REDUCING READMISSIONS
|
|
|
- Lesley Davis
- 6 years ago
- Views:
Transcription
1 REDUCING READMISSIONS Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015
2 Objectives What are hospitals with hospital-wide results doing? How does that differ from what we are doing? What are 3 practical ways to expand our strategies?
3 THANK YOU CMS 6 game-changing messages from CMS policies..
4 6 Very Important Messages from CMS 1. Readmission reduction pays at least inaction hurts 2. Hospitals must update & standardize transitional care processes 3. Reducing readmissions is a cross-continuum effort 4. Attend to non-clinical needs for post-hospital supports & services 5. We will flood the market with all best ideas on our dime 6. Reducing readmissions requires better data
5 HOWEVER. Powerful messages from powerful agencies can create blinders
6 CMS Focus Has Created Blinders 1. HF, AMI, PNA COPD, hip/knee replacement NOT the 5 most frequent diagnoses leading to readmissions CMS discharge diagnosis-specific penalty obscured other meaningful categorizations s/a frequent utilizer, social complexity, BH, functional status 2. Driven a Medicare focus to the exclusion of other high risk patient groups Medicaid adults have higher readmission rates than Medicare FFS 3. Driven a case-finding approach Interventions often focused on Medicare FFS with certain diagnosis Created a 2- tiered discharge process - at odds with principles of quality 4. Preferred first move among hospitals: hire new staff Lost the focus on redesigning transitional care for all patients Not engaging cross-setting providers/services as part of the solution
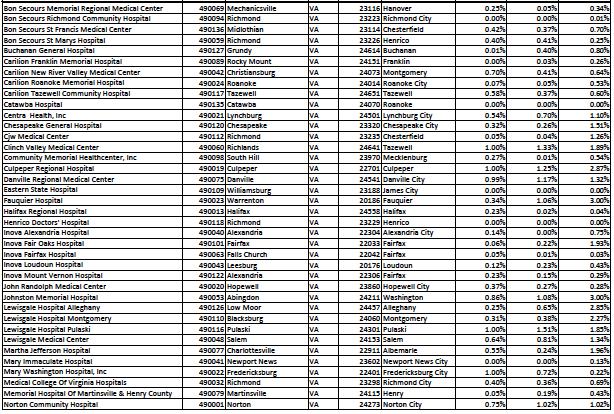
7 Medicare Readmission Penalties October September Up to 3% reduction in all Medicare payments for hospitals with high 30- day readmissions for AMI, HF, PNA, COPD and hip/knee replacement Average penalty DOUBLED this year 2,160 hospitals penalized; $480 MILLION In VA, 66 of 76 hospitals penalized = 86% 25 hospitals with >1% penalty this year 5 hospitals are subject to max (3%) penalty 10 hospitals have no penalty
8

9 Source: Kaiser Health News October 2014
10 CRUNCHING THE NUMBERS Will your current strategy get you to your goal?
11 Let s Run the Numbers: One Strategy Won t Get Us There Number Rate Medicare admits/year 5,000 admissions Medicare RA rate 20% # Medicare RA /year 1,000 readmissions Pilot project 200 high risk patients Pilot group RA rate 25% Expected # RA pilot 50 Expected effect of pilot 20% # RA reduced by pilot 10 # Medicare RA/year = = 990 1% Amy Boutwell 2014
12 Hospitals with hospital-wide results Know their data Analyze, trend, track, display, share, post Broad concept of readmission risk Way beyond case finding for diagnoses Multifaceted strategy Improve standard care, collaborate across settings, enhanced care Use technology to make this better, quicker, automated Automated notifications, implementation tracking, dashboards
13 EXPAND EFFORTS FOR IMPACT Broad concept of risk, broad understanding of patient needs
14 KNOW YOUR DATA Using data to dispel assumptions, expand opportunities for focus
15 Virginia Medicare FFS Readmissions Virginia Statewide % of Live Discharges Readmi?ed Within 30 Days 2011Q3-2014Q2 NaGonal State 20% 19% 18% 17% 18.79% 18.61% 18.49% 18.43% 18.42% 18.24% 18.57% 18.12% 18.05% 18.03% 18.44% 17.87% 18.28% 17.59% 17.77% 17.87% 17.88% 17.47% 17.49% 17.06% 17.96% 17.31% 16%

16 VA Pneumonia Readmissions by ZIP Source: VHA reports to hospitals
17 Top 10 Discharge Diagnoses Leading to Readmission in VA Virginia Top 10 Discharge Diagnoses Associated with Readmissions Q and Q Unspecified septicemia 1,592 Acute kidney failure, unspecified Pneumonia, organism unspecified Systolic heart failure (acute on chronic) Obstructive chronic bronchitis with (acute) exacerbation Diastolic heart failure (acute on chronic) Subendocardial infarction- initial episode of care Atrial fibrillation Urinary tract infection, site not specified Acute and chronic respiratory failure Sum of top 10 = 7,093 Top 10 diagnoses leading to RA: 7,093 Total number of Readmissions: 26,420 Top 10 diagnoses account for ~25% of all readmissions This is the opposite of the rule

18 Methods: - Used CCS groupers - Included OB Top 10 Medicare Dx: 1. CHF 2. Sepsis 3. Pneumonia 4. COPD 5. Arrythmia 6. UTI 7. Acute renal failure 8. AMI 9. Complication of device 10. Stroke Top 10 Medicaid Dx: 1. Mood disorder 2. Schizophrenia 3. Diabetes complications 4. Comp. of pregnancy 5. Alcohol-related 6. Early labor 7. CHF 8. Sepsis 9. COPD 10. Substance-use related
19


20 Pneumonia Readmissions, by Payer Source: VHA report to hospitals

21 % Medicare Patients that are Dually Eligible, by Zip Source: VHQC

22 % Medicare Patients Under 65, by Zip Source: VHQC
23 Readmissions by Days after Discharge Virginia Days UnGl Readmission Frequency Breakdown 2011Q3-2014Q ~25% <4 days ~50% <10 days Source: VHQC 23
")





24 Know your partners Social Network Analysis (SNA) Represents all transitions in community t i Red connectors represent provider pairs with high numbers of readmissions. The wider the connectors h the greater the number of shared transitions. Represents providers who share 30 or more h transitions 51 Represents providers who share 10 or more transitions Source: QIO data


25 VA Readmissions by Discharge Disposition Disposition # discharges # readmits RA rate % of all RA ALL 282,229 51, % 100% Home 135,345 22, % 43% Home Health 58,159 12,387 21% 24% *~50% PAC SNF 60,630 12,904 21% 25% Hospice 8, % 0.5% D/c to Home RA from Home D/c to Home Health RA from Home Health D/c to SNF RA from SNF Source: VHQC

26 Medicare v. Medicaid Discharge Disposition Measure Medicare Medicaid Discharge to Home 55% 84% Discharge to SNF/IRF/LTAC 24% 5% Discharge to Home with Home Health 14% 8% Other 7% 3%
27 County Hospital Readmission Stats Measure # % Total Discharges 11,850 Total Medicare Discharges 967 8% total Total (adult non-ob) Medicaid Discharges 4,288 36% total Total 30-day Readmissions 1,631 14% RA rate Total Medicare Readmissions 154, 9% total 16% RA rate Total (adult-non-ob) Medicaid Readmissions 823, 50% total 19% RA rate Medicaid RA are 35% higher than all-payer RA Medicaid RA account for 50% of ALL Readmissions
28 Medicaid High Utilizers - AHRQ >3 hospitalizations/year 85% are over age 21 Average ~6 hospitalizations/year v. 1.3 for non-high utilizers Average LOS 6.1 days v. 4.5 for non-high utilizers Average cost per hospitalization $11,600 v. $9,000 for non high-utilizers Readmission rate 52% v. 8% for non high-utilizers 74% of high utilizers are discharged to home Top Dx: mood disorders, schizophrenia, DM, chemo, sickle cell, ETOH, sepsis, CHF, COPD Jiang et al. HCUP Statistical Brief #184 Nov 2014
29 Readmission Analysis Use the most recent 12 months of data available. Using all hospital discharge data, exclude patients <18, all OB (DRG ), discharges dead, or transfers to another acute care hospital. Define a readmission as any return to inpatient status within 30-days of discharge from inpatient status. Measure Total Medicare Medicaid Private A. Total Discharges B. Total Readmissions C. Readmission Rate (B/A) D. Total Discharges to Home E. Total Discharges to SNF F. Total Discharges to Home Health Care G. Total Discharges with any coded Behavioral Health Diagnosis ( ) H. Total Readmissions with any coded Behavioral Health Diagnosis I. Number / % of readmissions occurring within 7 days of d/c J. Number of patients with 4 hospitalizations in past year K. Total number of discharges among [J] L. Total Number of 30-day readmissions among [J] M. Top 10 Discharge Diagnoses Resulting in Readmission, by Payer All Payer Medicare Medicaid N. Proportion of all readmissions represented by top 10 discharge diagnoses X% Y% Z%
30 ASK YOUR PATIENTS WHY Interview patients, caregivers for the story behind the chief complaint
31 Understand the story behind the chief complaint 61M with 8 hospitalizations this year for shortness of breath returns to the hospital 10 days after discharge with shortness of breath. 45F with HIV hospitalized for pneumonia discharged to home returns to the hospital 8 days later with pneumonia. 32M with uncontrolled DM, cognitive limitations, bipolar disorder, active substance use, homeless presents with flank pain to one hospital, readmitted with chest pain to another hospital Chart reviews and administrative analyses will NOT reveal what you need to know: you must talk to your patients, their families and caregivers, providers
32 Understand the story behind the chief complaint 77F recently hospitalized for an infected dialysis catheter returns to the hospital 8 days following discharge with shortness of breath. 86M with cancer hospitalized for constipation and abdominal pain returns to the hospital 1 day after discharge with abdominal pain. 61M with 8 hospitalizations this year for shortness of breath returns to the hospital 10 days after discharge with shortness of breath. 45F with HIV hospitalized for pneumonia discharged to home returns to the hospital 8 days later with pneumonia. 32M with every consequence of uncontrolled DM, released from prison, lives in the hospital: inpatient 105 of the past 160 days.
33 Root Cause of Chest Pain Admission: Shelter I need housing, not a shelter. I need someone to help make sure I take my medicines. In a shelter they don't do that and they kick you out every morning. I need a stable residence and no one is able to help with that." Acute Care Utilization over 180 days of freedom 15- Sep Prison Prison Prison Prison Prison Released 22- Sep ED DC 29- Sep 6- Oct ED ED IN IN 13- Oct IN IN DC 20- Oct ED DC 27- Oct IN ED DC ED 3- Nov IN IN IN IN IN DC/ED IN 10- Nov IN IN ED IN IN IN IN 17- Nov IN IN DC ED IN IN ED/DC 24- Nov IN ED ED ED IN 1- Dec ED IN DC ED 8- Dec IN IN IN IN IN IN IN 15- Dec IN IN DC 22- Dec 29- Dec 5- Jan ED ED IN DC ED 12- Jan ED 19- Jan ED IN IN IN IN DC ED 26- Jan DC ED ED IN 2- Feb IN IN IN IN IN IN IN 9- Feb IN IN IN IN IN IN IN 16- Feb IN IN IN DC IN IN IN ED (DC 23- Feb IN IN Brockton) IN? ED 2- Mar IN IN DC/ED IN 9- Mar DC ED DC ED IN IN IN 16- Mar IN IN
34 There is Never One Reason for Readmission.. KP team reviewed 523 readmissions across ~14 hospitals: 250 (47%) deemed potentially preventable Found an average of 9 factors contributed to each readmission Assessed factors related to 5 domains: 73% - care transitions planning & care coordination 80% - clinical care 49% - logistics of follow up care 41% - advanced care planning & end of life 28% - medications 250 readmissions identified 1,867 factors! Feingenbaum et al Medical Care 50(7): July 2012
35 Interviewed 60 patients who returned to ED after d/c from ED <9days Average age 43 (19-75) Majority had a PCP, but cited ED gave more tests, quicker answers, single site and ED more likely to treat the symptoms Most reported no problem filling medications 19//60 thought they didn t get prescribed the medications they needed (pain) 24/60 expressed concerns about clinical evaluation and diagnosis Primary reason for returning: fear and uncertainty about their condition Patients need more reassurance during and after episodes of care Patients need access to advice between visits Annals of Emergency Medicine
36 DESIGN A PORTFOLIO OF STRATEGIES There is no single bullet; we are engaged in system transformation

37 Develop A Multifaceted Portfolio of Efforts Improve hospital-based care processes for all patients, including ED Collaborate with cross-setting partners, including payers Provide enhanced services Use data, analytics, flags, workflow prompts, automation, dashboards to support continuous improvement, ensure reliability, drive to results

38 Develop Portfolio Strategy Improve hospital-based transitional care processes for ALL patients 1. Flag discharge <30d in chart 2. ED-based efforts to treat & return 3. Broaden view of readmission risks; assess whole-person needs 4. Develop transitional care plans that consider needs over 30 days 5. Ask patients & support persons why they returned, if readmitted 6. Ask patient & support persons what help they need; share with them their needs/risk assessment 7. Use teach-back, target the appropriate learner 8. Customize information 9. Arrange for post-hospital follow up 10. Use a check-list for all patients Collaborate with cross-setting partners 1. Use ADT notifications with medical and behavioral health providers 2. Ask community providers what they need and how they want to receive it 3. Collaborate to arrange timely follow up 4. Perform warm handoffs, and opportunity for clarification 5. Form a cross-continuum team that can access resources your staff are unaware of 6. Constantly refresh your awareness of social and behavioral health resources 7. Broaden partners to include Medicaid health plans and their care managers 8. Identify community partners with social work and behavioral health competencies Provide enhanced services for high risk 1. Segment high risk varying types of service & levels of intensity 2. Strategy for high utilizers 3. Strategy for navigating care 4. Strategy for accessing resources 5. Strategy for self-management 6. Strategy for frailty/medically complex 7. Strategy for end-of-life trajectory 8. Strategy for recurrent stable symptoms, etc individual care plans
39 Let s Run the Numbers: Three-part strategy Medicare admits/year Number 5,000 admissions Rate Medicare RA rate 20% # Medicare RA /year 1,000 readmissions 1. Improve standard care 5,000 admissions (20% RA rate) Expected effect 10% Expected # RA reduction 100 RA avoided 2. Collaborate with receivers 1650 admissions (1/3 total) (30% RA rate) Expected effect 20% Expected # RA reduction 3. Enhanced Service for Pilot 99 RA avoided 200 admissions (25% RA rate) Expected effect 20% Expected # RA reduction 10 RA avoided Total (*illustrative) 209 RA avoided* 209/1000 = 20% overall* Amy Boutwell 2013
40 46-study Meta-Analysis: What Works? Preventing 30-Day Hospital Readmissions A Systematic Review and Meta-analysis of Randomized Trials Leppin et al; JAMA Internal Medicine (online first) May Review of 42 published studies of discharge interventions Found that multi-faceted interventions were 1.4 times more effective Many components More people Support patient self-care Interventions published more recently had fewer components are were found to be less effective
41 2 HOSPITALS PORTFOLIO STRATEGIES Valley Baptist Medical Center, Harlingen TX Frederick Memorial Hospital, Frederick MD

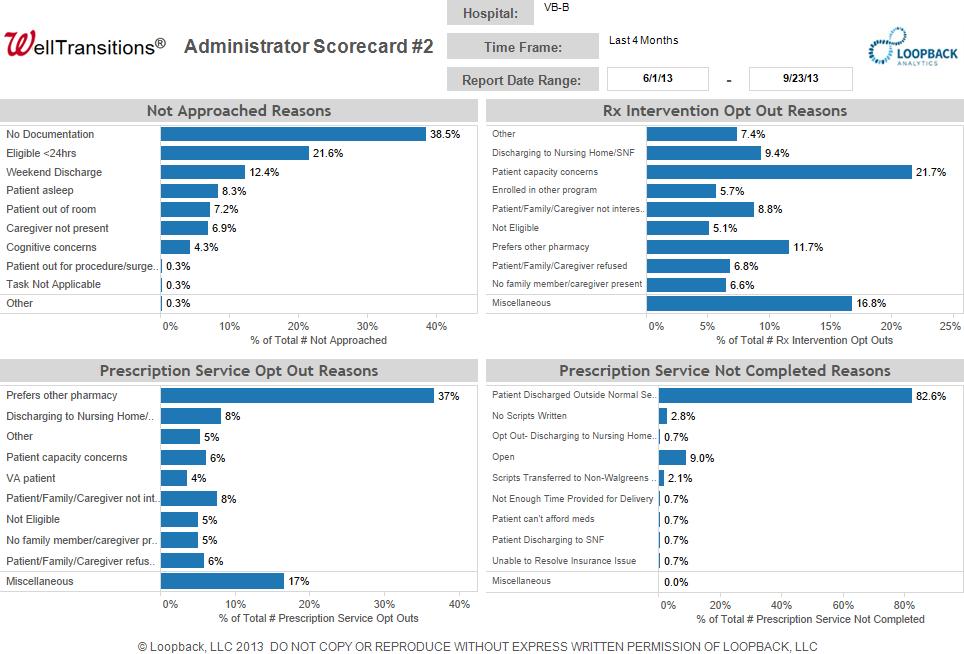
42 Valley Baptist Medical Center s Portfolio of Strategies Courtesy of Angela Blackford, VBMC

43 43


44 44
45 Valley Baptist Medical Center - Results All-cause readmissions Medicare Penalty FY 2011: 28% FY 2013: 21% 0.8% (of possible 1%) FY2014: 14% 0.2% (of possible 2%) FY 2014: 0.04% (of possible 3%) By the way, that s a 50% readmission reduction!!!
46 Frederick Memorial Hospital - Portfolio Improve Standard Hospital-based Processes ED-based SW/CM identify patients at point of entry CM screen for all patients move from 8B to behavioral interview Collaborate with Providers 25-member cross continuum team, meets monthly Track and trend H-SNF readmissions, review each, INTERACT Track and trend H-HH patients, weekly co-management virtual rounds (move up the continuum from HH to direct SNF if needed) Warm handoffs, points of contact with community BH provider Use off-site urgent care center for post-d/c appointments if needed Provide Enhanced Services to High Risk CM refer via order entry to Care Transitions Team Multi-disciplinary team works the case x 30+ days Cardiology NP Heart Bridge Clinic

47 Frederick Memorial Dashboard

48 Frederick Memorial Dashboard-2

49 SNF Readmissions, Frederick Memorial Courtesy of Heather Kirby
50 3-year results, Frederick Memorial All-payer all cause readmissions FY % FY 13 9% FY % That s a 28% reduction
51 Recommendations Know your data and your patients Adopt a broad concept of readmission risk Capture all reasons, whole-person approach Develop a multifaceted strategy Improve standard hospital-based care for ALL patients Start in ED Collaborate across settings with multi-sector partners Provide enhanced services Use technologies to make work better, quicker, automated
52 THANK YOU Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Lexington, Massachusetts
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
ASPIRE to Reduce Readmissions
 ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
ASPIRE to Knockout Pneumonia Readmissions Webinar #1. Amy Boutwell, MD, MPP March 1, 2018
 ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
NoCVA Preventing Avoidable Readmissions. Moving Beyond the Basics March 27, 2014
 NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement.
 Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia. Webinar #3 Post-Acute Care Readmissions September 8, 2016
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Readmissions Moving beyond blame to fill the patient needs. Jackie Conrad RN, MBA, RCC Cynosure Health
 Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
Community Health Needs Assessment Mercy Hospital Ardmore 2012
 Community Health Needs Assessment Mercy Hospital Ardmore 2012 Contents Table of Contents Introduction... 2 Description and Basic Community Demographics... 2 Who was Involved in Assessment?... 2 Community
Community Health Needs Assessment Mercy Hospital Ardmore 2012 Contents Table of Contents Introduction... 2 Description and Basic Community Demographics... 2 Who was Involved in Assessment?... 2 Community
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Balancing State, Federal and Internal Bundle Payment Initiatives
 Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
30-day Hospital Readmissions in Washington State
 30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Medicare Fee-For-Service (FFS) Hospital Readmissions: Q Q2 2014
 Hospital Readmissions: Q Q2 2014") Medicare Fee-For-Service (FFS) Hospital Readmissions: Q3 2013 Q2 2014 State of Florida Data Dictionary Provided on Page A Please contact Peggy Loesch via email at Peggy.Loesch@HCQIS.org or by phone at
Medicare Fee-For-Service (FFS) Hospital Readmissions: Q3 2013 Q2 2014 State of Florida Data Dictionary Provided on Page A Please contact Peggy Loesch via email at Peggy.Loesch@HCQIS.org or by phone at
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar. Thursday, December 13 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
The Camden Coalition of Healthcare. Management
 Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
Camden Coalition of Healthcare Providers Camden Coalition of Healthcare Providers The Camden Coalition of Healthcare Providers Approach to Risk Stratified Care Management Presentation by: Kennen S. Gross,
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Ambulatory-care-sensitive admission rates: A key metric in evaluating health plan medicalmanagement effectiveness
 Milliman Prepared by: Kathryn Fitch, RN, MEd Principal, Healthcare Management Consultant Kosuke Iwasaki, FIAJ, MAAA Consulting Actuary Ambulatory-care-sensitive admission rates: A key metric in evaluating
Milliman Prepared by: Kathryn Fitch, RN, MEd Principal, Healthcare Management Consultant Kosuke Iwasaki, FIAJ, MAAA Consulting Actuary Ambulatory-care-sensitive admission rates: A key metric in evaluating
William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs. Laura J. Dunlap, RN
 William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs Laura J. Dunlap, RN Background Research Questions Methods Results for North Carolina Results for Specific Counties
William B. Saunders, PhD, MPH Program Director, Health Informatics PSM & Certificate Programs Laura J. Dunlap, RN Background Research Questions Methods Results for North Carolina Results for Specific Counties
HCAHPS and Readmissions: Making the Connection Wednesday, September 18, :00 a.m. 10:00 a.m.
 HCAHPS and Readmissions: Making the Connection Wednesday, September 18, 2013 9:00 a.m. 10:00 a.m. Facilitated by: Katie McCullough, VHHA and Carla Thomas, VHQC Session Objectives: Understand the published
HCAHPS and Readmissions: Making the Connection Wednesday, September 18, 2013 9:00 a.m. 10:00 a.m. Facilitated by: Katie McCullough, VHHA and Carla Thomas, VHQC Session Objectives: Understand the published
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Financial Policy & Financial Reporting. Jay Andrews VP of Financial Policy
 Financial Policy & Financial Reporting Jay Andrews VP of Financial Policy 1 Members & Groups Supported Center for Healthcare Excellence Hospital Leadership & Quality Departments Hospital Finance Departments
Financial Policy & Financial Reporting Jay Andrews VP of Financial Policy 1 Members & Groups Supported Center for Healthcare Excellence Hospital Leadership & Quality Departments Hospital Finance Departments
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings
 Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
Outcomes for Iowa Medicaid Chronic Condition Health Home Program Enrollees. Policy Report. SFYs February 2017
 Policy Report February 2017 Outcomes for Iowa Medicaid Chronic Condition Health Home Program Enrollees Ss 2012-2015 Elizabeth Momany Assistant Director, Health Policy Research Program* Associate Research
Policy Report February 2017 Outcomes for Iowa Medicaid Chronic Condition Health Home Program Enrollees Ss 2012-2015 Elizabeth Momany Assistant Director, Health Policy Research Program* Associate Research
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Physician Performance Analytics: A Key to Cost Savings
 Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Saint Agnes Hospital. Pharmacist utilization of the LACE tool to prevent hospital readmissions. Program/Project Description, including Goals:
 Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Baseline and 9-Month Follow-Up Outcomes of Health Care for Iowa Medicaid Health Home Program Enrollees
 Health Policy 11-1-2013 Baseline and 9-Month Follow-Up Outcomes of Health Care for Iowa Medicaid Health Home Program Enrollees Elizabeth T. Momany University of Iowa Peter C. Damiano University of Iowa
Health Policy 11-1-2013 Baseline and 9-Month Follow-Up Outcomes of Health Care for Iowa Medicaid Health Home Program Enrollees Elizabeth T. Momany University of Iowa Peter C. Damiano University of Iowa
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
NASHP s 30 th Annual State Health Policy Conference. Timeline of Tennessee Health Care Innovation Initiative
 STATE OF TENNESSEE NASHP s 30 th Annual State Health Policy Conference 10/25/2017 Timeline of Tennessee Health Care Innovation Initiative 2012 2013 2014 2015 2016 2017 1210 Stakeholder Meetings 16 Partnerships
STATE OF TENNESSEE NASHP s 30 th Annual State Health Policy Conference 10/25/2017 Timeline of Tennessee Health Care Innovation Initiative 2012 2013 2014 2015 2016 2017 1210 Stakeholder Meetings 16 Partnerships
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Is It Really a UTI? Do You Know It When You See It?
 Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
Integrating Quality Into Your CDI Program: The Case for All-Payer Review
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
Health System Transformation. Discussion
 Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
Health System Transformation Patrick Conway, M.D., MSc CMS Chief Medical Officer Deputy Administrator for Innovation and Quality Director, Center for Medicare & Medicaid Innovation Director, Center for
STATISTICAL BRIEF #9. Hospitalizations among Males, Highlights. Introduction. Findings. June 2006
 HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #9 Agency for Healthcare Research and Quality June 2006 Hospitalizations among Males, 2003 C. Allison Russo, M.P.H. and Anne Elixhauser, Ph.D.
HEALTHCARE COST AND UTILIZATION PROJECT STATISTICAL BRIEF #9 Agency for Healthcare Research and Quality June 2006 Hospitalizations among Males, 2003 C. Allison Russo, M.P.H. and Anne Elixhauser, Ph.D.
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
MediServe. More than 25 Years Serving the Rehab and Respiratory Communities
 MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
MediServe More than 25 Years Serving the Rehab and Respiratory Communities Who We Are Respiratory Rehabilitation 250+ Clients Chandler, Arizona 26+ yrs of business CORE Focus (Compliance, Outcomes, Revenue,
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Care Coordination What Matters
 Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
OASIS ITEM ITEM INTENT
 (M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
(M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
Preventable Readmissions
 Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
Preventable Readmissions Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions Payment incentives Public reporting Quality
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 Medical Home Summit. Reducing Hospital. Innovative Model of Care
 2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Neighborhoods, resources and capacity to improve
 Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Innovative Coordinated Care Delivery
 Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2)
") Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD
 Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
Health Care Systems - A National Perspective Erica Preston-Roedder, MSPH PhD Outline Quality Overview Overview and discussion of CMS programs Increasing transparency Move from P4R to P4P Expanding beyond
SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT
 04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System