Transitional Care and Preventing Readmissions in San Francisco
|
|
|
- Darren Booth
- 6 years ago
- Views:
Transcription
1 Transitional Care and Preventing Readmissions in San Francisco 24th Annual Medical Surgical Conference April 10, 2014 South San Francisco Conference Center
2 San Francisco Transitional Care Program Carrie Wong, MSW, MPH, LCSW Director of Long Term Care Operations San Francisco Department of Aging and Adult Services
3 Abstract Community-based Care Transition Programs have been used to reduce costs by preventing unnecessary hospital readmissions, and improving the quality of care and the overall patient experience. The San Francisco Transitional Care Program is a unique partnership of government, hospitals, and community-based organizations with innovative approach to a seamless delivery of services from within hospital walls to the community, to secure better health outcomes, and to reduce healthcare costs without adverse human costs.
4 Learning Objectives To understand the context for Medicare Innovations, transitional care, and health care delivery To understand how the complexity of socioeconomic factors, health literacy, and support systems affect health outcomes
5 Agenda Why is transitional care important? Background Program Description Challenges Readmission Outcomes Questions?
6 Why is Transitional Care important? Making it personal
7 Background Almost one out of every five Medicare patients (approximately 2.6 million seniors) discharged from a hospital is readmitted within 30 days Total cost is over $26 billion every year Multiple factors along the care continuum that impact readmissions. Centers for Medicare and Medicaid Services created Community-based Care Transitions Program to encourage communities to work together to improve quality, reduce cost, and improve patient experience.
8 The Community-based Care Transitions Program (CCTP) Created by Section 3026 of the Affordable Care Act Launched in 2011 Test models for improving care transitions from the hospital to other settings and reducing readmissions for high-risk Medicare beneficiaries. Also a part of the Partnership for Patients which is a nationwide public-private partnership that aims to reduce preventative errors in hospitals by 40% and reduce hospital readmissions by 20%

9 Goals of the CCTP To improve transitions of beneficiaries from the inpatient hospital setting to other care settings To improve quality of care, to reduce readmissions for high risk beneficiaries To document measurable savings to the Medicare program

10 CCTP Participants 102 participants nationwide California has 11 CCTP Teams Northern California San Francisco Sonoma Marin Southern California Anaheim Glendale Los Angeles Reseda San Diego San Fernando Ventura
11 San Francisco Transitional Care Program A formal partnership that includes the Department of Aging & Adult Services, NCPHS/SF Senior Center and multiple community-based organizations and hospitals to: Help eligible older adults and adults with disabilities to transition safely from hospital to home Reduce unnecessary acute hospital readmissions
12

13 Target Population Older adults (age 60 or older) Adults with disabilities (age 18 to 59) Cognitive impairment Little or no formal or informal supports and/or lives alone Chronic illness and/or more than three medical co-morbidities Two or more readmissions within the last 6 months Difficulty managing medications and/or taking 8 or more routine medications Needs assistance with 2 or more activities of daily living Demonstrated need for service/resource to avoid readmissions

14 Eligibility Criteria Payor source: MediCare fee-for-service and MediCare/MediCal (eventual expansion to uninsured and MediCal only) Seniors age 60 & older or adults with disabilities age A resident of San Francisco In stable housing Referred by hospital during acute medical hospitalization Client, family or friends are able to benefit from coaching or care coordination services Willing to accept services

15 Infrastructure Collaboration of county, 8 hospitals, and 8 community-based organizations to address a citywide issue Specialized committees to guide program aspects -- Governance, Steering, Finance Centralized Intake System at Dept of Aging and Adult Services for information and referrals for SFTCP and other county services such as IHSS, APS, HDM, CLF, and I&R Web-based electronic client database for data management and reporting
