NoCVA Preventing Avoidable Readmissions. Moving Beyond the Basics March 27, 2014
|
|
|
- Milton Allen
- 5 years ago
- Views:
Transcription
1 NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014

2 Dr. Amy Boutwell
3 REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies March 27, 2014
4 Reducing Readmissions in 2014 Are we even targeting our work correctly? State-level data for VA & NC Developing a multifaceted strategy for work in 2014 Recommendations & Discussion
5 Would your targeted efforts serve these patients? 77F recently hospitalized for an infected dialysis catheter returns to the hospital 8 days following discharge with shortness of breath. 61M with 8 hospitalizations this year for shortness of breath returns to the hospital 10 days after discharge with shortness of breath. 86M with cancer hospitalized for constipation and abdominal pain returns to the hospital 1 day after discharge with abdominal pain. 45F with HIV hospitalized for pneumonia discharged to home returns to the hospital 8 days later with pneumonia.
6 77F recently hospitalized with sepsis returns 8 days later with shortness of breath 1 st hospitalization Tunneled catheter placed to initiate dialysis Acquired blood stream infection (sepsis) All anti-hypertensives and diuretic held Stabilized in ICU; transferred to floor; 14 day hospitalization At discharge BP stable x 24 hours off pressors Felt fine; eager to go home Readmission Progressively short of breath days 3-7 Volume overloaded Never resumed diuretics after d/c Patient demoralized to be back in hospital
7 61M with 8 hospitalizations this year for SOB returns to hospital 10 days post d/c with SOB 1 st hospitalization Isn t really first hospitalization is it? Intern H&P covers issues as if first presentation of HF Recognized marginal housing issues Recognized personality issues (inappropriate with staff) Refuses to work with PT At discharge Patient can not be placed in SNF due to criminal history Readmission Gained 30 lbs in 8 days oh honey, it always takes them about a week to tune me up Grabs remote, turns on TV and orders dinner
8 86M with metastatic cancer presents with abd pain and constipation, returns 1 day later with abd pain 1 st hospitalization Constipation x 8 days with abdominal pain Resolved in ED; ED concerned pain was due to cancer Observed, felt fine, started on bowel regimen At discharge Family eager to take him home Readmission Recurrent abdominal pain Family concerned it was due to cancer Family eager to do everything to have dad comfortable Patient clearly did not want to be there; didn t argue with family
9 41F with HIV hospitalized with pneumonia 1 st hospitalization: longstanding HIV Lives with mother family unaware At discharge: Discharged on anti-retroviral medications (new) Discharged on antibiotics for the pneumonia No infectious disease or primary care appointments made 2 nd hospitalization: Returned 8 days later for persistent coughing it would have helped if they made the appointment for me
10 Who is High Risk of Readmission? New diagnosis needs teaching, clear instructions New medications need medication review, instructions Complex medical needs continued active management Complex social isolated, active substance use, poverty Frailty/convalescence weakened, less able to manage Skilled care needs- nursing, therapy, medication management Personal care needs- caregiver, meals, respite Access to care needs- no PCP, financial, transportation Navigating low health literacy, language, cultural barriers Advocacy direct assistance in accessing resources/support Care seeking patterns- accustomed to using ED for care Chronic recurrent symptoms- need palliative care & care plan End of life goals of care decision making
11 TARGETED EFFORTS The good, the bad the data
12 6 Very Important Messages from CMS-1 1. Readmission reduction pays or hurts to some extent Avoidance in penalties, CMMI grants/ contracts 2. We will flood the market with all best ideas on our dime Partnership for Patients, Hospital Engagement Networks (HENs) ~ $280M 1. Reducing readmissions is a cross-continuum effort QIO 10 th SOW, Integrating Care for Populations and Communities Focused on engaging numerous providers within a community SNF readmission penalties proposed for 2017
13 6 Very Important Messages from CMS Attend to non-clinical issues eg integral role of community based support services 5. Reducing readmissions requires really good data QIO 10 th SOW social network analyses, readmissions from PAC providers, etc. 4. Hospitals must have updated processes in place May 2013 newly issues CMS Hospital Conditions of Participation
14 HOWEVER. Powerful messages from powerful agencies can create blinders
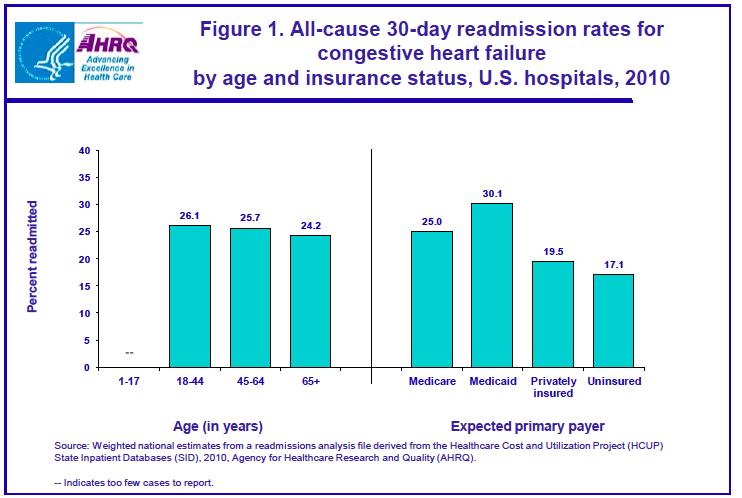
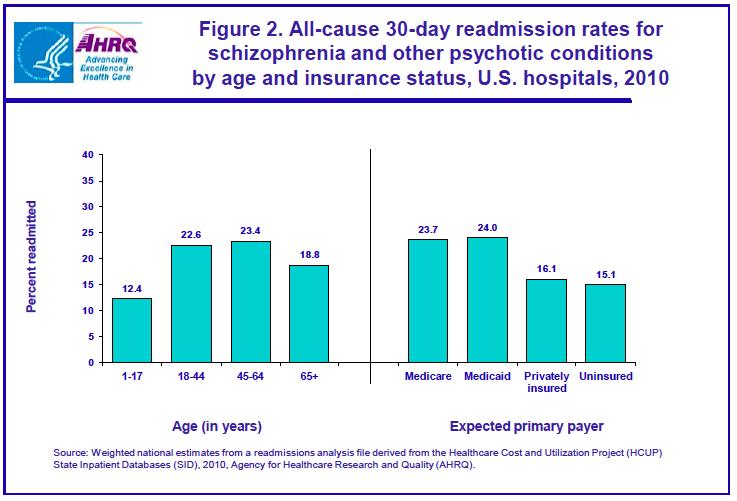
15 Inadvertent Blinders. 1. HF, AMI, PNA NOT the three most frequent causes of readmissions, even in Medicare FFS Many other very important targets, including high utilization & PAC 1. Driven a Medicare focus in the field Medicaid adults have as high or HIGHER readmission rates than Medicare FFS 2. Preferred first move: hire a transitional care FTE Lost a bit of the focus on the need to modernize & improve standard processes
16 ALL CAUSE ALL PAYER STATS

17 18 states, 14 million discharges 45% of all hospitalizations in US
18 HCUP: Readmissions by Volume
19 HCUP: Readmissions by Volume & Rate
20 HCUP: Highest Rates HCUP April 2013
21
22
23 STATE-LEVEL MEDICARE DATA Virginia & North Carolina, thanks to your QIOs
24 Medicare Readmission Stats Metric Virginia North Carolina # Medicare discharges 282, ,224 # Medicare patients 182, ,671 # Medicare readmissions 51,764 61,977 Readmission rate 18.3% 17.3% % RA to same / other hospital 76% / 24% 80% / 20% Median # days to readmission
25 Readmissions by Discharge Disposition Metric Virginia North Carolina % d/c to home / % RA from home 48% / 42% 52% / 47% Readmission rate from home 17% 16% % d/c to home health / % RA from home health 21% / 24% 18% / 22% Readmission rate among pts d/c to home health 22% 20% % d/c to SNF / % RA from SNF 21% / 25% 21% / 23% Readmission rate among pts d/c to SNF 22% 19%
26 Virginia - Top Diagnoses Leading to Readmission Discharge Diagnosis Readmission Counts Discharge Diagnosis Readmission Rates Sepsis 3806 CHF 3575 PNA 2751 COPD 2472 ARF 2273 UTI 1637 CVA 1428 Afib 1242 CAD 725 Total 19,909 % total RA 38% CHF 23.97% COPD 21.97% ARF 21.42% Sepsis 21.09% UTI 18.92% PNA 18.90% Afib 17.70% CAD 14.86% CVA 14.23% 62% all other diagnoses!
