It Takes a Community:
|
|
|
- Diana Murphy
- 5 years ago
- Views:
Transcription
1 It Takes a Community: Synchronizing Care Around Patients Needs Jenney Samuelson, MS, Vermont Blueprint for Health Miriam Sheehey, RN, OneCare Vermont Jill Lord, RN, MS, Mt. Ascutney Hospital Jeremiah Eckhaus, MD, Central Vermont Medical Center
2 Current State of Play in Vermont Statewide foundation of primary care medical homes Community Health Teams providing supportive services Statewide transformation and learning network Local innovation through community collaboratives Maturing health information & data systems, comparative reporting Accountable Care Organizations representing the majority of health care providers Potential for a unified accountable health system and all payer model Day 9/26/2016 2: Track 2 Laying the Course for Coordinated Patient Care 2
3 Community Collaboratives (CC) Formed under the joint leadership of the ACOs and Blueprint for Health Focused on improving ACO and population health measures, including quality projects and coordinating health and community based services Leadership teams to identify local priority area based on state priorities Recommended Leadership teams includes: clinical leaders from independent and federally qualified health center (FQHC) primary care practices, local hospital, mental health agency, area agency on aging, home health agency, pediatrics, housing organization, plus additional locally selected members (recommended not to exceed 11) Involve additional community stakeholders Day 9/26/2016 2: Track 2 Laying the Course for Coordinated Patient Care 3
4 Workgroups of the Community Collaboratives Committees or workgroups were created to implement specific quality and coordination projects, for example: o o o o o Enhancing care coordination across organizations Reducing emergency room use Decreasing hospital admissions Increasing hospice utilization Addressing addiction
5 Supports Initiated for Community Collabortives Examples Staff Clinical Quality Consultants, Project Managers, QI Facilitators All field team meeting Integrated Communities Care Management Learning Collaborative Accountable Communities for Health Peer Learning Lab

6 VITL Summit Interagency Care Coordination October 6, 2016 Jill Lord, RN, MS, Director of Community Health Services, Project Manager Blueprint for Health


7 Windsor The Birthplace of Vermont WINDSOR

8 Community Health Team in Windsor
9 A Process Care coordination activities promote a holistic and patient centered approach to ensure that a patient s needs and goals are understood and shared among providers, patients and families to improve quality of care, patient care experience and patient engagement in care plan/treatment plan goals as a patient interacts with health providers and settings. Identify Engagemen t Assessment s Prioritize Shared Care Plan Patient needing Care Coordination Lead Care Coordinator Obtain Consents Look back, Prioritizing cards, Eco Map, Identify Root Cause Hold Care Conference Communicate plan Reassess Update as needed
10 Our Process Analysis of top 5% risk patients Factors include complex care needs and high cost/utilization (ED and inpatient admissions) o Identified patients currently cared for by Community Health Team (CHT) partners o Follow-up done for patients not currently served by CHT o Selection of patients for interagency care planning
11 Our Process Attended Integrated Care Management Collaborative to learn best practice tools provided by national experts Provided five local in-services on use of best practice tools for community partners Obtained many copies of Camden cards to distribute to partners Invited partners to play with the tools as part of their practice Trialed an initial six patients with use of the entire process

12 Interdisciplinary Team Assignments Team reviews all patients and Lead Care Coordinator chosen for each patient Lead Care Coordinator speaks with patient to discuss program and get consent
13 Needs Based Individual Care Plan Person Centered Use of Eco Maps and Camden Cards Informed Choices Agreed outcomes and goal setting should be the result in an individualized Care Plan Copy of care plan given to patient and all community partners involved in the Action Plan
14 Eco Map Name: Date Started: Medical Home PCP SASH Homecare Family Friends Specialists Housing Person Transportatio n Online Community Mental Health Counseling Health Care Proxy Community and State Services Name of Worker: Date Completed: Dental Clinic

15 Prioritizing Cards Family Relationships Urgent Non Urgent Safety Health Insurance Really Important To Me Budgeting/Finances Transportation Housing Food & Nutrition Somewhat Important To Me Need to work on right now Drugs or Alcohol Utilities Work with Health Care Team Mental Health Education & Jobs
16 Shared Care Plan Interagency Care Plan Strengths and Social Support Active Health Care Issues Individual/Family Goals Team Goals Financial/ Insurance Inventory of Resources and Supports for Self Management Action Plan

17 Lessons Learned
18 Richness of the Tools Eco Maps Patients revealed, without hesitation, the supports they had that may not ever been mentioned prior to using Eco Maps Patients were able to easily sort out and recognize what they needed to work on first, and what could wait until later Camden Cards Assisted the patient to focus on what is important and engages the patient/family in an action plan Assisted the care coordinator to match programs with community partners and services with patient/family needs
19 Richness of the Process Formal involvement with other agencies increased trust with families Interagency involvement added insight and information for more comprehensive and successful care plan Communication was improved Patients were viewed as the experts and central to decision making, i.e., shift in focus to patient-centered approach
20 Case Study #1 66 yr. old female retired factory worker who lives alone in a mobile home in rural Vermont. Active health issues include Chronic Depression, Diabetes T2 poorly controlled, Morbid Obesity, PTSD, OB, Polycystic Ovarian Syndrome, and Arthritis right knee. Patient walks with 2 canes. Services included: Care coordinator/cde did home visits weekly for several weeks, training patient to participate in her own self care management. VNA, PT, HHA in home to oversee education on DM, self management, wound care, and help with personal care. SASH was involved for financial support assistance, and wellness nurse for self management support. Ottauquechee Health Foundation and Stagecoach provided grants to support her transportation challenges. Home Behavioral Health and Eldercare visits and psychiatric medication intervention Aging in Hartland assisted pt. with prescription pick up, getting her groceries and light house cleaning.