16 Main Roles Hospital Liaison with DAAS Intake Assist hospital staff/units with program information and referrals Initiate patient intervention during initial hospital visit Collectively cover all 7 hospital campuses every weekday Transitional Care Specialist Provide transitional care services in the 5 focus areas Complete home visits and appropriate follow up Arrange for service packages (transportation, meals, or homecare) Stabilize and refer to long term resources Complete Patient Activation Survey

17 Program Staff Program Manager Intake Coordinator Clinical Supervisor 11 Transitional Specialists Language Capacity Cantonese Mandarin Toisanese Japanese Russian Spanish Tagalog Vietnamese

18 The Intervention Coaching and care coordination model Transitional care services provided between 4-6 weeks after an acute hospitalization Hospital visit 24 hours prior to discharge Home visit within 3 days after discharge Additional home visits if needed Phone calls Service packages of meals, home care, and transportation Referrals to case management and other services as needed after transitional care services are completed

19 Client Areas of Focus Set a recovery goal Understand one's health issues and role of medications Recognize symptoms and have a plan of action if they occur Develop My Wellness Plan a tool to organize health information Secure/prepare for the first PCP appointment including questions and concerns Establish services/resources with emphasis on nutrition, transportation, care at home
20 Program-to-Date Outcomes 1346 clients referred 1317 clients enrolled initially 1192 clients completed the intervention 89.5% or 1079 clients successfully transitioned home 10.5% or 113 clients were rehospitalized *Preliminary data between December 2012 November 2013
21 Types of Services Provided 38% Coaching only 13% Care coordination only 48% Both coaching and care coordination *Preliminary data from April 2013 to November 2013
22 5 Focus Areas at Case Completion 100% of clients used My Wellness Plan 87% of clients were able to manage medication 90% of clients went to their first doctor appointment 76% of clients knew their own health red flags 54% of clients needed and accessed additional community based services *Preliminary data from April 2013 to August 2013

23 Readmissions for SFTCP Clients
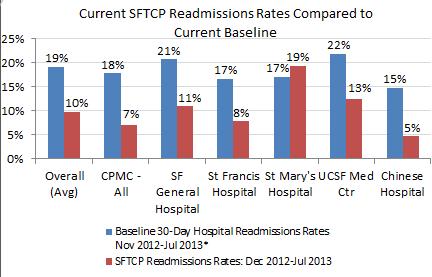
24 Readmissions
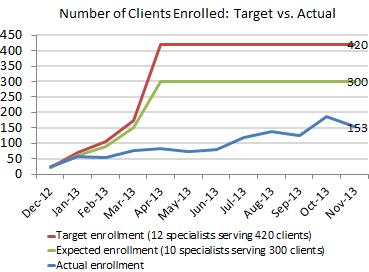
25 Referrals vs Enrollments
26 Ongoing Challenges
27 Contact Carrie Wong, MSW, MPH, LCSW Director of Long Term Care Operations San Francisco Department of Aging and Adult Services
San Francisco Transitional Care Program
 San Francisco Transitional Care Program A presentation for Make History at California Readmissions Summit Avoid Readmissions through Collaboration May 6, 2014 at Oakland Scottish Rite Center Presenters
San Francisco Transitional Care Program A presentation for Make History at California Readmissions Summit Avoid Readmissions through Collaboration May 6, 2014 at Oakland Scottish Rite Center Presenters
Medical Care Meets Long-Term Services and Supports (LTSS)
") Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Medical Care Meets Long-Term Services and Supports (LTSS) Cal MediConnect Providers Summit January 21, 2015 Moderator: Rebecca Malberg von Lowenfeldt, Director LTSS Practice, Harbage Consulting www.chcs.org
Department of Health & Human Services Division of Behavioral Health Services Alcohol & Drug Services. Uma K. Zykofsky, LCSW Behavioral Health Director
 Department of Health & Human Services Division of Behavioral Health Services Alcohol & Drug Services April 24, 2017 Presentation to Geographic Managed Care Providers Uma K. Zykofsky, LCSW Behavioral Health
Department of Health & Human Services Division of Behavioral Health Services Alcohol & Drug Services April 24, 2017 Presentation to Geographic Managed Care Providers Uma K. Zykofsky, LCSW Behavioral Health
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
LONG TERM CARE INTEGRATION
 LONG TERM CARE INTEGRATION Kristen D Smith, MPH Aging Program Administrator Aging & Independence Services County of San Diego Health and Human Services 1/11/2017 1 COUNTY OF SAN DIEGO Building Better Health
