Complex Care Coordination A new line of business
|
|
|
- Cameron Garrison
- 6 years ago
- Views:
Transcription


1 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex, effective, and potentially dangerous." Sir Cyril Chantler. BMJ 1998; 317:1666 1


2 Objectives Describe the need for improved care coordination to high risk/high cost individuals. Design a complex care coordination program that will have a positive impact on the quality of individual s lives and lower overall cost of medical care to a group of high cost individuals in particular Medicare and Medicaid members. Evaluate the impact of care coordination with health indices and cost of care measures. Healthcare is a Maze 2
3 Ho okele Overview Founded in 2006 enabling families to navigate the complicated health and elder care systems Professional staff RNs, MSWs, Health Coaches, In Home Aides Customers Individuals, Employers, Health Plans ihealthhome technology developed to enable cost effective care coordination at home TheAgingTsunami and The Aging Tsunami and Chronic Disease 3



4 Aging Tidal Wave 25 ng Alone ns) Seniors Livin (Million million seniors live alone, this number will double by 2030 Over ½ of all humans that have ever lived to be 65 or older are alive today! The Boomers are Here Every 8.5 seconds a baby boomer in the U.S. turns 50 years old 4
 Disproportionate drivers of healthcare costs.")
5 Chronic Disease Eight of ten Americans age 65 or older are living i with heart tdisease, diabetes or some other form of chronic disease. U.S. Center for Disease Control and Prevention (CDC) Disproportionate drivers of healthcare costs. These individual s in general experience poor health outcomes due to the fragmented healthcare delivery system. What to Do? 5
6 Care Coordination 11/5/ What is Care Coordination An approach to healthcare in which all of a patient s t needs are coordinated d with the assistance of a knowledgeable, single point of contact Medical Home & Community Based Services Functional Assistance Social Participation Personal Goals 6
7 Transitions 42% were able to state their diagnosis 40 80% of medication information is immediately forgotten Almost half of the information was remembered incorrectly Inner city NY hospital Makaryus. Mayo Clinic Proceedings Aug 2005;80:991 Challenges Fragmentation Medication compliance Missed MD appointments Life challenges Lack coordinationmultiple providers Leads to: ED visits Readmission Readmissions Study involved 11,855,702 beneficiaries 19.6% readmission rate within 30 days Significant number with no follow up with primary care physician at the time of rehospitalization $17.4 billion spent on readmissions Public reporting, shared incentives, shared accountability NEJM Medicare patients 7
8 Care Coordination Models Care Transitions Interventions (CTI) Coleman model 4 week intervention Transitional Care Model (TCM) Naylor 1 to 3 month intervention Guided Care John s Hopkins Longterm contact usually for life Geriatric Resources for Assessment and Care of Elders (GRACE) Longterm contact up to 2 years Complex Care Coordination One model 11/5/

9 Complex Care Coordination Model Intensive RN Care Coordination Health Coaching Client Technology Client Who would benefit Multiple chronic Within the top 1% to 5% conditions of highest cost members of a health plan Frequent hospital admission, re admissions Numerous ER visits Complex family and psychosocial environment High risk per health plan predictive modeling Challenging & time intensive for PCP s and office staff May be approaching end of life 9
10 Complex Care Coordination Attend to the highest risk and/or highest cost patients t within a physician s i panel: Population of Focus #1 72 members (3.4%) used 61% of cost ($3.4 M) Population of Focus #2 449 members (5.0%) used 63.5% of cost ($45.6M) Intensive RN Care Coordination RN Care Coordination Partnership with Primary Pi Care Physician i RN as central point of contact Initial intensive face to face interventions Pharmacist medication reconciliation NCQA care coordination standards 10