21 Case Study #1 (Continued) Challenges: Negative attitude and skepticism re: options of care for pain control and depression. Patient's weight - 380# and she does not fit into a regular sized car refuses to wear a seat belt. Dismissed the importance of portion control and SMBG. Outcome: A1c dropped from 8.9% to 7% with no insulin changes from initial dosing and subtle diet modification. Checks fs 2x daily. Wounds have healed. Patient reports less hopelessness, daily crying jags, and improved pain control.
22 Case Study #2 54 year old man, paraplegic, living in subsidized housing at one of the SASH hub sites. Primary issue is wound care that is long standing and he is currently using a wound vac. Very upbeat positive person who is in need of a strong circle of support. Identified by Community Health Team as high utilizer of services, complex care needs, multiple agency assist. Services included: VNH- three times a week dressing change and wound monitoring. VNH- Home health aid scheduled three times a week. VNH Choices for Care PCA every morning for two hours. Consumer directed Choices for Care services; two workers employed by him through ARIS. PT and OT were involved through VNH- not in at present. SASH Coordinator almost daily check-in and support. Mental Health Counselor- home visit weekly. SASH Coordinator identified as Lead Care Coordinator due to strong relationship and regular contact. SASH Coordinator did an Eco-Map with him to identify circles of support. Used Camden cards to identify areas of need and his priorities for coordination of care.
23 Case Study #2 (Continued) Patient Goal: Healing my wounds is most important to me so I do not have to stay in bed as much. Being in bed all the time is no way to live. Areas of Importance: Cards chosen included Self-Care, Food and Nutrition, Identification, Medication and Supplies, Education, and Mental Health. Self-care: Consistency of HHA s that I can count of and have confidence in. Nutrition: I do not have noon time help and often miss lunch. Supplies: Wound care staff and VNH staff need to communicate with the company that sends my supplies for my wound vac. Identification: I need a new non-drivers ID for Vermont. Education and Mental Health: I have trouble focusing and think that I have Attention Deficit Disorder. I can t get organized.
24 Case Study #2 (Continued) Planned Interventions: Secure funds for a small fridge and microwave for his room. PCA will fill with ready made meals weekly. Secure funds for a non-medical ride to DMV to get an ID. Needed to open a local bank account, access health care and obtain meds at pharmacy. Address concerns of ADD with mental health counselor and physician. Obtain seat cushion for wheelchair that will help him to sit in electric wheelchair more comfortably. Share care plan with all medical and non-medical providers.
25 Opportunities
26 Opportunities There is an opportunity to measure the impact of interagency care management through comparison of the ranking of risk and healthcare costs/ utilization at baseline and after the interventions of the interagency care management team. Experience gained through study and lessons learned will be used to evolve ongoing interagency care management system development and individual care. Critical team members participate from the continuum of care SASH, CHT, free clinic, inpatient, Senior Solutions, Home Health, HCRS, VCCI, SEVCA. Found new funding sources when working together.
27 Opportunities (Continued) Recognition that changes do not occur overnight, they come in small steps and should be celebrated. Listen, listen, listen and hear what s important in a patientcentered approach. Patients are able to accomplish realistic goals when they have an active role in the plan. It may take more than one patient encounter to use the tools and build and document the action plan in the EMR.



28 Questions Day 9/26/2016 2: Track 2 Laying the Course for Coordinated Patient Care 28

29 VITL Summit October 6, 2016 Jeremiah Eckhaus, MD 08/10/2016 Day 9/26/2016 2: Track 2 Laying the Course for Coordinated Patient Care 29 29
30 Berlin: A bit about us Population of Health Service Area : 33,000 Collaborative Team o Jeremiah Eckhaus, MD o Kari Little, LICSW, CHT Patient Navigator o Colleen Donegan, RN o Walter Ziske, CHT Panel Coordinator o Monika Morse, Practice Facilitator 08/10/
31 A bit about our project.. Planned Interventions: Secure funds for a small fridge and microwave for his room. PCA will fill with ready made meals weekly. Secure funds for a non-medical ride to DMV to get an ID. Needed to open a local bank account, access health care and obtain meds at pharmacy. Address concerns of ADD with mental health counselor and physician. Obtain seat cushion for wheelchair that will help him to sit in electric wheelchair more comfortably. Share care plan with all medical and non-medical providers.
32 Our Plan, Do, Study, Act Cycle Plan :UVMHN Goal Goal: Reduce CHF Readmissions by 5% Do: Develop Primary Care CHF Outpatient Clinic: Start with one practice, one provider, one complex diagnosis. Study: Reduced ER Visits & Inpatient Admissions, Increased Hospice Utilization & Advanced Directives Act :Expand Practice Wide Replicate Across the Medical Group 08/10/
33 Preliminary Chart Review 18 Patients with diagnosis of Heart Failure 10 had no documented Advanced Directive 13 Inpatient Admissions (9 CHF) 17 Emergency Room Visits (9 CHF) Patient X utilization o 6 Inpatient 5 ER no Advanced Directive Patient Y utilization o 7 Inpatient 9 ER None under care of Community Health Team
34 Aim Statement Improve outpatient primary care management of patients with heart failure to reduce emergency room utilization and inpatient admissions [Click to add practice name here]
