Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations
|
|
|
- Andra Ryan
- 5 years ago
- Views:
Transcription

1 Meet DEAN & EDNA: The Application of HHQI Resources in the Reduction of Avoidable Hospitalizations Cindy Sun, MSN, RN Objectives At the conclusion of this session, the participant will be able to: Access and locate HHQI tools and resources Design evidence based change strategies to improve hospitalization and oral medication rates Interpret their agency s HHQI Data Reports and focus quality improvement in identified areas of need Home Health Quality Improvement Goal: Improve the quality of care home health patients receive Special Project funded by Centers for Medicare & Medicaid Services Evidence based practice Free tools, resources, & networking 3 1

2 History 101 Phase 1: Focused on reducing ACH Phase 2: Focus on reducing ACH & Improving Oral Medication Rates Home health setting Home health focus but shifting towards cross setting care Focus on agency leadership More than 5,500 home health agencies enrolled to participate Patient Centered, Interdisciplinary More than 8,000 participant representing 4,000+ home health agencies 4 Phase 3: Sept July 2014 Focusing on quality of home health care measured by : ACH reduction Improvement in oral medication management Improvement of immunization rates Continuing HH focus, but all care settings and patients encouraged to participate Introducing Underserved Population Network (UP) More than 10,000 participants 5 Patient-Centered Care 6 2

3 Evidence-Based Practice Evidence based clinical decision making External evidence from research, theories, opinion leaders, expert panels Clinical expertise Patient preferences and values Melnyk and Fineout Overholt, 2011, p. 4 Current State of Home Health >3 million recipients of Medicare paid home health services in the Unites States each year, including: Medical, nursing, social, or therapeutic treatment Assistance with the essential activities of daily living Volume increasing over time Patients prefer to stay home when possible, but >25% of home health episodes end in rehospitalization Readmissions Almost one fifth of the Medicare beneficiaries who had been discharged from an acute care facility were rehospitalized within 30 days, and 34.0% were rehospitalized within 90 days (Jencks, Williams, and Coleman, 2009) Nearly 90% of readmissions are unplanned and potentially preventable, which translates into $17 billion or nearly 20% of Medicare s hospital payments (Hernandez et al., 2010) 3
 Phone monitoring and/or telehealth Patient self management programs www.homehealthquality.")
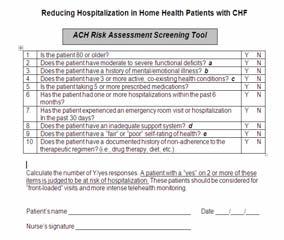
4 ACH Essential Interventions ACH risk assessment Emergency Care Planning Front loading based on risk assessment Easy access to a nurse (24/7 call, office nurse) Phone monitoring and/or telehealth Patient self management programs 11 BPIP 12 4

5 BPIP Sub menus Corss Settings BPIP Release Date Focused BPIP Primary BPIP LAN Creation November 1, 2012 Patient Self Management BPIP Schedule February 1, 2013 Underserved Populations (UP) X X April 2, 2013 June 3, 2013 August 1, 2013 November 1, 2013 February 3, 2014 Medication Management Disease Management: Part 1 Immunization / Infection Control MH: Aspirin Therapy and Blood Pressure Control MH: Cholesterol Control and Smoking Cessation X X X X X April 1, 2014 Disease Management: Part 2 X 5


6 HHQI Data Reports 16 Screen cap of Data Access Site 17 Network & Span tabs 6

7 UP BPIP Let s Meet EDNA & DEAN EDNA 7
8 Clinician s findings Medications Diabetes management Family dynamics are poor Transportation Vision impairments Health Literacy EDNA (cont.) DEAN 8

9 DEAN (cont) Primary caregiver of his wife Independent prior to recent fall (6 wks ago) Weak due to disease process and increased time in bed over past few weeks Feelings of helplessness with new medical conditions as well as no back up for caring for his wife Sound Familiar? How Can HHQI Help EDNA? HHQI Quarterly Best Practice Intervention Packages (BPIP) Free educational material for both leadership & clinical staff Theory, tools, resources & application for day to day implementation Turn key tools to quickly implement 9




10 HHQI BPIPs Help EDNA Pt. Self Management My Action Plan would allow EDNA to pick a goal that is meaningful to her Are You at Risk for Going to Hospital? tool allows her to explore & learn that she is at risk Pt/Clinician Interaction Level Tips & Motivational Interviewing tool will assist the clinicians to work more effectively with EDNA My Action Plan Patient Risk Assessment 10

 Network Tools to determine &")

")

11 Underserved Population (UP) Assistance Network Health Disparities Dual Eligible Small HHA Under served Areas HHQI BPIPs Help EDNA Underserved Population (UP) Network Tools to determine & create a plan for her health literacy issues Evaluate our current patient tools for literacy using guidelines in BPIP Evaluation tools for clinicians to know that she knows (information) Leadership insight to identify, track and improve population diversity & lower outcomes like all the EDNA s in the agency Teach Back 11


 Medication Management Tools & resources to improve EDNA s med management including reconciliation, education strategies Strategies to assist her to safely & consistently adhere")
12 Teach-Back Edna, I am glad you picked your sugar pill to talk about today. Let s talk about how to take the pill as the doctor wants you to, so you will feel better and can get to go to church.. Edna, do you have questions?. I would like you to tell me how you are going to take your medications just like your were the teacher. I take 2 of the sugar pills every morning. Great Edna that s right 2 sugar pills every morning. Can you show me how you are going fill the pill boxes? Sure! Every Sunday I am going to refill this box with my pills. I will use this paper you wrote for me in big lettering. I put 2 of the blue sugar pills in every morning slots just like this HHQI BPIPs Help EDNA (cont.) Medication Management Tools & resources to improve EDNA s med management including reconciliation, education strategies Strategies to assist her to safely & consistently adhere to correct medication schedule Collaborative network needs set up for EDNA with physicians & her pharmacist with awareness of financial difficulties and health literacy issues Medication Adherence 12
 Disease Management Clinician tools to address Diabetes that are 5 th 6 th")



13 HHQI BPIPs Help EDNA (cont.) Disease Management Clinician tools to address Diabetes that are 5 th 6 th grade level Resources to write blood glucose monitor instructions that EDNA can follow every time Clinician s can use resources to know the evidence based practices with Diabetes & Hypertension to verify EDNA is prescribed Importance of interdisciplinary case/team conference to ensure comprehensive care plan addresses all of her needs Bulletin Boards & Data 38 Data to monitor agency s outcomes & care to patients including EDNA Possibly underserved data Evaluate trending & clinical educational needs HHQI Data Help EDNA 13


 to implement")
14 ACH Underserved Populations Network (UP) UP Assistance Networks Multiple network calls will be established Focus on common barriers & issues for agencies with special populations Individual Assistance Smaller HHAs can receive assistance from HHQI team Assistance to implement tools, resources & strategies to overcome barriers HHQI Assistance Helps EDNA Individual assistance to adapt and implement tools and resources into agency level Ability to discuss unique agency barriers/issues Limited resources (staff or equipment) to implement HHQI at agency level 14

15 Now Back To DEAN How can HHQI help you help DEAN? Screenshot of Data Reports Portal 44 ACH 15

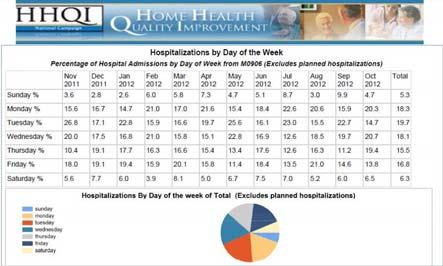
16 ACH National Hospitalization ber week ACH Monthly 16

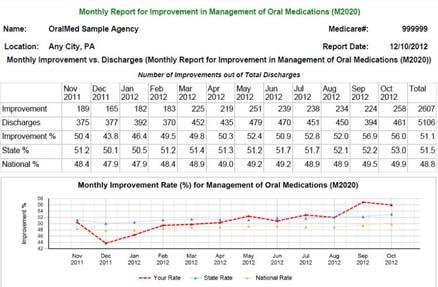
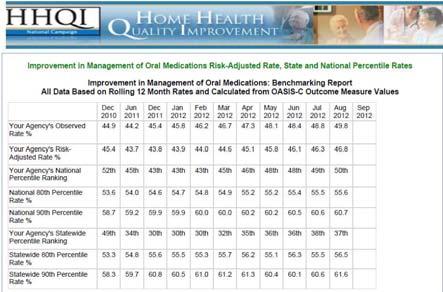
17 Reason(s) for Hospitalization Oral Meds monthly report Oral Meds state and national 17


18 Report for Oral Meds. Educational Resources - HF 18


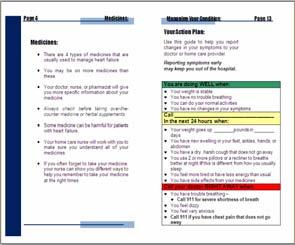
19 Educational Resources - HF Educational Resources - HF Educational Resources - HF 19



20 Educational Resources - HF Educational Resources - HF Educational Resources - HF 20




21 Educational Resources: Warfarin Educational Resources: Warfarin Educational Resources: Warfarin 21



22 Educational Resources: Warfarin Educational Resources: Mobility Educational Resources: Mobility 22


23 Educational Resources: ACH Educational Resources: ACH Patient Hospitalization Risk Form 23

24 Educational Resources: ACH SBAR Physician Communication Tool Specific for High Risk Patients Assistance How Can HHQI Help? Difficulties interpreting your Data Reports? Understand your reports but not sure where to start? Wonder what tools are available to help your patients? What s new? Assistance How Can HHQI Help? 24


25 Assistance How Can HHQI Help? Does your DEAN surf the web? Assistance How Can HHQI Help? Promoting Your Successes through: AOTM Blogs BPIPs e bulletins Assistance How Can HHQI Help? Contact: hhqi@wvmi.org 25

26 Network Live Chats Discussion Forums Learning Action Networks or LANs Network Coordinator Share your success stories QUIZ EDNA DEAN Million Hearts A Aspirin therapy B Blood Pressure measurement C Cholesterol measurement & management S Smoking cessation 26
27 Questions?? 79 Thank You! To reach me: And of course, we can always be reached at References Hernandez, A.F., Greiner, M.A., Fonarow, G.C., Hammill, B.G., Heidenreich, P.A., Yancy, C.W., Peterson, E.D., and Curtis, L.H. (2010). Relationship Between Early Physician Follow up and 30 Day Readmission Among Medicare Beneficiaries Hospitalized for Heart Failure. The Journal of the American Medical Association, 303, Jencks, S.F., Williams, M.V., & Coleman, E.A. (2009). Rehospitalizations among Patients in the Medicare Fee for Service Program. The New England Journal of Medicine, 360, Melnyk, B.M., & Fineout Overholt, E. (2011). Evidence Based Practice in Nursing & Healthcare (2 nd ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. 27
, an agency of the U.S. Department of Health and Human Services. The views presented do not necessarily reflect CMS policy.")
28 Thank You This material was prepared by the West Virginia Medical Institute, the Quality Improvement Organization supporting the Home Health Quality Improvement National Campaign, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The views presented do not necessarily reflect CMS policy. Publication Number: 10SOW WV HH BKH Approved 6/
Authentic Agency Success Stories
 Authentic Agency Success Stories Cindy Sun, MSN, RN, COS C Crystal Welch, MSN, RN Describe how to access Home Health Quality Improvement (HHQI) National Campaign tools and resources Identify three (3)
Authentic Agency Success Stories Cindy Sun, MSN, RN, COS C Crystal Welch, MSN, RN Describe how to access Home Health Quality Improvement (HHQI) National Campaign tools and resources Identify three (3)
Home Health Agencies & Reducing Readmissions. presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights
 Home Health Agencies & Reducing Readmissions presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights Objectives Describe the benefits of collaborating and utilizing
Home Health Agencies & Reducing Readmissions presented by Misty Kevech, RN, MS, COS C, CCP HHQI RN Project Coordinator WVMI & Quality Insights Objectives Describe the benefits of collaborating and utilizing
Leveraging External Improvement Resources for Success in HHVBP
 Home Health Value-Based Purchasing (HHVBP) Leveraging External Improvement Resources for Success in HHVBP March 9, 2017 Prepared for CMS by the HHVBP Technical Assistance, contract number HHSM-500-2014-0033I.
Home Health Value-Based Purchasing (HHVBP) Leveraging External Improvement Resources for Success in HHVBP March 9, 2017 Prepared for CMS by the HHVBP Technical Assistance, contract number HHSM-500-2014-0033I.
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Pave Your Path: How to Improve-Will, Ideas and Execution
 Pave Your Path This presenter has nothing to disclose Pave Your Path: How to Improve-Will, Ideas and Execution Cory Sevin, RN, MSN, NP Director, IHI Kate Bones, MSW Director, IHI February 19, 2013 Organization
Pave Your Path This presenter has nothing to disclose Pave Your Path: How to Improve-Will, Ideas and Execution Cory Sevin, RN, MSN, NP Director, IHI Kate Bones, MSW Director, IHI February 19, 2013 Organization
The Road Map to Success Implementation Checklist STEPS ACHIEVING THE MILESTONES RESOURCES TO SUPPORT YOU MILESTONE 1: JOIN & LEARN NOTES COMPLETION
 STEPS ACHIEVING THE MILESTONES RESOURCES TO SUPPORT YOU MILESTONE 1: JOIN & LEARN DATE COMPLETED BARRIERS TO COMPLETION NOTES 1-1 Identify an agency champion & back up Questions to ask: 1) Who is timely
STEPS ACHIEVING THE MILESTONES RESOURCES TO SUPPORT YOU MILESTONE 1: JOIN & LEARN DATE COMPLETED BARRIERS TO COMPLETION NOTES 1-1 Identify an agency champion & back up Questions to ask: 1) Who is timely
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State ( )
") RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
Home Health Infection Prevention Toolkit
 Home Health Infection Prevention Toolkit Paula Sitzman, RN, BSN Great Plains Quality Innovation Network Judy Riggert, RN, MS Visiting Nurse Association of the Midlands Map Great Plains Quality Innovation
Home Health Infection Prevention Toolkit Paula Sitzman, RN, BSN Great Plains Quality Innovation Network Judy Riggert, RN, MS Visiting Nurse Association of the Midlands Map Great Plains Quality Innovation
Quality Improvement: Utilization Measures
 Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
Home Health Value-Based Purchasing (HHVBP) Quality Improvement: Utilization Measures June 9, 2016 As prepared by the Centers for Medicare & Medicaid Services HHVBP Technical Assistance contract number
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Medication Therapy Management (MTM) Solution
 Solution") Medication Therapy Management (MTM) Solution Service Overview Updated 5.5.16 Congratulations on your decision to partner with Cardinal Health to help ensure that your patients receive beneficial Medication
Medication Therapy Management (MTM) Solution Service Overview Updated 5.5.16 Congratulations on your decision to partner with Cardinal Health to help ensure that your patients receive beneficial Medication
Improving Transitions Across the Continuum of Care
 Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Improving Transitions Across the Continuum of Care Presented By: Cheri A. Lattimer, RN, BSN - Executive Director, NTOCC NTOCC is a 501(c)(4) nonprofit coalition. The Statistics Were Staggering In 2006
Implementing Change to Decrease the Readmission Rate for Clients of a Care Transition Program
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Implementing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Implementing
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS
 TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
TRANSITIONS OF CARE: INCREASING PATIENT ENGAGEMENT AND COMMUNICATION ACROSS HEALTH CARE SETTINGS Leslie Lentz, BA Care Transitions Project Coordinator Health Care Excel, the Indiana Medicare Quality Improvement
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Quarterly Community Meeting. Barb Averyt, BSHA Director, Care Coordination and Nursing Homes Health Services Advisory Group (HSAG) July 14, 2016
 July 14, 2016") Quarterly Community Meeting Barb Averyt, BSHA Director, Care Coordination and Nursing Homes Health Services Advisory Group (HSAG) July 14, 2016 Today s Agenda Welcome and Introduction Community Updates
Quarterly Community Meeting Barb Averyt, BSHA Director, Care Coordination and Nursing Homes Health Services Advisory Group (HSAG) July 14, 2016 Today s Agenda Welcome and Introduction Community Updates
Implementation Guide: Critical Interventions in the First/Second Visit. VNAA Best Practice for Home Health
 Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Implementation Guide: Critical Interventions in the First/Second Visit VNAA Best Practice for Home Health Learning Objectives The participant will be able to: Identify three interventions that should take
Synergy Through Integration:
 WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
MIPS Improvement Activities:
 MIPS Improvement Activities: Quality Insights Tips, Tools & Support March 14, 2017 Maureen Kelsey, MA, Quality Insights, Practice Integration Task Lead MIPS in 2017 A MIPS score is calculated by adding
MIPS Improvement Activities: Quality Insights Tips, Tools & Support March 14, 2017 Maureen Kelsey, MA, Quality Insights, Practice Integration Task Lead MIPS in 2017 A MIPS score is calculated by adding
A New Vision for the Quality Improvement Organization Program
 A New Vision for the Quality Improvement Organization Program This material was prepared by Masspro, the Medicare Quality Improvement Organization for Massachusetts, under contract with the Centers for
A New Vision for the Quality Improvement Organization Program This material was prepared by Masspro, the Medicare Quality Improvement Organization for Massachusetts, under contract with the Centers for
Integrating Technology into Care: Telehealth and Beyond
 Integrating Technology into Care: Telehealth and Beyond Cindy Campbell RN, BSN, MHA (c) Director Operational Consulting Fazzi Associates, Inc. Play the 2018 Conference Post to Win Game for a chance to
Integrating Technology into Care: Telehealth and Beyond Cindy Campbell RN, BSN, MHA (c) Director Operational Consulting Fazzi Associates, Inc. Play the 2018 Conference Post to Win Game for a chance to
Medicare Quality Improvement Initiatives
 Medicare Quality Improvement Initiatives Participation Opportunities in Minnesota February 2016 Achieve national quality goals in Minnesota. Join Stratis Health in working to achieve the Centers for Medicare
Medicare Quality Improvement Initiatives Participation Opportunities in Minnesota February 2016 Achieve national quality goals in Minnesota. Join Stratis Health in working to achieve the Centers for Medicare
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Pave Your Path: Improvement Science & Helpful Techniques
 Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
Pave Your Path These presenters have nothing to disclose Pave Your Path: Improvement Science & Helpful Techniques Cory Sevin, RN, MSN, NP Director, IHI Jane Taylor, EdD Improvement Advisory May 21, 2013
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Orange County Care Transitions Collaborative
 Orange County Ettie Lande, BSN, MS, ACM-RN (HSAG) Thank You! For hosting today s meeting Saddleback Memorial Medical Center 2 1 Thank You! For sponsoring today s breakfast 24Hr Home Care and Blake Naudin
Orange County Ettie Lande, BSN, MS, ACM-RN (HSAG) Thank You! For hosting today s meeting Saddleback Memorial Medical Center 2 1 Thank You! For sponsoring today s breakfast 24Hr Home Care and Blake Naudin
Care Coordination in the New CoP s. Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017
 Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Care Coordination in the New CoP s Teresa Northcutt BSN RN COS-C HCS-D HCS-H WiAHC June 2017 Selman-Holman & Associates, LLC Lisa Selman-Holman, JD, BSN, RN, HCS-D, COS-C Home Health Insight Consulting,
Home Assessments Resulting in a Positive Effect on Outcome Score Cards
 Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
Home Assessments Resulting in a Positive Effect on Outcome Score Cards Presented by: Angela Benson, OTR/L, Clinical Specialist *graduated from Mount Aloysius College, Cresson, PA *9 years of experience
New England Home Health Collaborative
 New England Home Health Collaborative The Use of Aspirin in Heart Disease Kathryn D. Roby, M.Ed., M.S., CHCE, CHAP QIN-QIO Home Health Consultant April 8, 2015 The New England Quality Innovation Network
New England Home Health Collaborative The Use of Aspirin in Heart Disease Kathryn D. Roby, M.Ed., M.S., CHCE, CHAP QIN-QIO Home Health Consultant April 8, 2015 The New England Quality Innovation Network
PRESCRIPTION FOR HEALTH A COMPREHENSIVE WEB SITE TO HELP YOU IMPROVE PATIENTS MEDICATION ADHERENCE
 PRESCRIPTION FOR HEALTH A COMPREHENSIVE WEB SITE TO HELP YOU IMPROVE PATIENTS MEDICATION ADHERENCE MEDICATION ADHERENCE Medication adherence can be defined as how well a patient s* medication behavior
PRESCRIPTION FOR HEALTH A COMPREHENSIVE WEB SITE TO HELP YOU IMPROVE PATIENTS MEDICATION ADHERENCE MEDICATION ADHERENCE Medication adherence can be defined as how well a patient s* medication behavior
High Tech, High Touch Health Care
 High Tech, High Touch Health Care February 5, 2015 2015 Qualcomm Life. All rights reserved. 1 Tectonic Shift in Care Delivery Home is the fastest growing care setting in the US. Source: AHRQ, Agency for
High Tech, High Touch Health Care February 5, 2015 2015 Qualcomm Life. All rights reserved. 1 Tectonic Shift in Care Delivery Home is the fastest growing care setting in the US. Source: AHRQ, Agency for
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Accountable Care in Infusion Nursing. Hudson Health Plan. Mission Statement. for all people. INS National Academy of Infusion Therapy
 Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Accountable Care in Infusion Nursing INS National Academy of Infusion Therapy November 14 16, 2014 Atlanta, GA Margaret (Peggy) Leonard, MS, RN-BC, FNP Senior Vice President Clinical Services Hudson Health
Neighborhoods, resources and capacity to improve
 Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Care Transitions in Behavioral Health
 Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
Janssen Pharmaceuticals, Inc. Presents: Care Transitions in Behavioral Health Chuck Ingoglia, MSW Senior Vice President, Policy and Practice Improvement, National Council for Behavioral Health Nina Marshall,
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
AHRQ Research Agenda: Incentives & Value-based Care
 AHRQ Research Agenda: Incentives & Value-based Care Richard Kronick, Ph.D. Director Agency for Healthcare Research and Quality American Board of Medical Specialties 2015 National Policy Forum Washington,
AHRQ Research Agenda: Incentives & Value-based Care Richard Kronick, Ph.D. Director Agency for Healthcare Research and Quality American Board of Medical Specialties 2015 National Policy Forum Washington,
MTM Performance & Impact On Star Ratings 2016 & Beyond - OutcomesMTM Overview
 MTM Performance & Impact On Star Ratings 2016 & Beyond - OutcomesMTM Overview Today s Speaker Dan Rodriguez, RPh, BPharm Sr. Associate Network Performance OutcomesMTM Learning Objectives - Define Medication
MTM Performance & Impact On Star Ratings 2016 & Beyond - OutcomesMTM Overview Today s Speaker Dan Rodriguez, RPh, BPharm Sr. Associate Network Performance OutcomesMTM Learning Objectives - Define Medication
Draft 2014 CMS Advanced Notice and Call Letter to Medicare Advantage and Part D Prescription Drug Plans
 Jonathan Blum Center for Medicare Center for Medicare and Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, SW, MS:314G Washington, DC 20201 [Submitted electronically to: AdvanceNotice2014@cms.hhs.gov]
Jonathan Blum Center for Medicare Center for Medicare and Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, SW, MS:314G Washington, DC 20201 [Submitted electronically to: AdvanceNotice2014@cms.hhs.gov]
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
HH Compare. IMPACT Act. Measure HHVBP
 Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Decoding the QPP Year 2 Quality Measure Benchmarks and Deciles to Maximize Performance
 Decoding the QPP Year 2 Quality Measure Benchmarks and s to Maximize Performance Leila Volinsky, MHA, MSN, RN, PCMH CCE, CPHQ Senior Program Administrator New England Regional Lead Quality Payment Program
Decoding the QPP Year 2 Quality Measure Benchmarks and s to Maximize Performance Leila Volinsky, MHA, MSN, RN, PCMH CCE, CPHQ Senior Program Administrator New England Regional Lead Quality Payment Program
Rehospitalizations: How Do You Measure Up?
 Rehospitalizations: How Do You Measure Up? National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Today s Objectives Recognize the role skilled nursing facilities
Rehospitalizations: How Do You Measure Up? National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Today s Objectives Recognize the role skilled nursing facilities
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Partnering with Pharmacists to Enhance Medication Management
 Partnering with Pharmacists to Enhance Medication Management Tamara Ravn PharmD BCACP Staff Pharmacist Clinical Cancer Pharmacy Froedtert & The Medical College of Wisconsin April 6, 2016 Objectives Describe
Partnering with Pharmacists to Enhance Medication Management Tamara Ravn PharmD BCACP Staff Pharmacist Clinical Cancer Pharmacy Froedtert & The Medical College of Wisconsin April 6, 2016 Objectives Describe
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
At EmblemHealth, we believe in helping people stay healthy, get well and live better.
 At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
INTERACT Webinar Series
 INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions
 1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Primary Care Redesign Updates to DFM
 Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
Pharmacists Improve Care Through Team Collaboration
 Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
Home Health Quality Improvement Campaign
 Home Health Quality Improvement Campaign Description of Monthly Report for Improvement in Oral Medications Monthly Report for Improvement in Management of Oral Medications All data displayed illustrate
Home Health Quality Improvement Campaign Description of Monthly Report for Improvement in Oral Medications Monthly Report for Improvement in Management of Oral Medications All data displayed illustrate
Clinical Training: Medication Reconciliation. VNAA Best Practice for Home Health
 Clinical Training: Medication Reconciliation VNAA Best Practice for Home Health Learning Objectives To understand why medication reconciliation is important to providing quality care To understand the
Clinical Training: Medication Reconciliation VNAA Best Practice for Home Health Learning Objectives To understand why medication reconciliation is important to providing quality care To understand the
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11
 Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
Medicare: 2018 Model of Care Training
 Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Improvement Activities Data Validation Criteria
 Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Medication Adherence: Strategies for Improving Outcomes
 Medication Adherence: Strategies for Improving Outcomes Thursday, June 16, 2016, 12:00 p.m. to 1:00 p.m. Andrea H. Williams, RPh, MBA President, RX CONSULTANTS LLC, Wilmington, DE EDUCATIONAL OBJECTIVES
Medication Adherence: Strategies for Improving Outcomes Thursday, June 16, 2016, 12:00 p.m. to 1:00 p.m. Andrea H. Williams, RPh, MBA President, RX CONSULTANTS LLC, Wilmington, DE EDUCATIONAL OBJECTIVES
Quality Measurement at the Interface of Health Care and Population Health
 1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons
 Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Project BOOST Be'er Outcomes by Op2mizing Safe Transi2ons Mark V. Williams, MD, FACP, MHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal
Person-Centered Accountable Care
 Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
Person-Centered Accountable Care Nelly Ganesan, MPH, Senior Director, Avalere s Evidence, Translation and Implementation Practice October 12, 2017 avalere.com @NGanesanAvalere @avalerehealth Despite Potential
Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training
 Santa Clara County Behavioral Health provider training") Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training Anthem Blue Cross Cal MediConnect Plan Effective January 1, 2015, Anthem Blue Cross
Anthem Blue Cross Cal MediConnect Plan (Medicare- Medicaid Plan) Santa Clara County Behavioral Health provider training Anthem Blue Cross Cal MediConnect Plan Effective January 1, 2015, Anthem Blue Cross
MIPS Improvement Activities: Quality Insights Tips, Tools and Support Transcript from Live Webinar
 MIPS Improvement Activities: Quality Insights Tips, Tools and Support Transcript from Live Webinar Wednesday, March 14, 2017 Good afternoon and welcome everyone. Thank you for joining us. My name is Maureen
MIPS Improvement Activities: Quality Insights Tips, Tools and Support Transcript from Live Webinar Wednesday, March 14, 2017 Good afternoon and welcome everyone. Thank you for joining us. My name is Maureen
PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE
 PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE RAJEEV KUMAR MD FACP CHIEF MEDICAL OFFICER SYMBRIA OBJECTIVES Identify elements of key literature that describes post-hospital
PREVENTING HOSPITAL READMISSIONS: PHARMACISTS ROLE IN TRANSITIONS OF CARE RAJEEV KUMAR MD FACP CHIEF MEDICAL OFFICER SYMBRIA OBJECTIVES Identify elements of key literature that describes post-hospital