Care Management in the Patient Centered Medical Home. Self Study Module
|
|
|
- May Scott
- 6 years ago
- Views:
Transcription

1 Care Management in the Patient Centered Medical Home Self Study Module

2 Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management process
3 What is a Care Management Program? Care management programs apply systems, science, incentives, and information to improve medical practice and assist consumers and their support system to become engaged in a collaborative process designed to manage medical/social/mental health conditions more effectively. reference:
4 Goals of Care Management Enhance coordination of care Minimize fragmentation of care Improve patient s functional health status Eliminate duplication of services Reduce the need for unnecessary, costly medical services
5 Features of Successful Care Management Models Close collaboration between Care Manager and Primary Care Physician (PCP) High level of in-person contact between care manager and patient Close attention to transitions of care Handoffs are where many errors occur Need timely information on hospital/snf discharges Medication reconciliation is regularly performed Need access to patient record/ehr Assess adherence to medication regimens Target patients at high risk for hospitalization or ED use reference:
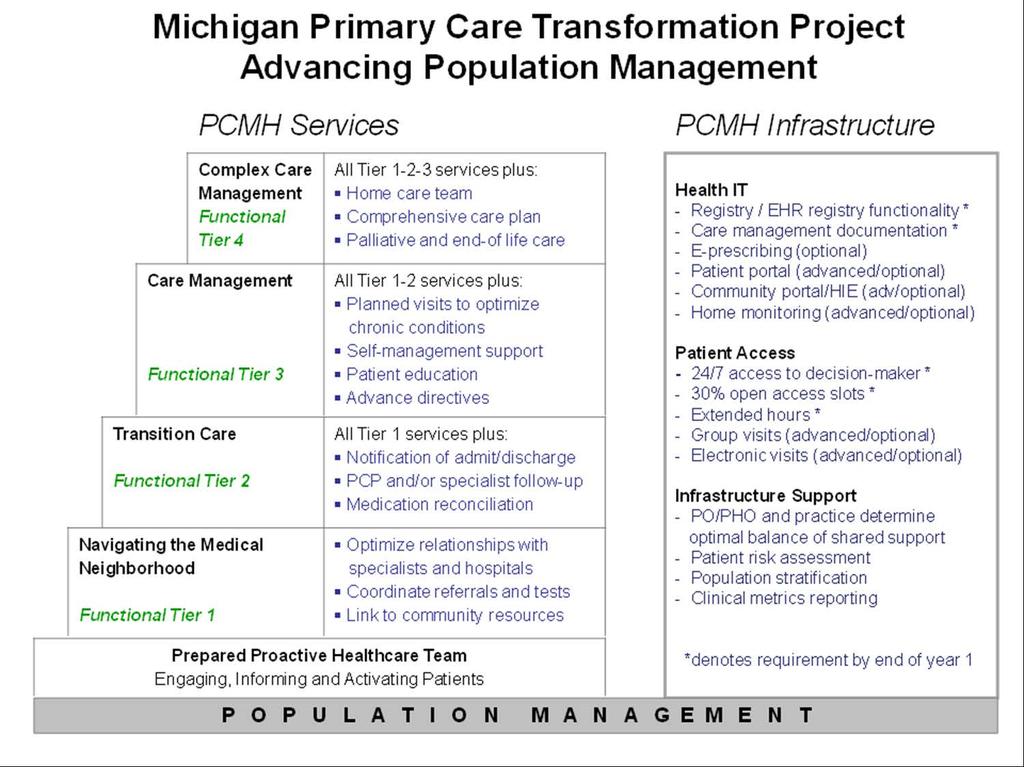
6 CASE STUDY MICHIGAN PRIMARY CARE TRANSFORMATION (MIPCT) BACKGROUND AND CARE MANAGEMENT INTERVENTION
7 CMS Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration Centers for Medicare & Medicaid Services (CMS) is exploring the role of the PCMH in improving US health care Participating in state-based PCMH demonstrations CMS Demo Stipulations Must include Commercial, Medicaid, Medicare patients Must be budget neutral over 3 years of project Must improve cost, quality, and patient experience 8 states selected for participation, including Michigan Michigan start date: January 1,
8 The Vision for a Multi-Payer Model Use the CMS Multi-Payer Advanced Primary Care Practice demo as a catalyst to redesign MI primary care Multiple payers will fund a common clinical model Allows global primary care transformation efforts Support development of evidence-based care models Create a model that can be broadly disseminated Facilitate measurable, significant improvements in population health for our Michigan residents Bend the current (non-sustainable) cost curve Contribute to national models for primary care redesign Form a strong foundation for successful ACO models
9 MiPCT Focus Areas Include Care Management Self-Management Support Care Coordination Linkages to Community Services
10

11 MiPCT Payers, Patients and Providers As of March 2015: 1814 providers 1,577 physicians 237 mid-level providers Over 500 care managers 346 PCMH practices 1,158,650 members # Patients % Patients Medicare 186, % Medicaid 214, % BCBSM 361, % BCN 275, % Priority Health 119, % Total 1,158, %
12 MiPCT Demonstration Timeline Original Demonstration Period 1/1/12 12/31/14 Demonstration Two Year CMS Extension 12/31/16 Post-Demo MiPCT GOAL: To sustain our gains (effective, efficient teambased care with embedded Care Managers) postdemonstration period
13 MiPCT Care Management Priorities Care Managers work in close proximity to PCP team - In PCP office as much as possible - Work with PCP team to meet their needs - Evidence supports this model as superior to vendor-based Ensure Complex Care Management coverage - Manage high-complexity, high-cost patients - Patients selected based on risk score plus PCP input Focus on evidence-based interventions - Medication reconciliation - Care transitions - In-person contact with patients whenever possible - Comprehensive care plan for complex patients
14 Care Management Care management is defined as a collaborative process of assessment, planning, facilitation, care coordination, evaluation, and advocating for options and services to meet an individual s health needs through communication and available resources to promote quality cost effective outcomes. reference: Care Management Society of America definition of care management
15 Case Management Society of America Guiding Principles Care Management is a patient-centric, collaborative partnership approach Facilitate self-care Comprehensive, holistic approach Practice cultural competence Use of evidence-based care Promote optimal patient safety Promote integration of behavioral change science and principles Link with community resources Assist with navigating the health care system
16 Functions of a Care Manager Partners with primary care practice leadership to integrate care management into the practice Assesses healthcare, educational, and psychosocial needs of patient/family Provides self management support empower patient/family Provides patient family education teach back Implements evidence based care Close gaps in care; addresses prevention, chronic conditions Assists with transitions between settings Assists with advanced directives, End of life care Completes Comprehensive Assessment, Creates and maintains individualized plan of care follow up visits, longitudinal
17 Managing Populations: Stratified approach to patient care and care management IV. Most complex (e.g., Homeless, Schizophrenia) <1% of population Caseload III. Complex Complex illness Multiple Chronic Disease Other issues (cognitive, frail elderly, social, financial) 3-5% of population Caseload II. Mild-moderate illness Well-compensated multiple diseases Single disease 50% of population Caseload~1000 I. Healthy Population
.")
18 Ramsay, Rebecca (2011). Implementing Effective Clinical Care Management; Building Care Management Capacity within a Transforming Primary Care System, Care Oregon (PowerPoint slides). Retrieved from shttp:// Rebecca (2011). Implementing Effective Clinical Care Management; Building Care Management Capacity within a Transforming Primary Care System, Care Oregon 20 Care Management Continuum:
19 Care Management Delivery Team Based Care Example of the Care Management Team in the Primary Care Office Care Manager RN, NP, PA, LMSW care manager who has responsibility for the care management of a patient in partnership with the patient s Primary Care Physician Other Health Care Professionals may include licensed practical nurse, certified diabetes educator, registered dietician, masters of science trained nutritionist, clinical pharmacist, behavioral health specialist, certified asthma educator, and others
20 Care Management Evidence Based Interventions Relationship-based Communication Transitions of Care across settings Behavior change Motivational Interviewing, Brief Action Planning Self-management Chronic Disease Management, Protocols, & Health Promotion
21 Care Management Process Five Steps: Referral Screening Enrollment Management Closure
22 Referral Physician input Transition of Care Gaps in Care uncontrolled chronic condition(s) Targeted chronic conditions

23 Screening Review the medical record Chronic conditions Psychosocial Utilization Emergency room visits Hospital admissions Underutilization Claims data Condition specific CHF COPD Children with complex needs CHF and COPD are currently at the top of list in terms reducing ED visits and inpatient hospitalizations.