LONG TERM CARE INTEGRATION Kristen D Smith, MPH Aging Program Administrator Aging & Independence Services County of San Diego Health and Human Services 1/11/2017 1 COUNTY OF SAN DIEGO Building Better Health
Introduction. Summary of Approved WPC Pilots
 The California Whole Person Care Pilot Program: County Partnerships to Improve the Health of Medi-Cal Beneficiaries Prepared by Lucy Pagel, Tanya Schwartz and Jennifer Ryan with support from The California
The California Whole Person Care Pilot Program: County Partnerships to Improve the Health of Medi-Cal Beneficiaries Prepared by Lucy Pagel, Tanya Schwartz and Jennifer Ryan with support from The California
SOCIAL WORK LEADERSHIP: A CRITICAL COMPONENT TO HEALTHCARE TRANSFORMATION
 A national innovator integrating social services with medical care to improve health, reduce costs, and create a better quality of life for the moderate to high-risk and most vulnerable populations SOCIAL
A national innovator integrating social services with medical care to improve health, reduce costs, and create a better quality of life for the moderate to high-risk and most vulnerable populations SOCIAL
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways
 Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways") Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
Overview and Current Status of Program of All-inclusive Care for the Elderly (PACE) Dr. Cheryl Phillips, M.D. Chief Medical Officer, On Lok Lifeways 1 What is On Lok? Original Vision: Help the low-income
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Kaiser Foundation Hospital Antioch
 Custodian: Compliance Officer Page: 1 of 17 1.0 Policy Statement 1.1. Kaiser Foundation Health Plan, Inc. and Kaiser Foundation Hospitals, The Permanente Medical Group, and the Southern California Permanente
Custodian: Compliance Officer Page: 1 of 17 1.0 Policy Statement 1.1. Kaiser Foundation Health Plan, Inc. and Kaiser Foundation Hospitals, The Permanente Medical Group, and the Southern California Permanente
August 25, Dear Acting Administrator Slavitt:
 August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
1.5. Health Plan provides alternative format materials in accordance with ADA Alternative Formats Policy.
 Page: 1 of 19 1.0 Policy Statement 1.1. Kaiser Foundation Health Plan, Inc. and Kaiser Foundation Hospitals, The Permanente Medical Group, Inc., and the Southern California Permanente Medical Group are
Page: 1 of 19 1.0 Policy Statement 1.1. Kaiser Foundation Health Plan, Inc. and Kaiser Foundation Hospitals, The Permanente Medical Group, Inc., and the Southern California Permanente Medical Group are
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
dual-eligible reform a step toward population health management
 FEATURE STORY REPRINT APRIL 2013 Bill Eggbeer Krista Bowers Dudley Morris healthcare financial management association hfma.org dual-eligible reform a step toward population health management By improving
FEATURE STORY REPRINT APRIL 2013 Bill Eggbeer Krista Bowers Dudley Morris healthcare financial management association hfma.org dual-eligible reform a step toward population health management By improving
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
California County Customer Service Centers Survey of Current Human Service Operations July 2012
 California County Customer Service Centers Survey of Current Human Service Operations July 2012 I. Introduction Early this spring, the County Welfare Directors Association of California (CWDA) worked with
California County Customer Service Centers Survey of Current Human Service Operations July 2012 I. Introduction Early this spring, the County Welfare Directors Association of California (CWDA) worked with
Ensuring safety: IHSS Caregiver Back-up System (BUS)
") P a g e 1 Ensuring safety: IHSS Caregiver Back-up System (BUS) ABSTRACT OF THE PROGRAM The In-Home Supportive Services (IHSS) Caregiver Back-Up System (BUS) is an innovative, 24- hour, in-home emergency
P a g e 1 Ensuring safety: IHSS Caregiver Back-up System (BUS) ABSTRACT OF THE PROGRAM The In-Home Supportive Services (IHSS) Caregiver Back-Up System (BUS) is an innovative, 24- hour, in-home emergency
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE. By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012
 PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
PACE Performance on Post-Discharge Primary Care Evaluations from Jan-Jun 2012 PACE By: Rocio Solano Padilla PCLP-NMF/GE Scholar Jul 23, 2012 2 INTRODUCTION Who am I? Physician Assistant student Towson/CCBC
WHAT IS PACE? A TRAINING GUIDE FOR OUTREACH & REFERRAL ORGANIZATIONS
 PACE is a health plan exclusively for individuals over 55 years of age. Our programs have been operating for over 40 years and are located throughout California. PACE is for individuals who are living
PACE is a health plan exclusively for individuals over 55 years of age. Our programs have been operating for over 40 years and are located throughout California. PACE is for individuals who are living
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Public Policy and Health Care Quality. Readmissions: Taking Progress into the Future
 Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
UNIVERSAL INTAKE FORM
 CLIENT DEMOGRAPHICS Agency Name: Fiscal Year: Funding Identifier: UNIVERSAL INTAKE FORM Title III B C1 C2 Title III D Title III E Title III E(G) 1 Linkages SNAP-Ed Applicant Last Name First Name Middle
CLIENT DEMOGRAPHICS Agency Name: Fiscal Year: Funding Identifier: UNIVERSAL INTAKE FORM Title III B C1 C2 Title III D Title III E Title III E(G) 1 Linkages SNAP-Ed Applicant Last Name First Name Middle
Contra Costa and Sonoma Counties Multipurpose Senior Services Program: Lessons for San Francisco County
 Contra Costa and Sonoma Counties Multipurpose Senior Services Program: Lessons for San Francisco County Hugh V. Wang E X E C U T I V E S U M M A R Y San Francisco s senior population is growing, and the
Contra Costa and Sonoma Counties Multipurpose Senior Services Program: Lessons for San Francisco County Hugh V. Wang E X E C U T I V E S U M M A R Y San Francisco s senior population is growing, and the
Medicare Community-Based Care Transitions Program. Linda M. Magno Director, Medicare Demonstrations
 Medicare Community-Based Care Transitions Program Linda M. Magno Director, Medicare Demonstrations Partnership for Patients n Government-wide partnership with private sector Prevent patients from getting
Medicare Community-Based Care Transitions Program Linda M. Magno Director, Medicare Demonstrations Partnership for Patients n Government-wide partnership with private sector Prevent patients from getting
Managed Long Term Services and Supports (MLTSS)
") Cal MediConnect 2017 Managed Long Term Services and Supports (MLTSS) 2017 CMC Annual Training Topics of Discussion What are MLTSS services? Overview of MLTSS programs MLTSS Referrals Services covered Eligibility
Cal MediConnect 2017 Managed Long Term Services and Supports (MLTSS) 2017 CMC Annual Training Topics of Discussion What are MLTSS services? Overview of MLTSS programs MLTSS Referrals Services covered Eligibility
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
The Community based Care Transitions Program (CCTP)
") The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
San Francisco Pilot Program Behavioral Health Focus
 San Francisco Pilot Program Behavioral Health Focus David Serrano Sewell Hospital Council of Northern & Central California Abbie Yant Dignity Health Convening for Change: Addressing San Francisco s Emergency
San Francisco Pilot Program Behavioral Health Focus David Serrano Sewell Hospital Council of Northern & Central California Abbie Yant Dignity Health Convening for Change: Addressing San Francisco s Emergency
UNIVERSAL INTAKE FORM
 Agency Name: Funding Identifier: Los Angeles County Area Agency on Aging UNIVERSAL INTAKE FORM Title IIIB Title C1 Title C2 Title IIIE Title IIIE(G) Linkages IDENTIFICATION DEMOGRAPHICS 1a Date: Applicant
Agency Name: Funding Identifier: Los Angeles County Area Agency on Aging UNIVERSAL INTAKE FORM Title IIIB Title C1 Title C2 Title IIIE Title IIIE(G) Linkages IDENTIFICATION DEMOGRAPHICS 1a Date: Applicant
Targeting Readmissions:
 Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Targeting Readmissions: A Collaborative Strategy for Hospitals, Health Plans and Local Communities Speaker: Gina Lasky, PhD, Senior Consultant, Warren Lyons, Principal, Suzanne Mitchell, MD, Principal,
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
The Medical Home: Home Care 2.0. Eric. C. Rackow, M.D. President, Humana At Home October 1, 2014
 The Medical Home: Home Care 2.0 Eric. C. Rackow, M.D. President, Humana At Home October 1, 2014 About Humana At Home Organization 3,000 employed telephonic care managers nationwide 14,700 employed and
The Medical Home: Home Care 2.0 Eric. C. Rackow, M.D. President, Humana At Home October 1, 2014 About Humana At Home Organization 3,000 employed telephonic care managers nationwide 14,700 employed and
Caring for the most complex and high-utilizing patients Emerging program models in California primary care clinics
 Caring for the most complex and high-utilizing patients Emerging program models in California primary care clinics Melissa Barajas, RN, BSN, PHN and Loreta Villemez, Neighborhood HealthCare Fern Ebeling,
Caring for the most complex and high-utilizing patients Emerging program models in California primary care clinics Melissa Barajas, RN, BSN, PHN and Loreta Villemez, Neighborhood HealthCare Fern Ebeling,
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015
 Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
Medicare / Accountable Care Organization CHS Finance Division CPE Day November 2, 2015 Steve Neorr Chief Administrative Officer, Triad HealthCare Network Jeff Jones Chief Financial Officer, Cone Health
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
A Health Care Innovation Grant Project: A Collaboration of Contra Costa County EHSD Aging & Adult Services Bureau and the Contra Costa Health Plan
 A Health Care Innovation Grant Project: A Collaboration of Contra Costa County EHSD Aging & Adult Services Bureau and the Contra Costa Health Plan La Valda R. Marshall EXECUTIVE SUMMARY Teamwork is the
A Health Care Innovation Grant Project: A Collaboration of Contra Costa County EHSD Aging & Adult Services Bureau and the Contra Costa Health Plan La Valda R. Marshall EXECUTIVE SUMMARY Teamwork is the
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
with Food, Nutrition, and Dining
 by Brenda Richardson, MA, RDN, LD, CD, FAND 1 HOUR CE CBDM Approved Reducing Hospital Admissions with Food, Nutrition, and Dining NUTRITION CONNECTION FOOD, NUTRITION, AND DINING ARE INTEGRAL COMPONENTS
by Brenda Richardson, MA, RDN, LD, CD, FAND 1 HOUR CE CBDM Approved Reducing Hospital Admissions with Food, Nutrition, and Dining NUTRITION CONNECTION FOOD, NUTRITION, AND DINING ARE INTEGRAL COMPONENTS
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Karen Stasium, BS, MPT, COS C, HCS D
 Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Karen Stasium, BS, MPT, COS C, HCS D Objectives Demonstrate how home health therapists are an integral part of minimizing re hospitalizations and safely transitioning the patient from hospital to home
Recuperative Care Center of Los Angeles
 Recuperative Care Center of Los Angeles Presented by National Health Foundation Elizabeth Yang, MA, Director Jeannine Pugliese, BSW, Coordinator October 26, 2012 Learning Objectives Define the benefits
Recuperative Care Center of Los Angeles Presented by National Health Foundation Elizabeth Yang, MA, Director Jeannine Pugliese, BSW, Coordinator October 26, 2012 Learning Objectives Define the benefits
Evolution of Emergency Medical Services
 CALIFORNIA Evolution of Emergency Medical Services White Paper 1966 Agenda for the FUTURE Institute of Medicine Report 2006 Community Paramedic Community Paramedicine Mobile Integrated Health 2013
CALIFORNIA Evolution of Emergency Medical Services White Paper 1966 Agenda for the FUTURE Institute of Medicine Report 2006 Community Paramedic Community Paramedicine Mobile Integrated Health 2013
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital
 Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
California s Duals Demonstration: A Transparent and Inclusive Stakeholder Process. Peter Harbage President Harbage Consulting
 California s Duals Demonstration: A Transparent and Inclusive Stakeholder Process Peter Harbage President Harbage Consulting 1 Today s Agenda 1. California Context 1. California s Stakeholder Engagement
California s Duals Demonstration: A Transparent and Inclusive Stakeholder Process Peter Harbage President Harbage Consulting 1 Today s Agenda 1. California Context 1. California s Stakeholder Engagement
Evolution of ACOs in California. Accountable Care Congress Los Angeles November 11, 2014 Jill Yegian, Ph.D.
 Evolution of ACOs in California Accountable Care Congress Los Angeles November 11, 2014 Jill Yegian, Ph.D. Integrated Healthcare Association Statewide multi stakeholder leadership group that promotes quality
Evolution of ACOs in California Accountable Care Congress Los Angeles November 11, 2014 Jill Yegian, Ph.D. Integrated Healthcare Association Statewide multi stakeholder leadership group that promotes quality
Engaging Consumers in Care
 Engaging Consumers in Care Cal MediConnect Providers Summit January 21, 2015 Moderator: Carolyn Ingram, Senior Vice President, CHCS www.chcs.org Reaching Medicare-Medicaid Enrollees Medicare-Medicaid enrollees
Engaging Consumers in Care Cal MediConnect Providers Summit January 21, 2015 Moderator: Carolyn Ingram, Senior Vice President, CHCS www.chcs.org Reaching Medicare-Medicaid Enrollees Medicare-Medicaid enrollees
Improving Transitions of Care
 Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
Improving Transitions of Care A Strategy to Defer Decline How the Foundation Got Started with Care Transitions First Quality Improvement Collaborative 2005-2006 Teams chose palliative care or transitions
A Care Coordination Model for Value-Based Performance Programs
 A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
AHA-AMGA Learning Fellowship. Monthly Webinar October 27, :00 3:30pm ET
 AHA-AMGA Learning Fellowship Monthly Webinar October 27, 2016 2:00 3:30pm ET Reminders Action Plan Due Date: Today, October 27 (send to bsutter@amga.org) In-Person Meeting: November 14-15 at the San Francisco
AHA-AMGA Learning Fellowship Monthly Webinar October 27, 2016 2:00 3:30pm ET Reminders Action Plan Due Date: Today, October 27 (send to bsutter@amga.org) In-Person Meeting: November 14-15 at the San Francisco
KEPRO Beneficiary and Family Centered Care Quality Improvement Organization. Andrea Plaskett, MPH
 KEPRO Beneficiary and Family Centered Care Quality Improvement Organization Andrea Plaskett, MPH 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the
KEPRO Beneficiary and Family Centered Care Quality Improvement Organization Andrea Plaskett, MPH 1 KEPRO KEPRO is a federal contractor for the Centers for Medicare & Medicaid Services (CMS) KEPRO is the
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care
 Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Rapid Response Nursing Program: Supporting Chronic Disease Management through Transitions in Care Geriatric Day Hospitals Institute Sunnybrook Health Science Centre November 25, 2013 Liana Sikharulidze,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
S a n F r a n c i s c o C o u n t y
 BAYVIEW HUNTERS POINT S a n F r a n c i s c o As of 3/11/2015 ADULT DAY HEALTH CENTER 1250 LaSalle Avenue San Francisco, CA 94124-2414 (415) 826-4774 Email: Bayviewadhc@aol.com Bayview Hunter's Point Multipurpose
BAYVIEW HUNTERS POINT S a n F r a n c i s c o As of 3/11/2015 ADULT DAY HEALTH CENTER 1250 LaSalle Avenue San Francisco, CA 94124-2414 (415) 826-4774 Email: Bayviewadhc@aol.com Bayview Hunter's Point Multipurpose
Same Disease, Different Care: How Patient Health Coverage Drives Treatment Patterns in California. The analysis includes:
 Same Disease, Different Care: How Patient Health Coverage Drives Treatment Patterns in California C A L I FOR N I A HEALTHCARE FOUNDATION Introduction As shown in The 2005 Dartmouth Atlas of Health Care,
Same Disease, Different Care: How Patient Health Coverage Drives Treatment Patterns in California C A L I FOR N I A HEALTHCARE FOUNDATION Introduction As shown in The 2005 Dartmouth Atlas of Health Care,
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
Navigating the Hospital Readmission Reduction Program At a U.S. Senate hearing in March 2013, a top Medicare official testified that while readmission rates had remained steady for the past five years
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Highline Health Connections: Care Navigation for Vulnerable Populations
 Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM
 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM KIMBERLY K. DELP, RN BSN January 26, 2017 AN OPPORTUNITY TO INTEGRATE NUTRITION SERVICES IN YOUR LOCAL HEALTHCARE SYSTEM 1
Solving the Medicare Spending Per Beneficiary Measure (MSPB) Puzzle
 Puzzle") Solving the Medicare Spending Per Beneficiary Measure (MSPB) Puzzle Chuck Bongiovanni, MSW, MBA, CSA, CFE Objections 1. Identify how MSPB incentivizes or penalizes acute care hospitals 2. Learn what the
Solving the Medicare Spending Per Beneficiary Measure (MSPB) Puzzle Chuck Bongiovanni, MSW, MBA, CSA, CFE Objections 1. Identify how MSPB incentivizes or penalizes acute care hospitals 2. Learn what the
Gaylord National Resort & Convention Center 8/23/2012
 Using Health Policy to Support Nutrition Programs and Link to Health Care August 23, 2012 Mary Jane Koren, M.D., M.P.H. VP LTC Quality Improvement The Commonwealth Fund Two of Five Older Adults Are Not
Using Health Policy to Support Nutrition Programs and Link to Health Care August 23, 2012 Mary Jane Koren, M.D., M.P.H. VP LTC Quality Improvement The Commonwealth Fund Two of Five Older Adults Are Not
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Safe Transitions: From Patient Centered Care to Patient Directed Care
 Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Safe Transitions: From Patient Centered Care to Patient Directed Care Presented by Stefan Gravenstein, MD, MPH Professor of Medicine, Alpert Medical School of Brown University Clinical Director, Healthcentric
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
CMS QUALITY MEASURES, COULD MEAN TO YOU MALNUTRITION, AND WHAT IT. Part I of Nutrition Division Webinar Series
 CMS QUALITY MEASURES, MALNUTRITION, AND WHAT IT COULD MEAN TO YOU Part I of Nutrition Division Webinar Series Welcome! During the webinar, the phone lines will be muted. There will be a 15 minute Q&A session
CMS QUALITY MEASURES, MALNUTRITION, AND WHAT IT COULD MEAN TO YOU Part I of Nutrition Division Webinar Series Welcome! During the webinar, the phone lines will be muted. There will be a 15 minute Q&A session
Special Needs Program Training. Quality Management Department
 10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial interest There is no
 None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial interest There is no commercial support for this CME activity RIVERSIDE COUNTY
None of the faculty, planners, speakers, providers nor CME committee has any relevant financial relationships with commercial interest There is no commercial support for this CME activity RIVERSIDE COUNTY
HEALTH CARE TEAM SACRAMENTO S MENTAL HEALTH CRISIS
 Team Leader/Issue Contact: HEALTH CARE TEAM Laura Niznik Williams, UC Davis Health System, (916) 276-9078, ljniznik@ucdavis.edu SACRAMENTO S MENTAL HEALTH CRISIS Requested Action: Evaluate the Institutions
Team Leader/Issue Contact: HEALTH CARE TEAM Laura Niznik Williams, UC Davis Health System, (916) 276-9078, ljniznik@ucdavis.edu SACRAMENTO S MENTAL HEALTH CRISIS Requested Action: Evaluate the Institutions
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
CMS Proposed Payment Rule FY Cheryl Phillips, MD Evvie Munley
 CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
CMS Proposed Payment Rule FY 2017 Cheryl Phillips, MD Evvie Munley Key Points The link for the full rule: https://www.gpo.gov/fdsys/pkg/fr-2016-04- 25/pdf/2016-09399.pdf Comments due CoB 6/20/16 You do
2015 CMS National Training Program Workshop Monika Vega, MSW Harbage Consulting, LLC Representing California s Department of Health Care Services
 California s Coordinated Care Initiative 2015 CMS National Training Program Workshop Monika Vega, MSW Harbage Consulting, LLC Representing California s Department of Health Care Services Roadmap Nationally
California s Coordinated Care Initiative 2015 CMS National Training Program Workshop Monika Vega, MSW Harbage Consulting, LLC Representing California s Department of Health Care Services Roadmap Nationally
Care1st Provider Model of Care Training
 Care1st Provider Model of Care Training Special Needs Plan (SNP) 2017-2018 SNP Model of Care (MOC) The Medicare Act of 2003 established a Medicare Advantage coordinated care plan that is designed to provide
Care1st Provider Model of Care Training Special Needs Plan (SNP) 2017-2018 SNP Model of Care (MOC) The Medicare Act of 2003 established a Medicare Advantage coordinated care plan that is designed to provide
Medication Error Reporting Program (MERP) Update. April 2010 *********************************************
 Update. April 2010 *********************************************") Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Improving healthcare for people with special or supportive-care needs
 Kara Carter, Razili Lewis, and Tim Ward Improving healthcare for people with special or supportive-care needs Healthcare Systems & Services September 2016 Certain individuals have especially complex medical
Kara Carter, Razili Lewis, and Tim Ward Improving healthcare for people with special or supportive-care needs Healthcare Systems & Services September 2016 Certain individuals have especially complex medical
FACT SHEET Low Income Assistance: Cal MediConnect (E-004) p. 1 of 6
 p. 1 of 6") FACT SHEET Low Income Assistance: Cal MediConnect (E-004) p. 1 of 6 Low Income Assistance: Cal MediConnect What is Cal MediConnect? California is one of 12 states that has signed a Memorandum of Understanding
FACT SHEET Low Income Assistance: Cal MediConnect (E-004) p. 1 of 6 Low Income Assistance: Cal MediConnect What is Cal MediConnect? California is one of 12 states that has signed a Memorandum of Understanding
Medical Respite Care:
 Medical Respite Care: Reducing Readmissions, LOS, and ED Visits of People Experiencing Homelessness Paula Crombie, LCSW, Director of Social Work Michael Ferry, LCSW, Senior Clinical Social Worker Alison
Medical Respite Care: Reducing Readmissions, LOS, and ED Visits of People Experiencing Homelessness Paula Crombie, LCSW, Director of Social Work Michael Ferry, LCSW, Senior Clinical Social Worker Alison
OneCare Model of Care
 OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
High-tech, high- cost care has shifted to low-tech care at a lower cost unregulated care, less overhead Times Union, January 7, 2014
 High-tech, high- cost care has shifted to low-tech care at a lower cost unregulated care, less overhead Times Union, January 7, 2014 Times Union, Oversight sought for walk-in centers, January 7, 2014 An
High-tech, high- cost care has shifted to low-tech care at a lower cost unregulated care, less overhead Times Union, January 7, 2014 Times Union, Oversight sought for walk-in centers, January 7, 2014 An
California s Pediatric Palliative Care. Jill Abramson, MD, MPH November 1, 2012
 California s Pediatric Palliative Care Jill Abramson, MD, MPH November 1, 2012 Outline How a program can change a life Pediatric Palliative Care PFC Overview PFC Results Challenges PFC in the future Case
California s Pediatric Palliative Care Jill Abramson, MD, MPH November 1, 2012 Outline How a program can change a life Pediatric Palliative Care PFC Overview PFC Results Challenges PFC in the future Case
RE-ADMITTING IN HOSPITALS: MODELS AND CHALLENGES. Murali Parthasarathy Dr. Paul Damien
 RE-ADMITTING IN HOSPITALS: MODELS AND CHALLENGES Murali Parthasarathy Dr. Paul Damien April 11, 2014 1 Major pain points Hospitals scored on five major pain points 1. Death rates among heart and surgery
RE-ADMITTING IN HOSPITALS: MODELS AND CHALLENGES Murali Parthasarathy Dr. Paul Damien April 11, 2014 1 Major pain points Hospitals scored on five major pain points 1. Death rates among heart and surgery
HPSM Medi-Cal Benefits A Guide on How to Get Your Health Care
 HPSM Medi-Cal Benefits A Guide on How to Get Your Health Care Health care and insurance benefits can be difficult to understand. This guide introduces you to your basic Medi-Cal benefits, to the Health
HPSM Medi-Cal Benefits A Guide on How to Get Your Health Care Health care and insurance benefits can be difficult to understand. This guide introduces you to your basic Medi-Cal benefits, to the Health