35 What We Did Designed CHF Outpatient Primary Care Clinic o Schedule with EHR Template o Huddle review scheduled patients (w/cvhhh) o 1 hour patient visits o Nurse assessment, risk index, health confidence o Co visits for patients with : Provider & Patient Navigator (CHT) o Post visit: Navigator teach back & Health Confidence o Aligned educational materials with hospital & HH [Click to add practice name here]
36 A bit more about the Patient Navigator This role is engaged in care coordination and social work: supporting the patient, caregivers and families in all settings. This might include home, long term care, primary care or specialty care. The navigator facilitates communication between the patient, the medical team, caregivers, family and community services. Main responsibilities are to coordinate outpatient, specialty and inpatient care, communicate with community agencies, monitor transitions of care, risk stratify this population, communicate with PCP about risk and changes in risk Communicate with other care team members and provide support

37 Project Team
38 What We Did Co Visits with Provider Care Coordination Between Visits Panel Management o Patient Panel, Chart Reviews & Data Collection Group Visits o o o o Pathophysiology Nutrition Education Mindful Eating Advanced Directives/Palliative Care & Hospice [Click to add practice name here]
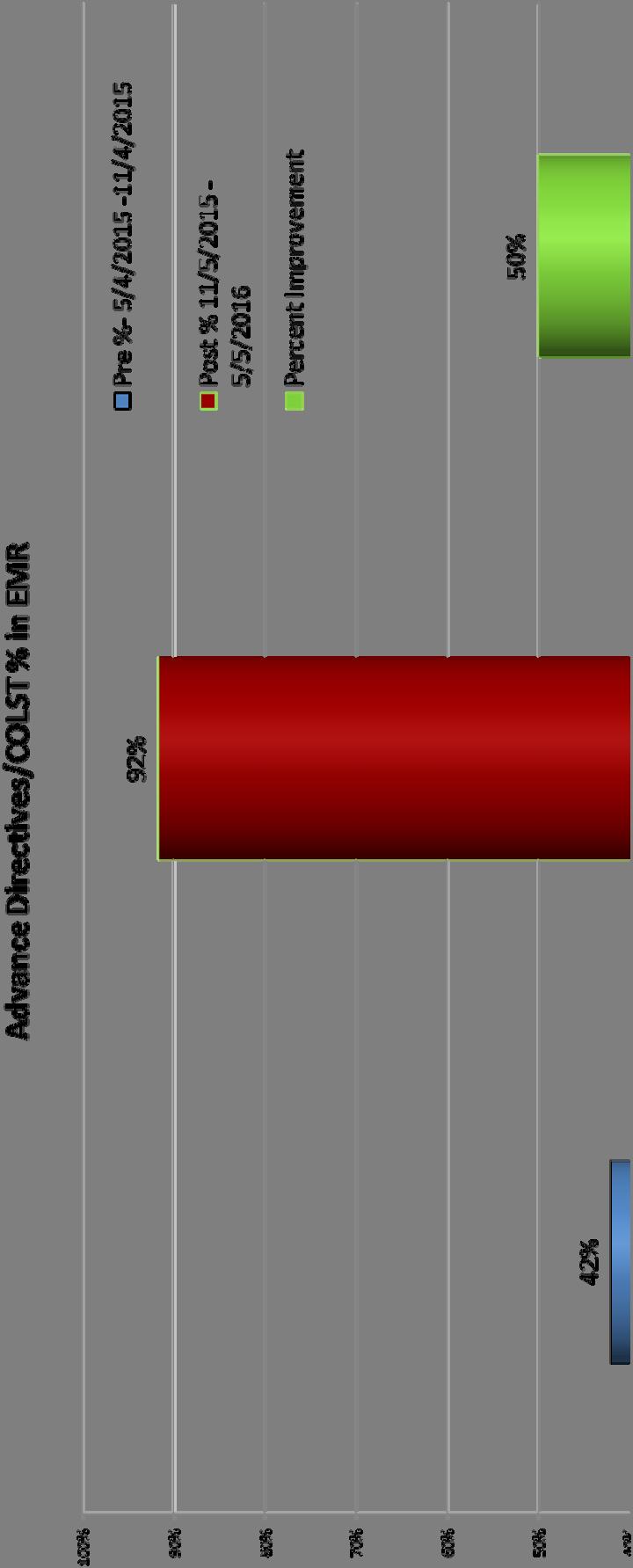
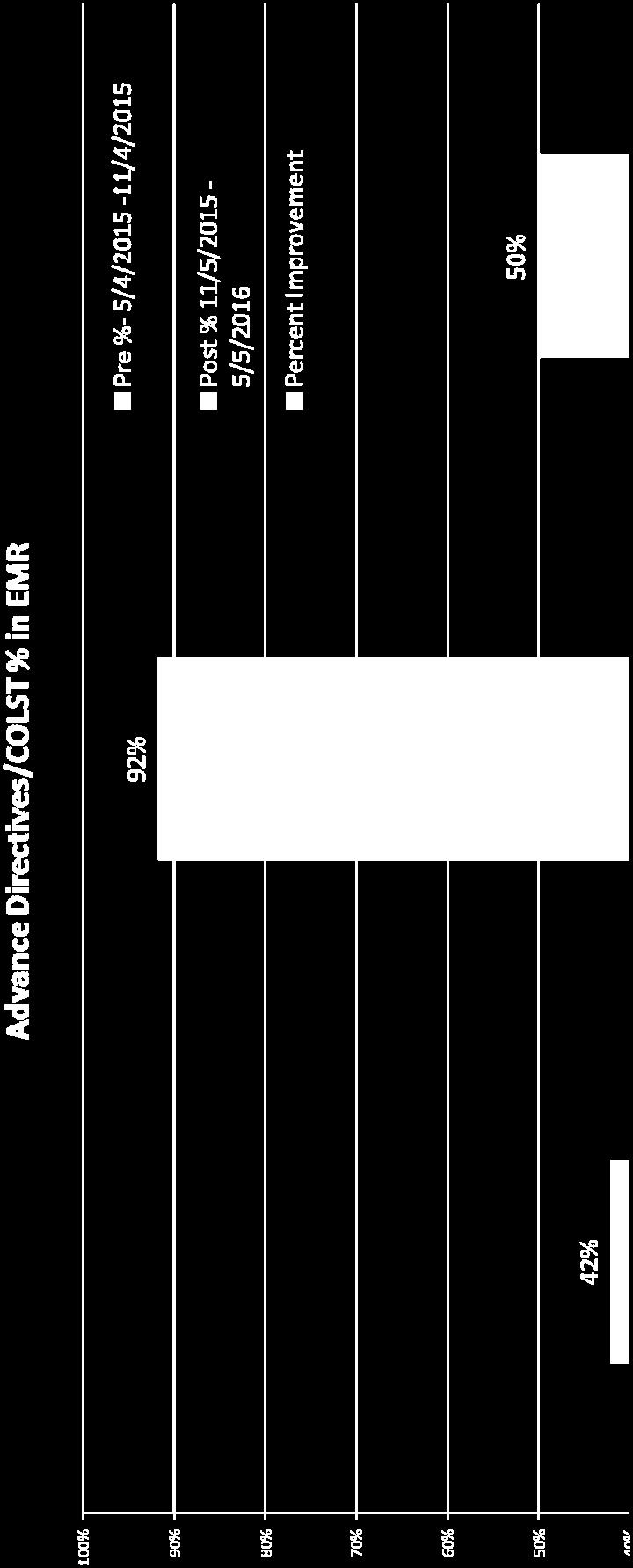
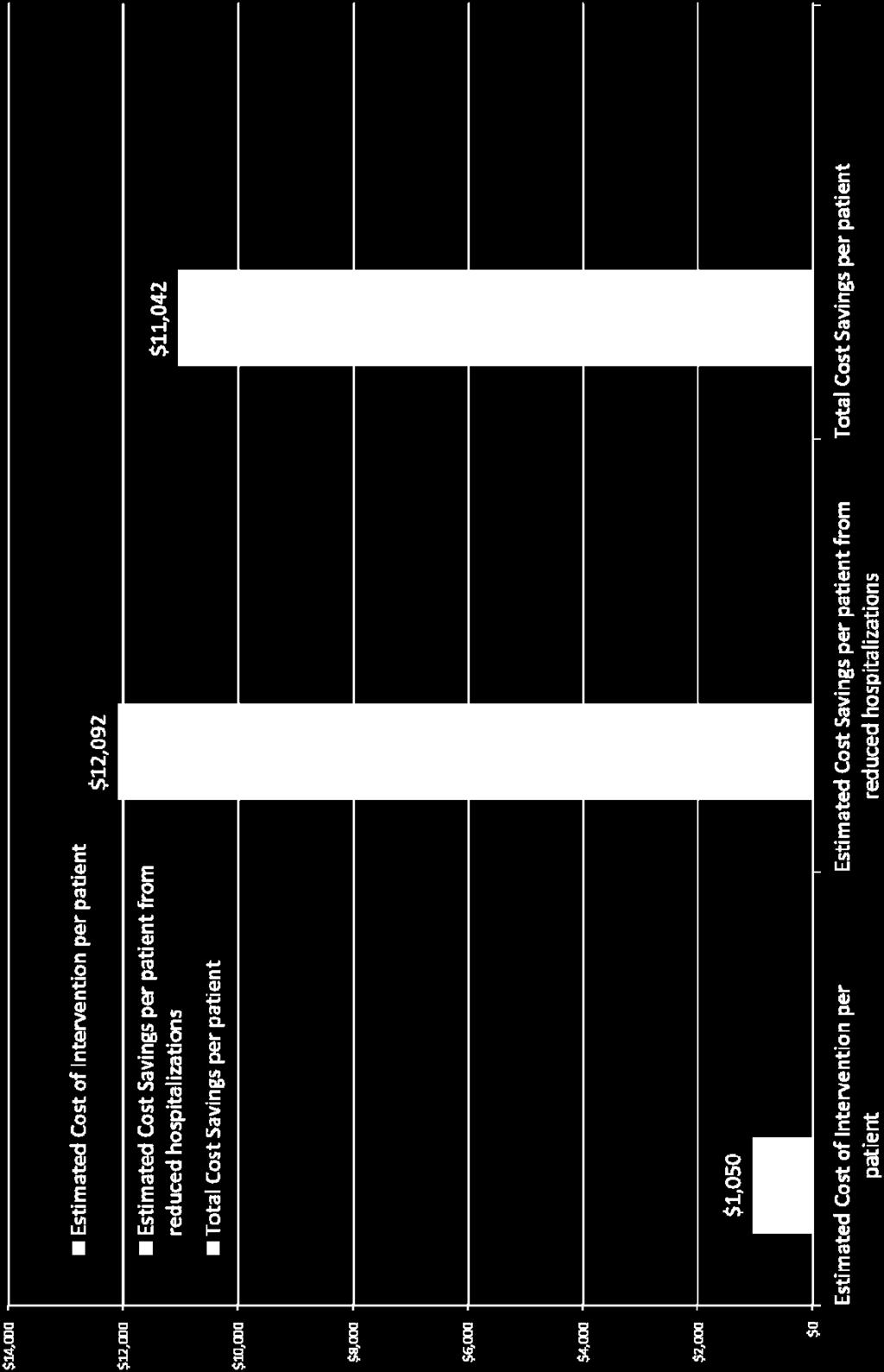
39 Measures and Results 6 Month Data Review o 75% reduction in overall number of hospital admissions o 57 % reduction in overall number of ER visits o 50% increase in Advanced Directives o $11,042 Cost Savings/Patient [Click to add practice name here]


40 CHF Pilot ED/Inpatient visit improvement Pre 5/4/ /4/ Post 11/5/2015 5/5/2016 Percent Reduction % 57% 50% 75% 2 0 ED Admission Any DX Inpatient Admissions Any DX ED Admissions for CHF Inpatient Admissions for CHF
41

42
43 Measures and Results 6 Month Data Review o Decreases in mean IP admissions and ER visits per patient (any diagnosis and CHF only) o Statistical analyses showed that these decreases were not statistically significant (all p values > 0.05) o Non significant results due to low sample size; increasing number of patients receiving intervention may show significant results [Click to add practice name here]
44 Lessons Learned This small pilot showed very promising results: there is much more to be learned We CAN impact costly utilization through care management Co visits with the provider provides detailed insight into the plan of care enhancing follow up interventions with patients 08/10/

45 Next Steps Can we expand practice wide??? Can we expand MGP Wide??? Challenges: Resources?! 08/10/
46 Contact Information Jenney Samuelson Miriam Sheehey Jill Lord Jeremiah Eckhaus
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices
 Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices Association of State and Territorial Health Officials (ASTHO) August 17, 2016 Dial-In
Patient-Centered Medical Homes in Rural and Underserved Areas: A Webinar and Peer Discussion for Primary Care Offices Association of State and Territorial Health Officials (ASTHO) August 17, 2016 Dial-In
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
National Resource Center on Native American Aging at the UNDSMHS Center for Rural Health
 Assessing Elder Needs How to Measure Benefits and Develop Links to Long-term Care Alan Allery, Ph.D. Richard L. Ludtke, PhD Leander R. McDonald, PhD National Resource Center on Native American Aging at
Assessing Elder Needs How to Measure Benefits and Develop Links to Long-term Care Alan Allery, Ph.D. Richard L. Ludtke, PhD Leander R. McDonald, PhD National Resource Center on Native American Aging at
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
CLINICAL PEARLS FOR SUCCESS IN MEDICAL RESPITE 2018 MEDICAL RESPITE TRAINING SYMPOSIUM PHOENIX, ARIZONA OCTOBER 1-2, 2018
 CLINICAL PEARLS FOR SUCCESS IN MEDICAL RESPITE 2018 MEDICAL RESPITE TRAINING SYMPOSIUM PHOENIX, ARIZONA OCTOBER 1-2, 2018 PRESENTERS: DAVE MUNSON, MD MEDICAL DIRECTOR BOSTON HEALTHCARE FOR THE HOMELESS
CLINICAL PEARLS FOR SUCCESS IN MEDICAL RESPITE 2018 MEDICAL RESPITE TRAINING SYMPOSIUM PHOENIX, ARIZONA OCTOBER 1-2, 2018 PRESENTERS: DAVE MUNSON, MD MEDICAL DIRECTOR BOSTON HEALTHCARE FOR THE HOMELESS
COMMUNITY HEALTH NEEDS ASSESSMENT 2015 IMPLEMENTATION PLAN Approved by the Mt. Ascutney Hospital and Health Center Board of Trustees on April 4, 2016
 COMMUNITY HEALTH NEEDS ASSESSMENT 2015 IMPLEMENTATION PLAN Approved by the Mt. Ascutney Hospital and Health Center Board of Trustees on April 4, 2016 1. Alcohol and drug misuse including heroin and use
COMMUNITY HEALTH NEEDS ASSESSMENT 2015 IMPLEMENTATION PLAN Approved by the Mt. Ascutney Hospital and Health Center Board of Trustees on April 4, 2016 1. Alcohol and drug misuse including heroin and use
What is Mental Health Integration?
 What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
Community Care of North Carolina
 Community Care of North Carolina 2007 Community Care of North Carolina Mail Service Center 2009 Raleigh, NC 27699-2009 (919) 715-1453 www.communitycarenc.com Background Several networks in the Community
Community Care of North Carolina 2007 Community Care of North Carolina Mail Service Center 2009 Raleigh, NC 27699-2009 (919) 715-1453 www.communitycarenc.com Background Several networks in the Community
Caregiver Stress. F r e q u e n t l y A s k e d Q u e s t i o n s. Q: Who are our nation's caregivers?
 Caregiver Stress Q: What is a caregiver? A: A caregiver is anyone who provides help to another person in need. Usually, the person receiving care has a condition such as dementia, cancer, or brain injury
Caregiver Stress Q: What is a caregiver? A: A caregiver is anyone who provides help to another person in need. Usually, the person receiving care has a condition such as dementia, cancer, or brain injury
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans
 Training Presentation for Managed Medical Assistance Specialty Plans") Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
HealthPartners SNBC Inspire
 Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
Click to edit Master title style HealthPartners SNBC Inspire March 28 & 30, 2017 Agenda New Team Members DHS SNBC Audit 6 Month Follow Up Calls Benefit Exception Inquiry Form Adjustments HealthPartners
Physical Health Integration Within Behavioral Healthcare: Promising Practices
 Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Community Paramedicine Seminar July, 20th 2015
 Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
Community Paramedicine Seminar July, 20th 2015 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes Commercial & Gov
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
HHSC Value-Based Purchasing Roadmap Texas Policy Summit
 HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and
 Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
Office of Mental Health Continuous Quality Improvement Initiative for Health Promotion and Care Coordination: 2013 Project Activities and Expectations March 2013 Overview Welcome 2013 CQI Project Options
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
Blueprint Integrated Pilot Programs
 Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Blueprint Integrated Pilot Programs Improving Access Improving Quality Improving Efficiency National Conference of State Legislatures December 10, 2008 Craig Jones MD Craig.jones@state.vt.us Health Care
Community Paramedicine Seminar Milbank Memorial Fund, Nov
 Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Community Paramedicine Seminar Milbank Memorial Fund, Nov. 6 2014 Partners DHS/MDH Hospitals EMS Medical Directors Primary care Home health Hospice Public health Affiliated clinics FQHC's CHC Look-alikes
Elliott Wilson Manager, Telehealth and Mobility Programs
 Elliott Wilson Manager, Telehealth and Mobility Programs 856-248-6575 exwilson@virtua.org THE TELEHEALTH JOURNEY Challenges and Opportunity Across the Continuum Agenda and Objectives Overview of Virtua
Elliott Wilson Manager, Telehealth and Mobility Programs 856-248-6575 exwilson@virtua.org THE TELEHEALTH JOURNEY Challenges and Opportunity Across the Continuum Agenda and Objectives Overview of Virtua
Innovative Coordinated Care Models
 Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
PCMH 2014 NCQA Standards and Guidelines
 PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
PCMH 2014 NCQA Standards and Guidelines Training Objectives Overview of process and timeline including new Renewal Option Overview of 2014 Standards Review updates and new concepts with focus on Must Pass
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia. Webinar #3 Post-Acute Care Readmissions September 8, 2016
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
COMMUNITY HEALTH IMPLEMENTATION PLAN
 COMMUNITY HEALTH IMPLEMENTATION PLAN 2017 2017-2020 Table of Contents Letter from Jeff Feasel, President & CEO 1 About Halifax Health 3 Executive Summary 6 Halifax Health Community Health Plan 2017-2020
COMMUNITY HEALTH IMPLEMENTATION PLAN 2017 2017-2020 Table of Contents Letter from Jeff Feasel, President & CEO 1 About Halifax Health 3 Executive Summary 6 Halifax Health Community Health Plan 2017-2020
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Special Needs Program Training. Quality Management Department
 10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
10/26/2017 1 Special Needs Program Training Quality Management Department 10/26/2017 2 Special Needs Plan (SNP) Overview 3 SNP Overview Medicare Advantage (MA) plans were created by the Medicare Modernization
Click to edit Master title style. ECHO Care: a program to care for complex patients
 ECHO Care: a program to care for complex patients Miriam Komaromy, MD Associate Director, Project ECHO miriamk1@salud.unm.edu ECHO Care is a special health care program designed to support patients insured
ECHO Care: a program to care for complex patients Miriam Komaromy, MD Associate Director, Project ECHO miriamk1@salud.unm.edu ECHO Care is a special health care program designed to support patients insured
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement.
 Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
o Recipients must coordinate these testing services with other HIV prevention and testing programs to avoid duplication of efforts.
 E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
Blue Quality Physician Program: Detailed Overview
 2018 Blue Quality Physician Program: Detailed Overview Program Definition The Blue Quality Physician Program is comprised of many components with one purpose: improve the care and quality for our members.
2018 Blue Quality Physician Program: Detailed Overview Program Definition The Blue Quality Physician Program is comprised of many components with one purpose: improve the care and quality for our members.
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Improving Patient Safety Across Michigan and Illinois Grand Rounds April 6, 2016 1 Agenda Grand Rounds Overview and Questions Care Transitions Vignette Fairfield Memorial s Care Check Program Grand Rounds
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
The Playbook: Better Care for People with Complex Needs
 The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
The Playbook: Better Care for People with Complex Needs Catherine Arnold Mather, MA Director Institute for Healthcare Improvement October 26, 2017 The Better Care Playbook is supported by a funders collaborative
MAHP Annual Conference. October 18 th -19th
 MAHP Annual Conference October 18 th -19th Learning Objectives Highlight UMMC s National Business strategy Provide MAHP members a UMMC Center for Telehealth update Understand the need for Telehealth services
MAHP Annual Conference October 18 th -19th Learning Objectives Highlight UMMC s National Business strategy Provide MAHP members a UMMC Center for Telehealth update Understand the need for Telehealth services
The TeleHealth Model THE TELEHEALTH SOLUTION
 The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
The Model 1 CareCycle Solutions The Solution Calendar Year 2011 Data Company Overview CareCycle Solutions (CCS) specializes in managing the needs of chronically ill patients through the use of Interventional
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012
 Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Institutional Handbook of Operating Procedures Policy
 Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Section: Clinical Policies Institutional Handbook of Operating Procedures Policy 09.01.13 Responsible Vice President: EVP and CEO Health System Subject: Admission, Discharge, and Transfer Responsible Entity:
Obesity and corporate America: one Wisconsin employer s innovative approach
 Focus On... Obesity Obesity and corporate America: one Wisconsin employer s innovative approach Amy Helwig, MD, MS; Dennis Schultz, MD, MSPH; Len Quadracci, MD Introduction The United States has an obesity
Focus On... Obesity Obesity and corporate America: one Wisconsin employer s innovative approach Amy Helwig, MD, MS; Dennis Schultz, MD, MSPH; Len Quadracci, MD Introduction The United States has an obesity
August 25, Dear Acting Administrator Slavitt:
 August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
August 25, 2016 Acting Administrator Andy Slavitt Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMS-1648-P P.O. Box 8016 Baltimore, MD 21244-8016 Re: Medicare
Community Paramedicine: Lessons Learned from South Carolina
 Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
NURSING ASSESSMENT AND MONITORING TOOL Member last name First name Middle name Medicaid number
 Contact Us 888-287-2443 MEDICALLY FRAGILE NURSING ASSESSMENT AND MONITORING TOOL Member last name First name Middle name Medicaid number Street address Date of birth City County State OK Zip Nurse completing
Contact Us 888-287-2443 MEDICALLY FRAGILE NURSING ASSESSMENT AND MONITORING TOOL Member last name First name Middle name Medicaid number Street address Date of birth City County State OK Zip Nurse completing
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service
 WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
WakeMed Rehab Hospital Stroke Rehabilitation Scope of Service WakeMed Rehab Hospital provides an integrated, comprehensive delivery of rehabilitation services utilizing evidenced-based practice directed
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
Best Practices Managing Patients with Multiple Chronic Conditions Fletcher Allen Health Care Case Study Organization Profile Located in Burlington, Fletcher Allen Health Care (FAHC) is Vermont s university
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
How Title Xx Vermont s Broadening
 How Title Xx Vermont s Broadening Subtitle Xx APCD Offers New Opportunities to Drive Value & Efficiencies Adam Moody, Director of Analytic Operations Onpoint Health Data Pat Jones, Assistant Director Presenter,
How Title Xx Vermont s Broadening Subtitle Xx APCD Offers New Opportunities to Drive Value & Efficiencies Adam Moody, Director of Analytic Operations Onpoint Health Data Pat Jones, Assistant Director Presenter,
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Introduction to the Provider Care Management Solutions Web Interface
 Introduction to the Provider Care Management Solutions Web Interface Release 0.2 Introduction to the Provider Care Management Solutions Web Interface Purpose Provider Care Management Solutions (PCMS) is
Introduction to the Provider Care Management Solutions Web Interface Release 0.2 Introduction to the Provider Care Management Solutions Web Interface Purpose Provider Care Management Solutions (PCMS) is
Organization Review Process Guide Perinatal Care Certification
 Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
Organization Review Process Guide Perinatal Care Certification 2016 Perinatal Care Certification Review Process Guide for Health Care Organizations 2016 What s New? Review process and contents of this
WakeMed Rehab Spinal Cord Injury Scope of Service
 WakeMed Rehab Spinal Cord Injury Scope of Service The WakeMed Rehab Continuum provides an integrated, comprehensive delivery of rehabilitation services utilizing evidence-based practice directed toward
WakeMed Rehab Spinal Cord Injury Scope of Service The WakeMed Rehab Continuum provides an integrated, comprehensive delivery of rehabilitation services utilizing evidence-based practice directed toward
Accountable Care for Low-income and Marginalized Populations
 Accountable Care for Low-income and Marginalized Populations Baylor Health Care System Office of Health Equity April 29, 2010 Purpose Describe the development of a hospitallinked Community Care Service
Accountable Care for Low-income and Marginalized Populations Baylor Health Care System Office of Health Equity April 29, 2010 Purpose Describe the development of a hospitallinked Community Care Service
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion. All Ohio Institute on Community Psychiatry March 25, 2017
 Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Welcome to the Rehabilitation (Rehab) Unit
 Unit") Welcome to the Rehabilitation (Rehab) Unit How to contact the Rehab Unit Page 2 What to expect with your child s care Page 3 Daily rounds Page 5 Staying overnight and visiting hours Page 8 Keeping your
Welcome to the Rehabilitation (Rehab) Unit How to contact the Rehab Unit Page 2 What to expect with your child s care Page 3 Daily rounds Page 5 Staying overnight and visiting hours Page 8 Keeping your