27 North Carolina - Top Diagnoses Leading to Readmission Discharge Diagnosis Readmission Counts Discharge Diagnosis Readmission Rates Sepsis 2953 CHF 2600 PNA 2379 COPD 1979 ARF 1902 Afib 1461 UTI 1402 AMI 1293 Resp Failure 1019 Total 19,909 % total RA 27% CHF 24.3% Resp Failure 24.3% COPD 20.9% ARF 19.2% AMI 18.9% Sepsis 18.7% PNA 17.4% UTI 16.8% Afib 16.5% 73% all other diagnoses!
28 Highest Impact Target Population Metric Virginia North Carolina # (%) of patients with 3 hospitalizations 23,682 (13%) 27,765 (12%) # (%) of hospitalizations used by H.U. 61,060 (22%) 108,814 (30%) # of readmissions among H.U. 36,998 42,204 % of readmissions that occur in H.U. 71% 68% Readmission rate among H.U. 40% 39%
29 CRUNCHING THE NUMBERS Will your current strategy get you to your goal?
30 Let s Run the Numbers: One Strategy Won t Get Us There Number Rate Medicare admits/year 5,000 admissions Medicare RA rate 20% # Medicare RA /year 1,000 readmissions Pilot project 200 high risk patients Pilot group RA rate 25% Expected # RA pilot 50 Expected effect of pilot 20% # RA reduced by pilot 10 # Medicare RA/year = = 990 1% Amy Boutwell 2013


31 Develop Portfolio Strategy Improve standard hospital-based care for all Identify risks & mitigate Identify learner Use Teach-back Schedule early follow up Timely communication Collaborate with receivers to improve transition SNF Circle Back INTERACT Cross-continuum teams Provide enhanced services for high risk HF clinic Transitional care Self-management coaching Intensive care management Amy Boutwell 2013
32 1. IMPROVE STANDARD CARE FOR ALL All patients, not just high risk patients
33 Standardize your Processes CMS Issued New Discharge Planning Conditions of Participation May 2013 that require hospitals demonstrate the following: 1. Have a process 2. Know your data; track rates & review readmissions 3. Assess & reassess patients for post-hospital needs 4. Engage patients and caregivers 5. Teach self-care to patients & caregivers 6. Provide a written discharge plan for all inpatients 7. Communicate effectively with receiving providers 8. Know the capabilities of area providers, including support services 9. Arrange for post-acute services, including support services
34 2. COLLABORATE WITH RECEIVERS
35 CMS New COPs: Know Your Cross-Continuum Partners While hospitals cannot address these concerns in isolation, they are expected to be knowledgeable about the care capabilities of area long term care facilities and to factor this knowledge into the discharge planning evaluation. Hospitals are expected to have knowledge of the capabilities and capacities of not only of long term care facilities, but also of the various types of service providers in the area where most of the patients it serves receive post-hospital care, in order to develop a discharge plan that not only meets the patient s needs in theory, but also can be implemented. This includes knowledge of community services, as well as familiarity with available Medicaid home and community- based services (HCBS), since the State s Medicaid program plays a major role in supporting post-hospital care for many patients.