11 Tools Checklists assist with training and education and promotes consistency of practice. Discharge Checklist Example Questions I have been involved in decisions about what will take place after I leave the facility. I understand what my medications are, how to obtain them and how to take them. I understand what symptoms I need to watch our for and whom to call should I notice them. Tool developed by Dr. Eric Coleman, UCHRC, HCPR 11
12 Tools Sign and Symptoms Great tool to train individuals on signs and symptoms and what to do if noted CALL 911 GO TO EMERGENCY! Health Coaching Health Coaching Patient Activation Motivational Interviewing Self Management Teaching Non Clinical Model 12

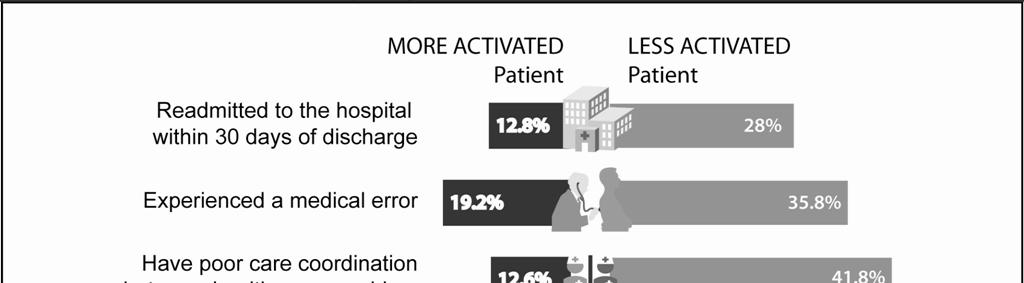
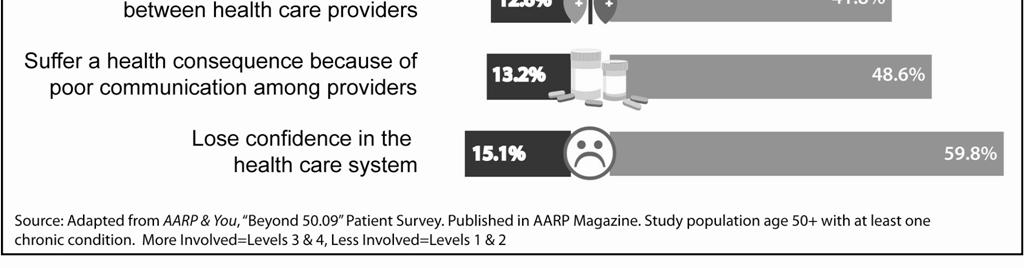
13 Patient Activation National Outcomes 13





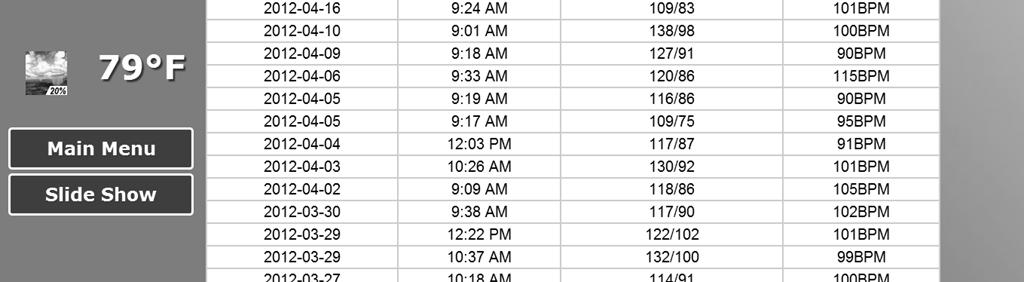
14 Personalized Education Personal Specific to Goals Relevant Digestible Easy to Access Easy to Review Virtual Delivery Technology Technology ihealthhome 14



15 Complex Care Coordination National Outcomes Veterans Administration 25% reduction in bed days 19% reduction in hospital admissions Geisinger Proven Health Navigator Program 18% reduction in hospital admissions 36% reduction in re admissions 7% reduction in overall cost TriHealth Cincinnati 23% reduction in readmissions Massachusetts General Hospital 15% reduction in ER Visits and Hospital Stays In Home Remote Monitoring 15


16 Interactive Self Management Engagement Video Education On line Assessment Skype Visits 16
17 A Story Mrs. B 11/5/ Mrs. B 68 years old female lives with her 70 y/o husband in public housing. English is their second language. She is dependent on her husband for her care 17
18 Goals Personal Goal To travel to her home country to see her 14 grandchildren. Clinical Goals Blood glucose range mg/dl HgA1c < 7% Weight range lbs BP range /70 78 Minimize readmissions due to respiratory infections Increase self management and compliance Outcomes Personal goal Mrs. B visited her children and grandchildren in 2012 Improved Health and Cost Blood Glucose Goal Met 50% improvement HbA1c Goal Met decreased 8% Weight Goal Met lost 12 lbs Li id G lm 6% i i l h l l Lipids Goal Met 6% improvement in total cholesterol Reduced hospitalizations by 20% No Admissions in Last 10 months Technology in Place = Automated hovering 18
19 A New Line of Business Home Health Care Agencies 11/5/ Business Opportunity Home health agencies are in a unique position to include complex care coordination as a new service line. Home care nurses roles can be expanded to coordinate care and resources for individuals with complex chronic disease as a value added service line 19
20 A Need AHRQ White Paper January 2012: private physicians Smaller practices have little reserve capacity or flexibility to devote extra time to the complex patient. Lack of time and emotional energy to spend on anything other than the acute needs of the complex. Private Physicians Time required to navigate the variety of community based, social and behavioral programs is overwhelms the lean practice staff Lack of time to maintain breadth of knowledge in multiple narrow topics for care of complex patients. Low prevalence of complex cases in a panel 20
21 Complex Care Coordination Goals Clinical Reduce ER Visits, hospitalization, re admissions Improve chronic condition health measures Technology Increase care coordinator efficiency Engage patients self management Payment Alignment Cost savings Increased automation scale Care team Common Attributes Comprehensive assessments. Individualized Plans of Care Enable access Community resources Monitoring and communication 21
22 How to Begin Design as a part of the current home health care position or a separate service line Training NCQA or other evidence based standards Design workflows Complex Care Coordinator Role Fosters partnerships with the individual s physician and healthcare team to promote continuity i of services. Responsibilities Coordinate care for medically Comprehensive assessment complex individuals in their Understand the individual s homes and community. culture, family and community relationships. Develop customized and comprehensive service plan. Provide individualized patient education. Evidence based tools Accompany clients to medical appointments care. Referral to community resources 22
23 A Story Mr. H 11/5/ Mr. H 76 year old male Malignant hypertension, Diabetes, Prostate CA Hypertension not responsive to medication therapies Baseline blood pressure of 210/ /94 2 ER Visits pre intervention and one hospitalization day of enrollment Client was seeking clinical trials on mainland on own CONFIDENTIAL 23
24 Goals Personal Go to Las Vegas and visit grandchildren in California Clinical Medication compliance BP 140/80 130/70/ Decrease ED visits No Hospitalizations due to BP complications Outcomes Personal goal Mr. H is planning a trip to Las Vegas and California this fall. Improved Health and Cost BP range 142/86 132/78 No Admissions or ED visits in Last 12 months Technology in Place = Automated hovering 24
25 Measurement Quality Improvement 11/5/ Measures Biometric improvement Hba1C Blood Pressure Lipids, Others as relevant Patient Activation Score Predictive Modeling Score Medication Reconciliation Medication Adherence % refills Pre vs. Post Intervention Cost of Care Hospitalization rate ER Visits Physician and Patient Satisfaction 25
26 HbA1c 36% Better HbA1C Baseline Post Sustained Mean Baseline 7.80 Post 5.04 Sustained % Pct Improvement 6.63 t value 0.00 p value Total Cholesterol 19% Better Total Cholesterol Total Cholesterol 0.00 Baseline Post Sustained Baseline Post Sustained Mean Baseline Post Sustained % Pct Improvement 4.28 t value 0.00 p value 26
27 LDL 10% Better LDL Level Baseline Post Sustained Mean Baseline Post Sustained % Pct Improvement 2.93 t value 0.00 p value HDL 13% Better HDL Level Baseline Post Sustained Mean Baseline Post Sustained % Pct Improvement 3.42 t value 0.00 p value 27
28 Triglycerides 37% Better Triglycerides Baseline Post Sustained Mean Baseline Post Sustained % Pct Improvement 6.75 t value 0.00 p value IP Admits 42% Reduction 28
29 ER Visits 20% Reduction PAM Outcomes 1.6 PAM Level Change: Baseline to Remeasure East West Total (Calculated) PAM Level Remeasure #1 vs. Mean StDev Baseline East West Total
30 Cost 42 of 72 enrollees had HMSA as a payer 19 of the 42 had HMSA as their primary 32% reduction in PMPM was observed in the HMSA members enrolled in the program. Sample size is statically small MD Satisfaction Survey 91% Percent of Responses rated the following as Strongly Agreeor Agree: The RN Navigator helped my patient to better understand and improve managing their health care Th RN N i t hl d d ffi tfft The RN Navigator helped me and my office staff to manage the details for my patient and address problems in a timely and professional manner 30
31 MD Comments Patients who were calling or coming in to the office frequently were able to reduce their visits it to every 3 4 months. Excellent service by skilled and compassionate professionals which improve care and cost. Following patients doings, help with their understanding of their medical problems Patient Satisfaction Survey % Responded as Strongly Agree or Agree: 96% My RN Navigator helped me to better understand my medical condition and what I needed to do to take care of myself 97% My RN Navigator listened to me to learn what I wanted and what problems I had before developing a plan to help me 89% I have a better idea of how to talk to my doctor and what to ask 31
32 Patient Comments "You took me to the hospital when I had no one else "I still want you folks to come and visit me, it helps me to know that you guys care about me" "I want more contact, I enjoyed the machine" "The equipment gave me confidence" "Why did they take the computer from me now I feel lost, I really got spoiled by you two" "Keep the program I like it" "I like to see my blood sugar now I no can" Patient Comments It seems that healthcare is a pile of jigsaw pieces My care navigator helped to show me how the pieces fit into a map of health. It helped to prioritize these, that allows my family and I to make better choices for me. CONFIDENTIAL 32

33 Summary The time is now The prevalence of chronic diseases and aging population. lti Hospital and MD incentives to improve transitions of care and care coordination across the continuum. Unique position and trained labor force 33
34 Thank you Questions? Bonnie Castonguay, RN Co Founder/CEO Ho okele Health Navigators 34
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Implementing Health Coaching
 Implementing Health Coaching Presented by: Amireh Ghorob, MPH Adriana Najmabadi Camille Prado UCSF Center for Excellence in Primary Care IHI Summit 2014, Washington DC March 10, 2014 Session: L9 These
Implementing Health Coaching Presented by: Amireh Ghorob, MPH Adriana Najmabadi Camille Prado UCSF Center for Excellence in Primary Care IHI Summit 2014, Washington DC March 10, 2014 Session: L9 These
Transitions of Care Project BOOST
 Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Transitions of Care Project BOOST Donald Pocock, MD, FACP, CPE Chief Medical Officer Morton Plant Mease Healthcare Jerry Corsello, MBA Unit Business Manager Med-Surg/Oncology Unit "Medicine used to be
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using the Patient Activation Measure (PAM) to Promote Patient Engagement
 to Promote Patient Engagement") Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Quality: Finish Strong in Get Ready for October 28, 2016
 Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
September, James Misak, M.D. Linda Stokes, MSPH The MetroHealth System
 Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
HEALTHY EMPLOYEES HEALTHY EMPLOYEE BENEFIT PLAN
 HEALTHY EMPLOYEES HEALTHY EMPLOYEE BENEFIT PLAN At a point in time when many employers are forced to cut benefits healthcare costs are increasing at 3 to 4 times the rate of inflation access to quality
HEALTHY EMPLOYEES HEALTHY EMPLOYEE BENEFIT PLAN At a point in time when many employers are forced to cut benefits healthcare costs are increasing at 3 to 4 times the rate of inflation access to quality
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Decreasing Medical. Costs. Are your members listening to you? PRESENTED BY: September 22, 2016
 Decreasing Medical Costs Are your members listening to you? PRESENTED BY: Aaron Crowell, Executive Vice President, MTM, Inc. Gary Jacobs, Executive Vice President, CareCentrix Dan Masciopinto, SVP of Product,
Decreasing Medical Costs Are your members listening to you? PRESENTED BY: Aaron Crowell, Executive Vice President, MTM, Inc. Gary Jacobs, Executive Vice President, CareCentrix Dan Masciopinto, SVP of Product,
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Click to edit Master title style
 Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
Preventing, Detecting and Managing Chronic Disease for Medicare Kenneth E. Thorpe, Ph.D. Robert W. Woodruff Professor and Chair of the Department of Health Policy & Management, Rollins School of Public
Learning Objectives. Federal Regulations. Upcoming Concerns. Discharge Planning & Follow up with Residents, Family, Team and Community Providers
 Discharge Planning & Follow up with Residents, Family, Team and Community Providers Elise Beaulieu, MSW, LICSW April 17, 2013 Learning Objectives O Understand the overall concepts of discharge planning
Discharge Planning & Follow up with Residents, Family, Team and Community Providers Elise Beaulieu, MSW, LICSW April 17, 2013 Learning Objectives O Understand the overall concepts of discharge planning
Quality Management Report 2018 Q1
 Quality Management Report 2018 Q1 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels These activities include: Centers for Medicare & Medicaid Services (CMS) Department
Quality Management Report 2018 Q1 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels These activities include: Centers for Medicare & Medicaid Services (CMS) Department
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
FAQ S. Frequently Asked Questions: WellCare Clinic Logistics
 Frequently Asked Questions: FAQ S WellCare Clinic Logistics 1. What is the City of Lawrence WellCare Clinic? The City of Lawrence WellCare Clinic is a part of the CHAMP Wellness Program. The WellCare Clinic
Frequently Asked Questions: FAQ S WellCare Clinic Logistics 1. What is the City of Lawrence WellCare Clinic? The City of Lawrence WellCare Clinic is a part of the CHAMP Wellness Program. The WellCare Clinic
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
A Care Coordination Model for Value-Based Performance Programs
 A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient. February 8, 2018
 A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
A Bridge Back Home: Care Transition Coaching for the Post-Acute Heart Failure Patient February 8, 2018 3 Partners in Care (Partners) A Mission-Driven Organization Our Mission Partners shapes the evolving
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Peripheral Arterial Disease: Application of the Chronic Care Model. Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario
 Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
Passport Advantage Provider Manual Section 8.0 Quality Improvement
 Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Behavioral Health Providers: The Key Element of Value Based Payment Success
 Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
A M.A.P. for improving blood pressure: Application within the QIN-QIO community
 A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
The New Wave of Health Care: Telehealth. FHCC 2014 Annual National Conference April 22-23, 2014
 The New Wave of Health Care: Telehealth FHCC 2014 Annual National Conference April 22-23, 2014 The New Wave of Health Care: Telehealth Plenary Session III Moderator: Ken Peach, Executive Director - Health
The New Wave of Health Care: Telehealth FHCC 2014 Annual National Conference April 22-23, 2014 The New Wave of Health Care: Telehealth Plenary Session III Moderator: Ken Peach, Executive Director - Health
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH
 What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
What will the PCMH Look Like in 2014? Joseph E. Scherger, MD, MPH What Is a Patient-Centered Medical Home? A Patient-Centered Medical Home (PCMH) is a model for care provided by physician practices that
Quality Management Report 2017 Q4
 Quality Management Report 2017 Q4 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels. These activities include: CMS DHS DHS & CMS HEDIS Member Satisfaction (CAHPS
Quality Management Report 2017 Q4 Care Wisconsin Participates in Many Quality Initiatives Across the State and Federal Levels. These activities include: CMS DHS DHS & CMS HEDIS Member Satisfaction (CAHPS
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Cathy Schoen. The Commonwealth Fund Grantmakers In Health Webinar October 3, 2012
 Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Innovating Care for Chronically Ill Patients Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org Grantmakers In Health Webinar October 3, 2012 Chronically Ill:
Test bank PowerPoint slides for each chapter Instructor guides for each chapter (with answers for discussion questions and case studies)
") This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
This is a sample of the instructor materials for Dimensions of Long-Term Care Management: An Introduction, second edition, edited by Mary Helen McSweeney-Feld, Carol Molinari, and Reid Oetjen. The complete
Managing Patients with Multiple Chronic Conditions
 Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Catholic Medical Partners
 Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1)
") Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Lessons for Community Pharmacy from the USC / AltaMed CMMI Healthcare Innovation Award (Round 1) Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Professor and Chair Titus Family Department of Clinical
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Best Practices. SNP Alliance. October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees
 SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
HEALTHCARE INFORMATION SYSTEMS: ENABLERS FOR QUALITY IMPROVEMENT. Kenneth W. Kizer, M.D., M.P.H. President and CEO National Quality Forum
 HEALTHCARE INFORMATION SYSTEMS: ENABLERS FOR QUALITY IMPROVEMENT Kenneth W. Kizer, M.D., M.P.H. President and CEO National Quality Forum January 14, 2002 The Paradox of American Healthcare 2003 Highly
HEALTHCARE INFORMATION SYSTEMS: ENABLERS FOR QUALITY IMPROVEMENT Kenneth W. Kizer, M.D., M.P.H. President and CEO National Quality Forum January 14, 2002 The Paradox of American Healthcare 2003 Highly
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Approaches to Extending Complex Care Models into the Community: Emerging Evidence
 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Medication Therapy Management
 Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Care Continuum or Unconnected Silos
 Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Care Continuum or Unconnected Silos Julie Bynum, MD, MPH Dartmouth Medical School December 10, 2009 Goals for Today Review what we have heard & introduce what we have not heard Understand the components
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
WEBINAR: Check. Change. Control. Cholesterol April 4, 2018
 WEBINAR: Check. Change. Control. Cholesterol April 4, 2018 Good afternoon, everyone. My name is Alberta I am from the New England QIN-QIO and I will be your moderator for today s webinar, Check. Change.
WEBINAR: Check. Change. Control. Cholesterol April 4, 2018 Good afternoon, everyone. My name is Alberta I am from the New England QIN-QIO and I will be your moderator for today s webinar, Check. Change.
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Rethinking the model of primary care. Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine
 Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Healthcare Clinic at Walgreens Access to Care Innovations Panel March 5, 2014
 Healthcare Clinic at Walgreens Access to Care Innovations Panel March 5, 2014 Dr. Alan London Vice President, Strategic Clinical Partnerships 2014 Walgreen Co. All rights reserved. Walgreens is Well-Positioned
Healthcare Clinic at Walgreens Access to Care Innovations Panel March 5, 2014 Dr. Alan London Vice President, Strategic Clinical Partnerships 2014 Walgreen Co. All rights reserved. Walgreens is Well-Positioned
Use Case Study: Remote Patient Monitoring for Chronic Disease
 Use Case Study: Remote Patient Monitoring for Chronic Disease Hackensack Alliance Accountable Care Organization New Jersey March 2014 The Hackensack Alliance Accountable Care Organization (ACO) was established
Use Case Study: Remote Patient Monitoring for Chronic Disease Hackensack Alliance Accountable Care Organization New Jersey March 2014 The Hackensack Alliance Accountable Care Organization (ACO) was established
=======================================================================
 ======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Ambulatory Care Practice Trends and Opportunities in Pharmacy
 Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Employee Benefits Planning Assn. Meredith Mathews, MD MPH
 Employee Benefits Planning Assn. Meredith Mathews, MD MPH 1 Meredith Mathews, MD, MPH Chief Medical Officer 18 years in practice of nephrology; CMO & SVP for Health Services, Premera Blue Cross; CMO &
Employee Benefits Planning Assn. Meredith Mathews, MD MPH 1 Meredith Mathews, MD, MPH Chief Medical Officer 18 years in practice of nephrology; CMO & SVP for Health Services, Premera Blue Cross; CMO &
Introduction to the Provider Care Management Solutions Web Interface
 Introduction to the Provider Care Management Solutions Web Interface Release 0.2 Introduction to the Provider Care Management Solutions Web Interface Purpose Provider Care Management Solutions (PCMS) is
Introduction to the Provider Care Management Solutions Web Interface Release 0.2 Introduction to the Provider Care Management Solutions Web Interface Purpose Provider Care Management Solutions (PCMS) is
CONNECTED SM. Blue Care Connection SIMPLY AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT
 SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015
 MODEL OF CARE TRAINING 2015") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses