Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
|
|
|
- Berenice Robinson
- 5 years ago
- Views:
Transcription







1 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7,
2 Integrated Whole Person Care in Community Behavioral Health Centers Project Goal Immediate: Integrate Primary Care Services into Community Behavioral Health Centers in King County. Long-term: Improve screening rates and access to chronic disease management/primary care services among individuals enrolled in behavioral health services. Deliverables to include: Screening of medical needs and primary care preventive care for individuals enrolled in behavioral health services; Diabetes monitoring for people with diabetes and behavioral health conditions (HbA1c and LDL- C), Diabetes screening for people using antipsychotic medication; Screening and referral for treatment for people with uncontrolled asthma; Antidepressant medication management - acute and continuous phase treatment; Initiation of substance use disorder treatment (1 visit within 14 days) and engagement (initiation and 2 visits within 44 days); Screening for clinical depression and follow up; Follow up after hospitalization for mental illness within 7 and 30 days; and Decrease potentially avoidable ED visits. Focus Populations Individuals with mental health and substance use disorders who are also at risk for or have chronic disease conditions (respiratory and cardiovascular disease including diabetes). Interventions Providers will be responsible for: 1) Having a partnership with and/or co-locating primary care services at behavioral health treatment sites. 2) Providing or facilitating clients with access to an annual physical/well visit (at a minimum) and address in a timely manner physical health concerns (i.e. sick visits) when indicated. 3) Screening all clients seen by the PCP on site for chronic conditions: i.e. hypertension/blood pressure, diabetes/a1c, asthma and height-weight/bmi and/or collaborating with a PCP at another clinic to understand a client s chronic condition(s). 4) Documenting all screening/lab results for both clinical and reporting purposes in the EHR. 5) Working collaboratively with the PCP to ensure referrals to external pre-identified specialists are made for laboratory tests/treatment when indicated.
3 6) Working with the PCP to ensure the full scope of primary care services is available to patients being served at behavioral health site. 7) Arranging for shared documentation to ensure communication about the patient is easily accessible and documented for reporting purposes. Innovations Measurement-based care with validated tools Coordinated, team-based care Stronger linkages to community-based organizations addressing social determinants Metrics Patient Engagement Metric The number of patients receiving primary care services at a Behavioral Health site (Mental Health or Substance Abuse Site) from a Primary Care Provider (PCP, NP, PA working closely with PCP). Clinical Metrics All-Cause Readmission Rate (30 Days) o Among Medicaid beneficiaries age years old, the percent of acute inpatient stays during the measurement year that were followed by an unplanned acute readmission within 30 days. Antidepressant Medication Management o Effective Acute Phase Treatment People 18 and older diagnosed with depression and treated with an antidepressant medication who remained on antidepressant medication during the entire 12-week acute treatment phase. o Effective Continuation Phase Treatment People 18 and older diagnosed with depression and treated with an antidepressant medication who remained on antidepressant medication for at least six months. Child and Adolescents Access to Primary Care Practitioners o The percentage of members 12 months - 19 years of age who had a visit with a primary care provider. Report four separate rates: months of age; 25 months - 6 years of age; 7-11 years of age; years of age. Comprehensive Diabetes Care: Hemoglobin A1c Testing o The percentage of members years of age with diabetes (type 1 and type 2) who had an HbA1c test during the measurement year. Comprehensive Diabetes Care: Medical Attention for Nephropathy o The percentage of members years of age with diabetes (type 1 and type 2) who received a nephropathy screening or monitoring test or had evidence of nephropathy during the measurement period. Comprehensive Diabetes Care: Eye Exam (Retinal) Performed o The percentage of members years of age with diabetes (type 1 and type 2) who had a retinal or dilated eye exam by an eye care professional during the measurement
4 period, or a negative retinal exam (no evidence of retinopathy) in the 12 months prior to the measurement period. *Diabetes Screening for People with behavioral health conditions who are Using Antipsychotic Medication o People age 18 to 64 with mental health or substance use disorders, who were using an antipsychotic medication who had a glucose test or HbA1c test during the measurement year. *Diabetes Monitoring for People with Diabetes and mental health or substance use disorder o People age 18 to 64 with behavioral health conditions and diabetes who had both an LDL-C test and an HbA1c test during the measurement year. *Initiation of Alcohol and Other Drug Dependence Treatment (1 visit within 14 days) o People age 13 and older with a new episode of substance use disorder who initiated treatment through an inpatient SUD admission, outpatient visit, intensive outpatient encounter, or medication assisted treatment (MAT) within 14 days of the index episode. Inpatient Hospital Utilization o For members 18 years and older, the risk-adjusted ratio of observed to expected acute inpatient discharges during the measurement year. Follow up After Emergency Department Visit for Alcohol or Other Drug Dependence o The percent of discharges for members 18 years and older who had a visit to the ED with a primary diagnosis of alcohol or other drug dependence during the measurement year AND who had a follow-up visit with any provider with a corresponding primary diagnosis of alcohol or other drug dependence, reported separately for follow-up within 7 and 30 days after discharge. Follow up After Emergency Department Visit for Mental Health o The percent of discharges for members 18 years and older who had a visit to the ED with a primary diagnosis of mental health during the measurement year AND who had a follow-up visit with any provider with a corresponding primary diagnosis of mental health, reported separately for follow-up within 7 and 30 days after discharge. Follow-up after hospitalization for Mental Illness o The percentage of discharges for members 6 years of age and older who were hospitalized for treatment of selected mental illness diagnoses and who had an outpatient visit, an intensive outpatient encounter or partial hospitalization with a mental health practitioner, reported separately for follow-up within 7 and 30 days of discharge. Medication Management for People with Asthma (5 64 Years) o The percentage of members 5-64 years of age who were identified as having persistent asthma and were dispensed appropriate medications that they remained on for at least 75% of their treatment period. Mental Health Treatment Penetration (Broad Version) o The percentage of members with a mental health service need who received mental health services in the measurement year. Separate reporting for three age groups: 6-17 years, years, and 65 years and older. All Cause Emergency Department Visits per 1000 Member Months
5 o The rate of Medicaid beneficiary visits to emergency department per 1000 member months, including visits related to mental health and substance use disorder, reported for three age groups: years, years, and 65 years and older. *Potentially Avoidable Use of the Emergency Room o The percentage of total ER visits considered potentially avoidable based on an agreedupon list of ICD codes. This is considered a conservative measure of potentially avoidable ER use. *Screening for Clinical Depression and Follow-up o People 18 and older with an outpatient visit who were screened for clinical depression using a standardized depression tool, and if positive, with follow-up plan within 30 days. Substance Use Disorder Treatment Penetration o The percentage of members with a substance use disorder treatment need who received substance use disorder treatment in the measurement year. Separate reporting for three age groups: years, years, and 65 years and older. *Metrics in addition to Healthier Washington pay for performance metrics for this project
6 Evidence Based Approaches All have been demonstrated in small-scale projects within our region already. We will have a clearer sense of the models that will be most appropriate for the various providers. Bree Collaborative BH Integration Recommendations Episodic BH conditions common in Primary Care Transformation $$ for planning, implementation, and outcome achievement Collaborative Care Model (UW AIMS) Enhanced Collaboration Chronic BH Condition managed by Primary Care Serious Mental Illness/Substance Use Disorders - managed by community BH Adapted from Julie Lindberg, Molina Healthcare 2
7 Bree Collaborative BH Integration Recommendation for integrating behavioral health care services into primary care for those with behavioral health concerns and diagnoses for whom accessing services through primary care would be appropriate. Step 1 Step 2 Step 3 Step 4 Step 5 Step 6 Step 7 Step 8 Integrated Care Team: Access to behavioral health and primary care services are available on the same day as much as feasible. At a minimum, a plan is developed on the same day that includes continuous patient engagement in ways that are convenient for patients, in person or by phone or videoconferencing. Patient Access to Behavioral Health as a Routine Part of Care: Access to behavioral health and primary care services are available on the same day as much as feasible. At a minimum, a plan is developed on the same day that includes continuous patient engagement in ways that are convenient for patients, in person or by phone or videoconferencing. Accessibility and Sharing of Patient Information: The integrated care team has access to actionable medical and behavioral health information via a shared care plan at the point of care. Clinicians work together via regularly scheduled consultation and coordination to jointly address the patient s shared care plan. Practice Access to Psychiatric Services: Access to psychiatric consultation services is available in a systematic manner to assist the care team in developing a treatment plan and adjusting treatments for patients who are not improving as expected under their current plan. For patients with more severe or complex symptoms and diagnoses, specialty behavioral health services are readily available and are well coordinated with primary care. Operational Systems & Workflows to Support Population Based Care: A structured method is in place for proactive identification and stratification of patients for targeted conditions. The practice uses systematic clinical protocols based on screening results and other patient data, like emergency room use, that help to characterize patient risk and complexity of needs. Practices track patients with target conditions to make sure patient is engaged and treated-to-target/remission and have a proactive follow-up plan to assess improvement and adapt treatment accordingly. Evidence Based Treatments: Age language, culturally, and religiously-appropriate measurement-based interventions for physical and behavioral health interventions are adapted to the specific needs of the practice setting. Integrated practice teams use behavioral health symptom rating scales in a systematic and quantifiable way to determine whether their patients are improving. The goal of treatment is to provide strategies that include the patient s goals of care and appropriate self-management support. Patient Involvement in Care: Patient goals inform the care plan. The practice communicates effectively with the patient about their treatment options and asks for patient input and feedback into care planning. Patient activation and self-care is supported and promoted. Data for Quality Improvement: System-level data regarding access to behavioral care, the patients experience, and patient outcomes is tracked. If system goals are not met, quality improvement efforts are employed to achieve patient access goals and outcome standards. 3
8 Collaborative Care (UW AIMS) A type of integrated care, developed at the University of Washington, that treats common mental health conditions such as depression and anxiety that require systematic follow-up due to their persistent nature. Patient Centered Team Care: Primary care and behavioral health providers collaborate effectively using shared care plans that incorporate patient goals thus decreasing duplicate assessments, increasing patient comfort, and increasing patient engagement (often resulting in better care experience and improved patient outcomes). Population Based Care Population Based Care: Care team shares a defined group of patients tracked in a registry to ensure no one falls through the cracks. Practices track and reach out to patients who are not improving and mental health specialists provide caseload-focused consultation, not just ad-hoc advice. Accountable Care: Providers are accountable and reimbursed for quality of care and clinical outcomes, not just the volume of care provided.. Accountable Care Evidence Based Care: Patients are offered treatments with credible research evidence to support their efficacy in treating the target condition. Patient Centered Team Care Evidence Based Care Measurement Based Treatment to Target Measurement Based Treatment to Target: Each patient s treatment plan clearly articulates personal goals and clinical outcomes that are routinely measured by evidence-based tools. Treatments are actively changed if patients are not improving as expected until the clinical goals are achieved. 4
 Co-located, Integrated.")
9 Enhanced Collaboration Healthier Here will apply core principles to integrating primary health into the behavioral health setting: 1) Off-site, Enhanced Collaboration; 2) Co-located, Enhanced Collaboration; and 3) Co-located, Integrated. Coordinated Integration through Communication Level 1 Minimal Collaboration: Separate facilities and systems, little to no communication Level 2 Basic Collaboration at a Distance: Separate facilities and systems, communication based on specific issues or patients Co-Located Integration through Physical Proximity Level 3 Basic Collaboration Onsite: Behavioral and physical health providers located at the same site, separate systems, referral process to behavioral health Level 4 Close Collaboration with Some System Integration: Providers located at same site, some shared systems and records, some face-toface communication. Integrated Integration through Practice Change Level 5 Close Collaboration Approaching an Integrated Practice: Providers work as a team, frequent communication, may have separate medical records Level 6 Full Collaboration in a Transformed Practice: Providers work as a team, patients have a single treatment plan, all patients treated as whole person 5
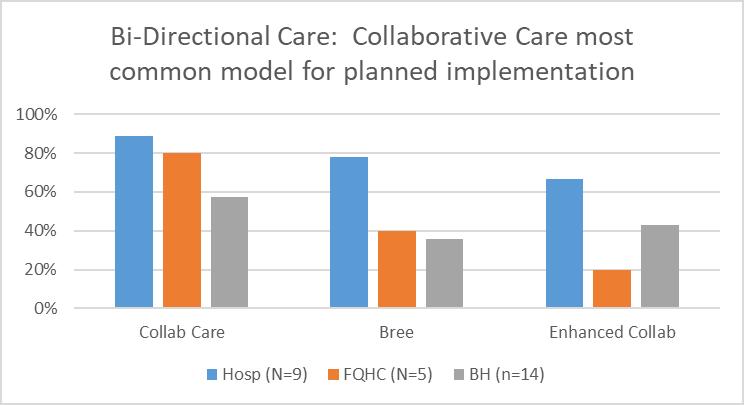
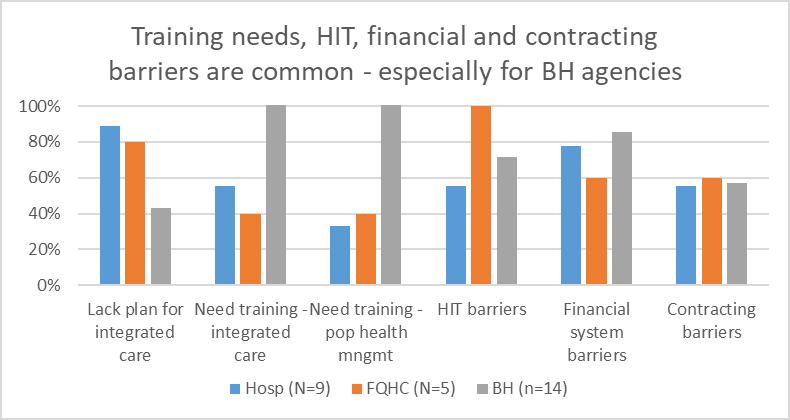
10 Bi-Directional Integration: Project-specific Current State Assessment Results
11
12

13 Graph indicates percentage of scores >5 indicating partial or full implementation

14 Graph indicates percentage of scores >5 indicating partial or full implementation



15 Primary & Behavioral Health Integrated Care Program (Model 2) Flow Chart Individual seen at BH site Is the patient connected with primary care provider? NO BH team refers patient to colocated PCP for screenings & wellness visits; document in EHR Can co-located PCP address assessed health needs? NO Co-located PCP will refer patient to appropriate provider for followup; communicate referral to BH team Referral is documented in EHR YES YES Communicate with PCP regarding screening and treatment; document in EHR Provider will communicate with Care manager and/ or BH provider; document in EHR Process Complete
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
MEDICAID TRANSFORMATION PROJECT TOOLKIT
 MEDICAID TRANSFORMATION PROJECT TOOLKIT Medicaid Transformation Demonstration Contents Domain 1: Health and Community Systems Capacity Building... 2 Financial Sustainability through Value based Payment...
MEDICAID TRANSFORMATION PROJECT TOOLKIT Medicaid Transformation Demonstration Contents Domain 1: Health and Community Systems Capacity Building... 2 Financial Sustainability through Value based Payment...
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE
 9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima Valley Farm Workers Clinic
 Clinical Integration of Behavioral Health in Washington State: The Development of Practice Standards for Primary Care Service Delivery Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima
Clinical Integration of Behavioral Health in Washington State: The Development of Practice Standards for Primary Care Service Delivery Brian E. Sandoval, Psy.D. Primary Care Behavioral Health Manager Yakima
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Healthcare Effectiveness Data and Information Set (HEDIS)
") Healthcare Effectiveness Data and Information Set (HEDIS) IlliniCare Health is a proud holder of NCQA accreditation as a managed behavioral health organization (MBHO) and prioritizes best in class performance
Healthcare Effectiveness Data and Information Set (HEDIS) IlliniCare Health is a proud holder of NCQA accreditation as a managed behavioral health organization (MBHO) and prioritizes best in class performance
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
TO BE RESCINDED Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
and HEDIS Measures
 1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
Physical Health Integration Within Behavioral Healthcare: Promising Practices
 Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Exhibit A.11.DY3. DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements
 Requirements") Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Domain 1 Patient Engagement Speed Data Reports & Schedule
 Domain 1 Patient Engagement Speed Data Reports & Schedule Suffolk Care Collaborative (SCC) Suffolk County Performing Provider System (PPS) Delivery System Reform Incentive Payment (DSRIP) Program 2 PRESENTATION
Domain 1 Patient Engagement Speed Data Reports & Schedule Suffolk Care Collaborative (SCC) Suffolk County Performing Provider System (PPS) Delivery System Reform Incentive Payment (DSRIP) Program 2 PRESENTATION
BHNNY PPS Phase Three Pay for Performance Measures. Measure Specification & Improvement Resource Guide
 Measure Specification & Improvement Resource Guide April 11, 2018 Contents: General overview and instructions for data collection with examples A synopsis of each measure including measure description,
Measure Specification & Improvement Resource Guide April 11, 2018 Contents: General overview and instructions for data collection with examples A synopsis of each measure including measure description,
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and
 Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
BHS Policies and Procedures
 BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
BHS Policies and Procedures City and County of San Francisco Department of Public Health San Francisco Health Network BEHAVIORAL HEALTH SERVICES 1380 Howard Street, 5th Floor San Francisco, CA 94103 415.255-3400
Transforming a School Based Health Center into a Patient Centered Medical Home
 Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Transforming a School Based Health Center into a Patient Centered Medical Home April 14, 2010 10:15 11:0 am Eugene F. Sun, MD, MBA Chief Medical Officer Molina Healthcare of New Mexico Outline Molina Healthcare
Tennessee Health Care Innovation Initiative
 March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
HEDIS TOOLKIT FOR PROVIDER OFFICES. A Guide to Understanding Medicaid Measure Compliance
 HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request
 DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
CPT only copyright 2014 American Medical Association. All rights reserved. 12/23/2014 Page 537 of 593
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2015 PHYSICIAN QUALITY REPTING OPTIONS F INDIVIDUAL
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
Appendix 4. PCMH Distinction in Behavioral Health Integration
 Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
Appendix 4 PCMH Distinction in Behavioral Health Integration Appendix 4 PCMH Distinction in 4-1 Distinction Purpose and Background Behavioral health conditions (mental illnesses and substance use disorders)
Instructions for Accessing the Secure Portal and the Verification Process
 Instructions for Accessing the Secure Portal and the Verification Process Community Checkup report: www.wacommunitycheckup.org More about the Alliance: www.wahealthalliance.org 1 Contents Overview... 3
Instructions for Accessing the Secure Portal and the Verification Process Community Checkup report: www.wacommunitycheckup.org More about the Alliance: www.wahealthalliance.org 1 Contents Overview... 3
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
HEDIS 101 for Providers 2018
 HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
HouseCalls Objectives
 Overview Agenda Overview Objectives Background Case studies Member Experience Primary Care Provider Experience Referrals and Follow-up Influence on Centers for Medicare & Medicaid Services (CMS) Star Ratings
Overview Agenda Overview Objectives Background Case studies Member Experience Primary Care Provider Experience Referrals and Follow-up Influence on Centers for Medicare & Medicaid Services (CMS) Star Ratings
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Articles of Importance to Read: UnitedHealthcare Goes Live With 13th Edition of Milliman Care Guidelines. Summer 2009
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)
 DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)") SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Fostering Effective Integration of Behavioral Health and Primary Care in Massachusetts Guidelines. Program Overview and Goal.
 Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Integrated Mental Health Care. Questions
 Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Core Issues in Successful Integration of Behavioral Health and Primary Care: Part 1 and Part 2. Colorado Behavioral Health Association October 3, 2010
 Core Issues in Successful Integration of Behavioral Health and Primary Care: Part 1 and Part 2 Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that in order
Core Issues in Successful Integration of Behavioral Health and Primary Care: Part 1 and Part 2 Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that in order
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
The CCBHC: An Innovative Model of Care for Behavioral Health
 The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
=======================================================================
 ======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
2) The percentage of discharges for which the patient received follow-up within 7 days after
 The percentage of discharges for which the patient received follow-up within 7 days after") Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Quality ID #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
OPERATIONS MANUAL CARE CONNECTIONS PROGRAM LOS ANGELES COUNTY DEPARTMENT OF HEALTH SERVICES
 OPERATIONS MANUAL CARE CONNECTIONS PROGRAM LOS ANGELES COUNTY DEPARTMENT OF HEALTH SERVICES SECTION: PATIENT REFERRAL and INTAKE PROCEDURES 1 P age 1 CCP Referral Procedure Referrals for the Care Connections
OPERATIONS MANUAL CARE CONNECTIONS PROGRAM LOS ANGELES COUNTY DEPARTMENT OF HEALTH SERVICES SECTION: PATIENT REFERRAL and INTAKE PROCEDURES 1 P age 1 CCP Referral Procedure Referrals for the Care Connections
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2
 Program Grantees: Part 2") SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support
 Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support by Sheri Richardt, L.C.S.W. Manager for Crisis/CL/First Access/MICCS/After Care and Shastri
Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support by Sheri Richardt, L.C.S.W. Manager for Crisis/CL/First Access/MICCS/After Care and Shastri
Payment Transformation 2018 Measure Changes and Updates. April 4, 2018
 Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard
 April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary
April Data Jam: Tracking Progress and Facilitating Improvement with your Data Dashboard Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary
Overview of New Nursing Roles in Whole Person Care. Session 1
 Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Primary Care and Behavioral Health Integration: Co-location for Article 28 and Article 31 Clinics
 Primary Care and Behavioral Health Integration: Co-location for Article 28 and Article 31 Clinics IMPLEMENTATION TOOLKIT Implementation Planning for Co-located Primary Care and Behavioral Health Services
Primary Care and Behavioral Health Integration: Co-location for Article 28 and Article 31 Clinics IMPLEMENTATION TOOLKIT Implementation Planning for Co-located Primary Care and Behavioral Health Services
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
Connected Care Connected Car Program Connected Care
 Connected Care Program Connected Care Initiative to improve the connection and coordination of care for those with Serious Mental Illness among health plans, PCPs, and behavioral health providers in outpatient,
Connected Care Program Connected Care Initiative to improve the connection and coordination of care for those with Serious Mental Illness among health plans, PCPs, and behavioral health providers in outpatient,
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
Integrated Behavioral Health
 1, Core Competencies, Chapter 16 Integrated Behavioral Health Contributor: Michael Mabanglo and Elizabeth Morrison Edited by Marc Avery Revision Date: 2/6/17 Definition and Why Supporting Integrated Behavioral
1, Core Competencies, Chapter 16 Integrated Behavioral Health Contributor: Michael Mabanglo and Elizabeth Morrison Edited by Marc Avery Revision Date: 2/6/17 Definition and Why Supporting Integrated Behavioral
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
What is a Pathways HUB?
 What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
What is a Pathways HUB? Q: What is a Community Pathways HUB? A: The Pathways HUB model is an evidence-based community care coordination approach that uses 20 standardized care plans (Pathways) as tools
Medical Assistance Program Oversight Council. January 10, 2014
 Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Behavioral and Mental Health: High-Weighted. Behavioral and Mental Health: Medium-Weighted. Implementation of co-location PCP and MH services
 Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
Behavioral and Mental Health: High-Weighted Implementation of co-location PCP and MH services *Implementation of integrated PCBH model Integration facilitation, and promotion of the colocation of mental
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL MEASURES REGISTRY ONLY
 Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
Measure #391 (NQF 0576): Follow-Up After Hospitalization for Mental Illness (FUH) National Quality Strategy Domain: Communication and Care Coordination 2016 PHYSICIAN QUALITY REPORTING OPTIONS FOR INDIVIDUAL
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions
 Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Behavioral Health Care
 Provider Communications MHN Behavioral Health Care PCP tools for coordinating care Tina Machi, Health Net We offer tools and resources for improving member health. Managed Health Network (MHN), Health
Provider Communications MHN Behavioral Health Care PCP tools for coordinating care Tina Machi, Health Net We offer tools and resources for improving member health. Managed Health Network (MHN), Health
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement
 Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Integrated Care. June Highlights:
 Spectrum of Health June 2016 Integrated Care Highlights: Current standards for mood and substance use screening and assessment Effective alternatives for integrating healthcare for your patients HEDIS
Spectrum of Health June 2016 Integrated Care Highlights: Current standards for mood and substance use screening and assessment Effective alternatives for integrating healthcare for your patients HEDIS
Behavioral Health Providers: The Key Element of Value Based Payment Success
 Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
COLORADO STATE INNOVATION MODEL Clinical Quality Measure Specifications Guidebook
 COLORADO STATE INNOVATION MODEL Clinical Quality Measure Specifications Guidebook Page 1 of 55 TABLE OF CONTENTS TABLE OF CONTENTS... 2 Introduction... 5 Acknowledgements... 6 Authors... 6 Correspondence...
COLORADO STATE INNOVATION MODEL Clinical Quality Measure Specifications Guidebook Page 1 of 55 TABLE OF CONTENTS TABLE OF CONTENTS... 2 Introduction... 5 Acknowledgements... 6 Authors... 6 Correspondence...
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
CCHN Clinical Quality Improvement Plan
 CCHN Clinical Quality Improvement Plan This Document is a Collaborative Work By HIT Sub Committee Clinical Advisory Work Group Colorado Clinical Advisory Network Colorado Dental Health Network CODAN Colorado
CCHN Clinical Quality Improvement Plan This Document is a Collaborative Work By HIT Sub Committee Clinical Advisory Work Group Colorado Clinical Advisory Network Colorado Dental Health Network CODAN Colorado