The PCMH St Joseph s Experience
|
|
|
- Darcy Powell
- 6 years ago
- Views:
Transcription


1 The PCMH St Joseph s Experience Priya Radhakrishnan, MD Roshni Kundranda, MD, MSPH Binh Doung, DO Jenni Schroeder, RN, BSN ACP Regional Meeting Tucson, 2013
2 Disclosure No financial conflicts of interest 2
3 My dogs Have a pet portal Online method of contacting for refills Gets a call one day and one week after illness

4 What is a Medical Home? The Patient-Centered Medical Home (PCMH) is an approach to providing comprehensive primary care for children, youth and adults. The PCMH is a health care setting that facilitates partnerships between individual patients, and their personal physicians, and when appropriate, the patient s family - Joint Principles of the Patient Centered Medical Home, Feb
5 Joint Principles Personal Physician- ongoing relationship with a physician to provide continuous and comprehensive care Physician directed medical practice- team of individuals take responsibility for ongoing care of patients Whole person orientation -responsible for care or for arranging for care for all healthcare needs Care is coordinated and integrated- across health care systems e.g. hospitals, nursing homes, and community based services by registries, IT etc, Quality and safety- with EBM, shared decision making, point of care support, voluntary reporting Enhanced access through open scheduling, expanded hours, other options for communication Team Based Care -NP/PA - RN/LPN -MA -Front office -Back office -Care coordinator -Social worker -Nutritionist/Educator -Pharmacist -Behavioral health -Others Payment- supported by structures that recognizes services and value 5
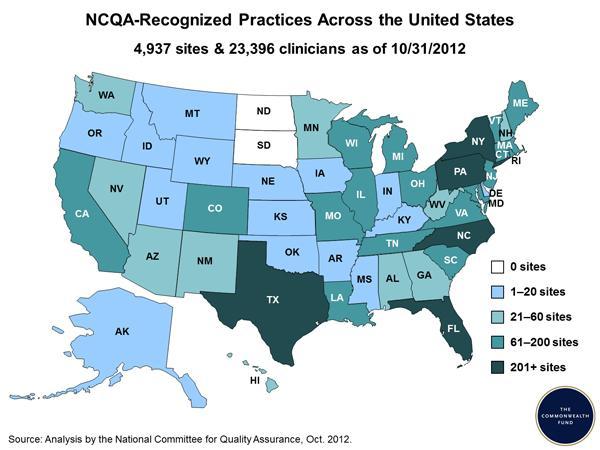
6 Update on Medical Homes As of June 2013, more than 5,700 practices and 26,000 physicians have been designated by NCQA as medical homes Nationwide, >90 commercial health plans, 42 state Medicaid programs, federal agencies and the military have adopted the PCMH on varying scales. PCMH is projected to save $189 billion nationally over the next 10 years 6
7 7
8 Background St. Joseph s Hospital and Medical Center is a 667 bed quaternary hospital in downtown Phoenix The internal medicine clinic is a combined resident and faculty run practice (9 faculty physicians and NP; 35 residents and students) 80 % of patients served have one or more chronic disease Non-emergent ER visits comprise about % of all ER visits By payer, AHCCCS accounts for 51.6 % of all ER visits The clinic averages about 100 patients a day, with 40 % of patients having 3 or more chronic conditions 8
9 Before Medical Home Paper charts Lack of access to patient information 90% post hospitalized patients- no information Lack of data re: health care costs Lack of data re: use of preventive services Access- next available appt follow up- 2 weeks- 2 months Physicians did it all Reactive- patient presents 9
10 Transformation 10
11 Transformation Physicians, RN, Practice Manager Rapid cycle PDSA Increased daily open access, evening hours, Saturday hours EMR implementation Process and Policy Updates in line with NCQA standards Ambulatory information registry Partnership with Mercy Care Plan, 2011 Evaluation of Practice Metrics Patient Advisory Council Care Coordinator- NCQA training Weekly meetings with Core Team NCQA certification December




12 Partnership with Mercy Care Plan Care coordinator Monthly meetings Information on members- ED visits/ inpatient admissions, disease based metrics, SMI, controlled substance prescribing Preferential assignment of patients to the medical home Higher payment per member for care coordination and bonuses based on quality metrics achieved 12
13 Transformation Weekly Meetings With Core Team / Evaluation of Practice Metrics PCMH Core Team: 1. Practice Manager 2. 3 Faculty Providers 3. PCMH Care Coordinator Weekly Meetings: 1. Initial evaluation of practice compared to PCMH 2011 Standards - What was currently being done was not always what the team thought was being done 2. Discussed/revised policies & procedures - Small workgroups including members of the practice were formed 3. Worked with Allscripts (EMR) and Ambulatory Information Management (AIM) to determine tracking and documentation capabilities 4. Developed quality improvement projects 13
14 Transformation Process and Policy Updates in Line With NCQA Standards Written policies and procedures are required for many elements within the PCMH 2011 standards Developed, or re-wrote, 23 policies to comply with the PCMH standards Written by PCMH Care Coordinator Approved by core PCMH team Signed by medical director Educated staff/providers/residents of policies and procedures Staff meetings s Huddles 14
15 Transformation Rapid Cycle PDSA: Plan-Do-Study-Act Four-stage problem-solving model used for improving a process or carrying out change: * Stage 1: Plan Identify an opportunity, and plan for improvement Stage 2: Do Start carrying out your plan Stage 3: Study Examine your results Stage 4: Act Continue to examine and re-examine your process using the PDSA cycle, by standardizing the improvement or developing a new theory, and establishing future plans * 15
16 Transformation Rapid Cycle PDSA: Plan-Do-Study-Act Access to Care: Can we improve patient satisfaction by offering same-day (urgent) appointments? 2 month project: 11.49% Tdap Immunizations in Diabetic Patients: Can we increase the number of diabetics that receive the Tdap immunizations? 1 month project: 11.7% Pneumonia Vaccine in Older Adults: Can we increase the number of older adults that receive the pneumonia vaccine? 1month project: 13.46% ED Visits: Can we increase the number of patients that are seen in the clinic following a visit to the emergency department? First month: 69% (Did not meet goal of 75%) Second month: 78% (Goal met!) 16

17 Transformation Increased Daily Open Access Two time slots per provider, per session, are maintained for same day appointments for urgent and non-urgent medical issues. The chart below demonstrates to NCQA how our practice was able to provide same-day appointments, which provides patients with access to routine/urgent care appointments. 17

18 Transformation Saturday Hours Extended hours appointments are available on Saturday from 8 AM to 12 noon Patients were notified of the available extended hours through the hospital internet system and flyers and brochures that are posted in the lobby of the Internal Medicine Health Center 18

19 Transformation Evening Hours Extended hour appointments have been available since August 6, 2012 Currently offered Monday through Wednesday from 5 PM to 7 PM. Patients were notified of the available extended hours through the hospital internet system and flyers and brochures that are posted in the lobby of the Internal Medicine Health Center 19
20 Transformation Ambulatory Information Management (AIM) Available through Allscripts (EMR) Registries: COPD, Diabetes, Asthma, Congestive Heart Failure (CHF), Coronary Artery Disease Preventive Screenings: Mammograms, Colonoscopies, Flu Vaccine Patient Information: DOB, Ethnicity, Addresses Clinical Data: Problem List, Allergies, Height/Weight, Smoking Status 20
21 Transformation Ambulatory Information Management Use Data for Population Management: - Preventive care services: Mammograms, Pneumovax >65 years and diabetics - Chronic care services (diabetic patients): HgbA1c, Lipids, Eye Exam, Pneumonia Vaccine, Foot Exam, Urine Microalbumin - Patients not seen in >1 year - Patients on specific medications: Coumadin 21
22 Transformation Patient Advisory Council SJHMC Internal Medicine Patient Advisory Council is a group of committed patients, caregivers, healthcare providers and staff who work together as active partners to improve the healthcare experience Mission Statement: Working to create patient-centered care through the voice of our patients Vision Statement: An innovative healthcare community that will respectfully and compassionately listen, learn and communicate with patients and their families to create safe, high-quality care What have they done? Produced an educational/informative DVD for the waiting room Developed a pre-appointment questionnaire Write articles for quarterly newsletter Update bulletin boards in the clinic Review patient satisfaction survey 22
23 Outcomes PCMH 1: Enhanced access and continuity Enhanced open access Every patient has an assigned PCP preferably at the first appointment Team based approach to maintain continuity of care (max 3 different providers) 30 minute time frame to return calls after hours and improved documentation of advice given in the EMR Reduction in ED visits and inpatient admissions 23
24 % of Calls that Meet Policy Documentation of After Hour Calls in the EMR 100% Provider Performance for After Hour Calls 90% 80% 70% 60% 50% 40% YES NO 30% 20% 10% 0%


25 ED Visits/k 01/01/ /31/2012 Perfomance for ED visits per ,800 1,600 1,645 1,400 1,257 1,200 1,101 1,155 1,117 1, Baseline Q1 Jan-Mar Q2 Apr-Jun Q3 Jul-Sep Q4 Oct-Dec Annual Performance Period 25

26 ED Visits/k 01/01/ /31/2012 Perfomance for IP Visits per Baseline Q1 Jan-Mar Q2 Apr-Jun Q3 Jul-Sep Q4 Oct-Dec Annual Performance Period 26


27 Outcomes ED visits Inpatient admissions 32 % 29 % 27
28 Outcomes PCMH 2: Identify and manage patient populations >90% of patients provided clinical summary of visit Currently managing Diabetes, Coumadin, preventive screenings Identifying patient s who have not been seen in the practice for > 1 year and calling them for appointments 28
29 Outcomes PCMH 3:Plan/Manage Care Development of templates/care guides in EMR which are evidence based. Registry data collection is based on evidence based guidelines Now able to identify patients who are high risk- based on chronic conditions, polypharmacy, age, insurance, controlled substance use, SMI, ED visits (from registry + MCP data) 40% of our practice is high risk 14-25% of patients from MCP are high risk Individualized plan for high risk, high utilizers- intensive care co-ordination Medication reconciliation January 1, 2013 June 30, % July 1, 2013 September 23, % 29
30 Outcomes PCMH 4: Provide Self Care Support/ Community Resources Increased ability to connect patient s with community based services Diabetes group visits, on site monthly CDE classes Increase in counseling documentation 30
31 Outcomes PCMH 5: Track and coordinate care Daily reports on ED visits from St. Joseph s Hospital and Banner First contact within 48 hours after ED visit or inpatient admission, and appointment within 7-14 days Transitional care visits Actively track referrals and obtain consultation reports 31
32 Outcomes PCMH 6: Measure/Improve Performance Comment cards in the rooms Patient survey Individual provider quality metrics 32
33 Implications Medical home yields results with significant investment Physician and practice adoption is a major challenge Care coordination is key Health information technology is essential Ability to populate and manage registries One size does not fit all Long term sustainability and maintenance of certification 33
34 Collateral Projects Population based curriculum QI projects for residents Active management of registries Patient portal E-visits Partnership with more health care plans Coordinating PCMH efforts across St. Joseph s primary care sites to ensure long term sustainability of all practices 34
35 Resources for Practices Benefits or Implementing the Primary care Patient- Centered Medical Home: A review of cost and quality results, 2012: Nielsen, M, Langner, B, Zema, C, Hacker, C,Grundy P 35

36 IMPACT 36
37 What do we need to change? Think Systems not individual Build resilience Teams HIT champions Systems change champions 37

38 If my dog can have coordinated care I deserve it too
39 Acknowledgements Brett Mcclain, CEO SJMG William Ellert, MD, CMO SJMG Mercy Care Plan Jo Barone, RN Veena Dhillon, Manager IMHC Cynthia ( Kim) Phan Rachita Gupta 39


40 Thank you
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
2017 HIMSS DAVIES APPLICANT
 2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
Setting Your QI Goals
 Question What data sources will you use to identify a performance gap in your practice? (Examples: performance measure data in a registry, PQRS report, performance measure calculated from patient records
Question What data sources will you use to identify a performance gap in your practice? (Examples: performance measure data in a registry, PQRS report, performance measure calculated from patient records
Presbyterian Healthcare Services Care Management
 Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
HPV Vaccination Quality Improvement: Physician Perspective
 HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Patient-centered care - from buzz word to meaningful reality. Current Health Care System
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System Traditionally, this is the only part of the health care system that is
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
meaningful reality Katie Coleman, MSPH
 Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
Patient-centered care - from buzz word to meaningful reality Katie Coleman, MSPH David K. McCulloch MD Current Health Care System T diti ll thi i th l Traditionally, this is the only part of the health
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
CHC-A Continuity Dashboard. All Sites Continuity - Asthma. 2nd Qtr-03. 2nd Qtr-04. 2nd Qtr-06. 4th Qtr-03. 4th Qtr-06. 3rd Qtr-04.
 PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
2017 HIMSS DAVIES APPLICANT
 2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Diabetes. Evidence Based/ Team Based Care in a Community Health Center ---
 Diabetes Evidence Based/ Team Based Care in a Community Health Center --- Sharon Mulvehill MD North Texas Area Community Health Center August 23, 2014 The Challenges Busy schedules, little time for system
Diabetes Evidence Based/ Team Based Care in a Community Health Center --- Sharon Mulvehill MD North Texas Area Community Health Center August 23, 2014 The Challenges Busy schedules, little time for system
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
Core Item: Clinical Outcomes/Value
 Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home Domains of Function. Interpretive Guidelines
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
The Pennsylvania Chronic Care Initiative
 The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
The Pennsylvania Chronic Care Initiative Richard L. Snyder, M.D. Senior Vice President Chief Medical Officer Independence Blue Cross William J. Warning II, M.D. Program Director Crozer-Keystone Family
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
University of Cincinnati Patient Centered Medical Home Leadership Decisions
 University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
University of Cincinnati Patient Centered Medical Home Leadership Decisions Eric J. Warm M.D., F.A.C.P. Program Director, Internal Medicine Associate Professor of Medicine University of Cincinnati College
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Piedmont Access to Health Services. Standing Orders for Patient Work-ups
 Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Referrals, Prior Authorizations, Medical Management, and Appeals
 Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Finding Progress on Timely Access Issues
 Finding Progress on Timely Access Issues Bill Barcellona SVP for Government Affairs, CAPG L. Gordon Moore, MD Senior Medical Director, 3M Health Data Science Group Dan Southard Deputy Director, Office
Finding Progress on Timely Access Issues Bill Barcellona SVP for Government Affairs, CAPG L. Gordon Moore, MD Senior Medical Director, 3M Health Data Science Group Dan Southard Deputy Director, Office
Disclosures. Learning Objectives 4/26/2017. Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic
 Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Improving HPV Vaccination Rates in a Large Pediatric Practice: Implementing Effective Quality Improvement
 Improving HPV Vaccination Rates in a Large Pediatric Practice: Implementing Effective Quality Improvement Alix Casler, M.D., F.A.A.P. Chief of Pediatrics, Medical Director of Pediatrics Orlando Health
Improving HPV Vaccination Rates in a Large Pediatric Practice: Implementing Effective Quality Improvement Alix Casler, M.D., F.A.A.P. Chief of Pediatrics, Medical Director of Pediatrics Orlando Health
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
College-wide Patient-Centered Medical Home Program Meharry Medical College
 + The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
+ The Key Elements: Using the Patient Centered Medical Home Model in Inter-Professional Education and Training Medical, Dental, and Public Health Education Curriculum Transformation Primary Care Residency
Transition from Hospital to Home: Importance of Medication Education and Reconciliation
 Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles. November 12, Wisconsin Council on Medical Education & Workforce
 A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles Wisconsin Council on Medical Education & Workforce November 12, 2015 Kathy Kerscher, Team Leader Primary Care Rob MacNeil, Sr.
A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles Wisconsin Council on Medical Education & Workforce November 12, 2015 Kathy Kerscher, Team Leader Primary Care Rob MacNeil, Sr.
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
PACT: The VA s Medical Home
 A5/B5 This presenter has nothing to disclose PACT: The VA s Medical Home What is working to change a big system Mike Davies, MD Director VA Systems Redesign Rich Stark, MD Director VA Primary Care Operations
A5/B5 This presenter has nothing to disclose PACT: The VA s Medical Home What is working to change a big system Mike Davies, MD Director VA Systems Redesign Rich Stark, MD Director VA Primary Care Operations
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018
 Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
Prescription Synchronization. Patient Care Services Pearls Part 1. Beverly A. Morrow, BS, Pharm D Madigan-Puyallup Community Based Medical Home
 CPE Information and Disclosures Patient Care Services Pearls Part 1 Beverly A. Morrow, BS, PharmD Jennifer L. Evans, PharmD, BCACP, C-TTS LT Jeannie Hong USPHS Robin John, RPh, CDE Beverly A. Morrow, Jennifer
CPE Information and Disclosures Patient Care Services Pearls Part 1 Beverly A. Morrow, BS, PharmD Jennifer L. Evans, PharmD, BCACP, C-TTS LT Jeannie Hong USPHS Robin John, RPh, CDE Beverly A. Morrow, Jennifer
West Valley and Central Valley Care Coordination Coalitions
 West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
West Valley and Central Valley Ettie Lande, MS, BSN, ACM-RN February 08, 2018 Thank You! For sponsoring today s breakfast AstraZeneca and Cyndi Black If you can sponsor breakfast at an upcoming community
Reducing Hospital Readmissions: Home Care as the Solution
 Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Reducing Hospital Readmissions: Home Care as the Solution Kathy Duckett RN, BSN Sutter Center for Integrated Care ducketk@sutterhealth.org www.suttercenterforintegratedcare.org Learning Objectives 1 Review
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
New Models of Health Care: The Patient Centered Medical Home. Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013
 New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
New Models of Health Care: The Patient Centered Medical Home Mark Gwynne, DO UNC- Chapel Hill Department of Family Medicine August 17, 2013 Objectives of this session: What s the burning platform for change?
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
History of Pennsylvania s Chronic Care Initiative
 History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
History of Pennsylvania s Chronic Care Initiative Pennsylvania Chronic Care Burden In 2007, government and healthcare leaders in Pennsylvania were reaching a growing consensus that some form of action
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals
 Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In?
 Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
Patient-Centered Medical Home: What Is It and How Do SBHCs Fit In? Sue Sirlin, CPEHR Director, HIT Consulting Services Bonni Brownlee, MHA CPHQ CPEHR Principal Consultant March 15, 2013 Advancing Healthcare
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
Meaningful Use Stage 1 Guide for 2013
 Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year
 A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Secrets for Performance Improvement with Data Driven Practice Transformation. Jessica Henderson Boyd, MD, MPH Chief Medical Officer
 Secrets for Performance Improvement with Data Driven Practice Transformation Jessica Henderson Boyd, MD, MPH Chief Medical Officer The Story Introduction to BMS Role of leadership Strategic alignment DRVS
Secrets for Performance Improvement with Data Driven Practice Transformation Jessica Henderson Boyd, MD, MPH Chief Medical Officer The Story Introduction to BMS Role of leadership Strategic alignment DRVS
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
California s Health Homes Program
 California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Medication Trauma Crisis: Primary Care Innovations. Session Code: D25, E25
 Medication Trauma Crisis: Primary Care Innovations Session Code: D25, E25 Speakers and Disclosures Speaker James Slater, PharmD Executive Pharmacy Director, CareOregon Kristen Benkstein, PharmD Pharmacy
Medication Trauma Crisis: Primary Care Innovations Session Code: D25, E25 Speakers and Disclosures Speaker James Slater, PharmD Executive Pharmacy Director, CareOregon Kristen Benkstein, PharmD Pharmacy
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Using the BaldrigeCriteria to Achieve High Reliability
 Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
The Triple Aim. Productivity: Digging Deep Enough 11/4/2013. quality and satisfaction); Improving the health of populations; and
; Improving the health of populations; and") NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model. ACO Congress November 5, 2013 Charles Kennedy
 Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
PROVIDER. Newsletter BETTER QUALITY IS OUR GOAL IN THIS ISSUE MEDICARE 2015 ISSUE II
 MEDICARE 2015 ISSUE II PROVIDER Newsletter BETTER QUALITY IS OUR GOAL Our Quality Improvement (QI) program is dedicated to finding ways to help deliver better care and service to our members, in collaboration
MEDICARE 2015 ISSUE II PROVIDER Newsletter BETTER QUALITY IS OUR GOAL Our Quality Improvement (QI) program is dedicated to finding ways to help deliver better care and service to our members, in collaboration
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
JMOC Update: Behavioral Health Redesign. March 16 th, 2017
 JMOC Update: Behavioral Health Redesign March 16 th, 2017 Ohio Medicaid Behavioral Health Redesign Initiative The Redesign Initiative is an integral component of Ohio s comprehensive strategy to rebuild
JMOC Update: Behavioral Health Redesign March 16 th, 2017 Ohio Medicaid Behavioral Health Redesign Initiative The Redesign Initiative is an integral component of Ohio s comprehensive strategy to rebuild
Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement
 Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas Health System Improvement Workforce Payment System Health Information Technology Insurance
Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas Health System Improvement Workforce Payment System Health Information Technology Insurance
The SOMC Employee Wellness Program
 The SOMC Employee Wellness Program A Focus on Results Not Participation Pike County Health Coalition Julie Thornsberry, RN, BSN Manager Employee Health & Wellness What are today s objectives? Identify
The SOMC Employee Wellness Program A Focus on Results Not Participation Pike County Health Coalition Julie Thornsberry, RN, BSN Manager Employee Health & Wellness What are today s objectives? Identify
Paving the Way for. Health Homes
 Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Practice Report Out. Western Slope CPC Practices
 Practice Report Out Western Slope CPC Practices Aspen Internal Medicine Consultants Ricci Bickling, Quality Improvement Specialist 2 Providers 8 Staff EMR: GE Centricity 1755 Active Patients Aspen Area
Practice Report Out Western Slope CPC Practices Aspen Internal Medicine Consultants Ricci Bickling, Quality Improvement Specialist 2 Providers 8 Staff EMR: GE Centricity 1755 Active Patients Aspen Area
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Performance Incentives in the Southern California Permanente Medical Group (SCPMG):
:") Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org