24 Enrollment / Patient Engagement Obtain patient consent Complete initial comprehensive assessment Lessons Learned PCP in person introduction of the care manager to patient/caregiver Helpful tools include* Flyer physician may use to explain the care management program Care Manager phone script *Note access tools here:
25 Management - Interventions Establish an individualized care plan and identify goals Identify any critical care plan needs and initiate action Set short and long term goals Make sure patients/care givers are a part of the plan of care Reinforce patient self-care and self-management Establish on going follow up monitor /adjust care plan
26 Case Closure Examples to consider for case closure: Improved ability to self manage Transfer to hospice care Disenrollment - patient no longer interested in participating in care management An important step - Collaboration and Communication Discuss with PCP prior to closing case
27 Building & Managing a Patient Case Load Design Workflow and Processes to address: Admission Discharge Transfer alerts (ADTs) Referrals to the Care Manager Office team members are aware of criteria for patients who may benefit from care management Multidisciplinary team in the physician office Ability to view the care managers patient schedule Ability to view the individualized patient care plan identify, review and update patient goals Tracking and Monitoring - Data Reports Billing the care manager visits Quality metrics ex. Care manager activity process metrics
28 The Right Care Manager/Patient Ratio? The right care manager / patient ratios will evolve over time The ratios will vary based on your patient population and acuity Care Manager embedded in the practice A common ratio seen in complex care programs is one care manager per 200 commercial patients, or one care manager per highest-acuity patients Analyze the particular needs of your population by looking at top diagnoses Reference: California Quality Collaborative Complex Care Management Toolkit,
29 MiPCT Example - Moderate Risk Care Manager Complex Care Manager Moderate Risk Care Manager (MCM) Complex Care Manager (CCM) Patient Population Patient Caseload Focus of Care Management Duration of Care Management Moderate risk patients identified by registry, PCP referral for proactive and population management. Caseload 500 (approx active patients); one MCM per 5,000 patients. Proactive, population management. Work with patients to optimize control of chronic conditions and prevent/minimize long term complications. Typically a series of 1 to 6 visits High risk patients identified by PCP referral and input, risk stratification, Caseload 150 (approx active patients); one CCM per 5,000 patients. Targeted interventions to avoid hospitalization, ER visits. Ensure standard of care, coordinate care across settings, help patients understand options. Frequency of visits high at times, duration of months

30 Michigan Care Management Resource Center Website micmrc.org Care Management 101 Topics Webinars
31 Michigan Care Management Resource Center Website micmrc.org Care Management 101 is a web based self study opportunity a suggested road map of staged content for the new Care Manager may be utilized to create customized curriculum for selfstudy based on the CM's self-assessment Care managers may identify their areas of strengths and gaps Review CM 101 content to select recorded webinars, tools, resources Access Care Management 101:

32 Michigan Care Management Resource Center Website micmrc.org Topics for Care Managers Include: Advance Care Planning Palliative Care Pediatrics Medication Management Transitions of Care Patient Centered Medical Home & Team Based Care Chronic Conditions Quality and Population Health Management Elderly Population Behavioral Health
33 Thank You! Questions
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project
 Project") The Michigan Primary Care Transformation (MiPCT) Project Sustainability Update May 14, 2014 1 Where We Started Together The Vision for a Multi Payer Model Use the CMS Multi Payer Advanced Primary Care
The Michigan Primary Care Transformation (MiPCT) Project Sustainability Update May 14, 2014 1 Where We Started Together The Vision for a Multi Payer Model Use the CMS Multi Payer Advanced Primary Care
Provider-Delivered Care Management Frequently Asked Questions Revised March 2018
 Provider-Delivered Care Management Frequently Asked Questions Revised March 2018 Table of Contents Section Name Page Background and Participation 2 Reimbursement and Billing 2 Training 5 Eligibility 7
Provider-Delivered Care Management Frequently Asked Questions Revised March 2018 Table of Contents Section Name Page Background and Participation 2 Reimbursement and Billing 2 Training 5 Eligibility 7
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
The Michigan Primary Care Transformation (MiPCT) Project: December PGIP Meeting Update. MiPCT Team December 2, 2011
 Project: December PGIP Meeting Update. MiPCT Team December 2, 2011") 1 The Michigan Primary Care Transformation (MiPCT) Project: December PGIP Meeting Update MiPCT Team December 2, 2011 2 Agenda Introduction MiPCT Participation Care Management Update Funding Update MiPCT
1 The Michigan Primary Care Transformation (MiPCT) Project: December PGIP Meeting Update MiPCT Team December 2, 2011 2 Agenda Introduction MiPCT Participation Care Management Update Funding Update MiPCT
Potential for an additional 5% PDCM-PCP BCBSM Value Based Reimbursement (VBR) onto your Patient Centered Medical Home designation VBR (estimated
 onto your Patient Centered Medical Home designation VBR (estimated") Revised 1/25/2018 1 Potential for an additional 5% PDCM-PCP BCBSM Value Based Reimbursement (VBR) onto your Patient Centered Medical Home designation VBR (estimated average of $4,000 per physician, varies
Revised 1/25/2018 1 Potential for an additional 5% PDCM-PCP BCBSM Value Based Reimbursement (VBR) onto your Patient Centered Medical Home designation VBR (estimated average of $4,000 per physician, varies
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Monarch HealthCare, a Medical Group, Inc.
 Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Monarch HealthCare, a Medical Group, Inc. Accountable Care in the Independent Practice Model June 7, 2010 Jay J. Cohen, MD, MBA President/Chairman Monarch HealthCare Monarch HealthCare, a Medical Group,
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions
 Project Frequently Asked Questions") Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Michigan Primary Care Transformation (MiPCT) Project Frequently Asked Questions Demonstration Design 1. What is the Michigan Primary Care Transformation (MiPCT) Project? The Centers for Medicare and Medicaid
Medicare: 2018 Model of Care Training
 Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Medicare: 2018 Model of Care Training Training Objectives This course will describe how Centene and its contracted providers work together to successfully deliver the duals Model of Care (MOC) program.
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30
 Michigan Primary Care Transformation www. mipct.org Volume 5 Issue 9 September 26, 2016 SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30 Important Dates: MiPCT
Michigan Primary Care Transformation www. mipct.org Volume 5 Issue 9 September 26, 2016 SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30 Important Dates: MiPCT
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Multi-payer G and CPT Care Management Code Summary v7
 Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
PRACTICE FLASH. Important Dates: SAVE THE DATES! MiPCT Regional Annual Summits
 PRACTICE FLASH Michigan Primary Care Transformation www.mipctdemo.org Volume 5 - Issue 3 - March 21, 2016 We can do this together - we can make care better...one patient at a time. SAVE THE DATES! MiPCT
PRACTICE FLASH Michigan Primary Care Transformation www.mipctdemo.org Volume 5 - Issue 3 - March 21, 2016 We can do this together - we can make care better...one patient at a time. SAVE THE DATES! MiPCT
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model. ACO Congress November 5, 2013 Charles Kennedy
 Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30
 Michigan Primary Care Transformation www. mipct.org Volume 5 Issue 9 September 12, 2016 SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30 As the MiPCT transitions
Michigan Primary Care Transformation www. mipct.org Volume 5 Issue 9 September 12, 2016 SIM PCMH/MiPCT Partnership Initiative Application Period - Submission Deadline September 30 As the MiPCT transitions
2014 Model of Care. Provider Training. Molina Medicare _rev_8-14_cab
 2014 Model of Care Provider Training Molina Medicare 2014 5-2013_rev_8-14_cab Course Overview The Model of Care (MOC) is Molina Healthcare s documentation of the CMS directed plan for delivering coordinated
2014 Model of Care Provider Training Molina Medicare 2014 5-2013_rev_8-14_cab Course Overview The Model of Care (MOC) is Molina Healthcare s documentation of the CMS directed plan for delivering coordinated
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community. Stewards of Change June 11, 2013
 An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
California s Health Homes Program
 California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Specialty practices and primary care practices join forces in providing patient centered medical care
 Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
Welcome, Neighbor! Specialty practices and primary care practices join forces in providing patient centered medical care We often hear our patients express their frustration as they navigate among their
March 15, 2017 UCCCN Learning Session - Summary
 March 15, 2017 UCCCN Learning Session - Summary Healthy U Molina Health Choice Utah SelectHealth Pediatric Specialty Learning Session Panelists (Insurers) Liz Armour-Roth, Manager, Care Management Sheila
March 15, 2017 UCCCN Learning Session - Summary Healthy U Molina Health Choice Utah SelectHealth Pediatric Specialty Learning Session Panelists (Insurers) Liz Armour-Roth, Manager, Care Management Sheila
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
A legacy of primary care support underscores Priority Health s leadership in accountable care
 Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Transforming Primary Care in the Adirondack Region of New York State
 Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
Transforming Primary Care in the Adirondack Region of New York State 2013 Southwind Institute October 22, 2013 Karen Ashline, Director Northern Adirondack Medical Home A Division of the Champlain Valley
P.O. FLASH. Important Dates: MiPCT Pediatric Care Manager Summit Fall 2015 Don t Forget to Register!
 P.O. FLASH Michigan Primary Care Transformation www.mipct.org Volume 4 - Issue 14 - August 17 2015 We can do this together - we can make care better...one patient at a time. MiPCT Pediatric Care Manager
P.O. FLASH Michigan Primary Care Transformation www.mipct.org Volume 4 - Issue 14 - August 17 2015 We can do this together - we can make care better...one patient at a time. MiPCT Pediatric Care Manager
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
New Opportunities for Case Management Leadership in our Changing Environment
 New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
A Care Coordination Model for Value-Based Performance Programs
 A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
A Care Coordination Model for Value-Based Performance Programs Richard S. Chung, MD Chief Clinical Officer APS Healthcare 8th National Pay for Performance (P4P) Summit February 20, 2013 Hyatt Regency Hotel,
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Special Needs Plan (SNP) Model of Care Training 2018
 Model of Care Training 2018") Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Special Needs Plan (SNP) Model of Care Training 2018 Table of Contents Training Overview Pg. 1 Denver Health Medical Plan s (HMO SNP) MOC Annual Training Pg. 2 Special Needs Plans (SNPs) Pg. 2 Special
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care
 Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Physician Engagement
 Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Pathways for Successful Accountable Care Organizations: Physician Engagement Thomas Kloos, MD Jim Barr, MD Atlantic ACO & Optimus Healthcare Partners ACO Helping providers Care Better for their patients.
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Blue Cross Blue Shield of Michigan MiPCT/PDCM Reimbursement Policy and Billing Guidelines Commercial
 Purpose Beginning April 1, 2012 BCBSM began accepting and paying claims for Provider Delivered Care Management services delivered by qualified Primary Care Physicians to patients in physician practices
Purpose Beginning April 1, 2012 BCBSM began accepting and paying claims for Provider Delivered Care Management services delivered by qualified Primary Care Physicians to patients in physician practices
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Agenda. ACMA A Strong Base
 New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
New Opportunities for Case Management Leadership in our Changing Environment 2012 ACMA Kentucky/Tennessee Chapter Case Management Conference By: W. June Simmons, MSW, CEO Partners in Care Foundation September
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
4. Regularly participate in PCMH Initiative conference calls, webinars and in-person events.
 1 PHYSICIAN ORGANIZATION (PO) RESPONSIBILITIES The PO is responsible for supporting with implementation of the PCMH Initiative, aiding participating Practices in their development of PCMH capabilities
1 PHYSICIAN ORGANIZATION (PO) RESPONSIBILITIES The PO is responsible for supporting with implementation of the PCMH Initiative, aiding participating Practices in their development of PCMH capabilities
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Molina Medicare Model of Care. Healthcare Services Molina Healthcare 2016
 Molina Medicare Model of Care Healthcare Services Molina Healthcare 2016 MHTPS_MOCTRN_062016 1 Molina s Mission Our mission is to provide quality health services to financially vulnerable families and
Molina Medicare Model of Care Healthcare Services Molina Healthcare 2016 MHTPS_MOCTRN_062016 1 Molina s Mission Our mission is to provide quality health services to financially vulnerable families and
SPECIAL NEEDS PLAN. Model of Care Training
 SPECIAL NEEDS PLAN Model of Care Training WHAT IS A SNP? The Medicare Modernization Act of 2003 established Special Needs Plans (SNP). Centers Plan for Healthy Living (CPHL) participates in two types of
SPECIAL NEEDS PLAN Model of Care Training WHAT IS A SNP? The Medicare Modernization Act of 2003 established Special Needs Plans (SNP). Centers Plan for Healthy Living (CPHL) participates in two types of
Medicare, Managed Care & Emerging Trends
 Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Medicare, Managed Care & Emerging Trends LeadingAge Michigan 2015 Annual Leadership Institute August 12, 2015 Jon Lanczak, Manager Beth Sullivan, Senior Manager Plante Moran, PLLC Overall Theme Healthcare
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Weaving Expanded Roles of the RN into Population Management
 Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training. Reviewed: 03/22/18
 Health Care Homes (HCH) HCH Recertification Training. Reviewed: 03/22/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training Reviewed: 03/22/18 1 Learning Objectives 1. Describe the Health Care Homes legislative criteria as required at
Minnesota Department of Health (MDH) Health Care Homes (HCH) HCH Recertification Training Reviewed: 03/22/18 1 Learning Objectives 1. Describe the Health Care Homes legislative criteria as required at
Model of Care Training
 Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Provider Guide. Medi-Cal Health Homes Program
 Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE
 AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE 1 Road map What is DSRIP (Delivery System Reform Incentive Payments) Integrating the mission of DSRIP & End the Epidemic
AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE 1 Road map What is DSRIP (Delivery System Reform Incentive Payments) Integrating the mission of DSRIP & End the Epidemic
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
OneCare Model of Care
 OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
OneCare Model of Care Note: Content of this course was current at the time it was published. As Medicare policy changes frequently, check with your immediate supervisor regarding recent updates. 2018 Learning
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees
 TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
TECHNICAL ASSISTANCE BRIEF J UNE 2 0 1 2 Low-Cost, Low-Administrative Burden Ways to Better Integrate Care for Medicare-Medicaid Enrollees I ndividuals eligible for both Medicare and Medicaid (Medicare-Medicaid
Medicare: 2017 Model of Care Training 4/13/2017
 Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
Medicare: 2017 Model of Care Training Training Objectives This course will describe how MHS Health Wisconsin Medicare Advantage and its contracted providers work together to successfully deliver the Model
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
CAL MEDICONNECT: Understanding the Health Risk Assessment. Physician Webinar Series
 CAL MEDICONNECT: Understanding the Health Risk Assessment Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for CAPG members. For a general overview of the
CAL MEDICONNECT: Understanding the Health Risk Assessment Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for CAPG members. For a general overview of the
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Lessons Learned in Care Management. Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference
 Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing
Lessons Learned in Care Management Meghan Sheridan, RD, CDE Ohio Association of Community Health Centers 2017 Annual Conference 1 Objectives: Rationale for team-based care model Lessons learned in implementing