Medical Council of New Zealand
|
|
|
- Brenda Austin
- 6 years ago
- Views:
Transcription
 which will record and track skills and knowledge acquired by new doctors during their first two years of medical practice Page")
1 Level 2, Customs House Whitmore Street PO box Wellington Phone: Medical Council of New Zealand REQUEST FOR PROPOSAL A national IT system (an e-portfolio) which will record and track skills and knowledge acquired by new doctors during their first two years of medical practice Page 1
2 Glossary Clinical attachment Clinical Supervisor Intern NZCF PGY1 PGY2 Prevocational Educational Supervisor Prevocational medical training Trainee Intern (TI) PDP CPD MSF Medsys A MCNZ accredited 13 week rotation worked by an intern A vocationally registered senior medical officer supervising an intern on a clinical attachment A doctor in their first or second year of postgraduate training after graduating from medical school New Zealand Curriculum Framework for Prevocational Medical Training Post graduate year 1 following graduation medical school Post graduate year 2 following graduation from medical school A Council appointed vocationally registered doctor who has oversight of the overall educational experience of a group of PGY1 and/or PGY2 doctors The two years following graduation from medical school A medical student in the final year of medical school Professional development plan Continuing professional development Mulitsource feedback MCNZ registration database Page 2
3 Table of contents 1.0 Statement of work Purpose The Council Background Key elements of the e-portfolio Elements which make up the e-portfolio Information flow between elements Key processes Scope of work High level requirements Device support Stored data requirements Access to the system and data Reporting Data security and Disaster Recovery/BCP Compliance with legislation Delivery model General Information Original RFP Document Non-commitment of MCNZ Confidentiality Conflict of interest Schedule of events RFP updates Correspondence/clarifications The Council s responses Proposer enquiries Proposal Preparation Instructions Proposer s understanding of the RFP Good Faith Statement Contract not guaranteed Proposal Submission Criteria for Selection Selection and Notification Page 3
4 1.0 Statement of work 1.1 Purpose The purpose of this request for proposal (RFP) is to invite prospective providers to submit a proposal to supply a system (an e-portfolio) which will record and track skills and knowledge acquired by new doctors during their first two years of medical practice. The Medical Council of New Zealand (the Council) plans to support the delivery of Prevocational Medical Training for doctors in New Zealand by implementing an e-portfolio which will ensure that the skills and knowledge acquired during PGY1 and PGY2 are recorded and tracked consistently for each intern in New Zealand. The system must be simple and not onerous. The system will support the continuum of lifelong learning which begins in medical school and continues for the duration of a doctor s career. While this proposal is for a system relating to the first two years of training after graduation, the system needs to be able to import/export information from other systems used by for example medical schools and medical colleges. The system will act as a central repository for an intern to record their learning, reducing the reliance on a paper based system. It will ensure interns can monitor their progress in meeting the learning outcomes in the New Zealand Curriculum Framework for Prevocational Medical Training (NZCF) and will assist those involved in assessment of learning through providing a wide range of information to inform discussions about a doctor s performance. 1.2 The Council The Council is the regulatory authority for doctors in New Zealand established and governed by the Health Practitioners Competence Assurance Act 2003 (HPCAA). The primary purpose of the Council is to protect the health and safety of members of the public by providing for mechanisms to ensure that doctors are competent and fit to practise their profession. Council has the following key functions (see Appendix 1 for section 118 of the HPCAA): registering doctors setting standards and guidelines accreditation of recertification processes and the promotion of lifelong learning for doctors reviewing practising doctors if there is a concern about performance, professional conduct or health accreditation of New Zealand and Australian medical schools and post graduate training programmes. 1.3 Background Prevocational medical training spans the two years following graduation from medical school and includes both postgraduate year 1 (PGY1) and postgraduate year 2 (PGY2). Page 4
5 Council commenced a review of prevocational training in late 2010, focusing on the issues relating to education and training of doctors. The review was undertaken by the Council with support from Health Workforce New Zealand (HWNZ). An initial (Stage 1) consultation process commenced in May 2011 and in February 2013 the consultation paper A review of prevocational training requirements for doctors in New Zealand: Stage 2 was released to stakeholders. At its meeting on 10 July 2013 Council made a number of decisions about changes to prevocational training and each of these is described in detail, along with the reasons for Council s decisions in the Report on the feedback and decisions following the consultation of: A review of prevocational training requirements for doctors in New Zealand: Stage 2. Council has approved the New Zealand Curriculum Framework for Prevocational Medical Training (NZCF) which outlines the learning outcomes an intern must have substantively attained by the end of PGY1 and PGY2. These outcomes are to be achieved through a mix of clinical attachments, educational programmes and individual learning, in order to promote safe quality healthcare. The NZCF builds on the prior learning, experience, competencies, attitudes and behaviours acquired during medical school, particularly the Trainee Intern (TI) year (the year prior to commencing prevocational training). A framework for assessment had been developed which will: nurture a culture of learning, focusing on improvement over the course of the year ensure defined skills are attained at a defined level identify and assist those who are under performing at an early stage provide a natural fit with workplace learning and preparation for lifelong CPD ensure that learning is tailored to identify individual learning needs. The framework for assessment aims to: Improve the learning experience for all interns ensuring consistency and quality of training, with a focus on assessment for learning rather than assessment of learning. Improve the mechanisms for interns to receive high quality feedback on their performance with a focus on ongoing improvement over the course of the year. Council resolved to implement a record of learning maintained in an e-portfolio, to create a nationally consistent means of tracking an intern s progress and recording skills and knowledge acquired during the intern years (PGY1 and PGY2). The e-portfolio would be owned by the intern with access granted to the Prevocational Educational Supervisor and Clinical Supervisor so they can guide the intern s learning. The e-portfolio is expected to be implemented in November 2014; it will aid the transition of the doctor along the continuum of learning, capture overall learning and help to identify future learning needs. It should also decrease the bureaucratic burden for both interns and supervisors. Page 5
6 2.0 Key elements of the e-portfolio There are multiple elements which make up the e-portfolio. Information on these elements, how they are linked, and how the information in one element is used to populate other elements listed in this section. 2.1 Elements which make up the e-portfolio New Zealand Curriculum Framework for Prevocational Training (NZCF) - Appendix 2 The NZCF is a list of learning outcomes which an intern must substantively attain during PGY1 and PGY2, taking into consideration prior learning from the TI year. The latest version of the NZCF can be downloaded from Council s website at: Professional Development Plan (PDP) data The PDP is a short planning document compiled by the intern in collaboration with their Prevocational Educational Supervisor with input from their Clinical Supervisor. The PDP records goals focused on what an intern wants to learn, needs to learn and needs to consolidate and looks at how these might be met. It will help an intern to structure and focus learning, strengthen existing skills, and develop new ones. High level goals will be created at the start of each post graduate year in collaboration with the Prevocational Educational Supervisor. The PDP will also be updated at the start of each new clinical attachment (quarterly) with the Clinical Supervisor to allow specific goals and objectives for the clinical attachment to be created related to the learning outcomes which can be attained on that particular clinical attachment. The PDP is revisited mid-attachment and at the end of the attachment. At any given time, an intern s PDP will show what learning outcomes need to be achieved. There needs to be provision for the Clinical Supervisor and Prevocational Educational Supervisor to view the information in the PDP and make comments. An intern needs to be able to create goals as well as record their progress in meeting them Skills Log The Skills Log is a record of all the learning outcomes which an intern has achieved against the full list of learning outcomes in the NZCF. Interns can record prior learning acquired during medical school, particularly during the Trainee Intern (TI) year. As learning outcomes are attained, they should be recorded in the Skills Log, adding to the record of the intern s learning. The intern will regularly update this list as they achieve the learning outcomes in the NZCF. Page 6
7 An intern s Prevocational Educational Supervisor and Clinical Supervisor should review the Skills Log each time they meet with the intern to inform their conversations which will help to ensure that the intern has been objective in updating their log Clinical attachments A clinical attachment is a 13 week rotation worked by an intern in a particular field of medicine. Each clinical attachment must be accredited by MCNZ to ensure it provides a quality learning experience and opportunities to attain the learning outcomes in the NZCF. Training providers will identify the learning outcomes from the NZCF which can generally be attained on the clinical attachment (this process will not be complete until November 2015). Knowing what learning outcomes are associated with each clinical attachment will assist training providers in assigning an intern four clinical attachments which will provide them with the opportunity to substantively attain the learning outcomes in the NZCF. The Clinical Supervisor for each clinical attachment will need to be able to view this information so they know which learning outcomes can be achieved and which have already been achieved on their clinical attachment. Knowing which learning outcomes have not been achieved either on a particular attachment or on a combination of attachments will assist the Prevocational Educational Supervisor and Clinical Supervisor in targeting learning to address any gaps, which can be recorded as goals in the PDP Learning Modules/Continued Professional Development (CPD) activities Interns will achieve some of the learning outcomes listed in the NZCF through attending training organised by their training provider (learning modules) or through CPD activities. The e-portfolio should have the ability for interns to include evidence of attendance, course overviews, and when they were completed. It must also record completion of educational activities such as certification in Advanced Cardiac Life Support (ACLS) Supervision reports At the end of each clinical attachment the Clinical Supervisor will electronically complete an End of clinical attachment supervision report (Appendix 3) for each intern they have supervised. An electronic process will enable the Clinical Supervisor to create a record of the complete supervision report including a rating of the intern s overall performance on that clinical attachment and the intern and Prevocational Educational Supervisor s comments and signoff. The supervision form should not be able to be deleted or modified by the intern. A paper version of the form to be used for PGY1 is attached as Appendix 3. A similar form will be used for PGY2. While the form is electronic, an option to print is required (max 3 pages) Multisource feedback Multisource feedback is feedback collected from the intern s colleagues and patients around the intern s communication and professionalism using a set questionnaire. Although the collection of multisource feedback is not being implemented until November 2015, the e- portfolio will need to be ready to store this information. It is likely that this feedback will be stored in the form of a report summarising the multisource feedback. The Prevocational Page 7
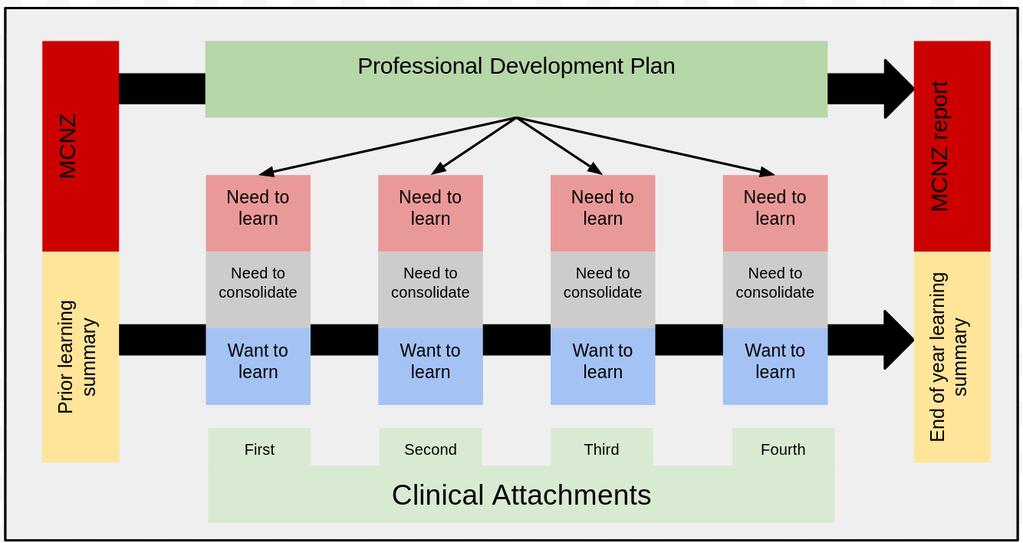
8 Educational Supervisor would receive the report and discuss the results in a face-to-face meeting before a record of the report can be stored in the intern s e-portfolio Community based experience An intern must complete one clinical attachment in a community based setting during PGY1 or PGY2. When training providers submit a clinical attachment for accreditation, they will be asked to identify whether the clinical attachment provides community based experience. The e- portfolio must be able to record that a clinical attachment includes community based experience so it can easily be checked whether an intern has met this requirement by looking at which clinical attachments they have completed Personal notes There should be somewhere an intern can record personal notes and reflections about their learning experience and career plan which by default, will not be visible to the Clinical Supervisor or Prevocational Educational Supervisor, but can be shared with them at the discretion of the intern. 2.2 Information flow between elements The following diagram illustrates how the learning outcomes detailed in the NZCF, except those which have been gained through prior learning, inform goal setting in each intern s PDP. During each clinical attachment, CPD activities, learning modules, supervision reports and multisource feedback inform which learning outcomes have been met during the clinical attachment, and which learning outcomes still need to be met. Learning outcomes which have been met are recorded in the Skills Log by the intern, and learning outcomes which still need to be met should remain visible. After the last clinical attachment has been completed, the Skills Log then becomes the learning summary (or record of learning) for the intern for that year Basic diagram of information flow between elements Page 8

9 Page 9
10 3.0 Key processes The process from an intern beginning PGY1 through to completing PGY2 is described in Appendix Scope of work 4.1 High level requirements A system which meets our requirements will be able to do the following: Requirement Allow online access for all stakeholders who need to access the system Allow public access to specified content including the NZCF, framework for assessment, and information on accreditation standards and the process for accreditation Allow access from all commonly used electronic devices including desktop personal computers, laptops and mobile devices like tablets and smart phones running commonly used operating systems Allow interns to access their information offline and make changes which can be updated to their online information later. Priority Required Required Required Desirable Store profile information about the intern. Required Generate and store a Professional Development Plan (PDP) for each intern. The PDP is live and is regularly reviewed and updated by the intern, Prevocational Educational Supervisor and Clinical Supervisors Store a Skills Log for each intern. This Skills Log will track each intern s progress in meeting the learning outcomes identified in the NZCF Store a record of Continued Professional Development (CPD) activities completed by each intern Allow supervision reports to be completed for an intern following each clinical attachment by the Clinical Supervisor for that attachment. The intern and Prevocational Educational Supervisor should have the ability to sign off the completed form and include comments. Required Required Required Required Store the details of the NZCF in a format which will allow Required Page 10
11 the information to be publically available online, and also be used as a basis for the Skills Log and the PDP to assist in setting goals. The details also need to be able to be modified by approved users as they change over time Store the details of accredited clinical attachments. The details need to be able to be modified by approved users as they change over time Allow the creation and subsequent modification of reports based on the information stored in the system. Reports should be able to be secured to allow access only by specific people or groups Secure all information stored, especially any retained login information and personal information about interns in accordance with accepted industry best practice Allow users to update and reset passwords in line with accepted best practice including security questions which can be selected by the user. Required Required Required Required Comply with all relevant legislation. Required Incorporate industry standard business continuity and disaster recovery processes and procedures ensuring that no data is lost, and the system is available at all times (see 4.6) Store the outcomes from multisource feedback (MSF) for each intern. MSF is not being implemented until November 2015, but the system will need to be ready to be able to accommodate this requirement Allow training providers to assign accredited clinical attachments to interns who are recorded as being employed by them Allow for a particular combination of accredited clinical attachments to be tested to ensure that a particular set of four clinical attachments incorporate a sufficient number of the learning outcomes listed in the NZCF Allow for different users of the system to be able to access only the information they are permitted to see. See section 4.4 for further information Allow functionality to survey interns for feedback relating to prevocational training when required. Required Required Required Required Required Required Page 11
12 4.2 Device support The system should be able to be accessed via different types of devices with different operating systems and browsers including, but not limited to: Computer running Windows operating systems including XP, Vista, 7 and 8 or Mac OS operating systems. Tablets running ios, Android and Windows Mobile. 4.3 Stored data requirements Intern profile data The following minimum data needs to be able to be recorded for each intern: Data Details Name First, middle and last name of the intern. This also needs to allow for changes to the name and record previous names where appropriate MCNZ number Include the doctor s registration number Date of birth The intern s date of birth Qualifications Sourced from an underlying code table of available qualifications, including information about the primary medical qualification such as name, year, and issuing organisation Gender Male/Female Employments Where the intern is employed to work. The available values for this will come from a set list of accredited training providers. Employments will change over time, so each employment will have an associated start date and end date and history Clinical attachments Information about each clinical attachment will be available, for example approved supervisor/s, name of training institution or hospital, and area of medicine. The learning outcomes available in each accredited clinical attachment or combination of four clinical attachments will be stored and available, to assist in allocating a mix of four clinical attachments. Information on which clinical attachments the intern is undertaking, and which clinical attachments the intern has completed. The available values for this will come from a set list of approved clinical attachments. Clinical attachments Page 12
13 will have an associated start date and end date to record the period over which the attachment was completed Prevocational Educational Supervisor Name of Prevocational Educational Supervisor from an approved list Professional Development Plan (PDP) data The PDP is where the intern records their goals and tracks their progress in achieving them. See section for more information. The following minimum data needs to be able to be recorded as part of a PDP for an intern: Data Details Goals Details of goals set in collaboration with the Prevocational Educational Supervisor and Clinical Supervisor. This will require a number of fields for example date created, goal title, goal description, how it will be achieved, timeframes and status How identified Drop down list to indicate how the goal was identified what I want to learn, what I need to learn, identified area for improvement from supervision report Learning outcomes The learning outcomes which can be met through achieving the goal. Intern can select from a list of learning outcomes which are available on the current clinical attachment. Once completed the list could update the skills log Comments Interns, Prevocational Educational Supervisors and Clinical Supervisors can add comments against each goal Summary view A way to filter the goals by their status, when they were created, when they were attained, how they were identified etc Skills Log data The Skills Log is made up of all of the learning outcomes listed in the NZCF which an intern is expected to substantially complete by the end of PGY2. The intern will regularly update the list as they achieve outcomes. Additionally, the intern can record which skills have been acquired through prior learning. Page 13
14 Clinical and Prevocational Educational Supervisors will review the log to ensure interns have been objective in updating their lists. The following data needs to be able to be recorded as part of a Skills Log for an intern: Data Details Date Date learning outcome achieved How achieved Method of identifying whether the learning outcomes has been achieved through prior learning, on a specific attachment or through a learning module etc. An ability to filter the Skills Log to view for example learning outcomes achieved by prior learning, learning outcomes not achieved, learning outcomes achieved on a particular attachment would be useful Continuing Professional Development (CPD) data Require the ability to upload files for example certificates and records of achievement or attendance for CPD activities in a PDF format. The following data needs to be able to be recorded for any CPD activities (including uploaded records in PDF) or learning modules the intern completes: Data Details Name Name of the learning module or activity Provider Name of the organisation which organised the learning module or activity (if applicable) Date Date on which the learning module or activity occurred Supervision report At the end of a clinical attachment the Clinical Supervisor and intern meet and an electronic supervision form is completed (See Appendix 3). The Clinical Supervisor completes a summative assessment of the intern s performance and the intern and Prevocational Educational Supervisor include comments and sign-off. Where an intern s performance is deemed to be unsatisfactory a remediation plan is put in place. Ability for the system to electronically remind the relevant parties when they need to complete their section is required. 4.4 Access to the system and data There will be a number of stakeholders requiring access to the system and the levels and duration of access will be different. Page 14
15 Intern Require indefinite access to their e-portfolio. Training provider Prevocational Educational Supervisor Require access to the full e-portfolios of the interns they are supervising for the period of supervision and a defined period after. The period of supervision is usually 1or 2 years. Clinical Supervisor Require access to the full e-portfolio of those they are supervising on the individual clinical attachment, excluding the personal notes section, for the period of supervision and a defined period after. The period of supervision is usually 3 months at a time. Other groups/individuals Within the training institution there will be different groups of people for example CMO or delegate, advisory panel and RMO units who need access to the e-portfolio or data from the e-portfolio of interns undertaking prevocational training at their organisation. The duration and levels of access may differ between the groups. This information is to be determined. Medical Council of New Zealand (Council) The Council will not necessarily wish to access individual e-portfolios but would need to be able to load information into the system, such as the training providers, clinical attachments as they become accredited, and updated NZCF following the 3 year review. The Council will also run various reports using the data available. 4.5 Reporting Interns, the Council, HWNZ, and other stakeholders will need to be able to access the information stored in the system. To meet this need, the system will need to allow the creation and subsequent modification of a wide variety of reports drawing on all of the data stored Details of initial reports required Some examples of reports which are needed are detailed in the table below. As mentioned, our requirements for reports will change over time, and so we will need the ability to add to these, as well as to modify existing reports as needed. Report Details Skills not yet achieved This report will list the skills in an intern s Skills Log which are still to be achieved, informing the intern of areas where they need to focus their learning in the future Advisory panel Summary of learning report for each intern Accredited clinical attachments Report of all accredited attachments, including information about approved supervisors, learning outcomes available, and training provider. Page 15
16 Interns Status of all interns completing PGY1 and PGY2 and information about completed clinical attachments Evaluation A wide range of reports will need to be run using all of the data over a number of years to inform the evaluation programme which will measure the outcomes of the changes to prevocational training against the objectives. 4.6 Data security and Disaster Recovery/BCP The provider needs to ensure that all data stored in the system is secured in line with current best practice for web applications. Please provide details of how data stored in the system will be protected to help us best evaluate your proposal. The vendor must also provide an appropriate business continuity and disaster recovery plan for the system. Council is interested in comparing the relative costs of different levels of continuity and recovery. Vendors should indicate if they are able to provide the different levels of continuity and recovery in the table below, as well as what the relative costs would be for each level (both up-front costs and any ongoing costs), and as much as possible, how that particular level would be achieved. Return time objective (RTO) Return point objective (RPO) Level 1 72 hours - 1 week Level hours Level 3 Less than 8 hours Level 4 0 minutes Last full backup - less than 1 week Last backup - less than 24 hours Last backup - less than 15 minutes before the event 0 minutes One fixed requirement is that the business continuity and disaster recovery plan must include backup to tape or other media, and these backups must be stored in a different geographic location from the system. If any data stored in the system would be stored outside of New Zealand, this should be noted in the proposal. 4.7 Compliance with legislation Legislation the e-portfolio will need to comply with will include: 1. Health Practitioners Competence Assurance Act Privacy Act Health Information Privacy Code 1994; and 4. Any other relevant legalisation or New Zealand law. 4.8 Delivery model The Council is not committed to any particular delivery model, and is interested in exploring all possibilities in order to ensure the cost-effective delivery of the system. Possible models range from full MCNZ ownership where Council owns and manages the system, to a fully Page 16
17 outsourced delivery model where the supplier manages the system, to models which fall somewhere in between. Where proposers are including multiple delivery options, the different costs of each option must be clearly and separately identified. Capital costs and revenue costs must be clearly and separately identified. 5.0 General Information 5.1 Original RFP Document The Council shall retain the RFP, and all related terms and conditions, exhibits and other attachments, in original form in an archival copy. Any modification of these, in the proposer s submission, is grounds for immediate disqualification. 5.2 Non-commitment of MCNZ All proposers are advised that the Council is not committed to any course of action as a result of issuing this RFP and/or receiving a response from the proposers in respect of it. In particular, it should be noted by proposers responding to the RFP that Council may: reject any information which does not conform to instructions as specified within the RFP not accept responses or variations after the final submission date cancel, amend or withdraw all or part of this RFP at any time. Proposers shall also note that Council is not obliged to pay for any information or other preparation work required in connection with this RFP. 5.3 Confidentiality The provider s staff, in developing and in managing or supporting the system, may see private, sensitive or confidential information that is patient or practice related or that is the property of the Council. The provider will be required to agree to keep all such information, whether written, electronic or oral, strictly confidential. The requirement for confidentiality shall apply equally to any sub-contractor used by the provider. Providers or their agents shall not, without prior written consent from Council, make any public statements in relation to this RFP, or subsequent short-listing, contract negotiation or the awarding of a contract. 5.4 Conflict of interest The provider must comply with the Council s conflict of interest policy and must advise the Council of any conflicts of interest (Appendix 5). Page 17
18 5.5 Schedule of events The following is a tentative schedule that will apply to this RFP, but may change in accordance with the Council s needs or unforeseen circumstances. Changes will be communicated by to all invited proposers: Issuance of RFP 29 April 2014 Expressions of interest 13 May 2014 Technical Questions/Enquiries Due 13 May 2014 RFP Closes 28 May 2014 Complete Initial Evaluation of proposals 13 June 2014 Presentations by selected proposers 27 June 2014 Final Award Notification 31 July 2014 Following award notification there would be three stages to implementation: 1. developing the detailed requirements (may include workshops) 2. finalising the solution 3. assisting with implementation. 5.6 RFP updates If during the RFP process the Council decides to provide further clarification, all proposers will receive formal notification. If the due date is extended for a proposer, the same extension will be offered to all proposers. The due date will not be extended once the due date is less than 7 calendar days away. 5.7 Correspondence/clarifications No verbal communication will be entered in to with regards to this RFP. All communication must be in writing ( is acceptable). Communications between the Council and the provider shall include, but are not limited to: Information or comments shared between the Council and the proposer. Questions concerning this RFP (these must be submitted in writing and be received prior to 13 May 2014 Errors and omissions in this RFP and enhancements. Proposers may identify to the Council any discrepancies, errors, or omissions that may exist within this RFP. With respect to this RFP, proposers may request to the Council any enhancements, which the Council will consider. These must be submitted in writing and be received prior to 13 May Enquiries about technical interpretations must be submitted in writing and be received prior to 13 May Verbal and/or written presentations. Negotiations under this RFP. Council s response. Page 18
19 5.8 The Council s responses The Council will make a good-faith effort to provide a written response to each question or request for clarification within five business days. All questions and answers will be shared with all prospective proposers who have logged an expression of interest. It is Council's intention that these will be issued simultaneously to all participants and will, upon issue, be deemed to become part of the RFP. The Council will not respond to any questions or requests for clarification if received by the Council after 13 May If a prospective proposer is unable to obtain clarification on any matter relating to the requirements of this RFP, they should indicate where it believes the RFP to be ambiguous or unclear in any way and should describe the interpretation it has adopted in preparing its proposal. 5.9 Proposer enquiries Enquiries, questions, and requests for clarification related to this RFP are to be directed in writing to: Medical Council of New Zealand PO Box Manners Street Wellington 6142 Attention: Andrea Flynn, Project Coordinator aflynn@mcnz.org.nz 6.0 Proposal Preparation Instructions 6.1 Proposer s understanding of the RFP In responding to this RFP, the proposer accepts full responsibility to understand the RFP in its entirety, and in detail, including making any enquiries to the Council as necessary to gain such understanding. 6.2 Good Faith Statement All information provided by the Council in this RFP is offered in good faith. Individual items are subject to change at any time. The Council is not responsible or liable for any use of the information or for any claims asserted. 6.3 Contract not guaranteed Council reserves the right not to enter into any contract, to add and/or delete elements, or to change any element of the coverage and participation at any time during the RFP process without prior notification and without any liability or obligation of any kind or amount. Page 19
20 6.4 Proposal Submission The proposer will provide three A4 copies (one of which is to be unbound and single sided) and an electronic copy (on CD or USB device) of their response and any supporting documentation by the RFP deadline to Joan Crawford (address provided below): Proposals must be delivered sealed to: Joan Crawford Strategic Programme Manager Medical Council of New Zealand PO Box 11649, Manners Street Wellington 6142 on or prior to 28 May The Council shall not accept proposals received by fax or Criteria for Selection The evaluation of each proposal will be based on its demonstrated competence, compliance, format, and organisation. The purpose of this RFP is to identify those suppliers that have the interest, capability, and financial strength to supply the Council with the system defined in the scope of work (section 4) Evaluation Criteria: The following criteria organised according to priority will be assessed in evaluating proposals: 1. Capability of supplier to meet or exceed requirements set forth in Scope of Work. 2. Technical design proposed. 3. Future sustainability of the capability of the proposer, and any proposed subcontractors, to meet or exceed the requirements of the Scope of Work. 4. Proposed cost. 5. Track record of other successful implementation of similar services. 6. Expressed interest in working with the Medical Council of New Zealand. Please respond to every point under Scope of Work (section 4). The following codes are suggested for suppliers to use in indicating the extent to which their proposal addresses each point under Scope of Work (section 4). Page 20
21 (Y) Yes (C) Customisation (D) Development (N) No Fully conforms, as at the proposal closing date Some customisation (by the proposer) is required (supply an explanation) Currently under Development (supply expected delivery date) Does not conform Further explanatory text is invited for all questions Presentation Council may invite proposers to present to an evaluation panel following the RFP close date; the presentation would be followed by a question and answer session. 6.6 Selection and Notification Suppliers which are determined by the Council to possess the capacity to satisfy all criteria in this RFP will be selected to move into the negotiation phase of this process. Written notification will be sent to these proposers by mail. Those suppliers not selected for the negotiation phase will also be notified by mail. Page 21
22 Appendix 1 Health Practitioners Competence Assurance Act 2003 Section Functions of authorities The functions of each authority appointed in respect of a health profession are as follows: o (a) to prescribe the qualifications required for scopes of practice within the profession, and, for that purpose, to accredit and monitor educational institutions and degrees, courses of studies, or programmes: o (b) to authorise the registration of health practitioners under this Act, and to maintain registers: o (c) to consider applications for annual practising certificates: o (d) to review and promote the competence of health practitioners: o (e) to recognise, accredit, and set programmes to ensure the ongoing competence of health practitioners: o (f) to receive and act on information from health practitioners, employers, and the Health and Disability Commissioner about the competence of health practitioners: o (g) to notify employers, the Accident Compensation Corporation, the Director-General of Health, and the Health and Disability Commissioner that the practice of a health practitioner may pose a risk of harm to the public: o (h) to consider the cases of health practitioners who may be unable to perform the functions required for the practice of the profession: o i) to set standards of clinical competence, cultural competence, and ethical conduct to be observed by health practitioners of the profession: o (j) to liaise with other authorities appointed under this Act about matters of common interest: o (k) to promote education and training in the profession: o (l) to promote public awareness of the responsibilities of the authority: o (m) to exercise and perform any other functions, powers, and duties that are conferred or imposed on it by or under this Act or any other enactment. Page 22

23 New Zealand Curriculum Framework for Prevocational Medical Training Version 1.0, Released February 2014 PROFESSIONALISM COMMUNICATION CLINICAL MANAGEMENT CLINICAL PROBLEMS AND CONDITIONS PROCEDURES AND INTERVENTIONS To navigate this document: This document contains a series of links to make it simple and easy to navigate. All links are underlined. The links above take you to an overview of the content of each of the five sections of this curriculum framework. From the overview page you can view the learning outcomes associated with a particular heading by clicking on the heading. To go back to the section overview from the list of learning outcomes click on any of the headings underlined on the page. Comments or requests for further information about the New Zealand Curriculum Framework for Prevocational Medical Training should be ed to prevocationalfeedback@mcnz.org.nz. Introduction Prevocational medical training spans the 2 years following graduation from medical school and includes both postgraduate year 1 (PGY1) and postgraduate year 2 (PGY2). The New Zealand Curriculum Framework for Prevocational Medical Training (NZCF) outlines the learning outcomes to be substantively completed in PGY1 and by the end of PGY2. These outcomes are to be achieved through clinical attachments, educational programmes and individual learning, in order to promote safe quality healthcare. The NZCF builds on the prior learning, experience, competencies, attitudes and behaviours acquired during medical school, particularly the trainee intern (TI) year. A mix of clinical attachments, and other educational support, over PGY1 and PGY2 will ensure a breadth of exposure and opportunity to achieve the learning outcomes. It is important to note: that assessment will be on the job and multi facetted the record of learning will allow an intern to track their own progress against the NZCF that at the beginning of PGY1 interns will be able to identify and take into account learning from the prior years assessment will be based on a high level of trust that assumes that nearly all interns will exceed the minimum levels of competence. PURPOSE STRUCTURE ACKNOWLEDGEMENTS 1 Page 23
24 Purpose The NZCF aims to: build on undergraduate education by guiding recently graduated doctors to develop and consolidate the attributes needed for professionalism, communication and patient care guide generic training that ensures PGY1 and PGY2 doctors develop and demonstrate a range of essential interpersonal and clinical skills for managing patients with both acute and long-term conditions, regardless of the specialty guide the seeking of opportunities to develop leadership, team working and supervisory skills in order to deliver care in the setting of a contemporary multidisciplinary team and to begin to make independent clinical decisions with appropriate support guide decisions on career choice. Learning outcomes The NZCF should be used to guide a doctor s continuum of learning from medical school through to PGY1 and PGY2. It outlines the desired learning outcomes; however it is recognised that proficiency in achievement of the capabilities will occur at different stages in training. At the end of PGY1, doctors should have gained the necessary competencies to gain registration in a general scope of practice. During PGY2, doctors should continue their learning to ensure they are competent to enter vocational training or to work in independent practice in a collegial relationship with a senior doctor at the end of PGY2. When commencing new clinical attachments, the NZCF provides an essential guide for discussing and identifying the learning opportunities that are available from a given attachment. It will help to identify particular opportunities that may be taken during the attachment in order to assist learning. The learning outcomes in the NZCF are underpinned by two central concepts: 1. Patient safety Patient safety must be at the centre of healthcare and depends on both individual practice and also effective multidisciplinary team work. 2. Personal development Throughout their careers, doctors must strive to improve their performance to ensure their progression from competent through proficient to expert practitioner, with the aspiration always to provide the highest possible quality of healthcare. PGY1 and PGY2 doctors are expected to develop critical thinking and professional judgement, especially where there is clinical uncertainty. PGY1 and PGY2 doctors should regularly reflect on what they perform well and which aspects of performance could be improved in order to develop their skills, understanding and clinical acumen. PGY1 and PGY2 doctors are expected to be proactive in managing their continuing education and career development. PGY1 and PGY2 doctors must work closely with their supervisors and multidisciplinary team to ensure maximum benefit from the learning opportunities that are available in the prevocational years. Who should use the NZCF The NZCF will be used by PGY1 and PGY2 doctors, prevocational educators, supervisors, employers, and others responsible for high quality patient care. 2 Page 24
25 Structure The NZCF is split into five sections. Professionalism Doctor and society Professional behaviour Teaching, learning and supervision Communication Patient interaction Working in teams Managing information Clinical management Safe patient care Patient assessment Emergencies Patient management Clinical problems and conditions Procedures and interventions The learning outcomes within each of the sections are broken into: a list of core competencies a doctor must substantively attain by the end of PGY1 competencies that a doctor should develop and consolidate by the end of PGY2. Competencies should be extended with the acquisition of new skills including those relevant to future vocational training. Acknowledgements The Medical Council of New Zealand (Council) would like to acknowledge the Confederation of Postgraduate Medical Education Councils (CPMEC) for allowing us to use the Australian Curriculum Framework for Junior Doctors (ACF) as a basis for the New Zealand Curriculum Framework for Prevocational Medical Training (NZCF). Council would also like to thank all those who have contributed to developing the NZCF: Prof John Nacey, MCNZ Education Committee Chair and CPMEC Board member Dr Ken Clark, Chair of National DHB, Chief Medical Officer Group Prof Pete Ellis, MCNZ Education Committee member and Deputy Chair of MedSac Dr Jonathan Foo, New Zealand Medical Association, Doctors in Training Council Dr Oliver Hansby, former MCNZ Education Committee member Dr Alex Lee, MCNZ Education Committee member Dr Lyndy Matthews, Chair of Council of Medical Colleges Dr Heidi Mayer, RNZCGP Prof Phillippa Poole, Chair of Prevocational Training Committee, Northern Regional Training Hub Dr John Thwaites, Intern Supervisor, Canterbury DHB Prof Tim Wilkinson, Associate Dean (Medical Education), University of Otago Dr John Adams, former Chair of MCNZ Mr Philip Pigou, Chief Executive, MCNZ Ms Joan Crawford, Strategic Programme Manager, MCNZ 3 Page 25
26 Professionalism Doctors should be able to provide safe treatment to patients by practising medicine in a professional manner. The following outcome statements apply to all aspects of professionalism. PGY1 By the end of PGY1, doctors are able to practise medicine in a professional manner, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. PGY2 By the end of PGY2 the core professional skills identified for PGY1 should be developed and consolidated. In addition, competencies should be extended with the acquisition of new skills including those relevant to future vocational training. DOCTORS AND SOCIETY PROFESSIONAL BEHAVIOUR TEACHING LEARNING AND SUPERVISION Access to healthcare Cultural competence Health promotion Health and work Healthcare resources Māori patients and their whānau Medicine and the law Pacific patients and their families Professional standards Doctors as leaders Ethical practice Personal well-being Professional development Practitioner in difficulty Professional responsibility Time management Assessment and feedback Self-directed learning Supervision Teaching 4 Page 26
27 Communication Doctors should be able to provide safe treatment to patients through effective communication. The following outcome statements apply to all aspects of communication. PGY1 By the end of PGY1 doctors are able to identify and practise effective communication, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. PGY2 By the end of PGY2 the core communication skills identified for PGY1 should be developed and consolidated. In addition, competencies should be extended with the acquisition of new skills including those relevant to future vocational training. PATIENT INTERACTION WORKING IN TEAMS MANAGING INFORMATION Breaking bad news Complaints Context Meetings with families and whānau, or carers Open disclosure Providing information Respect Communication in healthcare teams Team structure Working in health care teams Electronic Health records Written 5 Page 27
28 Clinical Management Doctors should be able to provide safe treatment to patients by delivering appropriate clinical management. The following outcome statements apply to all aspects of clinical management. PGY1 By the end of PGY1 doctors are able to demonstrate the following clinical management skills, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. PGY2 During PGY2 the ability to recognise and demonstrate important aspects of clinical management as provided for in PGY1 should be developed and consolidated. In addition, competencies should be extended, and new clinical management skills acquired, including those relevant to future vocational training. SAFE PATIENT CARE PATIENT ASSESSMENT EMERGENCIES PATIENT MANAGEMENT Adverse events and near misses Infection control Medication safety Public health Radiation safety Risk and prevention of error and/or harm Evidence-based practice History and examination Investigations Patient identification Problem formulation Referral and consultation Advanced cardiac life support Assessment Basic life support Prioritisation Disasters Return to work, ambulatory and community care Discharge planning/transfer of care End-of-life care Fluid, electrolyte and blood product management Management options Systems Pain management Therapeutics 6 Page 28
29 Clinical problems and conditions Doctors should be able to adequately identify common or important conditions through history taking, eliciting the relevant signs at examination and investigations. They should then formulate a differential diagnosis and establish and monitor an initial management plan. PGY1 By the end of PGY1 doctors are able to recognise and manage core clinical problems and conditions, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. PGY2 Doctors should have acquired greater knowledge and broader clinical skills to manage all of the clinical problems and conditions listed for PGY1. Doctors should also have extended the range of clinical problems and conditions they are able to manage including those relevant to future vocational training. General Endocrine Immunology Obstetric Abnormal investigation results Eyes (ophthalmology) Infectious diseases Oncological emergency Circulatory Gastrointestinal Musculoskeletal Oral disease Dermatological Genito urinary Nephrology Pharmacology/toxicology Domestic violence Gynaecological Neurological Psychiatric/drug and alcohol Ear, nose and throat Haemopoietic Nutrition/metabolic Respiratory 7 Page 29
30 Procedures and interventions Doctors should be able to provide safe treatment to patients by competently performing certain procedural and assessment skills. The following outcome statements apply to all procedures and interventions. Decision-making Informed consent Preparation Procedures Post-procedure Prescribing PGY1 By the end of PGY1 doctors are able to perform the following procedures and interventions, while recognising the limits of their personal capabilities. They should also be able to recognise complex or uncertain situations and seek advice appropriately. Cardiopulmonary Injections Ophthalmic Trauma Diagnostic Intravenous/intravascular Respiratory Urogenital Ear, nose and throat Mental health Surgical Women s health PGY2 By the end of PGY2 the core procedural skills and interventions identified for PGY1 should be developed and consolidated. In addition, competencies should be extended with the acquisition of new skills including those relevant to future vocational training. 8 Page 30
31 Professionalism Doctors should be able to provide safe treatment to patients by practising medicine in a professional manner. The following outcome statements apply to all aspects of professionalism. PGY1 By the end of PGY1 doctors are able to practise medicine in a professional manner, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. DOCTOR AND SOCIETY Access to healthcare Demonstrate a non-discriminatory approach to patient care Facilitate access to culturally appropriate healthcare Identify how access to and use of healthcare is influenced by the patient s ethnicity and education Identify how physical or cognitive disability can limit patients access to and use of healthcare services Cultural competence Demonstrate an awareness of the general beliefs, values, behaviours and health practices of particular cultural groups most often encountered, and demonstrate knowledge of how this can be applied in the clinical situation Demonstrate an awareness of the limitations of their knowledge and an openness to ongoing learning and development in partnership with patients Demonstrate an awareness that cultural factors influence health and illness, including disease prevalence and response to treatment Demonstrate respect for patients and an understanding of their cultural beliefs, values and practices Develop a rapport and communicate effectively with patients of other cultures Identify the cultural issues that might impact on the doctor-patient relationship Recognise their own cultural values and the influence these may have on their interactions with patients Seek appropriate cultural advice Work with the patient s cultural beliefs, values and practices in developing a relevant management plan Health promotion Advocate for healthy lifestyles and discuss environmental and lifestyle risks to patient health Distinguish the positive and negative aspects of health screening and prevention when making healthcare decisions Use a non-judgemental approach to patients lifestyle choices, for example, discuss options, offer choices Health and work Describe the key relationship between employment status and health status and be able to help formulate a safe plan to either stay at work or return to work Promote the use of work as a part of safe treatment and rehabilitation 9 Page 31
32 Healthcare resources Identify the impact of resource constraint on patient care Use healthcare resources wisely to achieve the best outcomes Māori patients and their whānau Ask patients about their ethnic background Assist patients to understand their condition and treatment plan Demonstrate a willingness to develop a rapport with Māori patients Demonstrate an awareness of the general beliefs, values, behaviours and health practices of Māori, and demonstrate knowledge of how this can be applied in the clinical situation Involve whānau when a patient brings them to a consultation Seek appropriate cultural advice Show awareness of the health disparities that exist in Māori communities and their origins Medicine and the law Complete required medico-legal documentation appropriately Comply with the legal requirements in patient care, for example Mental Health Act 1992, Privacy Act 1993, death certification, coronial legislation Comply with the Code of Health and Disability Services Consumers' Rights 1996 Liaise with legal and statutory authorities, including mandatory reporting where applicable Pacific patients and their families Demonstrate an awareness of the general beliefs, values, behaviours and health practices of Pacific peoples, and demonstrate knowledge of how this can be applied in the clinical situation Show awareness of the family-based decision-making that may apply Show awareness of the health disparities that exist in Pacific communities Professional standards Adhere to professional standards and professional codes of conduct Comply with the legal requirements of being a doctor, for example, maintaining registration Maintain professional boundaries Respect patient privacy and confidentiality PROFESSIONAL BEHAVIOUR Doctors as leaders Commit to improving the performance of others and the system in which they work Exhibit the qualities of a good leader and take the leadership role when required Show an ability to work well with and lead others 10 Page 32
33 Ethical practice Accept responsibility for ethical decisions Behave in ways that acknowledge the ethical complexity of practice and follow professional and ethical codes Consult colleagues about ethical concerns Show integrity, honesty and moral reasoning Personal well being Balance availability to others with care for personal health, managing fatigue, stress and illness Behave in ways that mitigate the potential risk to others from own health status, for example infection Have their own GP Show awareness of and optimise personal health and well being Professional development Demonstrate a commitment to improving performance Participate in a variety of continuing education opportunities Practitioner in difficulty Identify the support services available Recognise the signs of a colleague in difficulty Refer appropriately and respond with empathy Professional responsibility Act as a role model of professional behaviour both within the workplace and outside including the appropriate use of social media Demonstrate accountability for their practice Demonstrate reliability and fulfil obligations Demonstrate respectful and effective interactions with others in the health system Maintain an appropriate standard of professional practice and work within personal capabilities Reflect on and learn from personal experiences, actions and decision-making Time management Demonstrate punctuality Prioritise workload to maximise patient outcomes and health service functions TEACHING, LEARNING AND SUPERVISION Assessment and feedback Participate in feedback and assessment processes 11 Page 33
34 Provide constructive, timely and specific feedback based on observation of performance Seek and respond to feedback Self-directed learning Commit to continuous improvement of performance through lifelong learning Take opportunities to participate in research where appropriate Establish and use current evidence-based resources to support learning Identify and address personal learning objectives Participate in clinical audit Participate in quality improvement activities Seek opportunities to reflect on and learn from clinical practice Supervision Adapt level of supervision to the learner s performance and confidence Commit to developing skills to become an effective supervisor Provide effective supervision, for example, by being available, offering an orientation, learning opportunities and by being a role model Teaching Commit to helping other health professionals learn Incorporate teaching into clinical work Use approaches that are responsive to the learning needs of others PGY2 By the end of PGY2, the core professional skills identified for PGY1 should be developed and consolidated. In addition, competencies should be extended with the acquisition of new skills including those relevant to future vocational training. Examples include: Exhibit the qualities of a good leader and take the leadership role when required New Zealand Triple Aim for quality improvement: Improved quality, safety and experience of care Improved health and equity for all populations Best value for public health system resources Participate in formalised educational opportunities in relation to professionalism and ethics Participate in quality improvement Participate in research 12 Page 34
35 Communication Doctors should be able to provide safe treatment to patients through effective communication. The following outcome statements apply to all aspects of communication. PGY1 By the end of PGY1 doctors, are able to identify and practise effective communication, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. PATIENT INTERACTION Breaking bad news Participate in breaking potentially distressing news to patients and carers Recognise and manage potentially distressing communications with patients and carers Show empathy and compassion Complaints Identify factors likely to lead to complaints and act appropriately to minimise the risk of complaints Use local protocols to respond to complaints, including notifying more senior staff Context Arrange an appropriate environment for communication, for example, private, no interruptions Use effective strategies to deal with difficult situations or vulnerable patients Use principles of good communication to ensure effective healthcare relationships Meetings with families and whānau or carers Ensure relevant family/whānau/carers are included appropriately in meetings and decision-making Identify the impact of family dynamics on effective communication Respect the role of families/whānau in patient healthcare Open disclosure Explain and participate in implementing the principles of open disclosure Help ensure patients and carers are supported and cared for after an adverse event Providing information Apply the principles of good communication (verbal and non-verbal) and communicate with patients and carers in ways they understand Involve patients in discussions and decisions about their care 13 Page 35
36 Use interpreters for non-english speaking backgrounds or communication impairments, when appropriate Respect Ask patients about their preferences and be willing to follow their lead Build rapport and demonstrate empathy and compassion Demonstrate politeness, courtesy and patience Maintain privacy and confidentiality Provide clear and honest information to patients and respect their treatment choices Treat patients courteously and respectfully, showing awareness and sensitivity to different backgrounds WORKING IN TEAMS Communication in healthcare teams Communicate effectively with team members in a variety of situations, including acute settings, team meetings, ward rounds, telephone consultations Concisely present cases to senior medical staff and other healthcare professionals in a range of contexts Engage patients and carers in the team decision-making process where possible Perform effective written and verbal handover at different stages of medical care for patient safety and continuity of care (for example, team member to team member, service to service, hospital to general practice) Team structure Adopt an appropriate role within a healthcare team Recognise and understand the role and functions of a range of healthcare teams and team members, including teams that extend outside the hospital Recognise, understand and respect the roles and responsibilities of multidisciplinary team members Understand the characteristics of effective teams, leaders and team members Working in healthcare teams Contribute to teamwork by behaving in ways that maximise the team s effectiveness Demonstrate an ability to work with others Demonstrate flexibility and ability to adapt to change Lead when appropriate Seek to prevent or resolve conflicts that may arise MANAGING INFORMATION Electronic Comply with policies regarding information technology, for example, passwords, and internet Use electronic patient records to optimise patient care where available 14 Page 36
37 Use electronic resources appropriately in patient care, for example decision support systems, electronic access to results, completion of discharge summaries, and referencing pharmacopoeia Health records Comply with legal/institutional requirements for health records Facilitate appropriate coding and classification by accurate documentation Written Accurately document drug prescription and administration Comply with organisational policies regarding timely and accurate documentation Demonstrate high quality written skills in all clinical communications (writes legible, concise and informative discharge summaries) PGY2 By the end of PGY2, the core communication skills identified for PGY1 should be developed and consolidated. In addition, competencies should be extended with the acquisition of new skills including those relevant to future vocational training. Examples include: Undertake formalised communication courses that are offered by medical colleges Clinical management Doctors should be able to provide safe treatment to patients by delivering appropriate clinical management. The following outcome statements apply to all aspects of clinical management. PGY1 By the end of PGY1, doctors are able to demonstrate the following clinical management skills, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. SAFE PATIENT CARE Adverse events and near misses Document and report adverse events in accordance with local incident reporting systems Manage adverse events and near misses Recognise harm caused by adverse events and near misses 15 Page 37
38 Infection control Practise correct hand-hygiene and aseptic techniques Use antibiotics appropriately and rationally with consideration given to cost implications and appropriate prescribing guidelines Use methods to minimise transmission of infection between patients Medication safety Document patient allergies in every case Identify the medications most commonly involved in prescribing and administration errors Prescribe and administer medications safely Provide adverse drug reaction reporting Routinely report medication errors and near misses in accordance with local requirements Public health Inform authorities of each case of a 'notifiable disease' Recognise which diseases are notifiable Radiation safety Minimise the risk to patient or self associated with exposure to radiological investigations or procedures Request appropriate radiological investigations and procedures Risk and prevention of error and / or harm Explain and report potential risks to patients and staff Minimise risk and identify the main sources of error to prevent harm where possible Recognise and act on personal factors that may contribute to patient and staff risk Systems Advocate for the improvement of systems Identify and understand concept of system errors Participate in continuous quality improvement, for example, clinical audit Use mechanisms that minimise error, for example, checklists, clinical pathways PATIENT ASSESSMENT Evidence-based practice Critically appraise evidence and information Describe the principles of evidence-based practice and hierarchy of evidence Use best available evidence in clinical decision-making 16 Page 38
39 History and examination Elicit symptoms and signs relevant to the presenting of problems or conditions Recognise how patients present with common acute and chronic problems and conditions Undertake and can justify clinically relevant patient assessments Undertake specific examinations, for example, a bimanual pelvic examination, rectal examination and bedside neurocognitive examination/mental state examination where indicated Investigations Follow up and interpret investigation results appropriately to guide patient management Identify and provide relevant and succinct information when ordering investigations Negotiate with patients the need for tests and explain results Select, request and justify investigations in the course and context of particular patient presentation Patient identification Comply with the organisation's procedures for avoiding patient misidentification Follow the stages of a verification process to ensure the correct identification of a patient Problem formulation Establish a possible differential diagnosis relevant to patients presenting problems or conditions Regularly re-evaluate the patient problem list as part of the clinical reasoning process Synthesise clinical information to generate a ranked problem list containing appropriate provisional diagnoses Referral and consultation Apply the criteria for referral or consultation relevant to a particular problem or condition Collaborate with other health professionals in patient assessment Identify and provide relevant and succinct information EMERGENCIES Advanced cardiac life support Deliver advanced cardiac life support (ACLS) at a level 7 standard Participate in decision-making, and debriefing after cessation of resuscitation Assessment Initiate resuscitation when clinically indicated Recognise and effectively assess potentially acutely ill, deteriorating or dying patients Recognise the abnormal physiology and clinical manifestations of critical illness 17 Page 39
40 Basic life support Effectively use semi-automatic and automatic defibrillators Implement basic airway management, ventilatory and circulatory support Prioritisation Describe the principles of triage Identify patients requiring immediate resuscitation and when and how to call for help Provide clinical care in order of medical priority Disasters Describe their own role in the organisation s disaster management plan PATIENT MANAGEMENT Return to work, ambulatory and community care Identify and appropriately certify work capacity Identify and arrange ambulatory and community care services appropriate for each patient Identify patients suitable for aged care, rehabilitation or palliative care programmes Identify available community care services Discharge planning/transfer of care Follow organisational guidelines to ensure smooth discharge and transfer Liaise with appropriate health professionals, family and other support personnel to ensure proper discharge or transfer of care Undertake effective discharge planning End-of-life care Contribute to team plans involving initiation and coordination of palliative care Manage the confirmation and certification of death and complete death certificates under supervision Recognise cases that may need to be referred to the Coroner Identify and follow the Coroner s procedures Fluid, electrolyte and blood product management Develop, implement, evaluate and maintain an individualised patient management plan for fluid, electrolyte and blood product use Identify the indications for and risks of fluid and electrolyte therapy and use of blood products Manage blood transfusion reactions Recognise and manage the clinical consequences of fluid and electrolyte imbalance in a patient 18 Page 40
41 Management options Identify and justify the patient management options for common problems and conditions Implement and evaluate the management plan in consultation with the patient Provide appropriate advice in situations where a patient s lifestyle may be impacting adversely on their health Recognise complex or uncertain situations and seek advice appropriately Pain management Evaluate the pain management plan to ensure it is clinically relevant Prescribe pain therapies to match the patient s analgesia requirements Specify and can justify the hierarchy of therapies and options for pain control Therapeutics Evaluate the outcomes of medication therapy Involve nurses, pharmacists and other allied health professionals appropriately in medication management Prescribe safely for women who are pregnant or breastfeeding When prescribing, take account of the interactions and actions, indications and contraindications, monitoring requirements and potential adverse effects of each medication used PGY2 During PGY2 the ability to recognise and demonstrate important aspects of clinical management as provided for in PGY1 should be developed and consolidated. In addition, competencies should be extended and new clinical management skills acquired, including those relevant to future vocational training. Examples include: Advance care courses General audit and research Clinical problems and conditions Doctors should be able to adequately identify common or important conditions through history taking, eliciting the relevant signs at examination and investigations. They should then formulate a differential diagnosis and establish and monitor an initial management plan. PGY1 By the end of PGY1 doctors are able to recognise and manage core clinical problems and conditions, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. 19 Page 41
42 General Cognitive or physical disability Early recognition of the deteriorating patient Functional decline or impairment Injury prevention Lifestyle factors adversely impacting on health Perioperative care Abnormal investigation results Abnormal blood results Abnormal INR and / or coagulation profile Electrolyte abnormalities Red cell abnormalities White cell abnormalities Arterial blood gases Abnormal imaging Abnormal pathology results Circulatory Cardiac arrhythmias Chest pain Electrolyte disturbances Heart failure Hypertension Ischaemic heart disease Leg ulcers Limb ischaemia Reduced urinary output Shock Thromboembolic disease Dermatological Common skin conditions, for example, eczema, allergic skin conditions Skin malignancies, for example, basal cell carcinoma (BCC), squamous cell carcinoma (SCC), melanoma Domestic violence Child abuse Elder abuse 20 Page 42
43 Family violence Ear, nose and throat Epistaxis Upper airway compromise Endocrine Abnormal thyroid functions Adrenal disease Diabetic ketoacidosis General management of diabetes and its complications Metabolic syndrome Post-operative diabetic management Eyes (ophthalmology) Foreign body identification Red eye Refractive difficulties Sudden loss of vision Gastrointestinal Abdominal pain Common liver disease, for example, alcoholic liver disease, hepatitis, non-alcoholic fatty liver disease Constipation Diarrhoea Gastrointestinal bleeding Jaundice Nausea and vomiting Recognition of acute abdomen Genito urinary Contraception and sexual health Dysuria and/or frequent micturition Pyelonephritis and UTIs Urinary incontinence Urinary retention 21 Page 43
44 Gynaecological Abnormal menstruation Pain and bleeding in early pregnancy Pelvic pain Haemopoietic Abnormal bleeding due to platelet and coagulation disorders Anaemia Bleeding in the anticoagulated patient Cytopenia Thromboembolic disease Immunology Anaphylaxis Drug reactions Urticaria Infectious diseases Local infections Meningitis Non-specific febrile illness Septicaemia Sexually transmitted infections (STIs) Musculoskeletal Acute joint swelling Joint disorders Minor trauma Neck and back pain Sprains and strains Nephrology Renal failure Neurological Acute headache Delirium Falls, especially in the elderly 22 Page 44
45 Loss of consciousness Seizure disorders Stroke/TIA Subarachnoid haemorrhage Syncope Nutrition / metabolic Weight gain Weight loss Obstetric Postpartum haemorrhage Pre-eclampsia Pre-term labour Oncological emergency Spinal cord compression Raised intracranial pressure Hypercalcaemia Neutropenia Oral disease Toothache Oral infections Pharmacology/toxicology Poisoning Psychiatric/drug and alcohol Addiction (smoking, alcohol, drug) Anxiety Deliberate self-harm Dementia Depression Disturbed or aggressive patient Psychosis Substance abuse Suicide risk assessment 23 Page 45
46 Respiratory Asthma Breathlessness Chronic obstructive pulmonary disease Cough Obstructive sleep apnoea Pneumonia/respiratory infection Respiratory failure Upper airway obstruction PGY2 Doctors should have acquired greater knowledge and broader clinical skills to manage all of the clinical problems and conditions listed for PGY1. Doctors should also have extended the range of clinical problems and conditions they are able to manage, including those relevant to future vocational training. Procedures and interventions Doctors should be able to provide safe treatment to patients by competently performing certain procedural and assessment skills. The following outcome statements apply to all procedures and interventions. Decision-making Explain the indications and contraindications for common procedures Select appropriate procedures with involvement of senior clinicians and the patient Informed consent Apply the principles of informed consent in day-to-day clinical practice Identify the circumstances that require informed consent to be obtained by a more senior clinician Provide a full explanation of a procedure to a patient when undertaking that procedure Preparation Arrange appropriate equipment and describe its use Prepare and position the patient appropriately Recognise the indications for local, regional or general anaesthesia Procedures Arrange appropriate support staff and define their roles 24 Page 46
47 Provide appropriate analgesia Post-procedure Identify and manage common complications Interpret results and evaluate outcomes of treatment Monitor the patient and provide appropriate aftercare Prescribing Prescribing is an intervention and expected skills required for this are found under the headings of infection control, medication safety, pain management, and therapeutics in the clinical management section of the NZCF. PGY1 By the end of PGY1, doctors are able to perform the following procedures and interventions, while recognising the limits of their personal capabilities. They should also be able to recognise complex or uncertain situations and seek advice appropriately. Cardiopulmonary 12-lead electrocardiogram recording and interpretation Bag and mask ventilation Completed ACLS level 7 Laryngeal mask airway placement Oropharyngeal airway Oxygen therapy Diagnostic Blood culture Blood glucose testing MSU Nasal swab Throat swab Urethral swab Wound swab Ear, nose and throat Anterior nasal pack insertion Anterior rhinoscopy 25 Page 47
48 Injections Intramuscular injections Subcutaneous injections Intravenous/intravascular Arterial and venous blood gas sampling and interpretation Blood transfusion Intravenous cannulation Intravenous electrolyte administration Intravenous fluid and drug administration Intravenous infusion set-up Venepuncture Mental health Alcohol withdrawal scale use Ophthalmic Corneal foreign body removal Eye bandage application Eye drop administration Eye irrigation Eyelid eversion Respiratory Nebuliser/inhaler therapy Peak flow measurement and interpretation Spirometry measurement and interpretation Surgical Administration of local anaesthesia Scrub, gown and glove Simple skin lesion excision Surgical knots and simple wound suturing Suture removal Wound debridement Wound dressing 26 Page 48
49 Trauma Apply splints and slings Cervical collar application Inline immobilisation of cervical spine Pressure haemostasis Urogenital Bladder catheterisation (Male and Female) Women s health Genital swabs/cervical smear Speculum examination of the vagina and cervix PGY2 By the end of PGY2 the core procedural skills and interventions identified for PGY1 should be developed and consolidated. In addition, competencies should be extended with the acquisition of new skills including those relevant to future vocational training. Examples include: Advanced prescribing Anaesthetic techniques, for example, simple regional anaesthesia Basic surgical techniques, for example, simple wound closure Critical care interventions, for example, non invasive ventilation Diagnostic ultrasound Invasive diagnostic techniques, for example, joint aspiration, lumbar puncture, biopsies Management of trauma, for example, reduction of simple fractures and dislocations Psychological interventions, for example, behavioural interventions, counselling skills 27 Page 49

50 End of Clinical Attachment Assessment The PGY1 Intern NZ/Australian graduates NZREX graduates Intern s Registration Number: Level 6, 80 The Terrace, PO Box , Wellington, New Zealand To be completed by the Clinical Supervisor at the end of the attachment. This form will also guide the mid-cycle formative feedback and promote the ongoing development (fine tuning) of the Professional Development Plan (PDP). If an Intern scores a 1 or 2 in any of the 12 domains; this does not necessarily constitute a failed clinical attachment. These scores will require the Intern, the Prevocational Educational and Clinical supervisors to meet to decide actions to be included in the PDP. A marginal performance score on the final SUMMATIVE ASSESSMENT does not necessarily constitute a failed clinical attachment but requires the Intern, the Prevocational Educational and Clinical supervisors to meet to decide actions that must be included in the PDP. An overall unsatisfactory score on the final SUMMATIVE ASSESSMENT constitutes a failed clinical attachment. A remediation plan that addresses the competency deficiencies must be developed by the Prevocational Educational supervisor and the Intern and be reflected in the PDP. The Intern must have FOUR satisfactory End of Clinical Attachment assessments to apply for general registration. This assessment summary must take into account the assessments of the unit s registrars (vocational trainees), nurses and others who routinely work with the Intern. The form must be returned to the RMO Unit and signed by your designated Prevocational Educational Supervisor. Please retain a copy for your own records. Name:. Employer:... Qualifications:.. Date registration started:../../. This doctor is currently employed as......until../../. Dates of attachment: (From) / / (To) / / Supervising consultants: Accredited Clinical Attachment:... KEY: 1 Below expectation - requires further development (e.g. PDP) 2 Borderline performance - would benefit from further development in PDP 3 Meets expectation - performs at a satisfactory level 4 Above expectation - performs at a level better than that which would be expected for the level of experience 5 Exceptional - performs at a level beyond that which would be expected for the level of experience N/O Not observed PROFESSIONALISM: By the end of PGY1 Interns are able to practise medicine in a professional manner, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately. 1 Doctor and Society (Examples - The Intern demonstrates cultural competence (particularly when working with Maori and Pacific patients and their whanau / families), health and work promotion, best health resource use, knowledge of the law as pertains to the practice of Medicine, and the maintenance of professional standards.) 2 Professional behaviours (Examples - The Intern, demonstrates team work and ability to provide clinical leadership, practises ethically, manages personal health / well-being, engages in professional development, identifies and assists another practitioner in difficulty, manages personal time and does not bring the profession into disrepute.) 3 Teaching, learning and supervision (Examples - The Intern participates effectively in assessment and feedback, demonstrates self-directed learning, is developing personal supervision skills and participates in effective teaching in the department or organisation.) COMMUNICATION: By the end of PGY1 Interns are able to identify and practise effective communication, while recognising the limits of their personal capabilities. They should be able to recognise complex or uncertain situations and seek advice appropriately N/O N/O Page 50 1
Medical Council of New Zealand
 Level 13, Mid City Tower 139 143 Willis Street PO box 11649 Wellington Phone: 0800 286 801 Medical Council of New Zealand Invitation for an Expression of Interest Invitation to submit expression of interest
Level 13, Mid City Tower 139 143 Willis Street PO box 11649 Wellington Phone: 0800 286 801 Medical Council of New Zealand Invitation for an Expression of Interest Invitation to submit expression of interest
STRENGTHENING RECERTIFICATION FOR VOCATIONALLY-REGISTERED DOCTORS IN NEW ZEALAND A DISCUSSION DOCUMENT
 STRENGTHENING RECERTIFICATION FOR VOCATIONALLY-REGISTERED DOCTORS IN NEW ZEALAND A DISCUSSION DOCUMENT September 2018 1 Contents Introduction... 3 What is recertification?... 3 Recertification in New Zealand...
STRENGTHENING RECERTIFICATION FOR VOCATIONALLY-REGISTERED DOCTORS IN NEW ZEALAND A DISCUSSION DOCUMENT September 2018 1 Contents Introduction... 3 What is recertification?... 3 Recertification in New Zealand...
WHAT YOU NEED TO KNOW ABOUT MEDICAL REGISTRATION IN NEW ZEALAND
 Medical Council of New Zealand Te Kaunihera Rata o Aotearoa WHAT YOU NEED TO KNOW ABOUT MEDICAL REGISTRATION IN NEW ZEALAND May 2018 TE KAUNIHERA RATA O AOTEAROA MEDICAL COUNCIL OF NEW ZEALAND Protecting
Medical Council of New Zealand Te Kaunihera Rata o Aotearoa WHAT YOU NEED TO KNOW ABOUT MEDICAL REGISTRATION IN NEW ZEALAND May 2018 TE KAUNIHERA RATA O AOTEAROA MEDICAL COUNCIL OF NEW ZEALAND Protecting
Medical Council of New Zealand Protecting the public, promoting good medical practice. Strategic plan from 1 July 2017 to 30 June 2018
 Medical Council of New Zealand Protecting the public, promoting good medical practice Strategic plan from 1 July 2017 to 30 June 2018 Our vision We will provide leadership to the medical profession and
Medical Council of New Zealand Protecting the public, promoting good medical practice Strategic plan from 1 July 2017 to 30 June 2018 Our vision We will provide leadership to the medical profession and
Australian Medical Council Limited
 Australian Medical Council Limited Procedures for Assessment and Accreditation of Specialist Medical Programs and Professional Development Programs by the Australian Medical Council 2017 Specialist Education
Australian Medical Council Limited Procedures for Assessment and Accreditation of Specialist Medical Programs and Professional Development Programs by the Australian Medical Council 2017 Specialist Education
Perioperative Nurse Coordinator Lead [Surgical]
![Perioperative Nurse Coordinator Lead [Surgical]](/thumbs/80/80543803.jpg "Perioperative Nurse Coordinator Lead [Surgical]") Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
Date : July 2017 Job Title : Perioperative Nurse Coordinator Lead Note: Lead role is equivalent to Associate Clinical Charge Nurse Level [SN 4] Department : Surgical and Ambulatory Services Otorhinolaryngology
Initial education and training of pharmacy technicians: draft evidence framework
 Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
Registered Nurse ACC Clinical Case Management
 Date: 14/08/2017 Job Title : Registered Nurse ACC Clinical Case Department : ACC Unit, Hospital Services Location : North Shore Hospital Reporting To : Manager ACC and Eligibility for performance within
Date: 14/08/2017 Job Title : Registered Nurse ACC Clinical Case Department : ACC Unit, Hospital Services Location : North Shore Hospital Reporting To : Manager ACC and Eligibility for performance within
Clinical Nurse Specialist / Nurse Practitioner Intern Women s Health
 Date: December 2017 Job Title : Clinical Nurse Specialist / Nurse Practitioner The CNS / NP Intern for Women s Health works in a collaborative environment, to facilitate the development of advanced nursing
Date: December 2017 Job Title : Clinical Nurse Specialist / Nurse Practitioner The CNS / NP Intern for Women s Health works in a collaborative environment, to facilitate the development of advanced nursing
Accreditation Manager
 Guideline Name: Clinical Learning for Junior Doctors Consultation and Date Approved: Accreditation Committee approval: 18 September 2017 Review: 2020 Responsible Officer: Purpose and Scope Accreditation
Guideline Name: Clinical Learning for Junior Doctors Consultation and Date Approved: Accreditation Committee approval: 18 September 2017 Review: 2020 Responsible Officer: Purpose and Scope Accreditation
Clinical Nurse Specialist - Research General Surgery
 Date : May 2018 Clinical Nurse Specialist - Research Job Title : Clinical Nurse Specialist Research Department : Department of, Surgical & Ambulatory Service Location : North Shore Hospital Reporting To
Date : May 2018 Clinical Nurse Specialist - Research Job Title : Clinical Nurse Specialist Research Department : Department of, Surgical & Ambulatory Service Location : North Shore Hospital Reporting To
GATEWAY ASSESSMENT SERVICE: SERVICE SPECIFICATION
 GATEWAY ASSESSMENT SERVICE: SERVICE SPECIFICATION 2017 GATEWAY ASSESSMENT SERVICE SPECIFICATION 1 Table of Contents 1. About the Service Specification... 4 Purpose... 4 2. Service overview... 5 Brief description
GATEWAY ASSESSMENT SERVICE: SERVICE SPECIFICATION 2017 GATEWAY ASSESSMENT SERVICE SPECIFICATION 1 Table of Contents 1. About the Service Specification... 4 Purpose... 4 2. Service overview... 5 Brief description
Clinical Nurse Director
 Date: March 2018 Job Title : Clinical Nurse Director Department : Acute and Emergency Medicine Division and Specialty Medicine & Health of Older People Division Location : North Shore Hospital, Waitakere
Date: March 2018 Job Title : Clinical Nurse Director Department : Acute and Emergency Medicine Division and Specialty Medicine & Health of Older People Division Location : North Shore Hospital, Waitakere
Professional Practice Guideline 14:
 Professional Practice Guideline 14: National codes and standards relevant to psychiatry practice and mental health services in Australia and New Zealand April 2017 Authorising Committee: Responsible Committee:
Professional Practice Guideline 14: National codes and standards relevant to psychiatry practice and mental health services in Australia and New Zealand April 2017 Authorising Committee: Responsible Committee:
Request for Proposal PROFESSIONAL AUDIT SERVICES
 Request for Proposal PROFESSIONAL AUDIT SERVICES FORENSIC AUDIT OF CITY S FINANCE DEPARTMENT, URA ACCOUNTS AND DEVELOPMENT AUTHORITY ACCOUNTS PROCEDURES CITY OF FOREST PARK TABLE OF CONTENTS I. INTRODUCTION
Request for Proposal PROFESSIONAL AUDIT SERVICES FORENSIC AUDIT OF CITY S FINANCE DEPARTMENT, URA ACCOUNTS AND DEVELOPMENT AUTHORITY ACCOUNTS PROCEDURES CITY OF FOREST PARK TABLE OF CONTENTS I. INTRODUCTION
GUIDELINES FOR JUNIOR DOCTORS USING THE NATIONAL ASSESSMENT TOOLS
 GUIDELINES FOR JUNIOR DOCTORS USING THE NATIONAL ASSESSMENT TOOLS This training manual contains materials which are intended to be used to assist JUNIOR DOCTORs in using the National Assessment Tools.
GUIDELINES FOR JUNIOR DOCTORS USING THE NATIONAL ASSESSMENT TOOLS This training manual contains materials which are intended to be used to assist JUNIOR DOCTORs in using the National Assessment Tools.
Guide for Recently. Registered Medical. Radiation Therapy Practitioners. Medical Radiation Technology (medical imaging and radiation therapy)
") Guide for Recently Registered Medical Imaging and Radiation Therapy Practitioners Medical Radiation Technology (medical imaging and radiation therapy) July 2017 01 The Board 02 02 The Practitioner 06 03
Guide for Recently Registered Medical Imaging and Radiation Therapy Practitioners Medical Radiation Technology (medical imaging and radiation therapy) July 2017 01 The Board 02 02 The Practitioner 06 03
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Request for Proposal for Digitizing Document Services and Document Management Solution RFP-DOCMANAGESOLUTION1
 City of Hinesville 115 East ML King Jr Drive Hinesville, GA 31313 Request for Proposal for Digitizing Document Services and Document Management Solution RFP-DOCMANAGESOLUTION1 Closing Date: December 20,
City of Hinesville 115 East ML King Jr Drive Hinesville, GA 31313 Request for Proposal for Digitizing Document Services and Document Management Solution RFP-DOCMANAGESOLUTION1 Closing Date: December 20,
POSITION DESCRIPTION
 POSITION DESCRIPTION TITLE: Charge Nurse, Oncology Outpatients REPORTS TO: Nurse Unit Manager PROFESSIONAL REPORTING: Nurse Unit Manager LOCATION: Auckland City Hospital (Grafton) AUTHORISED BY: Nurse
POSITION DESCRIPTION TITLE: Charge Nurse, Oncology Outpatients REPORTS TO: Nurse Unit Manager PROFESSIONAL REPORTING: Nurse Unit Manager LOCATION: Auckland City Hospital (Grafton) AUTHORISED BY: Nurse
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Clinical Nurse Specialist - Quality & Research Dept of Anaesthesiology
 Date: June 2017 Job Title : Clinical Nurse Specialist - Quality & Research Clinical Nurse Specialist, Dept of Anaesthesiology & Perioperative Medicine Department : Department of Anaesthesia & Perioperative
Date: June 2017 Job Title : Clinical Nurse Specialist - Quality & Research Clinical Nurse Specialist, Dept of Anaesthesiology & Perioperative Medicine Department : Department of Anaesthesia & Perioperative
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
Duty Nurse Manager Waitemata Central Position Description
 Date: January 2016 (review January 2017) Job Title : Department : Location : Waitemata DHB (based at NSH and/or WTH) Reporting to Professional Line Operations Manager (NSH and /or WTH) Charge Nurse Manager
Date: January 2016 (review January 2017) Job Title : Department : Location : Waitemata DHB (based at NSH and/or WTH) Reporting to Professional Line Operations Manager (NSH and /or WTH) Charge Nurse Manager
Designated Title: Clinical Nurse Specialist. Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery
 Designated Title: Clinical Nurse Specialist Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery This role is considered a non-core children s worker and will be subject to safety checking
Designated Title: Clinical Nurse Specialist Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery This role is considered a non-core children s worker and will be subject to safety checking
NATIONAL GUIDELINES FOR THE ACCREDITATION OF NURSING AND MIDWIFERY PROGRAMS LEADING TO REGISTRATION AND ENDORSEMENT IN AUSTRALIA
 NATIONAL GUIDELINES FOR THE ACCREDITATION OF NURSING AND MIDWIFERY PROGRAMS LEADING TO REGISTRATION AND ENDORSEMENT IN AUSTRALIA NATIONAL GUIDELINES FOR THE ACCREDITATION OF NURSING AND MIDWIFERY PROGRAMS
NATIONAL GUIDELINES FOR THE ACCREDITATION OF NURSING AND MIDWIFERY PROGRAMS LEADING TO REGISTRATION AND ENDORSEMENT IN AUSTRALIA NATIONAL GUIDELINES FOR THE ACCREDITATION OF NURSING AND MIDWIFERY PROGRAMS
National Accreditation Guidelines: Nursing and Midwifery Education Programs
 National Accreditation Guidelines: Nursing and Midwifery Education Programs February 2017 National Accreditation Guidelines: Nursing and Midwifery Education Programs Version Control Version Date Amendments
National Accreditation Guidelines: Nursing and Midwifery Education Programs February 2017 National Accreditation Guidelines: Nursing and Midwifery Education Programs Version Control Version Date Amendments
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Practice Review Guide
 Practice Review Guide October, 2000 Table of Contents Section A - Policy 1.0 PREAMBLE... 5 2.0 INTRODUCTION... 6 3.0 PRACTICE REVIEW COMMITTEE... 8 4.0 FUNDING OF REVIEWS... 8 5.0 CHALLENGING A PRACTICE
Practice Review Guide October, 2000 Table of Contents Section A - Policy 1.0 PREAMBLE... 5 2.0 INTRODUCTION... 6 3.0 PRACTICE REVIEW COMMITTEE... 8 4.0 FUNDING OF REVIEWS... 8 5.0 CHALLENGING A PRACTICE
VET Student Handbook
 Boonah State High School VET Student Handbook Prepared by Velg Training Version 1, January 2015 velgtraining.com Table of Contents Introduction... 3 The Australian Qualifications Framework (AQF)... 3 AQF
Boonah State High School VET Student Handbook Prepared by Velg Training Version 1, January 2015 velgtraining.com Table of Contents Introduction... 3 The Australian Qualifications Framework (AQF)... 3 AQF
Course Related Work Experience Vice-Chancellor's Directive
 Course Related Work Experience Vice-Chancellor's Directive Abstract This Directive prescribes core UTS requirements designed to ensure that UTS students and staff experience of Course Related Work Experience
Course Related Work Experience Vice-Chancellor's Directive Abstract This Directive prescribes core UTS requirements designed to ensure that UTS students and staff experience of Course Related Work Experience
Practice Review Guide April 2015
 Practice Review Guide April 2015 Printed: September 28, 2017 Table of Contents Section A Practice Review Policy... 1 1.0 Preamble... 1 2.0 Introduction... 2 3.0 Practice Review Committee... 4 4.0 Funding
Practice Review Guide April 2015 Printed: September 28, 2017 Table of Contents Section A Practice Review Policy... 1 1.0 Preamble... 1 2.0 Introduction... 2 3.0 Practice Review Committee... 4 4.0 Funding
Independent prescribing conversion programme. De Montfort University Report of a reaccreditation event May 2017
 Independent prescribing conversion programme De Montfort University Report of a reaccreditation event May 2017 GPhC, independent prescribing conversion programme reaccreditation report Page 1 of 10 Event
Independent prescribing conversion programme De Montfort University Report of a reaccreditation event May 2017 GPhC, independent prescribing conversion programme reaccreditation report Page 1 of 10 Event
POSITION DESCRIPTION. Clinical Team Coordinator. Adult Community Services Mental Health
 POSITION DESCRIPTION Clinical 0.5 Coordination 0.5 Clinical Adult Community Services Mental Health Date Reviewed: June 2012 Note - as this is a newly created role, the Job Description will be reviewed
POSITION DESCRIPTION Clinical 0.5 Coordination 0.5 Clinical Adult Community Services Mental Health Date Reviewed: June 2012 Note - as this is a newly created role, the Job Description will be reviewed
Competencies for registered nurses
 1 Competencies for registered nurses Ki te whakarite i nga ahuatanga o nga Tapuhi e pa ana mo nga iwi katoa Regulating nursing practice to protect public safety December 2007 2 Competencies for registered
1 Competencies for registered nurses Ki te whakarite i nga ahuatanga o nga Tapuhi e pa ana mo nga iwi katoa Regulating nursing practice to protect public safety December 2007 2 Competencies for registered
INTERNAL MEDICINE PHYSICIAN POSITION DESCRIPTION
 INTERNAL MEDICINE PHYSICIAN POSITION DESCRIPTION Role Title: Reports To: Directorate: Direct Reports: Location: Internal Medicine Physician Clinical Leader, Medicine Service Manager, Medicine Medical Supervision
INTERNAL MEDICINE PHYSICIAN POSITION DESCRIPTION Role Title: Reports To: Directorate: Direct Reports: Location: Internal Medicine Physician Clinical Leader, Medicine Service Manager, Medicine Medical Supervision
INTERNATIONAL FOUNDATION FOR ELECTORAL SYSTEMS (IFES) Request for Proposals for Office Security Services in Pakistan RFP/17/015
 Request for Proposals for Office Security Services in Pakistan RFP/17/015") INTERNATIONAL FOUNDATION FOR ELECTORAL SYSTEMS (IFES) Request for Proposals for Office Security Services in Pakistan November 2, 2016 TABLE OF CONTENTS 1 INTRODUCTION...3 1.1 PURPOSE...3 1.2 COVERAGE &
INTERNATIONAL FOUNDATION FOR ELECTORAL SYSTEMS (IFES) Request for Proposals for Office Security Services in Pakistan November 2, 2016 TABLE OF CONTENTS 1 INTRODUCTION...3 1.1 PURPOSE...3 1.2 COVERAGE &
MENTAL HEALTH & ADDICTION SERVICES
 MENTAL HEALTH & ADDICTION SERVICES Position: Report To: Responsible For: Location: Hours of Work: Liaise With: Occupational Therapist Case Manager Regional Clinical Co-ordinator; Voyagers Child and Adolescent
MENTAL HEALTH & ADDICTION SERVICES Position: Report To: Responsible For: Location: Hours of Work: Liaise With: Occupational Therapist Case Manager Regional Clinical Co-ordinator; Voyagers Child and Adolescent
Social Worker, Specialty Medicine and Health of Older People, Acute and Emergency Medicine, and Surgical and Ambulatory Service - Renal
 Date: February 2018 Job Title : Social Worker, Allied Health, North and West Department : Medicine, and Surgical and Ambulatory Service Location : North Shore and Waitakere Reporting To : 1. Allied Health
Date: February 2018 Job Title : Social Worker, Allied Health, North and West Department : Medicine, and Surgical and Ambulatory Service Location : North Shore and Waitakere Reporting To : 1. Allied Health
THE CODE. Professional standards of conduct, ethics and performance for pharmacists in Northern Ireland. Effective from 1 March 2016
 THE CODE Professional standards of conduct, ethics and performance for pharmacists in Northern Ireland Effective from 1 March 2016 PRINCIPLE 1: ALWAYS PUT THE PATIENT FIRST PRINCIPLE 2: PROVIDE A SAFE
THE CODE Professional standards of conduct, ethics and performance for pharmacists in Northern Ireland Effective from 1 March 2016 PRINCIPLE 1: ALWAYS PUT THE PATIENT FIRST PRINCIPLE 2: PROVIDE A SAFE
Pre-registration. e-portfolio
 Pre-registration e-portfolio 2013 2014 Contents E-portfolio Introduction 3 Performance Standards 5 Page Appendix SWOT analysis 1 Start of training plan 2 13 week plan 3 26 week plan 4 39 week plan 5 Appraisal
Pre-registration e-portfolio 2013 2014 Contents E-portfolio Introduction 3 Performance Standards 5 Page Appendix SWOT analysis 1 Start of training plan 2 13 week plan 3 26 week plan 4 39 week plan 5 Appraisal
Guidance on supporting information for revalidation
 Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Role Description. Locum General Surgeon - sub speciality Breast. Clinical Leader General Surgery Operations Manager, Surgery
 Role Description Position: Service / Directorate: Responsible to: Locum General Surgeon - sub speciality Breast General Surgery Surgery, Women s and Children s Health Clinical Leader General Surgery Operations
Role Description Position: Service / Directorate: Responsible to: Locum General Surgeon - sub speciality Breast General Surgery Surgery, Women s and Children s Health Clinical Leader General Surgery Operations
BSc (HONS) NURSING IN THE HOME/ DISTRICT NURSING
 NURSING IN THE HOME/ DISTRICT NURSING") BSc (HONS) NURSING IN THE HOME/ DISTRICT NURSING PRACTICE TEACHER HANDBOOK OCTOBER 2014 (Hons) Nursing in the Home District Nursing Practice Teacher Handbook.doc 1 CONTENTS 1 INTRODUCTION 1 2 THE PROGRAMME
BSc (HONS) NURSING IN THE HOME/ DISTRICT NURSING PRACTICE TEACHER HANDBOOK OCTOBER 2014 (Hons) Nursing in the Home District Nursing Practice Teacher Handbook.doc 1 CONTENTS 1 INTRODUCTION 1 2 THE PROGRAMME
MENTAL HEALTH & ADDICTION SERVICES
 MENTAL HEALTH & ADDICTION SERVICES Position: Report To: Responsible For: Location: Hours Of Work: Liaise With: Addiction Clinician Clinical Team Leader - BOPAS Nil Staff Regional (Tauranga based) 80 hours
MENTAL HEALTH & ADDICTION SERVICES Position: Report To: Responsible For: Location: Hours Of Work: Liaise With: Addiction Clinician Clinical Team Leader - BOPAS Nil Staff Regional (Tauranga based) 80 hours
REQUEST FOR PROPOSAL
 1 REQUEST FOR PROPOSAL FOR 3 rd Party Ambulance Billing Services PROPOSAL NO. FY2013/004 BY SPOKANE TRIBE OF INDIANS PURCHASING/PROPERTY DEPARTMENT 6195 FORD/WELLPINIT RD PO BOX 100 WELLPINIT WA 99040
1 REQUEST FOR PROPOSAL FOR 3 rd Party Ambulance Billing Services PROPOSAL NO. FY2013/004 BY SPOKANE TRIBE OF INDIANS PURCHASING/PROPERTY DEPARTMENT 6195 FORD/WELLPINIT RD PO BOX 100 WELLPINIT WA 99040
PRIVACY MANAGEMENT FRAMEWORK
 PRIVACY MANAGEMENT FRAMEWORK Section Contact Office of the AVC Operations, International and University Registrar Risk Management Last Review July 2014 Next Review July 2017 Approval SLT14/7/176 Effective
PRIVACY MANAGEMENT FRAMEWORK Section Contact Office of the AVC Operations, International and University Registrar Risk Management Last Review July 2014 Next Review July 2017 Approval SLT14/7/176 Effective
STATE OF RHODE ISLAND OFFICE OF THE GENERAL TREASURER
 STATE OF RHODE ISLAND OFFICE OF THE GENERAL TREASURER REQUEST FOR PROPOSALS TO PROVIDE An Automated Reconciliation Software Solution The Office of the General Treasurer 50 Service Avenue Warwick, RI 02886
STATE OF RHODE ISLAND OFFICE OF THE GENERAL TREASURER REQUEST FOR PROPOSALS TO PROVIDE An Automated Reconciliation Software Solution The Office of the General Treasurer 50 Service Avenue Warwick, RI 02886
CAREER & EDUCATION FRAMEWORK
 CAREER & EDUCATION FRAMEWORK FOR NURSES IN PRIMARY HEALTH CARE ENROLLED NURSES Acknowledgments The Career and Education Framework is funded by the Australian Government Department of Health under the Nursing
CAREER & EDUCATION FRAMEWORK FOR NURSES IN PRIMARY HEALTH CARE ENROLLED NURSES Acknowledgments The Career and Education Framework is funded by the Australian Government Department of Health under the Nursing
Charge Nurse Manager Adult Mental Health Services Acute Inpatient
 Date: February 2013 DRAFT Job Title : Charge Nurse Manager Department : Waiatarau Acute Unit Location : Waitakere Hospital Reporting To : Operations Manager Adult Mental Health Services for the achievement
Date: February 2013 DRAFT Job Title : Charge Nurse Manager Department : Waiatarau Acute Unit Location : Waitakere Hospital Reporting To : Operations Manager Adult Mental Health Services for the achievement
Required Competencies: Anaesthetic Technicians
 Required Competencies: Anaesthetic Technicians The Profession of Anaesthetic Technology Anaesthetic Technology is the provision of perioperative technical management and patient care for supporting the
Required Competencies: Anaesthetic Technicians The Profession of Anaesthetic Technology Anaesthetic Technology is the provision of perioperative technical management and patient care for supporting the
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa
 Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Core competencies* for undergraduate students in clinical associate, dentistry and medical teaching and learning programmes in South Africa Developed by the Undergraduate Education and Training Subcommittee
Specialty Nurse Endoscopy Nurse Coordinator
 Date: October 2016 Job Title : Endoscopy Nurse Specialty Nurse Department : Gastroenterology/Endoscopy Department Location : Waitemata District Health Board Reporting To : Operations Manager, Gastroenterology
Date: October 2016 Job Title : Endoscopy Nurse Specialty Nurse Department : Gastroenterology/Endoscopy Department Location : Waitemata District Health Board Reporting To : Operations Manager, Gastroenterology
Ready for revalidation. Supporting information for appraisal and revalidation
 2012 Ready for revalidation Supporting information for appraisal and revalidation During their annual appraisals, doctors will use supporting information to demonstrate that they are continuing to meet
2012 Ready for revalidation Supporting information for appraisal and revalidation During their annual appraisals, doctors will use supporting information to demonstrate that they are continuing to meet
AMC Workplace-based Assessment Accreditation Guidelines and Procedures. 7 October 2014
 AMC Workplace-based Assessment Accreditation Guidelines and Procedures 7 October 2014 Contents Part A: Workplace-based assessment accreditation procedures... 1 1. Background information... 1 2. What is
AMC Workplace-based Assessment Accreditation Guidelines and Procedures 7 October 2014 Contents Part A: Workplace-based assessment accreditation procedures... 1 1. Background information... 1 2. What is
Clinical Nurse Specialist Breast Cancer & Breast Reconstruction
 Date : January 2018 Position Title : Clinical Nurse Specialist - Department : Surgical Services. Location : Waitemata District Health Board Reporting To : Head of Division Nursing Surgical and Ambulatory
Date : January 2018 Position Title : Clinical Nurse Specialist - Department : Surgical Services. Location : Waitemata District Health Board Reporting To : Head of Division Nursing Surgical and Ambulatory
Outpatient Dietitian
 POSITION DESCRIPTION Outpatient Dietitian Date Produced/Reviewed: Position Holder's Name:... Position Holder's Signature:... Manager/Supervisor's Name:... Manager/Supervisor's Signature:... Date:... Document
POSITION DESCRIPTION Outpatient Dietitian Date Produced/Reviewed: Position Holder's Name:... Position Holder's Signature:... Manager/Supervisor's Name:... Manager/Supervisor's Signature:... Date:... Document
Clinical Nurse Specialist Palliative Care Position Description
 Date: February 2018 Job Title : Department : Hospital Palliative Care Service Location : North Shore Hospital/Waitakere Hospital, Specialty Medicine and Health of Older People Division Reports to [Line]
Date: February 2018 Job Title : Department : Hospital Palliative Care Service Location : North Shore Hospital/Waitakere Hospital, Specialty Medicine and Health of Older People Division Reports to [Line]
Role Profile: Clinical Nurse Specialist
 Role Profile: Clinical Nurse Specialist Role Title Purpose of the Role Details of the service/background to the post Department/Directorate Key Reports Key Direct Reports Grade Clinical Nurse Specialist
Role Profile: Clinical Nurse Specialist Role Title Purpose of the Role Details of the service/background to the post Department/Directorate Key Reports Key Direct Reports Grade Clinical Nurse Specialist
Level 2: Exceptional LEP Review Visit by School Level 3: Exceptional LEP Trigger Visit by Deanery with Externality... 18
 Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
Registered Nurse - Clinical Coach ADU
 Date: November 2017 Job Title : Registered Nurse - Clinical Coach, Department : Assessment and Diagnostic Unit, North Shore Hospital Location : North Shore Hospital Reporting To : [Line) Charge Nurse Manager
Date: November 2017 Job Title : Registered Nurse - Clinical Coach, Department : Assessment and Diagnostic Unit, North Shore Hospital Location : North Shore Hospital Reporting To : [Line) Charge Nurse Manager
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
POSITION DESCRIPTION. Clinical Psychologist Paediatric Consult Liaison Psychological Medicine
 POSITION DESCRIPTION Clinical Psychologist Paediatric Consult Liaison Psychological Medicine This role is considered a core children s worker and will be subject to safety checking as part of the Vulnerable
POSITION DESCRIPTION Clinical Psychologist Paediatric Consult Liaison Psychological Medicine This role is considered a core children s worker and will be subject to safety checking as part of the Vulnerable
POSITION DESCRIPTION
 POSITION DETAILS: POSITION DESCRIPTION TITLE: Public Health Nurse Refugee Health Screening Service REPORTS TO: Programme Supervisor LOCATION: Auckland Regional Public Health Service (ARPHS). Position based
POSITION DETAILS: POSITION DESCRIPTION TITLE: Public Health Nurse Refugee Health Screening Service REPORTS TO: Programme Supervisor LOCATION: Auckland Regional Public Health Service (ARPHS). Position based
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Protocol for. The use of Independent Best Interests Assessors for. Deprivation of Liberty Safeguards Assessments in care homes and hospitals
 Protocol for The use of Independent Best Interests Assessors for Deprivation of Liberty Safeguards Assessments in care homes and hospitals Report Author: Lorraine Currie Revised April 2013 Review Date:
Protocol for The use of Independent Best Interests Assessors for Deprivation of Liberty Safeguards Assessments in care homes and hospitals Report Author: Lorraine Currie Revised April 2013 Review Date:
Conditions of Registration 2018/19
 Conditions of Registration 2018/19 Supplementary Agreement (Nursing) Contents Scope... 2 What this document covers... 2 What this document does not cover... 2 Supplementary Agreements superseded by this
Conditions of Registration 2018/19 Supplementary Agreement (Nursing) Contents Scope... 2 What this document covers... 2 What this document does not cover... 2 Supplementary Agreements superseded by this
WORKING DRAFT. Standards of proficiency for nursing associates. Release 1. Page 1
 WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
Competencies for the Registered Nurse Scope of Practice Approved by the Council: June 2005
 Competencies for the Registered Nurse Scope of Practice Approved by the Council: June 2005 Domains of competence for the registered nurse scope of practice There are four domains of competence for the
Competencies for the Registered Nurse Scope of Practice Approved by the Council: June 2005 Domains of competence for the registered nurse scope of practice There are four domains of competence for the
The Director is the legally responsible person must manage the RTO s compliance with the Standards for RTO s 2015.
 Duty Statement - Director The Director is the legally responsible person must manage the RTO s compliance with the Standards for RTO s 2015. RTO compliance delegation The Director may delegate their key
Duty Statement - Director The Director is the legally responsible person must manage the RTO s compliance with the Standards for RTO s 2015. RTO compliance delegation The Director may delegate their key
The Trainee Doctor. Foundation and specialty, including GP training
 Foundation and specialty, including GP training The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust
Foundation and specialty, including GP training The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust
POSITION DESCRIPTION
 POSITION DESCRIPTION Position details: Title: Reports to: Reports professionally to: Date: Charge Nurse Te Whetu Tawera Nurse Manager Nurse Director Mental Health and Addiction Healthcare Service Group
POSITION DESCRIPTION Position details: Title: Reports to: Reports professionally to: Date: Charge Nurse Te Whetu Tawera Nurse Manager Nurse Director Mental Health and Addiction Healthcare Service Group
Title: Senior Medical Officer Department: Cardiothoracic and Vascular ICU (CVICU) and HDU. Clinical Director, Cardiothoracic and Vascular ICU and HDU
 and HDU. Clinical Director, Cardiothoracic and Vascular ICU and HDU") POSITION DESCRIPTION Position Details: Title: Senior Medical Officer Department: Cardiothoracic and Vascular ICU (CVICU) and HDU Reports to: Location: Clinical Director, Cardiothoracic and Vascular ICU
POSITION DESCRIPTION Position Details: Title: Senior Medical Officer Department: Cardiothoracic and Vascular ICU (CVICU) and HDU Reports to: Location: Clinical Director, Cardiothoracic and Vascular ICU
St Augustine s. VET Student Handbook Prepared by Velg Training Version 1, January 2015 velgtraining.com
 St Augustine s College S pringfield VET Student Handbook 2017 Prepared by Velg Training Version 1, January 2015 velgtraining.com Table of Contents Introduction 3 The Australian Qualifications Framework
St Augustine s College S pringfield VET Student Handbook 2017 Prepared by Velg Training Version 1, January 2015 velgtraining.com Table of Contents Introduction 3 The Australian Qualifications Framework
P O L I C Y F O R A C C R E D I T A T I O N C L I N I C A L D E P A R T M E N T S F O R T H E
 P O L I C Y F O R A C C R E D I T A T I O N OF C L I N I C A L D E P A R T M E N T S F O R T H E D I A G N O S T I C I M A G I N G M E D I C A L P H Y S I C S T R A I N I N G P R O G R A M Author : S Howlett
P O L I C Y F O R A C C R E D I T A T I O N OF C L I N I C A L D E P A R T M E N T S F O R T H E D I A G N O S T I C I M A G I N G M E D I C A L P H Y S I C S T R A I N I N G P R O G R A M Author : S Howlett
Registered Nurse Children s Community Nurse (HC4KS) Position Description
 Position Description") Date: July 2016 Job Title : Community Children s Nurse Department : Child Women and Family Reporting to : Operations Manager for operational support to meet performance management objectives and provision
Date: July 2016 Job Title : Community Children s Nurse Department : Child Women and Family Reporting to : Operations Manager for operational support to meet performance management objectives and provision
Accreditation Guidelines
 Postgraduate Medical Education Council of Tasmania Accreditation Guidelines May 2016 Guidelines outlining the accreditation process for intern training programs in Tasmania Objectives of the Accreditation
Postgraduate Medical Education Council of Tasmania Accreditation Guidelines May 2016 Guidelines outlining the accreditation process for intern training programs in Tasmania Objectives of the Accreditation
Role Profile. CNM II Clinical Facilitator Staff Development Co-Ordinator MedEl Directorate
 Role Profile Role Title Purpose of the Role Department/Directorate Key Reports Grade CNM II Clinical Facilitator Staff Development Co-Ordinator MedEl Directorate The post holder is responsible for leading
Role Profile Role Title Purpose of the Role Department/Directorate Key Reports Grade CNM II Clinical Facilitator Staff Development Co-Ordinator MedEl Directorate The post holder is responsible for leading
The Code Standards of conduct, performance and ethics for chiropractors. Effective from 30 June 2016
 The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016 2 The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016
The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016 2 The Code Standards of conduct, performance and ethics for chiropractors Effective from 30 June 2016
Senior Medical Education Officer Recurring vacancies may become available in other work units Status
 Role description Job ad reference GC236694 Role title Senior Medical Education Officer Recurring vacancies may become available in other work units Status Permanent full time Please note, future vacancies
Role description Job ad reference GC236694 Role title Senior Medical Education Officer Recurring vacancies may become available in other work units Status Permanent full time Please note, future vacancies
FAMILY WELLBEING GUIDELINES
 FAMILY WELLBEING GUIDELINES 2016 Table of Contents Table of Contents... 1 1. About these guidelines... 2 Who are these guidelines for?... 2 What is the purpose of these guidelines?... 2 How should these
FAMILY WELLBEING GUIDELINES 2016 Table of Contents Table of Contents... 1 1. About these guidelines... 2 Who are these guidelines for?... 2 What is the purpose of these guidelines?... 2 How should these
Policy on continuing professional development activities
 Category APC and Recertification Effective Date December 2009 Last Modified January 2010 Review Date December 2012 Approved By Contact Person Council Senior Business Development Advisor 1 This policy provides
Category APC and Recertification Effective Date December 2009 Last Modified January 2010 Review Date December 2012 Approved By Contact Person Council Senior Business Development Advisor 1 This policy provides
New Zealand. Standards for. Critical Care. Nursing Practice
 New Zealand Standards for Critical Care Nursing Practice New Zealand Standards for Critical Care Nursing Practice Critical Care Nurses Section New Zealand Nurses Organisation Reproduction of material 2014
New Zealand Standards for Critical Care Nursing Practice New Zealand Standards for Critical Care Nursing Practice Critical Care Nurses Section New Zealand Nurses Organisation Reproduction of material 2014
Clinical Research Nurse Position Description
 Date: September 2015 Job Title : Clinical Research Nurse Department : Haematology Research Unit General Medicine & Older People Location : North Shore Hospital Reporting To : Operationally to: Operations
Date: September 2015 Job Title : Clinical Research Nurse Department : Haematology Research Unit General Medicine & Older People Location : North Shore Hospital Reporting To : Operationally to: Operations
REQUEST FOR PROPOSAL FOR POLICE OPERATIONS STUDY. Police Department CITY OF LA PALMA
 REQUEST FOR PROPOSAL FOR POLICE OPERATIONS STUDY Police Department CITY OF LA PALMA Released on November 27, 2013 Police Operations Study REQUEST FOR PROPOSAL ( RFP ) 1. BACKGROUND The City of La Palma
REQUEST FOR PROPOSAL FOR POLICE OPERATIONS STUDY Police Department CITY OF LA PALMA Released on November 27, 2013 Police Operations Study REQUEST FOR PROPOSAL ( RFP ) 1. BACKGROUND The City of La Palma
National Competency Standards for the Registered Nurse
 National Competency Standards for the Registered Nurse INTRODUCTION DESCRIPTION OF REGISTERED NURSE DOMAINS NATIONAL COMPETENCY STANDARDS GLOSSARY OF TERMS Introduction The Australian Nursing and Midwifery
National Competency Standards for the Registered Nurse INTRODUCTION DESCRIPTION OF REGISTERED NURSE DOMAINS NATIONAL COMPETENCY STANDARDS GLOSSARY OF TERMS Introduction The Australian Nursing and Midwifery
BOARD OF FINANCE REQUEST FOR PROPOSALS FOR PROFESSIONAL AUDITING SERVICES
 TOWN OF KILLINGWORTH BOARD OF FINANCE REQUEST FOR PROPOSALS FOR PROFESSIONAL AUDITING SERVICES DATE: February 14, 2018 1 I. INTRODUCTION A. General Information The Town of Killingworth is requesting proposals
TOWN OF KILLINGWORTH BOARD OF FINANCE REQUEST FOR PROPOSALS FOR PROFESSIONAL AUDITING SERVICES DATE: February 14, 2018 1 I. INTRODUCTION A. General Information The Town of Killingworth is requesting proposals
TRAINEE CLINICAL PSYCHOLOGIST GENERIC JOB DESCRIPTION
 TRAINEE CLINICAL PSYCHOLOGIST GENERIC JOB DESCRIPTION This is a generic job description provided as a guide to applicants for clinical psychology training. Actual Trainee Clinical Psychologist job descriptions
TRAINEE CLINICAL PSYCHOLOGIST GENERIC JOB DESCRIPTION This is a generic job description provided as a guide to applicants for clinical psychology training. Actual Trainee Clinical Psychologist job descriptions
LOCAL SPORT DEFIBRILLATOR GRANT PROGRAM GUIDELINES OPENING: 1 NOVEMBER 2017 CLOSING: 20 DECEMBER 2017
 LOCAL SPORT DEFIBRILLATOR GRANT PROGRAM GUIDELINES OPENING: 1 NOVEMBER 2017 CLOSING: 20 DECEMBER 2017 2 CONTENTS MINISTER S INTRODUCTION ABOUT THE PROGRAM FUNDING AVAILABLE WHO IS ELIGIBLE TO APPLY? WHAT
LOCAL SPORT DEFIBRILLATOR GRANT PROGRAM GUIDELINES OPENING: 1 NOVEMBER 2017 CLOSING: 20 DECEMBER 2017 2 CONTENTS MINISTER S INTRODUCTION ABOUT THE PROGRAM FUNDING AVAILABLE WHO IS ELIGIBLE TO APPLY? WHAT
Registered Midwife. Location : Child Women and Family Division North Shore and Waitakere Hospitals
 Date: November 2017 Job Title : Registered Midwife Department : Maternity Service Location : Child Women and Family Division North Shore and Waitakere Hospitals Reporting To : Charge Midwife Manager for
Date: November 2017 Job Title : Registered Midwife Department : Maternity Service Location : Child Women and Family Division North Shore and Waitakere Hospitals Reporting To : Charge Midwife Manager for
Medical revalidation: three countries, three approaches
 Medical revalidation: three countries, three approaches The UK experience Professor Jenny Simpson OBE Clinical Director, Revalidation NHS England Background The initial thinking about revalidation in the
Medical revalidation: three countries, three approaches The UK experience Professor Jenny Simpson OBE Clinical Director, Revalidation NHS England Background The initial thinking about revalidation in the
Policies and Procedures for In-Training Evaluation of Resident
 Policies and Procedures for In-Training Evaluation of Resident First Edition Dec. 2013 This policy and procedure was approved by the Board of Trustee of Kuwait Institute for Medical Specialization (KIMS)
Policies and Procedures for In-Training Evaluation of Resident First Edition Dec. 2013 This policy and procedure was approved by the Board of Trustee of Kuwait Institute for Medical Specialization (KIMS)
Statement of Guidance: Outsourcing Regulated Entities
 Statement of Guidance: Outsourcing Regulated Entities 1. STATEMENT OF OBJECTIVES 1.1 This Statement of Guidance ( Guidance ) is intended to provide guidance to regulated entities on the establishment of
Statement of Guidance: Outsourcing Regulated Entities 1. STATEMENT OF OBJECTIVES 1.1 This Statement of Guidance ( Guidance ) is intended to provide guidance to regulated entities on the establishment of
Montgomery Housing Authority 525 South Lawrence Street Montgomery, Alabama REQUEST FOR PROPOSALS RFP WEBSITE DEVELOPMENT AND REDESIGN
 Montgomery Housing Authority 525 South Lawrence Street Montgomery, Alabama 36104 REQUEST FOR PROPOSALS RFP 2017-04 WEBSITE DEVELOPMENT AND REDESIGN DATE ISSUED: September 29, 2017 TYPE OF PROJECT: CONTACT
Montgomery Housing Authority 525 South Lawrence Street Montgomery, Alabama 36104 REQUEST FOR PROPOSALS RFP 2017-04 WEBSITE DEVELOPMENT AND REDESIGN DATE ISSUED: September 29, 2017 TYPE OF PROJECT: CONTACT
Clinical Nurse Specialist Cardiac Rehabilitation & Heart Failure
 Date: November 2014 Job Title : Clinical Nurse Specialist Cardiac Rehabilitation and Heart Failure Department : Cardiology Location : North Shore and Waitakere sites Reporting To : Cardiology Operations
Date: November 2014 Job Title : Clinical Nurse Specialist Cardiac Rehabilitation and Heart Failure Department : Cardiology Location : North Shore and Waitakere sites Reporting To : Cardiology Operations
Programme title: Foundation Degree Science Nursing Associate (Apprenticeship)
") Faculty of Health Studies School of Nursing and Healthcare Leadership Programme Specification Programme title: Foundation Degree Science Nursing Associate (Apprenticeship) Academic Year: 2017/2018 Degree
Faculty of Health Studies School of Nursing and Healthcare Leadership Programme Specification Programme title: Foundation Degree Science Nursing Associate (Apprenticeship) Academic Year: 2017/2018 Degree
MPI Grants Portal. Getting Started Guide. Vet Bonding Scheme
 MPI Grants Portal Getting Started Guide Vet Bonding Scheme Issue Date: January 2016 Contents 1. About this document... 3 2. Overview of the Vet Bonding Scheme... 4 3. Overview of the Grants Portal... 6
MPI Grants Portal Getting Started Guide Vet Bonding Scheme Issue Date: January 2016 Contents 1. About this document... 3 2. Overview of the Vet Bonding Scheme... 4 3. Overview of the Grants Portal... 6
Application for registration within a vocational scope of practice
 Application for registration within a vocational scope of practice VOC3 Aug 2017 For doctors who hold a postgraduate medical qualification which is not the prescribed New Zealand or Australasian postgraduate
Application for registration within a vocational scope of practice VOC3 Aug 2017 For doctors who hold a postgraduate medical qualification which is not the prescribed New Zealand or Australasian postgraduate