HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia. Webinar #3 Post-Acute Care Readmissions September 8, 2016
|
|
|
- Patricia Pierce
- 5 years ago
- Views:
Transcription



1 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016

2 HOUSEKEEPING Slides were sent this morning Webinar is being recorded Please use the telephone option Audio pin prompt All participants are muted Raise your hand Ask a question Warm up
 965-1214")
3 WELCOME AND OVERVIEW Abraham Segres VHHA Vice President, Quality & Patient Safety (804)
4 VIRGINIA HOSPITAL & HEALTHCARE ASSOCIATION An association of 30 member health systems representing 107 community, psychiatric, rehabilitation and specialty hospitals throughout Virginia. Vision Through the power of collaboration, the association will be the recognized driving force behind making Virginia the healthiest state in the nation by Mission Working with our members and other stakeholders, the association will transform Virginia s health care system to achieve top-tier performance in safety, quality, value, service and population health. The association s leadership is focused on: principled, innovative and effective advocacy; promoting initiatives that improve health care safety, quality, value and service; and aligning forces among health care and business entities to advance health and economic opportunity for all Virginians.

5 VHHA IMPROVEMENT PRIORITIES 1. Hospital readmissions 1a. Hospital-wide 1b. Post-acute transfers 1c. Total hip/total knee Replacement 30-day readmissions 2. Clostridium difficile Healthcare-acquired Infections 3. Patient Experience HCAHPS 4. Serious Safety Events
6 Statewide Learning & Action Statewide collaborative June 2016 to November 2018 Focus on PAC, HU, THR/TKR in parallel Engage with partners in PAC Engage with VHQC for cross-continuum work Engage with AAAs for community based care/cti Provide, use, interpret data from VHHA & VHQC
7 Planned Activities for Learning & Action June 16 th* August 17 th* September 8 th* October 20 th* High Leverage Strategies Data/Measurement Reducing PAC Readmissions Improving Care for High Utilizers November 15 th In-Person Learning Event 9-3:30 *All webinars will be offered at 10am

8 A FEW OF OUR PARTNERS Virginia Healthcare Association (VHCA) Virginia Association of Home Care and Hospice LeadingAge Virginia VHQC Virginia Department of Aging & Rehabilitative Services (DARS)


9 REDUCING READMISSIONS FROM POST-ACUTE CARE Amy Boutwell, MD, MPP Collaborative Healthcare Strategies President (617)
10 AGENDA Readmissions from post-acute care in Virginia Identifying root causes of readmissions from post-acute care Developing a multi-faceted approach to reducing readmissions from post-acute care Specific action steps
11 OBJECTIVES 1. Describe common root causes of readmissions from post-acute care, and identify practical ways for hospitals and PAC providers to identify their own root causes; 2. Describe 3 effective strategies for reducing readmissions for patients discharged to post-acute care; 3. Discuss methods used to collaborate with post acute providers



12 PORTFOLIO OF STRATEGIES Reduce PAC Readmissions Improve processes & practices for SNF patients Improve processes & practices for Home Health patients Reduce All Cause All Payer Readmissions by 20% by 2020 Reduce HU Readmissions Whole-person care teams, care plans Reduce Total Hip/Knee Replacement Readmissions Improve pre-op, peri-op, post-op and rehab practices & processes Reduce Readmissions from Home Coaching and Linkage to Services (AAA/SIM)
13 READMISSIONS FROM POST ACUTE CARE IN VIRGINIA

14 READMISSIONS BY DISCHARGE DISPOSITION IN VIRGINIA Medicare FFS Readmission Rates, by Discharge Setting: Home, SNF, HH 20% PAC 18.6% Average Axis Title % Home Q1 Q2 Q3 Q4 Home HHA SNF State Avg Source: 2015 VA Medicare FFS data, courtesy of VHQC
15 KEY STATISTICS TO KNOW Medicare ~275k Medicare discharges ~50k Medicare readmissions ~18% Medicare readmission rate Medicare to PAC ~110k Medicare discharges to PAC ~22k readmissions from PAC ~20% readmission rate ~40% of discharges are to post acute care A 20% reduction would avoid 4,400 readmissions per year in VA Reducing PAC readmissions would reduce the state-wide rate from 18.2% to 16.6% *PAC = Home Health or SNF
16 CALCULATE THE IMPACT OF REDUCING PAC READMISSIONS ON YOUR HOSPITAL S READMISSION RATE Formula Example Total hospital* discharges A 1000 Total hospital readmissions B 150 Hospital readmission rate = B/A 15% Total PAC** discharges (40% of total) C =.4A 400 Total PAC readmissions (20% rate) D =.2C 80 Goal: 20% reduction PAC readmissions =.20 x D 16 New hospital readmissions = B (.2D) = E = 134 New hospital readmission rate = E/A 13.4% Calculate this for your hospital * hospital = adult, non-ob **PAC = Home Health or SNF
17 EXAMINE ROOT CAUSES OF READMISSIONS FROM PAC
18 ROOT CAUSES OF READMISSIONS Incomplete information about clinical status Incomplete information about functional status Incomplete information about behavioral health or sundowning Missing hard copies of controlled substance prescriptions Missing documentation of placement of tubes or lines (eg picc lines) Delays in obtaining (rare, expensive) medications Change in clinical status requiring provider evaluation but not emergencies Patient/family dissatisfaction with the facility seeking different placement Readmissions following discharge from SNF to home
19 Purpose: READMISSION REVIEW TOOL To understand patient perspective To understand root causes To understand there are multiple factors To identify opportunities for improvement To develop a better plan for the patient To develop better services to offer Recommendation: Conduct at least 5 Best practice: review all readmissions AHRQ Hospital Guide to Reducing Medicaid Readmissions


20 Available at:

21 READMISSIONS AFTER TRANSITION FROM SNF TO HOME 55,980 Medicare d/c from 694 SNFs 67% d/c to home care after SNF 12,350 (22%) returned to acute care <30d 15% readmitted ~50% of returns <30d occurred <10d! indicates the need for interventions to improve transition from SNF to home Toles et al JAGS 2014
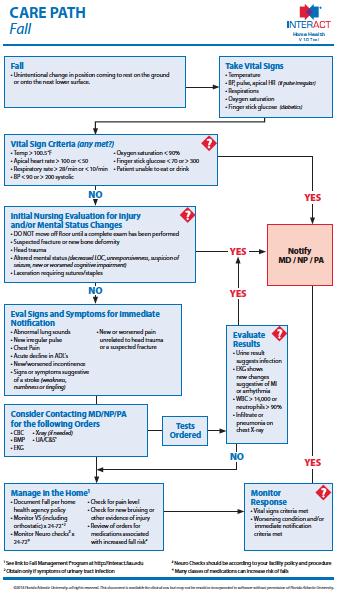
22 BEST PRACTICES Interview (readmission review) patients while they are in the hospital Listen for all of the factors that contributed to a readmission Ask the person who sent the patient to the ED to provide their perspective View all readmissions as potentially avoidable by asking 5 whys Readmission review and root cause analyses is most productive when conducted in the spirit of open inquiry and seeking opportunities to improve Use readmission reviews and root cause analysis as the basis for your collaborative work with post-acute providers
23 REDUCING READMISSIONS FROM PAC: BEST PRACTICES Collaborate in managing care across settings and over time: not just a handoff
24 PAC BEST PRACTICE #1 SNF WARM HANDOFFS WITH CIRCLE BACK Warm RN-RN Handoff to SNF Hospital calls back SNF 3-24h after d/c to ask 6 questions 1. Did the patient arrive safely? 2. Did you find admission packet in order? 3. Were the medication orders correct? 4. Does the patient s presentation reflect the information you received? 5. Is patient and/or family satisfied with the transition from the hospital to your facility? 6. Have we provided you everything you need to provide excellent care to the patient? Source: Emily Skinner, Carolinas Healthcare System
25 PAC BEST PRACTICE #2 ACUTE CARE MANAGEMENT TEAM WARM FOLLOW UP ACO or Bundle clinical coordinator Air traffic control (lists of patients, coordinates virtual co-management rounds) Physical rounds in SNF Acute Care Team sends RN / NP to see patient, discuss plan with SNF staff Respond to changes in clinical status to manage in setting Virtual care management rounds with SNF Weekly telephonic rounds ACO/bundle coordinator and SNF LOS, progress toward discharge goals, discharge planning Tele-medicine consults in SNF Direct admit to SNF from home if need escalated care
26 LESSONS FROM ACOS AND BUNDLES Key lessons: Took time to develop a collaborative rapport v. hospital in-charge No substitute for verbal communication and problem solving Active co-management and care management gets results
27 PAC BEST PRACTICE #3 HALLMARK HEALTH SYSTEM TREAT-AND-RETURN TO SNF Hallmark Health System 2 hospital system, 20 ED docs, 17 PAs Why are almost all SNF patients admitted? Patients only seen once a month ; can t do IVs, etc If they send them here they can t take care of them Actions: Asked ED clinicians 5 whys Education: posted INTERACT SNF capacity sheets in ED Simplicity : establish contacts, standard transfer information # Treat-and-Return to SNF Results: increase in number of patients transferred from ED to SNF Source: Dr Steven Sbardella, CMO and Chief of ED Hallmark Health System Melrose, MA
28 PAC BEST PRACTICE #4 SNF TRANSITION TO HOME PROGRAM Home and Healthy Program Comprehensive discharge planning: appointments, services made Reviews all information with resident, family, caregiver Direct contact after SNF discharge Phone call next day Once a week for a month Once a month for 3 months Courtesy of Keswick Multi-Care, Maryland
29 INTERACT TOOLS TO REDUCE POST-ACUTE HOSPITALIZATIONS Hospitals need to know these tools in order to more effectively collaborate
 Customized Guides for SNF,")



30 INTERACT (INTERVENTIONS TO REDUCE ACUTE CARE TRANSFERS) Customized Guides for SNF, Home Health and Assisted Living Facilities Implementation Guide Measurement and Root Cause Analyses Tools Changes in Clinical Status Tools Hospital Communication Tools Patient / Family Communication Tools All available for free to download at

31 Available at:


32 Available at:


33 Available at:


34 Available at:


35 Available at:

36 Available at:


37 Available at:
38 COLLABORATING WITH PAC PROVIDERS TO REDUCE READMISSIONS


39 AHRQ Hospital Guide to Reducing Medicaid Readmissions


40 AHRQ Hospital Guide to Reducing Medicaid Readmissions


41 Available at:
42 BEST PRACTICES OF CROSS SETTING COLLABORATION Shared understanding of (best-available) data Shared understanding of patients and caregivers perspective Shared understanding of receivers perspective Clear articulation of specific, feasible opportunities for improvement Improvements are made & hardwired into new standard processes Regular meetings, active collaboration and joint problem-solving
43 OPPORTUNITIES AND RECOMMENDATIONS

44 VHQC CAN SUPPORT YOUR EFFORTS TO WORK WITH PAC PROVIDERS Contact Carla Thomas:
45 ADDITIONAL WEBINAR THIS WEEK Attend the national launch webinar for the Agency for Healthcare Research and Quality s Hospital Guide to Reducing Medicaid Readmissions This new guide supports hospitals in developing a data-informed and whole-person approach to reducing readmissions, using the ASPIRE Framework Tomorrow: Friday September 9 from 3-4:30 No cost to attend Registration link can be found on Amy Boutwell s LinkedIn page
46 RECOMMENDATIONS 1. Know your data: how many discharges and readmissions from PAC? 2. Review 5 readmissions from post-acute care settings 3. Convene a meeting with a group of post acute providers 4. Identify 3 ways the hospital can improve the transition from hospital to PAC 5. Identify 3 ways the PAC provider(s) can reduce acute care transfers
47 QUESTIONS?
48 THANK YOU FOR YOUR COMMITMENT TO REDUCING READMISSIONS Amy E. Boutwell, MD, MPP Advisor, VHHA Center for Healthcare Excellence President, Collaborative Healthcare Strategies
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
ASPIRE to Reduce Readmissions
 ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Organizational Overview
 Organizational Overview June 2015 Background The Virginia Hospital & Healthcare Association (VHHA) consists of 30 member health systems, representing 107 community, psychiatric, rehabilitation and specialty
Organizational Overview June 2015 Background The Virginia Hospital & Healthcare Association (VHHA) consists of 30 member health systems, representing 107 community, psychiatric, rehabilitation and specialty
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
NoCVA Preventing Avoidable Readmissions. Moving Beyond the Basics March 27, 2014
 NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Care Alert Sprint: Introduction & Goals. December
 Care Alert Sprint: Introduction & Goals December 14 2016 Agenda Purpose of the care alert sprint Specific goal, timeline, measurement Key concepts and resources Schedule of webinars, meetings Helpful tips
Care Alert Sprint: Introduction & Goals December 14 2016 Agenda Purpose of the care alert sprint Specific goal, timeline, measurement Key concepts and resources Schedule of webinars, meetings Helpful tips
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement.
 Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
HCAHPS and Readmissions: Making the Connection Wednesday, September 18, :00 a.m. 10:00 a.m.
 HCAHPS and Readmissions: Making the Connection Wednesday, September 18, 2013 9:00 a.m. 10:00 a.m. Facilitated by: Katie McCullough, VHHA and Carla Thomas, VHQC Session Objectives: Understand the published
HCAHPS and Readmissions: Making the Connection Wednesday, September 18, 2013 9:00 a.m. 10:00 a.m. Facilitated by: Katie McCullough, VHHA and Carla Thomas, VHQC Session Objectives: Understand the published
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
ASPIRE to Knockout Pneumonia Readmissions Webinar #1. Amy Boutwell, MD, MPP March 1, 2018
 ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care
 Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Skills, Technologies & Attributes Case Managers Need to Succeed In Value- Based Care January 19, 2017 Kimberly S. Hodge, MSN, RN, ACNS-BC, CCRN-K Learning Objectives After attending this presentation,
Care Transitions in Michigan
 Care Transitions in Michigan Nancy D. Vecchioni, RN, MSN, CPHQ 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org
Care Transitions in Michigan Nancy D. Vecchioni, RN, MSN, CPHQ 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org 22670 Haggerty Road, Suite 100, Farmington Hills, MI 48335 www.mpro.org
Rhonda Dickman, RN, MSN, CPHQ
 Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Rhonda Dickman, RN, MSN, CPHQ Rhonda Dickman is a Quality Improvement Specialist with the Tennessee Hospital Association s Tennessee Center for Patient Safety, supporting hospitals in their quality improvement
Quality and Health Care Reform: How Do We Proceed?
 Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
Quality and Health Care Reform: How Do We Proceed? Susan D. Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Dean of Clinical Affairs Quality and Patient Safety Associate Professor
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Value Based Care in LTC: The Quality Connection- Phase 2
 Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Value Based Care in LTC: The Quality Connection- Phase 2 Joseph J. Tomaino, M.S., R.N., Principal Healthcare Transformation Consulting ChemRx/PharmMerica Geriatric Skilled Nursing Seminar December 7, 2017
Data-Driven Strategy for New Payment Models. Objectives. Common Acronyms
 Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
Data-Driven Strategy for New Payment Models Mark Sharp, CPA Partner msharp@bkd.com Objectives Understand new payment model reforms and bundling arrangements Learn how these new payment models can impact
IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4
 Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, July 25, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 4 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
Partnerships: Developing an Elective Joint Replacement Program
 Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
Partnerships: Developing an Elective Joint Replacement Program Amy R. Ehrlich, MD Angela Schonberg, MPT Wojciech Rymarowicz, MPT Overview Session Overview: Montefiore network Program Development Data and
Glendale Healthier Community Care Coordination Collaborative. Health Services Advisory Group (HSAG) March 06, 2018
 March 06, 2018") Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
Glendale Healthier Community Care Coordination Collaborative Health Services Advisory Group (HSAG) March 06, 2018 Today s Agenda and Packet Materials Welcome and Introductions Community Readmissions and
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
Care Transitions The most interesting things happen in doorways --Inferno, Dan Brown. The Triple Aim through the Lens of Care Transitions
 Care Transitions The most interesting things happen in doorways --Inferno, Dan Brown An Under recognized Key to Improving Transitional Care: Feedback Loops Eric A. Coleman, MD, MPH But Dr. Coleman, we
Care Transitions The most interesting things happen in doorways --Inferno, Dan Brown An Under recognized Key to Improving Transitional Care: Feedback Loops Eric A. Coleman, MD, MPH But Dr. Coleman, we
A Brave New World: Lessons Learned From Healthcare Reform. Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage
 A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
A Brave New World: Lessons Learned From Healthcare Reform Brandy Shumaker, MBA, LPTA, LNHA Regional Vice President HealthPRO/Heritage 1 Learning Objectives Participants will understand: The impact health
Financial Policy & Financial Reporting. Jay Andrews VP of Financial Policy
 Financial Policy & Financial Reporting Jay Andrews VP of Financial Policy 1 Members & Groups Supported Center for Healthcare Excellence Hospital Leadership & Quality Departments Hospital Finance Departments
Financial Policy & Financial Reporting Jay Andrews VP of Financial Policy 1 Members & Groups Supported Center for Healthcare Excellence Hospital Leadership & Quality Departments Hospital Finance Departments
Measure Applications Partnership (MAP)
") Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Measure Applications Partnership (MAP) Uniform Data System for Medical Rehabilitation Annual Conference Aisha Pittman, MPH Senior Program Director National Quality Forum August 9, 2012 Overview MAP Background
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor of Medicine, Brown University
 Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Improving the Safety of Care Transitions through Best Practices and Community Collaboration The Rhode Island Experience Rebekah Gardner, MD Senior Medical Scientist, Healthcentric Advisors Assistant Professor
Post-Acute Care. December 6, 2017 Webinar Louise Bryde and Doug Johnson
 Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Care December 6, 2017 Webinar Louise Bryde and Doug Johnson Topics for Discussion Background What Is Post Acute Care? Lexicon Levels of Care Why Focus on Post Acute Care? Emerging PAC Trends
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017
 Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Post-Acute Preferred Provider Arrangements Strategies for Partnership Transacting in the Post-Acute Care Space Crash Course November 28, 2017 2017 Epstein Becker & Green, P.C. All Rights Reserved. ebglaw.com
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
The Impact of Health Care Reform on Long- Term Care
 The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
The Impact of Health Care Reform on Long- Term Care AMY RUNGE, CPA Moss Adams LLP Partner & National Practice Leader, Long-Term Care MARCY BOYD, CPA Moss Adams LLP Partner September 22, 2014 1 The material
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
CASE MANAGEMENT. Process into Practice
 CASE MANAGEMENT Process into Practice HINTS Prep Handbook- candidate and written Think globally Study Buddy Scenarios First TESTING Handbook Review Find textbooks on the case management process Multiple
CASE MANAGEMENT Process into Practice HINTS Prep Handbook- candidate and written Think globally Study Buddy Scenarios First TESTING Handbook Review Find textbooks on the case management process Multiple
Physician Performance Analytics: A Key to Cost Savings
 Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
What is Value-Based Care
 Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers
 Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
Partners in the Continuum of Care: Hospitals and Post-Acute Care Providers Presented to the Wisconsin Association for Home Health Care November 3, 2017 By: Laura Rose WHA Vice President, Policy Development
The Future of Healthcare Delivery; Are we ready?
 The Future of Healthcare Delivery; Are we ready? Lisa K. Saladin, PT, PhD, FAPTA Dean and Professor Medical University of South Carolina copyright LisaSaladin 2016 Objectives 1. Discuss 5 of the projected
The Future of Healthcare Delivery; Are we ready? Lisa K. Saladin, PT, PhD, FAPTA Dean and Professor Medical University of South Carolina copyright LisaSaladin 2016 Objectives 1. Discuss 5 of the projected
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Introduction 4/7/2015
 The Perfect Storm: A Distinguished Post-Acute Rehabilitation Program (Session # W25) Wednesday April 29 th, 2:30-4:30 Presented by: Hilary Forman PT, RAC-CT Senior Vice President of Clinical Strategies
The Perfect Storm: A Distinguished Post-Acute Rehabilitation Program (Session # W25) Wednesday April 29 th, 2:30-4:30 Presented by: Hilary Forman PT, RAC-CT Senior Vice President of Clinical Strategies
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
The Challenges and Opportunities in Using Data Bundled Payment, Care Improvement
 The Challenges and Opportunities in Using Data Bundled Payment, Care Improvement Helen Macfie, Pharm.D., FABC For IHI Leading Population Heath Transformation February, 2017 It started with a project PHYSICIAN
The Challenges and Opportunities in Using Data Bundled Payment, Care Improvement Helen Macfie, Pharm.D., FABC For IHI Leading Population Heath Transformation February, 2017 It started with a project PHYSICIAN
Transitions of Care. Scott Clark, President Leading Edge Health Care
 Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
Transitions of Care Scott Clark, President Leading Edge Health Care Tools to Reduce Readmissions Skilled Home Health Services (VNA) Private Duty Home Health Housecalls Physician Practice R.E.A.C.H. Program
4/26/2016. The future is not what it used to be. Driving Transformation for Comprehensive Care for Joint Replacement (CJR) Understand Redesign Align
 Understand Redesign Align") Driving Transformation for Comprehensive Care for Joint Replacement (CJR) Redesign Align 22 ND A N N U A L M ID W E S T C A R E C O O R D IN AT IO N C O N F E R E N C E The future is not what it used to
Driving Transformation for Comprehensive Care for Joint Replacement (CJR) Redesign Align 22 ND A N N U A L M ID W E S T C A R E C O O R D IN AT IO N C O N F E R E N C E The future is not what it used to
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
Healthcare Transformation and the Affordable Care Act David Nilasena, MD, MSPH, MS Chief Medical Officer, CMS Region VI
 National Readmission Prevention Collaborative Dallas, TX October 22, 2015 Healthcare Transformation and the Affordable Care Act David Nilasena, MD, MSPH, MS Chief Medical Officer, CMS Region VI Disclaimers
National Readmission Prevention Collaborative Dallas, TX October 22, 2015 Healthcare Transformation and the Affordable Care Act David Nilasena, MD, MSPH, MS Chief Medical Officer, CMS Region VI Disclaimers
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Connecting Care Across the Continuum
 Connecting Care Across the Continuum A Guide for Providers > Discharging patients should be quick, easy, and painless for everyone including patients, families and the hospital. That s why a hospital that
Connecting Care Across the Continuum A Guide for Providers > Discharging patients should be quick, easy, and painless for everyone including patients, families and the hospital. That s why a hospital that
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
HRET HIIN Reducing Sepsis Readmissions Virtual Event. Fishbowl Event #2 May 8, 2018
 HRET HIIN Reducing Sepsis Readmissions Virtual Event Fishbowl Event #2 May 8, 2018 1 Radhika Parekh, MHA Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
HRET HIIN Reducing Sepsis Readmissions Virtual Event Fishbowl Event #2 May 8, 2018 1 Radhika Parekh, MHA Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS 4/19/2016. April 20, 2016
 HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
RPC VALUE BASED PAYMENT AD HOC WORK GROUP EDUCATIONAL SERIES: Care Transitions Network. July 12, PM
 RPC VALUE BASED PAYMENT AD HOC WORK GROUP EDUCATIONAL SERIES: Care Transitions Network July 12, 2017 1-2PM AGENDA Welcome Regional Planning Consortiums VBP Ad Hoc Work Groups Care Transitions Network Q&A
RPC VALUE BASED PAYMENT AD HOC WORK GROUP EDUCATIONAL SERIES: Care Transitions Network July 12, 2017 1-2PM AGENDA Welcome Regional Planning Consortiums VBP Ad Hoc Work Groups Care Transitions Network Q&A
What s Next for CMS Innovation Center?
 What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
West Valley and Central Valley Care Coordination Coalitions
 West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Medical Home as a Platform for Population Health
 Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Medical Home as a Platform for Population Health Population Health Colloquium March 8, 2016 Emily Brower Vice President, Population Health Atrius Health Emily_Brower@atriushealth.org 2016 Atrius Health,
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Healthcare Workforce to Promote
 Accreditation, Certification, and Credentialing: Levers for Training the Healthcare Workforce to Promote Children s Behavioral Health Marci Nielsen, PhD, MPH President & CEO Patient-Centered Primary Care
Accreditation, Certification, and Credentialing: Levers for Training the Healthcare Workforce to Promote Children s Behavioral Health Marci Nielsen, PhD, MPH President & CEO Patient-Centered Primary Care
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS
 Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
Kate Goodrich, MD MHS Director, Quality Measurement and Health Assessment Group, CMS CMS support of Health Care Delivery System Reform (DSR) will result in better care, smarter spending, and healthier
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Webinar Instructions. A nonprofit service and advocacy organization National Council on Aging
 Webinar Instructions 1 Health Care and Community-Based Organizations: A Win-Win Partnership Sue Lachenmayr, MPH, CHES Program Director Center for Healthy Aging National Council on Aging Pam Piering Consultant,
Webinar Instructions 1 Health Care and Community-Based Organizations: A Win-Win Partnership Sue Lachenmayr, MPH, CHES Program Director Center for Healthy Aging National Council on Aging Pam Piering Consultant,
Improving Health Status through Behavioral Health Interventions
 Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
Comorbidity in the Dual Eligible Population: Improving Health Status through Behavioral Health Interventions PREPARED FOR THE CALIFORNIA ASSOCIATION OF HEALTH PLANS 2013 SEMINAR SERIES JUNE 25, 2013 BEACON
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Objectives. Assisted Living. O 2 : Opportunities & Outcomes in Assisted Living. Presented by: Chief Clinical Officer
 O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
O 2 : Opportunities & Outcomes in Assisted Living Presented by: Leigh Ann Frick, PT, MBA Chief Clinical Officer Melissa Moffitt, MS, CCC-SLP Senior Vice President of Senior Living Objectives Identify the
Postacute care (PAC) cost variation explains a large part
 cost variation explains a large part") INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
INNOVATIVE GERIATRIC PRACTICE MODELS: PRELIMINARY DATA Creating a Network of High-Quality Skilled Nursing Facilities: Preliminary Data on the Postacute Care Quality Improvement Experiences of an Accountable
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Welcome and Orientation Webinar
 Welcome and Orientation Webinar Care Transitions Network for People with Serious Mental Illness National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of
Welcome and Orientation Webinar Care Transitions Network for People with Serious Mental Illness National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of
MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships
 MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships June 2014 avalerehealth.net Today s Panelists John Hackett - JHackett@extendicare.com o Vice President of Strategy & Development,
MCOs Revealed: Strategies for Building Strong Hospital & Referral Relationships June 2014 avalerehealth.net Today s Panelists John Hackett - JHackett@extendicare.com o Vice President of Strategy & Development,
8/28/2018. Presentation agenda CURRENT STATE OF THE POST ACUTE PROVIDER SECTOR. Impact of The Medical Director in Preserving Your Future
 Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Impact of The Medical Director in Preserving Your Future Rajeev Kumar MD FACP Chief Medical Officer Symbria Aaron Hagopian MBA Director of Data Analytics Symbria Copyright 2018 Symbria, Inc. Presentation
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations. April 26, 2018
 Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
Improving Care and Lowering Costs: The Use of Clinical Data by Medicaid Managed Care Organizations April 26, 2018 Agenda Welcome and Overview of Interview Results Claudia Ellison, Director of Programs,
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
NDNQI Rhythms in Quality 2010 Data Use Conference
 NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
NDNQI Rhythms in Quality 2010 Data Use Conference National Priority Partners Goals and Opportunities for Nurses Care Coordination Spotlight Gerri Lamb, PhD, RN, FAAN Arizona State University January 21-22,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement
 to Improve Functional Outcomes and Reduce Readmissions and Burden of Care. Opportunity Statement") Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
Creating a Virtual Continuing Care Hospital (CCH) to Improve Functional Outcomes and Reduce Readmissions and Burden of Care Robert D. Rondinelli, MD, PhD Paulette Niewczyk, MPH, PhD AlphaFIM, FIM, SigmaFIM,
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
Let s All Pull Together:
 Let s All Pull Together: Effective Partnering Across Quality Networks at the Community Level Sven Berg, MD Chief Medical Officer, West Virginia Medical Institute Keith T. Kanel, MD Chief Medical Officer,
Let s All Pull Together: Effective Partnering Across Quality Networks at the Community Level Sven Berg, MD Chief Medical Officer, West Virginia Medical Institute Keith T. Kanel, MD Chief Medical Officer,