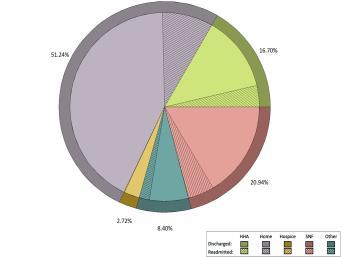






36 Readmissions from Different Care Settings Home Health Home SNF
37 Increasing Focus on SNF Readmissions, Cost, Quality 1 in 4 NH residents are hospitalized Wide variation in rates state to state (10-38%) Hospitalizations from SNF cost $14B annually Each hospitalization from SNF 33% higher cost 1 in 5 NH residents experience adverse event 60% potentially avoidable Due to inadequate care, delays Resulting hospital costs = $2.8B annually

38 Increasing Focus on SNF Readmissions, Cost, Quality Effect of Hospital-SNF Referral Linkages on Rehospitalization 1. Stronger hospital-snf linkages were found to reduce readmission rates 2. The greater the concentration of discharges a hospital sends to a single SNF, the lower the rate of readmission 3. Specifically lower rates of immediate bounce-backs (days 0-3) Rahman et al, December 2013
39
40
41 Actively Collaborate to Improve Transition Carolinas HealthCare SNF Circle Back Multi-hospital system in North Carolina Pilot in one hospital; commitment to spread system-wide if effective Problem: early readmissions from SNF Test: warm handoffs to SNF Call back to SNF 3-24 hours after transfer to answer questions Details: RCA revealed SNF-readmission patters Hospital readmission champion met with SNFs to discuss shared goals Hospital (with some leadership effort) asked SNF to participate in this communication RN calls nurse at SNF SW or care coordinator calls for follow up clarification 3-24 hours after transfer Daily workflow (with some modifications for weekends, done next business day) Follow up calls are scripted and documented in Allscripts system Pilot on paper with 1 RN and 1 SW Pilot expanded to RN call report to SNF Pilot expanded to add follow up calls Pilot expanded to build questions into Allscripts Expand to all; new standard of practice Source: Emily Skinner, Carolinas Healthcare System
42 Actively Collaborate to Improve Transition Carolinas HealthCare SNF Circle Back SNF Circle Back Questions 1. Did the patient arrive safely? 2. Did you find admission packet in order? 3. Were the medication orders correct? 4. Does the patient s presentation reflect the information you received? 5. Is patient and/or family satisfied with the transition from the hospital to your facility? 6. Have we provided you everything you need to provide excellent care to the patient? Insights Transitions are a PROCESS (forms are useful, but only a tool to achieve intent) Best done ITERATIVELY with COMMUNICATION Source: Emily Skinner, Carolinas Healthcare System
43 Actively Collaborate to Improve Transition Mass General 3-day waiver experience Warm follow-up Process with SNFs: Warm handoff from ED to SNF clinician-clinician; joint decision Support staff were available to facilitate Telephonic card flipping between MGH team & SNF Key lessons: Took a while to develop collaborative rapport v. in-charge No substitute for verbal communication and problem solving

44 Know Your Partners Capabilities

45 Know Your Partners Service Improvements
46 3. PROVIDE ENHANCED SERVICES Best transition out and reception in won t suffice for some patients
47 High Risk Care Teams Funded by hospital or ACO or plan/payer North Carolina example for nation: CCNC Often multi-disciplinary Navigator Behavioral health Social Work Pharmacist Address full complement of medical, social, logistical needs Affordable medications; waiving office visit copayments Transportation Stable housing Navigating the healthcare system, asking questions, making appointments Identify using combination of clinical and non-clinical criteria History of high utilization, no PCP, numerous prescribers, numerous meds, behavioral health comorbidities, homeless.not just chronic disease
48 Let s Run the Numbers: Three-part strategy Medicare admits/year Number 5,000 admissions Rate Medicare RA rate 20% # Medicare RA /year 1,000 readmissions 1. Improve standard care 5,000 admissions (20% RA rate) Expected effect 10% Expected # RA reduction 2. Collaborate with receivers 100 RA avoided 1650 admissions (1/3 total) (30% RA rate) Expected effect 20% Expected # RA reduction 3. Enhanced Service for Pilot 99 RA avoided 200 admissions (25% RA rate) Expected effect 20% Expected # RA reduction 10 RA avoided Total (*illustrative) 209 RA avoided* 209/1000 = 20% overall* Amy Boutwell 2013
49 RECOMMENDATIONS Updating your readmission reduction strategy in 2014
50 Recommendations 1. Know your data for ALL readmissions Don t forget sepsis, behavioral health, renal failure, cancer, frailty Recognize all these risks are the whole of general medicine 2. Move beyond Medicare or disease specific criteria 3. Recognize Medicaid as independent risk of readmission 4. Know what your current strategy is expected to achieve 5. Implement a multifaceted strategy: improve standard care, cross-setting collaboration and enhanced services
51 THANK YOU Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Lexington, Massachusetts
52 Reducing Avoidable Readmissions Collaborative June 2014 June 2015 IHI STAAR model and tools 3 in-person learning sessions Monthly content and networking webinars Small group coaching and sharing calls Guided improvement activity

53 Mission To improve transitions in care and reduce avoidable hospital readmissions.
54 Goals Reduce readmission rates by 20% (from 2010 baseline). Increase the number of patients in the pilot unit or population who undergo assessment for risk of readmission to 95%. Increase number of patients in the pilot unit or population who are assessed to be at high risk of readmission who are scheduled for a follow-up physician visit within 7 days of discharge from hospital to 95%. Increase the number of patients in the pilot unit or population who are assessed to be at high risk of readmission who receive a follow-up visit or telephone call to 95%. Test and implement process improvements in four key areas: enhanced assessment of post-hospital needs, effective teaching/enhanced learning, ensuring post-hospital care follow-up and providing real-time handover communications. 10% improvement or national 25 th percentile in scores on four HCAHPS dimensions
55 Methods Pilot Unit Multidisciplinary tiered project team Assessment of 5 recent readmissions Observations Process maps Risk assessment Follow up appointments and follow up calls or visits
56 Methods Test improvement in 4 key areas: Enhanced assessment of patient post-hospital needs Effective teaching and enhanced patient learning Ensuring post-hospital care follow-up Providing real-time handover communications Implement and spread improvements Community engagement readiness assessment Community cross continuum team
57 For all NoCVA hospitals: Quarterly webinars Resources on website Targeted 1:1 coaching NC ACT Care Transitions Summit January 30, 2015
58 Contact For more information, contact: Laura Maynard, Director of Collaborative Learning, Erica Preston-Roedder, Director of Quality Measurement, Dean Higgins, Project Manager,
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
ASPIRE to Reduce Readmissions
 ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
ASPIRE to Knockout Pneumonia Readmissions Webinar #1. Amy Boutwell, MD, MPP March 1, 2018
 ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia. Webinar #3 Post-Acute Care Readmissions September 8, 2016
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
Preventing Avoidable Readmissions: Collaborative Measurement. July 24, 2013
 Preventing Avoidable Readmissions: Collaborative Measurement July 24, 2013 Collaborative Goals Reduce readmission rates by 20% Increase the number of patients in the pilot unit or population who undergo
Preventing Avoidable Readmissions: Collaborative Measurement July 24, 2013 Collaborative Goals Reduce readmission rates by 20% Increase the number of patients in the pilot unit or population who undergo
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement.
 Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Effective Care Transitions to Reduce Hospital Readmissions
 Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Effective Care Transitions to Reduce Hospital Readmissions November 8, 2017 Anchorage, Alaska The vicious cycle of readmissions What is Care Transitions? The movement of patients across settings, referred
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
Executive Summary CREATING A CULTURE OF QUALITY Pursuing Excellence in Care Transitions Enhancing Safety in Kidney Patient Care September 11-12, 2012
 Executive Summary CREATING A CULTURE OF QUALITY Pursuing Excellence in Care Transitions Enhancing Safety in Kidney Patient Care September 11-12, 2012 Core Objectives: 1. Why is it important to improve
Executive Summary CREATING A CULTURE OF QUALITY Pursuing Excellence in Care Transitions Enhancing Safety in Kidney Patient Care September 11-12, 2012 Core Objectives: 1. Why is it important to improve
HCAHPS and Readmissions: Making the Connection Wednesday, September 18, :00 a.m. 10:00 a.m.
 HCAHPS and Readmissions: Making the Connection Wednesday, September 18, 2013 9:00 a.m. 10:00 a.m. Facilitated by: Katie McCullough, VHHA and Carla Thomas, VHQC Session Objectives: Understand the published
HCAHPS and Readmissions: Making the Connection Wednesday, September 18, 2013 9:00 a.m. 10:00 a.m. Facilitated by: Katie McCullough, VHHA and Carla Thomas, VHQC Session Objectives: Understand the published
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
30-day Hospital Readmissions in Washington State
 30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Care Transitions: Don t Lose Your Patients
 Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
Care Transitions: Don t Lose Your Patients Sabrina Edgington, MSSW Program and Policy Specialist National Health Care for the Homeless Council March 14, 2013 CARE TRANSITIONS Definition The movement of
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Pharmacists Improve Care Through Team Collaboration
 Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
STAAR Initiative STate Action on Avoidable Rehospitalizations
 Amy Boutwell, MD MPP Primary Investigator, STAAR Initiative Institute for Healthcare Improvement Commonwealth Fund-supported initiative to reduce avoidable rehospitalizations, taking states as unit of
Amy Boutwell, MD MPP Primary Investigator, STAAR Initiative Institute for Healthcare Improvement Commonwealth Fund-supported initiative to reduce avoidable rehospitalizations, taking states as unit of
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS 4/19/2016. April 20, 2016
 HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
Readmission Prevention: A Community Collaborative Approach
 Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Readmission Prevention: A Community Collaborative Approach Kim Fuller, Administrative Director, Case Management, Shawnee Mission Medical Center Catherine Lauridsen RN, BSN, Care Transition Coach, Shawnee
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
 Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)") Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs) Referral Review referrals to determine if care needs can be met in your facility by: Triaging
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Medical Home as a Platform for Population Health
 Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
Deborah Perian, RN MHA CPHQ. Reduce Unplanned Hospital Admissions: Focus on Patient Safety
 Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
Deborah Perian, RN MHA CPHQ Reduce Unplanned Hospital Admissions: Focus on Patient Safety Objectives At the end of this lesson, the learner will be able to: Identify key clinical and policy issues associated
NoCVA North Carolina Preventing Avoidable Readmissions Collaborative
 NoCVA North Carolina Preventing Avoidable Readmissions Collaborative Measurement Update, Using A3, and Community Engagement Check-in April 17, 2013 Agenda Measurement Updates A3: Homework Review and Problem
NoCVA North Carolina Preventing Avoidable Readmissions Collaborative Measurement Update, Using A3, and Community Engagement Check-in April 17, 2013 Agenda Measurement Updates A3: Homework Review and Problem
Patient-Centered Case Management Assessment & Patient Interview Techniques
 Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
Patient-Centered Case Management Assessment & Patient Interview Techniques Rose M. Turner, RN, BSN, ACM Thursday, January 8 th, 2015 The information provided in AHC Media Webinars does not, and is not
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Neighborhoods, resources and capacity to improve
 Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Performance Scorecard 2013
 NORTHWESTERN LAKE FOREST HOSPITAL Performance Scorecard 2013 updated May 2013 Northwestern Lake Forest Hospital is committed to providing the communities we serve the highest quality health care through
NORTHWESTERN LAKE FOREST HOSPITAL Performance Scorecard 2013 updated May 2013 Northwestern Lake Forest Hospital is committed to providing the communities we serve the highest quality health care through
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 2010, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 2012, the
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care
 Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Stanford Coordinated Care
 Stanford Coordinated Care Support the patients, manage their care Ann Lindsay MD Alan Glaseroff MD IHI Innovation Network Webinar April 12, 2013 Where s the Leverage on Trend? Registries Gaps in Care Planned
Stanford Coordinated Care Support the patients, manage their care Ann Lindsay MD Alan Glaseroff MD IHI Innovation Network Webinar April 12, 2013 Where s the Leverage on Trend? Registries Gaps in Care Planned
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter