STRATEGIES TO REDUCE READMISSIONS
|
|
|
- Bonnie Blankenship
- 5 years ago
- Views:
Transcription
1 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person Transitional Care New York State Partnership for Patients HIIN Readmissions Launch Webinar January 25, 2017
2 Agenda The importance of effectively engaging patients and caregivers Who? Why? How? Resources
3 Objectives Being patient and caregiver-centered requires us to: Understand who is at risk of readmission Understand why patients return to the hospital Listen for all transitional care needs and readmission risks Be helpful: facilitate, advocate, connect
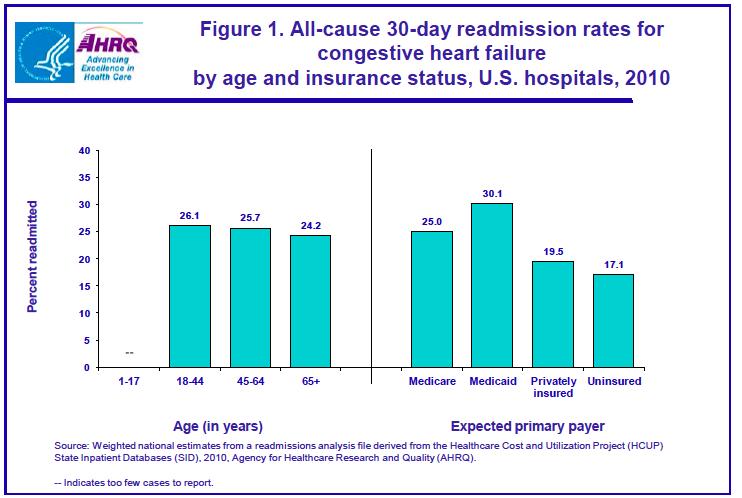
4 WHO Who is at risk of readmission?

5
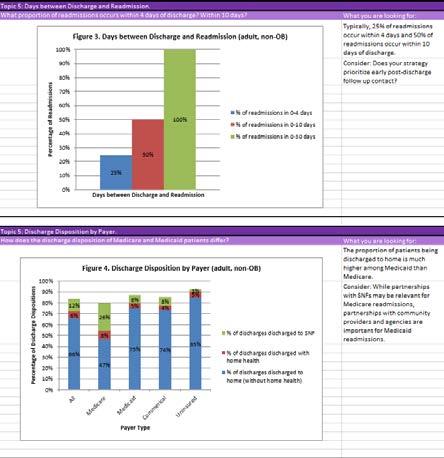
6 Discharge Disposition Source: Massachusetts Center for Health Information and Analysis Medicare (% discharges to) Medicaid (% discharges to) Discharge to Home 55% 84% Discharge to SNF/IRF/LTAC 24% 5% Discharge to Home with Home Health 14% 8%
7

8 Methods: - Used CCS groupers - Included OB Top 10 Medicaid Dx: 1. Mood disorder 2. Schizophrenia 3. Diabetes complications 4. Comp. of pregnancy 5. Alcohol-related 6. Early labor 7. CHF 8. Sepsis 9. COPD 10. Substance-use related Top 10 Medicare Dx: 1. CHF 2. Sepsis 3. Pneumonia 4. COPD 5. Arrythmia 6. UTI 7. Acute renal failure 8. AMI 9. Complication of device 10. Stroke

9 Readmission Rate: Any Behavioral Health Condition Massachusetts Center for Health Information and Analysis, 2016.

10 Readmissions for Patients with High Utilization 4+ hospitalizations/year Readmission rate 40% v. 8% 74% of discharged to home Top Discharge Diagnoses: Mood disorders Schizophrenia Diabetes Chemotherapy Sickle cell Alcohol Sepsis Heart Failure COPD Massachusetts Center for Health Information and Analysis, 2016 Jiang et al. HCUP Statistical Brief #184 Nov 2014
11 Ask your patients "Why" Elicit the personal/caregiver perspective; root causes
12 Take a "whole person" view of readmission risks, causes 41 woman with HIV; hospitalized for pneumonia, started on HIV medications and antibiotics and told to follow up with HIV and PCP providers. Readmitted 8 days later. 61 man with 8 hospitalizations this year for shortness of breath returns to the hospital after 10 days with shortness of breath. 86 man with recently diagnosed prostate cancer hospitalized initially for abdominal pain, readmitted 1 day after discharge for abdominal pain. Billing data aren t going to tell you whether a patient needed a pharmacy intervention, needed a place to live, or couldn t afford their medications.
13 41 woman with HIV hospitalized with pneumonia 1 st hospitalization: Longstanding HIV, never previously hospitalized Diagnosed with pneumonia, found to have high HIV viral load Lives with mother unaware of her HIV At discharge: Discharged on new anti-retroviral medications Discharged on new antibiotics for the pneumonia No infectious disease or primary care appointments made Readmission: Returned 8 days later for persistent coughing Returned because instructions said return if symptoms don t improve It would have helped if they made the appointment for me
14 61 man with 8 hospitalizations this year for SOB 1 st hospitalization: This really isn t his first hospitalization, is it? Intern H&P presents case as if new presentation to hospital Discover he is marginally housed Discover he has personality disorder issues Refuses to work with physical therapy At discharge: Patient can not be placed in facility due to a criminal history Discharged to home, told to follow up with PCP (hasn t been in > a year) Readmission: Reports he gained 20 lbs in 8 days Oh honey, it always takes them about a week to tune me up Grabs remote, turns on TV and orders dinner
15 86 man with prostate cancer and abdominal pain 1 st hospitalization Completed diagnosis and staging evaluation as outpatient Started on oxycodone as needed for pain Patient presented with constipation x 8 days Resolved in ED; admitted anyway At discharge Added bowel regimen Readmission Daughter in NJ dropped everything to rush to dad s side Saw him at home and asked if he had any pain; he said yes She brought him back to ED requesting admission to address pain Patient did not want to be readmitted, but did not want to argue with loving daughter
16 Do not over-medicalize root causes of readmissions Kaiser Permanente team reviewed 523 readmissions across ~14 hospitals: Found an average of 9 factors contributed to each readmission Philadelphia team interviewed patients who returned to ED after discharge: Average age 43 (19-75) Majority had a PCP; most reported no problem filling medications Found primary root cause for return: fear and uncertainty Patients need more reassurance during and after episodes of care Patients need access to advice between visits Feingenbaum et al Medical Care 50(7): July 2012 Rising et al, Annals of Emergency Medicine 2015
17 HOW? Adopt a data-informed, whole-person approach
18 What is a "Data-Informed" Approach?
19 Why Take A Data-Informed Approach? Many readmission reduction efforts have been launched in direct response to Medicare readmission penalties The discharge diagnoses in the penalty program are not the top reasons for readmissions in the Medicare population There are many high risk patients that go without improved transitional care when the focus is just on penalty conditions A data-informed approach is a more patient-centered approach
20 Data-Informed Approach Understand root causes of readmissions among your patients Design and implement readmission reduction efforts that are designed to address common root causes of readmissions Design and implement readmission reduction efforts that will effectively meet the transitional care needs of patients/caregivers Track implementation and outcome data to continuously improve processes to reach your goal A data-informed approach is responsive to root causes and is designed to better meet patient/caregiver transitional care needs
21 Why Take a "Whole-Person" Approach?
22 Whole-Person Approach Analyses highlight the multi-factorial causes of readmissions Patient interviews Root cause analysis Experience in the field has found success with transitional care models that address clinical, behavioral, and social needs Interdisciplinary, social work, social service models appear effective Several "clinical" approaches have been adapted to include social work, navigation, advocacy, resources to address basic needs
23 "Whole-Person" Adaptations to Transitional Care Navigating Hand-holding Arranging for. Providing with. Harm reduction Meet "where they are" Patient/caregiver priorities first Relationship-based
24 Whole-Person Approach Successful readmission reduction teams state: "We look at the whole person, the big picture" "We always address goals and ask what the patient wants" "We meet the patient where they are" "First and foremost it's about a trusting relationship" "You can't talk to someone about their medications if there is no food in the fridge" "We do whatever it takes"
25 Using Care Plans to Improve Care Over Time and Across Settings
26 Types of Care Plans: Observations from the Field Longitudinal Care Plan A comprehensive plan to achieve health-promoting goals and objectives. Specific goals regarding clinical, behavioral, and/or functional status are often included, and are measured via serial assessments over time. Longer term; care management over time. Transitional Care Plan Identifies post-hospital needs, patient priorities, and readmission risks and the plan to address those needs, priorities and mitigate risks in the 30 days post discharge. Focus on ensure linkage to providers and services within the 30 day transitional period. ED Care Plan Summary information for the ED provider to inform safe, effective, and consistent care in the ED and facilitate discharge with team-based follow up, as appropriate.
27 RESOURCES "Designing and Delivering Whole-Person Transitional Care: The AHRQ Hospital Guide to Reducing Medicaid Readmissions"

28 Introduction Table of Contents Why focus on Medicaid Readmissions? How to Use This Guide Analyze Your Data Survey Your Current Readmission Reduction Efforts Plan a Multi-Faceted Data-Informed Portfolio of Strategies Implement Whole-Person Transitional Care for All Reach Out to Collaborate With Cross- Continuum Providers Enhance Services for High-Risk Patients

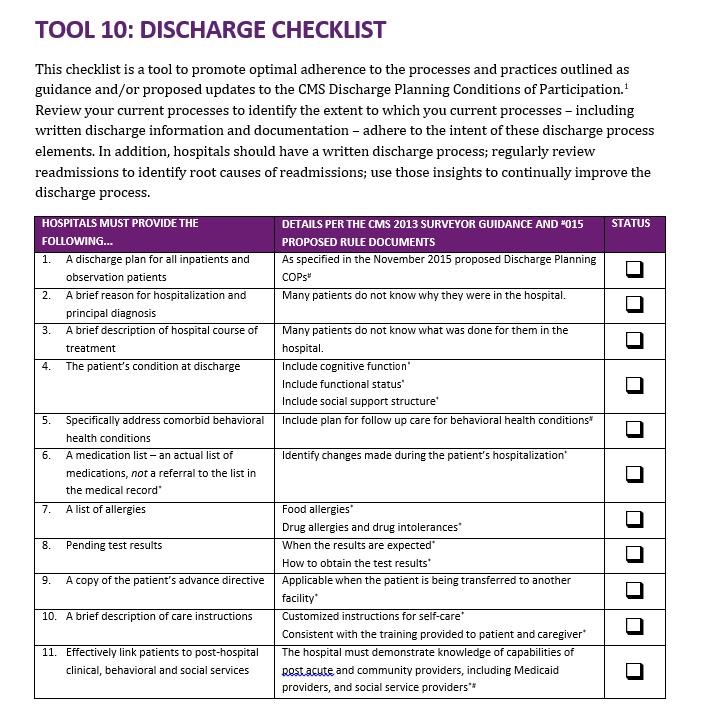
29 List of Tools The guide comes with 13 customizable tools to be used in hospital teams' day-to-day operations. 1. Data Analysis 2. Readmission Review 3. Hospital Inventory 4. Community Inventory 5. Portfolio Design 6. Operational Dashboard 7. Portfolio Presentation 8. Conditions of Participation Handout 9. Whole-Person Transitional Care Planning 10. Discharge Process Checklist 11. Community Resource Guide 12. Cross Continuum Collaboration 13. ED Care Plan Examples


30 Tool 1: Data Analysis Tool

31 Tool 2: Readmission Review Tool Purpose: To understand patient perspective To understand root causes To understand there are multiple factors To identify opportunities for improvement To develop a better plan for the patient To develop better services to offer Recommendation: Conduct at least 5 during planning Review all readmissions

32
33 Tool 9: Whole-Person Transitional Care Planning
34
35 THANK YOU FOR YOUR COMMITMENT TO REDUCING READMISSIONS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, AHRQ Reducing Medicaid Readmissions Project Expert Advisor, New York State DSRIP Super Utilizer Collaborative
ASPIRE to Reduce Readmissions
 ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
REDUCING READMISSIONS - 2015 Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February 13 2015 Objectives What are hospitals
NoCVA Preventing Avoidable Readmissions. Moving Beyond the Basics March 27, 2014
 NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
ASPIRE to Knockout Pneumonia Readmissions Webinar #1. Amy Boutwell, MD, MPP March 1, 2018
 ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement.
 Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia. Webinar #3 Post-Acute Care Readmissions September 8, 2016
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
Readmissions Moving beyond blame to fill the patient needs. Jackie Conrad RN, MBA, RCC Cynosure Health
 Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Coordinated Care: Key to Successful Outcomes
 Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
Coordinated Care: Key to Successful Outcomes Best practices in care coordination improve health, lower costs and increase patient satisfaction 402 Lippincott Drive Marlton, NJ 08053 856.782.3300 www.continuumhealth.net
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
30-day Hospital Readmissions in Washington State
 30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
Kentucky Stroke Transitions Assistance Resource
 Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
Kentucky Stroke Transitions Assistance Resource Patrick Kitzman, Ph.D., MSPT, Division of Physical Therapy, University of Kentucky Violet Sylvia, Ph.D., Director ARH System of Rehabilitation Services Kentucky
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
30-day Readmission Survey. Monica Thurston, OMS 2 Mary Herberger, OMS 2
 30-day Readmission Survey Monica Thurston, OMS 2 Mary Herberger, OMS 2 Meet Mary Herberger and Monica Thurston, OMS 2 COMP-NW Lebanon, OR Satellite Campus of Western University of Health Sciences in Pomona,
30-day Readmission Survey Monica Thurston, OMS 2 Mary Herberger, OMS 2 Meet Mary Herberger and Monica Thurston, OMS 2 COMP-NW Lebanon, OR Satellite Campus of Western University of Health Sciences in Pomona,
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Talking to Your Doctor About Hospice Care
 Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
Talking to Your Doctor About Hospice Care Death and dying subjects that were once taboo in our culture are becoming increasingly relevant as more Americans care for their aging parents and consider what
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings
 Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
When and How to Introduce Palliative Care
 When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Hospice Discharges. Legacy Hospice
 Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
Hospice Discharges Legacy Hospice Live Discharges Once a Medicare beneficiary elects the hospice benefit, hospice may not automatically or routinely d/c the beneficiary at it s discretion, even if the
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics
 Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Succeeding in the Post-Acute Market Strive for 5 Effective Communication with Physicians, Hospitals and Other Partners and Miscellaneous Other Topics Luis L Gonzalez, Jr, MD FACP FAAHPM CMD Objectives
Balancing State, Federal and Internal Bundle Payment Initiatives
 Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
HRET HIIN Readmissions Virtual Event. Fishbowl Event #5: The Fish Finale September 14, 2017
 HRET HIIN Readmissions Virtual Event Fishbowl Event #5: The Fish Finale September 14, 2017 1 Shereen Shojaat, MS Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Poll 1: How did you get here? How did
HRET HIIN Readmissions Virtual Event Fishbowl Event #5: The Fish Finale September 14, 2017 1 Shereen Shojaat, MS Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Poll 1: How did you get here? How did
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Providing Hospice Care in a SNF/NF or ICF/IID facility
 Providing Hospice Care in a SNF/NF or ICF/IID facility Education program Insert name of your hospice program Insert your logo Objectives Review the philosophy of hospice care and discuss what hospice care
Providing Hospice Care in a SNF/NF or ICF/IID facility Education program Insert name of your hospice program Insert your logo Objectives Review the philosophy of hospice care and discuss what hospice care
HealthPartners SNBC Inspire
 Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Patient and Family Caregiver Interview Tool
 Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
Patient and Family Caregiver Interview Tool Instructions: We recommend you select at least 5-10 patients who have been readmitted to your organization within the past 30 days to include in the group of
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014
 Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Care Coordination as a Team Sport. Sharon Quinlan MS, MBA, RN, NEA-BC November 3, 2017
 Care Coordination as a Team Sport Sharon Quinlan MS, MBA, RN, NEA-BC November 3, 2017 Objectives Explain critical elements of coordination and teamwork and their relationship to quality outcomes Describe
Care Coordination as a Team Sport Sharon Quinlan MS, MBA, RN, NEA-BC November 3, 2017 Objectives Explain critical elements of coordination and teamwork and their relationship to quality outcomes Describe
Quality Management (QM) Program AmeriHealth Pennsylvania
 Program AmeriHealth Pennsylvania") Quality Management (QM) Program AmeriHealth Pennsylvania Goals and Objectives The goals and objectives of the Quality Management (QM) Program are to promote the quality and safety of medical and behavioral
Quality Management (QM) Program AmeriHealth Pennsylvania Goals and Objectives The goals and objectives of the Quality Management (QM) Program are to promote the quality and safety of medical and behavioral
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
HH Compare. IMPACT Act. Measure HHVBP
 Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care
 Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
Creating Care Pathways Committees
 Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Presentation Creating Care Title Pathways Committees December 12, 2012 December 12, 2012 Creating Care Pathways Committees LeadingAge Indiana Integrated Care & Payment Executive Series 1 2012 Health Dimensions
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Community Health Needs Assessment Three Year Summary
 Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
Community Health Needs Assessment Three Year Summary 2013 2016 Community Health Needs Assessment Three Year Summary 2014 2016 Key needs were identified by community stakeholders which included the following:
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Navigating the Hospital Readmission Reduction Program
 Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Navigating the Hospital Readmission Reduction Program Since the Affordable Care Act passed in 200, a hospital s 30-day readmission rate has become synonymous with quality of care. Beginning in 202, the
Home Health. Improving Patient Outcomes & Reducing Readmissions. Home Health: Improving Outcomes & Reducing Readmissions
 Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
Home Health Improving Patient Outcomes & Reducing Readmissions Home Health: Improving Outcomes & Reducing Readmissions Benefits of Home Health Care Scientific evidence proves people heal more quickly,
July 2, 2010 Hospital Compare: New ED and Outpatient. Information; Annual Update to Readmission and Mortality Rates
 July 2, 2010 Hospital Compare: New ED and Outpatient Information; Annual Update to Readmission and Mortality Rates AT A GLANCE The Issue: In early July, information on care provided in the hospital outpatient
July 2, 2010 Hospital Compare: New ED and Outpatient Information; Annual Update to Readmission and Mortality Rates AT A GLANCE The Issue: In early July, information on care provided in the hospital outpatient
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Factors that Impact Readmission for Medicare and Medicaid HMO Inpatients
 The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
The College at Brockport: State University of New York Digital Commons @Brockport Senior Honors Theses Master's Theses and Honors Projects 5-2014 Factors that Impact Readmission for Medicare and Medicaid
Community Health Needs Assessment Mercy Hospital Ardmore 2012
 Community Health Needs Assessment Mercy Hospital Ardmore 2012 Contents Table of Contents Introduction... 2 Description and Basic Community Demographics... 2 Who was Involved in Assessment?... 2 Community
Community Health Needs Assessment Mercy Hospital Ardmore 2012 Contents Table of Contents Introduction... 2 Description and Basic Community Demographics... 2 Who was Involved in Assessment?... 2 Community
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Stage 2 GP longitudinal placement learning outcomes
 Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
Faculty of Life Sciences and Medicine Department of Primary Care & Public Health Sciences Stage 2 GP longitudinal placement learning outcomes Description This block focuses on how people and their health
RETHINKING CARE PROGRAM SPOTLIGHT
 RETHINKING CARE PROGRAM SPOTLIGHT Improving Medicaid Care Management for People with Serious Mental Illness in Pennsylvania A bout four years ago, Shervene, a 43-year-old grandmother of two, was diagnosed
RETHINKING CARE PROGRAM SPOTLIGHT Improving Medicaid Care Management for People with Serious Mental Illness in Pennsylvania A bout four years ago, Shervene, a 43-year-old grandmother of two, was diagnosed
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network. Monday, September 12, 2011
 Care Coordination and the Role of the Aging Network. Monday, September 12, 2011") National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
National Coalition on Care Coordination (N3C) Care Coordination and the Role of the Aging Network Monday, September 12, 2011 Washington, DC Hyatt Regency on Capitol Hill Yellowstone/Everglades 4:00 PM
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Policy & Providers. for Managing Chronic Care Patients. Mary Alexander Strategic Alliances Director - Home Instead, Inc. Kelly Funk.
 Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Policy & Providers Lessons From The Health Care Arena for Managing Chronic Care Patients Producer: Bob Bua President - CareScout Panel: Peter Sosnow VP Corporate Development - Humana / SeniorBridge Mary
Care Transitions: From Hospital to Home
 Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Care Transitions: From Hospital to Home Michael Halling & Care Transitions Team TRANSITION PROGAM PURPOSE Assist patients/clients as they transition from the acute care setting back to their homes Improve
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill
 Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Improving Care and Managing Costs: Team-Based Care for the Chronically Ill Cathy Schoen Senior Vice President The Commonwealth Fund www.commonwealthfund.org cs@cmwf.org High Cost Beneficiaries: What Can
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans
 Training Presentation for Managed Medical Assistance Specialty Plans") Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
04/08/2015. Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists. Pharmacist Objectives. Technician Objectives
 1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
1 2 Thinking Beyond the Hospital Walls: Readmission Reduction Strategies for Pharmacists Stacey Zorska, Pharm.D., MHA Director of Pharmacy Services Southwest General Middleburg Heights, OH Pharmacist Objectives
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN
 TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
TCPI Tools for Population Management: Guide to Preventing Readmissions among Racially and Ethnically Diverse Medicare Beneficiaries Hosted by HCDI SAN This webinar is provided free-of-charge and is supported
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Care Coordination for Special Populations
 Care Coordination for Special Populations Joy Twesigye, MS, MPP, WHNP-BC Associate Director, Programs and Professional Services June 4, 2013 NASBHC Offerings Advocacy Policies Programs Funding Training
Care Coordination for Special Populations Joy Twesigye, MS, MPP, WHNP-BC Associate Director, Programs and Professional Services June 4, 2013 NASBHC Offerings Advocacy Policies Programs Funding Training
HRET HIIN Reducing Sepsis Readmissions Virtual Event. Fishbowl Event #2 May 8, 2018
 HRET HIIN Reducing Sepsis Readmissions Virtual Event Fishbowl Event #2 May 8, 2018 1 Radhika Parekh, MHA Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
HRET HIIN Reducing Sepsis Readmissions Virtual Event Fishbowl Event #2 May 8, 2018 1 Radhika Parekh, MHA Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
CareTrek : Nebraska s Journey to Safe Care Transitions
 CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
CareTrek : Nebraska s Journey to Safe Care Transitions Audrey Paulman, MD, MMM Principal Clinical Coordinator CIMRO of Nebraska This material was prepared by CIMRO of Nebraska, the Medicare Quality Improvement
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015
 MODEL OF CARE TRAINING 2015") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.