Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees
|
|
|
- Juliana Gilmore
- 6 years ago
- Views:
Transcription

, AN AGENCY OF THE U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES. THE CONTENTS PRESENTED DO NOT NECESSARILY REFLECT CMS POLICY. QP1-CTSIP.")
1 Care Transitions (CT) Special Innovation Project (SIP) Improving care transitions among Medicare-Medicaid enrollees Christi Quarles Smith, PharmD Manager, Quality Programs Arkansas Foundation for Medical Care THIS MATERIAL WAS PREPARED BY THE ARKANSAS FOUNDATION FOR MEDICAL CARE INC. (AFMC), THE MEDICARE QUALITY IMPROVEMENT ORGANIZATION FOR ARKANSAS, UNDER CONTRACT WITH THE CENTERS FOR MEDICARE & MEDICAID SERVICES (CMS), AN AGENCY OF THE U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES. THE CONTENTS PRESENTED DO NOT NECESSARILY REFLECT CMS POLICY. QP1-CTSIP.PPT,1-2/13
2 Objectives Describe a Medicare SIP to reduce 30-day readmissions for Medicare-Medicaid enrollees Discuss the benefits of community organizing and coalition formation Outline the root cause analysis process for the SIP Summarize the SIP interventions used to reduce 30- day readmission rates: a home health communication toolkit and a community resource guide 2
3 Introduction to AFMC s CT SIP team
4 AFMC CT SIP team Christi Quarles Smith, PharmD AFMC Care Transitions Project Manager Nichole Sanders, PhD AFMC Epidemiologist Judy Johnston AFMC Statistical Data Analyst Jamey Mantz, RN, BSN AFMC Quality Specialist Tonyia Haynes AFMC Senior Program Coordinator Amy Witherow, MPH, CHES AFMC Coalition Coordinator Faye Nipps, MBA, RN, BSN, CPHQ AFMC Quality Specialist Jerry Wicker, BS, LNHA, CPHQ, CDP AFMC Quality Specialist Ashley Gibson, RN, BSN AFMC Quality Specialist Kristina Bondurant, PhD, MPH AFMC Epidemiologist



5 AFMC CT SIP Team Above: Dr. Nichole Sanders From Left: Jamey Mantz, Amy Witherow, Faye Nipps, Jerry Wicker, Dr. Christi Quarles Smith, Ashley Gibson, Dr. Kristy Bondurant, Tonyia Haynes Above: Judy Johnston 5
6 Medicare 30-day readmission data
7 Arkansas readmissions per 1,000 Medicare beneficiaries 7
8 Arkansas diagnosis-specific readmissions per 1,000 Medicare beneficiaries 8

9 Arkansas Medicare post-acute care setting readmissions (CY 2012) 9


10 Annual Medicare home health agency readmission rates 10
11 Improving care transitions among Medicare-Medicaid enrollees A Medicare SIP
12 Purpose Improve care transitions and reduce 30-day readmissions in the Medicare-Medicaid (dual eligible) population by: Performing a root cause analysis (RCA) of care transitions for the dual eligible (DE) enrollee population within the selected community Based on the RCA, develop and/or modify care transitions interventions for the DE population 12
13 Target population: Medicare-Medicaid beneficiaries In 2008, Arkansas had 118,000 DEs Most are chronically ill, potentially living with both functional and cognitive impairments Utilize the health care system at higher rates compared to individuals solely covered by Medicare (26 percent for DEs and 18 percent for Medicare-only) More likely to have two or more hospitalizations compared to Medicare-only patients (11 percent versus 6 percent) 13
14 Arkansas Care Transitions (ACT) DELTA The CT SIP community coalition
15 Community selection 15
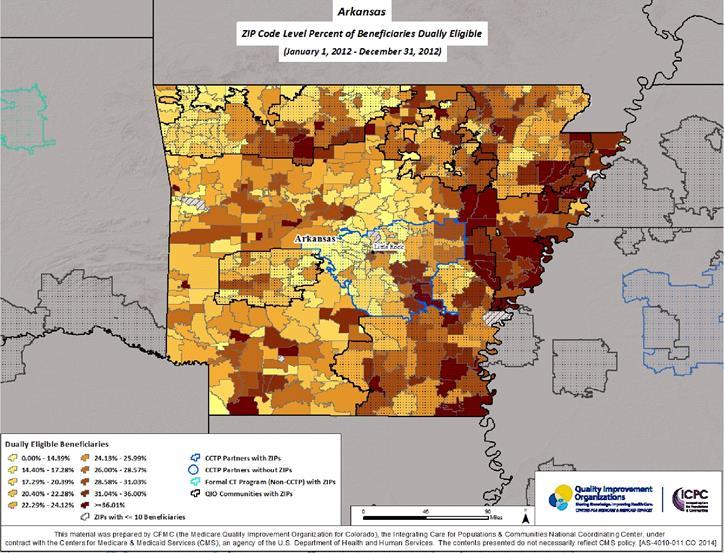
16 16

17 ACT DELTA community Located in Arkansas lower Mississippi Delta region Seven counties Approx. 7,000 DE beneficiaries 1 Nearly one in five DE beneficiaries are readmitted within 30 days 2 1. Arkansas Department of Human Services, Division of Medical Services, Medicaid Data Analytics Department, Medicare Part A Claims Data. July 1, 2011-June 30,
18 Community characteristics High rates of poverty Poor educational attainment Low literacy Low life expectancy rates High rates of chronic conditions (heart disease, diabetes, obesity, etc.) Poor access to health care/resources 18

19 ReThink Health 1 training
20 ReThink Health 1 Personal narrative Mapping of actors 1:1 meetings Coalition formation the Snowflake Model Defining your ask
21 Community organizing and coalition formation 21
22 ACT DELTA partners Eight hospitals (Greater Delta Alliance for Health, Inc.) Nine home health agencies (HHAs) 13 skilled nursing facilities (SNFs) Community health workers Civic leaders Clinics Area Agencies on Aging Hospice organizations Other health care providers/stakeholders 22
23 ACT DELTA Logo Piecing together the health care continuum.. 23

24 ACT DELTA coalition kick-off meeting April 23, attendees 32 coalition charters signed 24

25 ACT DELTA coalition kick-off meeting What does care transitions mean to you? 25


26 ACT DELTA coalition kick-off meeting We are from the ARKANSAS DELTA and this is what great health care means to us.. 26
27 Arkansas Care Transitions (ACT) DELTA Root cause analysis (RCA)
28 RCA Data analysis Medicare Part A claims data Hospital chart reviews Home health chart reviews Qualitative 1:1 meetings Focus groups at coalition meetings 28

29 RCA findings Highest readmission rates for DEs were for those discharged home with home health services 1 Poor provider-toprovider communication Underutilization of community resources 1. Medicare Part A Claims Data. July 1, 2011-June 30,
30 ACT DELTA Interventions
31 Intervention to Reduce Acute Care Transfers (INTERACT) for Home Health Agencies
32 INTERACT for HHAs Quality improvement program designed to: Reduce the frequency of acute care hospitalizations Improve early identification and evaluation of a patient s change in condition Improve communication between HHA staff and other providers (hospitals, physician offices, etc.)
33 INTERACT for HHAs Types of tools: Communication Decision support Advanced care planning Quality improvement
34 INTERACT for HHAs Toolkit implemented by nine HHAs in the coalition area Eight hospitals in the area are implementing the Hospital-to-HHA Transfer Form INTERACT training included: Two webinar training sessions Onsite trainings at each HHA by AFMC quality specialists Development and distribution of an INTERACT Tools Usage Form Virtual technical assistance as needed

35 INTERACT for HHAs HHA Capabilities Checklist Displays the capabilities of all recruited HHAs Distributed >60 lists to providers to-date 35
36 INTERACT for HHAs Most used tools SBAR tool: Situation, background, assessment, request Communication form and progress note Enhance evaluation and communication of information to primary care providers

37 INTERACT for HHAs Most used tools Stop and Watch tool: Early warning tool Aids in identification of a change in condition Can be used by any HHA staff member and/or the patient s family/caregivers
38 INTERACT for HHAs Examples of successes Using the Stop and Watch tool Using the SBAR tool Using the Medication Reconciliation tool 38
39 Community resource guides and events 39


40 Community resource guides Worked with coalition to develop a community resource guide Categorized by county and type of resource Separate guides for providers and beneficiaries 40

41 Community resource guides Provider guide: Three-ring hardcover binder > 50 guides distributed to 30 different providers Beneficiary guide: 8.5 in. x 5.5 in. softcover booklet Recently began distribution at resource guide events Online guide 41

42 Community resource events One event per county Providers and community resources exhibit for beneficiaries 42
43 ACT DELTA Results
44 Data collection Process: Monthly HHA chart reviews by AFMC quality specialists Timeframes: Baseline = (Oct. 16,2012 March 16, 2013) Remeasurement = (Oct. 16, 2013 March 16, 2014) 44

45 Number of unique DE patients identified 45
46 Emergency department (ED) visits and admissions among HHA DE patients 46

47 Percentage of DE charts with hospital discharge information present 47

48 Percentage of DE charts with community resource referrals 48

49 Community resource responses 49
50 INTERACT tool utilization 50

51 INTERACT tool usage by HHAs 51

52 Medication discrepancy rates 52

53 Admissions among DE patients 53
54 30-Day readmissions among DE patients (from chart reviews) 54
")
55 30-Day readmissions among DE patients (estimation) 55
56 For more information: Christi Quarles Smith, PharmD AFMC Care Transitions Project Manager
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Christi Quarles Smith, Pharm.D.
 CURRICULUM VITAE Christi Quarles Smith, Pharm.D. Personal Information Business Licensure: 4301 West Markham Street, Slot 571 Arkansas Pharmacist License #PD11445 72205 (issued 2010) Phone: (501) 686-6694
CURRICULUM VITAE Christi Quarles Smith, Pharm.D. Personal Information Business Licensure: 4301 West Markham Street, Slot 571 Arkansas Pharmacist License #PD11445 72205 (issued 2010) Phone: (501) 686-6694
Care Transitions in Michigan
 Care Transitions in Michigan Nancy D. Vecchioni, RN, MSN, CPHQ 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org
Care Transitions in Michigan Nancy D. Vecchioni, RN, MSN, CPHQ 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes
 Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Welcome to the Reducing Readmissions Preparation Program: Understanding Changes in Readmission Measures for Nursing Homes Lindsay Holland, MHA Director, Care Transitions, HSAG California Jennette Silao,
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
West Valley and Central Valley Care Coordination Coalitions
 West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Home Health and Care Transitions. Objectives. The Care Transitions Theme: 9/28/2010
 Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
Home Health and Care Transitions Jane Brock, MD, MSPH Colorado Foundation for Medical Care This material was prepared by CFMC, the Medicare Quality Improvement Organization for Colorado, under contract
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Best Practices. SNP Alliance. October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees
 SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
SNP Alliance Best Practices October 2013 Commonwealth Care Alliance: Best Practices in Care for Frail and Disabled Medicare Medicaid Enrollees Commonwealth Care Alliance is a Massachusetts-based non-profit,
Care Transitions: Care Across the Continuum
 Arkansas Hospital Association Hospital Engagement Network And Arkansas Foundation for Medical Care, subcontractor with TMF Quality Innovation Network Quality Improvement Organization Presents Care Transitions:
Arkansas Hospital Association Hospital Engagement Network And Arkansas Foundation for Medical Care, subcontractor with TMF Quality Innovation Network Quality Improvement Organization Presents Care Transitions:
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations
 The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
The Stepping Stones Project Community Engagement to Reduce Unnecessary Rehospitalizations Evan Stults Executive Director, Communications Quality & Safety Initiatives Qualis Health Seattle, Washington About
Early Recognition of Sepsis in Long-Term Care
 Early Recognition of Sepsis in Long-Term Care September 19, 2018 HealthInsight Team Donna Thorson Senior Project Manager Nevada Shannon Cupka Project Manager New Mexico Leah Brandis Project Manager Oregon
Early Recognition of Sepsis in Long-Term Care September 19, 2018 HealthInsight Team Donna Thorson Senior Project Manager Nevada Shannon Cupka Project Manager New Mexico Leah Brandis Project Manager Oregon
Santa Clara Care Coordination Collaborative Meeting. Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018
 June 8, 2018") Santa Clara Care Coordination Collaborative Meeting Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018 You Are Here! Improving care coordination together with
Santa Clara Care Coordination Collaborative Meeting Debra Nixon, PhD, MSHA, BSN Corporate Advisor Health Services Advisory Group (HSAG) June 8, 2018 You Are Here! Improving care coordination together with
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Care Transitions: Care Across the Continuum
 Arkansas Hospital Association Hospital Engagement Network Presents Care Transitions: Care Across the Continuum Embassy Suites, Little Rock Jointly Provided by Arkansas Foundation for Medical Care, subcontractor
Arkansas Hospital Association Hospital Engagement Network Presents Care Transitions: Care Across the Continuum Embassy Suites, Little Rock Jointly Provided by Arkansas Foundation for Medical Care, subcontractor
Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar
 Intervention Kick-Off Webinar") Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar Wednesday, January 17, 2018 National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Introduction
Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar Wednesday, January 17, 2018 National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Introduction
kaiser medicaid and the uninsured commission on O L I C Y
 P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
P O L I C Y B R I E F kaiser commission on medicaid and the uninsured 1330 G S T R E E T NW, W A S H I N G T O N, DC 20005 P H O N E: (202) 347-5270, F A X: ( 202) 347-5274 W E B S I T E: W W W. K F F.
The Stepping Stones Project Care Transitions and the Coaching Model
 The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Stepping Stones Project Care Transitions and the Coaching Model Selena Bolotin, MSW Care Transitions Project Manager Quality & Safety Initiatives Qualis Health Seattle, Washington About Qualis Health...
The Changing Landscape: A Confluence of National Attention. Eric A. Coleman, MD, MPH
 Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Infusing True Person Centered Care into Improving the Quality of Transitional Care What Are the Primary Goals for Transitioning Patients from Hospitals? Eric A. Coleman, MD, MPH, AGSF, FACP Professor of
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
The BOOST California Collaborative
 The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
The BOOST California Collaborative California HealthCare Foundation Hospital Association of Southern California LA Care Health Plan The John A. Hartford Foundation Objectives for the Day Review the rationale
Sharing advanced INTERACT Success!
 Sharing advanced INTERACT Success! Developed by the following workgroup members: Irene Fleshner Pam Zanes William Thompson Laura Tubbs Judith Taubenheim Presentations by: Matt Tobalsky, LNHA Misti Valentino,
Sharing advanced INTERACT Success! Developed by the following workgroup members: Irene Fleshner Pam Zanes William Thompson Laura Tubbs Judith Taubenheim Presentations by: Matt Tobalsky, LNHA Misti Valentino,
2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA)
") 2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA) Donna DeBello, RN Quality Improvement Director Health Services Advisory Group (HSAG): End Stage
2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA) Donna DeBello, RN Quality Improvement Director Health Services Advisory Group (HSAG): End Stage
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events
 Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
Medication Safety Quality Improvement: Collaboration to Reduce Adverse Drug Events Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota Disclosure
Quarterly Community Meeting
 (HSAG) Today s Agenda Welcome and Introduction Readmission and Adverse Drug Event (ADE) Data High-Risk Medication (HRM) Resources Behavioral Health Education and Updates Break 7-Day Readmission Focus Nursing
(HSAG) Today s Agenda Welcome and Introduction Readmission and Adverse Drug Event (ADE) Data High-Risk Medication (HRM) Resources Behavioral Health Education and Updates Break 7-Day Readmission Focus Nursing
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR
 CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
CALTCM SNF 2.0 Readmissions Webinar, Utilizing SBAR California Association of Long Term Care Medicine (CALTCM) and Health Services Advisory Group (HSAG) Wednesday, August 9, 2017 Webinar Presenters Lindsay
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Record Linkages in Project Talent
 Record Linkages in Project Talent Copyright 2011 American Institutes for Research All rights reserved. Kelly Peters Principal Psychometrician June 5, 2017 Agenda Project Talent History and Objectives Enhancing
Record Linkages in Project Talent Copyright 2011 American Institutes for Research All rights reserved. Kelly Peters Principal Psychometrician June 5, 2017 Agenda Project Talent History and Objectives Enhancing
Safe Transitions Best Practice Measures for
 Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Safe Transitions Best Practice Measures for Nursing Homes Setting-specific process measures focused on cross-setting communication and patient activation, supporting safe patient care across the continuum
Medicare and Medicaid Spending on Dual Eligible Beneficiaries
 Medicare and Medicaid Spending on Dual Eligible Beneficiaries June 2010 Presentation at the AcademyHealth Annual Research Meeting Arkadipta Ghosh James Verdier Mark Flick Ellen Singer Characteristics of
Medicare and Medicaid Spending on Dual Eligible Beneficiaries June 2010 Presentation at the AcademyHealth Annual Research Meeting Arkadipta Ghosh James Verdier Mark Flick Ellen Singer Characteristics of
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar. Thursday, December 13 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
August 25, Dear Acting Administrator Slavitt:
 August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
Quarterly Community Meeting. Barb Averyt, BSHA Director, Care Coordination and Nursing Homes Health Services Advisory Group (HSAG) April 21, 2016
 April 21, 2016") Quarterly Community Meeting Barb Averyt, BSHA Director, Care Coordination and Nursing Homes Health Services Advisory Group (HSAG) April 21, 2016 Today s Agenda 8:30 a.m. Welcome and Opening Remarks 8:45
Quarterly Community Meeting Barb Averyt, BSHA Director, Care Coordination and Nursing Homes Health Services Advisory Group (HSAG) April 21, 2016 Today s Agenda 8:30 a.m. Welcome and Opening Remarks 8:45
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Advancing Popula/on Health and Consumerism
 Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
INTERACT Webinar Series
 INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
INTERACT Webinar Series Session 4: Communication Tools (Part 1) Stop & Watch & SBAR Quality Improvement: PDSA Cycle May 27, 2015 with presenters: Florence Johnson, MSN, MHA Sheila Eckenrode, BSN, MA, CPHQ
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
M7: Reducing Avoidable Rehospitalizations. Overview of the Problem and Promising Approaches
 M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
M7: Reducing Avoidable Rehospitalizations Overview of the Problem and Promising Approaches Eric A. Coleman, MD, MPH Director, Care Transitions Program This presenter has nothing to disclose. Session Objectives
Is It Really a UTI? Do You Know It When You See It?
 Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Tools Use Suggested Formats. All facility staff Provides a visual depiction of INTERACT in daily practice
 INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
INTERACT Version 1.0 Tools This table outlines the INTERACT tools, and briefly describes their use, and suggests recommended formats for use. You may not want to use all of the tools. The core tools are
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Care Transitions Success Stories and Lessons Learned
 Care Transitions Success Stories and Lessons Learned April 30, 2015 Stratis Health, based in Bloomington, Minnesota, is a nonprofit organization that leads collaboration and innovation in health care quality
Care Transitions Success Stories and Lessons Learned April 30, 2015 Stratis Health, based in Bloomington, Minnesota, is a nonprofit organization that leads collaboration and innovation in health care quality
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
A Call to Action: Readmission Strategies from the Field
 A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
A Call to Action: Readmission Strategies from the Field Vicky Mahn-DiNicola, RN, MSN,CPHQ VP Research & Market Insights Brenda Pettyjohn, RN, CPHQ Solutions Advisor Tina Esposito Vice President, Center
CAL MEDICONNECT: Understanding the Health Risk Assessment. Physician Webinar Series
 CAL MEDICONNECT: Understanding the Health Risk Assessment Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for CAPG members. For a general overview of the
CAL MEDICONNECT: Understanding the Health Risk Assessment Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for CAPG members. For a general overview of the
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Model of Care Heritage Provider Network & Arizona Priority Care Model of Care 2018
 Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Presentation Objectives
 Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
Transforming to Value-Based Purchasing (VBP) QI tools can drive your value proposition Paul Mulhausen, MD, AGSF, FACP Medical Director Telligen Quality Improvement Network Quality Improvement Organization
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage
 Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Improving the Continuum of Care: Progress on Selected Provisions of the Affordable Care Act One Year Post-Passage March 23, 2011 marks the oneyear anniversary of the signing of the Patient Protection and
Public Policy and Health Care Quality. Readmissions: Taking Progress into the Future
 Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
2017 OIG Work Plan and Current Compliance Topics - Home Health and Hospice
 HCCA Web Conference November 20, 2015 2017 OIG Work Plan and Current Compliance Topics - Home Health and Hospice Bill Musick, BS, MBA, CHC, CHCP Senior Associate & Consulting Projects Manager Your trusted
HCCA Web Conference November 20, 2015 2017 OIG Work Plan and Current Compliance Topics - Home Health and Hospice Bill Musick, BS, MBA, CHC, CHCP Senior Associate & Consulting Projects Manager Your trusted
Leading and Sustaining Systemic Change Collaborative: Overview
 Leading and Sustaining Systemic Change Collaborative: Overview Beth Hercher, CPHQ Quality Improvement Advisor Julie Clark, LPTA Quality Improvement Advisor John Wright, MSN, RN-BC, WCC Quality Improvement
Leading and Sustaining Systemic Change Collaborative: Overview Beth Hercher, CPHQ Quality Improvement Advisor Julie Clark, LPTA Quality Improvement Advisor John Wright, MSN, RN-BC, WCC Quality Improvement
Quality Measurement at the Interface of Health Care and Population Health
 1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
Approaches to Extending Complex Care Models into the Community: Emerging Evidence
 Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Advancing innovations in health care delivery for low-income Americans Enhancing Complex Care Beyond the Walls of a Clinical Setting Series: Approaches to Extending Complex Care Models into the Community:
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling. Speaker: Thomas Martin November 2014
 Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018
 Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018 Corley Roberts, MHA, CPHQ, ACSM EP-C, EIM Quality Improvement Advisor, Qsource/atom Alliance croberts@qsource.org Readmissions
Community Data Update Knoxville Community Readmissions Coalition January 25 th, 2018 Corley Roberts, MHA, CPHQ, ACSM EP-C, EIM Quality Improvement Advisor, Qsource/atom Alliance croberts@qsource.org Readmissions
Model of Care Training
 Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
To Reduce Resident s Pain Using Non-Medicine Treatments
 Best Practices for Pain Management and Prevention of Re-admissions Angela Trahan, Mennonite Home Kris J. Modl, Dove Healthcare Jordan Emley, Grandview Heights Rehab and Healthcare August 14, 2018 To Reduce
Best Practices for Pain Management and Prevention of Re-admissions Angela Trahan, Mennonite Home Kris J. Modl, Dove Healthcare Jordan Emley, Grandview Heights Rehab and Healthcare August 14, 2018 To Reduce
Program Development. Completion of Gap Analysis. Review of Data. Multi-disciplinary team
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
What is SNF Value Based Purchasing?
 SNF Value Based Purchasing How reducing rehospitalizations impacts revenue and margins James Muller, Senior Director of Research, AHCA Marinela Shqina, Chief Financial Officer, Manchester and Vernon Manor
SNF Value Based Purchasing How reducing rehospitalizations impacts revenue and margins James Muller, Senior Director of Research, AHCA Marinela Shqina, Chief Financial Officer, Manchester and Vernon Manor
Episode Payment Models Final Rule & Analysis
 Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Episode Payment Models Final Rule & Analysis February 15, 2017 Agenda Overview Changes from Proposed Rule Categorization of Episodes Episode Attribution Reconciliation Quality Performance Cardiac Rehab
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit
 Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
5/26/2016. What's New? What's Changed? Urgent Updates QM Manual v10. Faculty Disclosure. Requirements for Successful Completion
 What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
Quality Improvement Program Evaluation
 Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
The Community based Care Transitions Program (CCTP)
") The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created
The Community-based Care Transitions Program Juliana R. Tiongson, MPH The Innovation Center Centers for Medicare and Medicaid Services 1 The Community based Care Transitions Program (CCTP) The CCTP, created