 UCSF Nursing Home Labor Market Issues Testimony for the Institute of Medicine Committee on the Future of Health Care Workforce for Older Americans Charlene Harrington, Ph.D., R.N., FAAN Professor of Nursing
UCSF Nursing Home Labor Market Issues Testimony for the Institute of Medicine Committee on the Future of Health Care Workforce for Older Americans Charlene Harrington, Ph.D., R.N., FAAN Professor of Nursing
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home. Your thoughts
 Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
Smooth Moves: Stimulating Mindful Transitions from Hospital to Nursing Home Cari Levy, MD, PhD University of Colorado Department of Medicine Division of Health Care Policy and Research Denver- Seattle
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Developing an Organizational QAPI Plan
 Developing an Organizational QAPI Plan Kathleen Lavich, R.N. Senior Clinical Quality Consultant MPRO LeadingAge Michigan - 2017 Annual Conference and Trade Show MPRO: Our Work QUALITY IMPROVEMENT REVIEW
Developing an Organizational QAPI Plan Kathleen Lavich, R.N. Senior Clinical Quality Consultant MPRO LeadingAge Michigan - 2017 Annual Conference and Trade Show MPRO: Our Work QUALITY IMPROVEMENT REVIEW
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Coordinated Care: Key to Successful Outcomes
 Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
Welcome and Orientation Webinar
 Welcome and Orientation Webinar Care Transitions Network for People with Serious Mental Illness National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of
Welcome and Orientation Webinar Care Transitions Network for People with Serious Mental Illness National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available