Accountable Care for Low-income and Marginalized Populations
|
|
|
- Brett Briggs
- 5 years ago
- Views:
Transcription
1 Accountable Care for Low-income and Marginalized Populations Baylor Health Care System Office of Health Equity April 29, 2010
2 Purpose Describe the development of a hospitallinked Community Care Service Line and the emerging Accountable Care Organizational (ACO) strategy Expanding Capacity Expanding Access Improving Quality 2
3 Overview Emergence of the Community Care Service Line A hospital-safety net clinic collaboration strategy for targeted (i.e. chronically ill) low income & marginalized populations The Community Care Model Innovation to reduce utilization & costs while reducing disparities and increasing quality (e.g. Accountable Care) Market changes demand better alignment Community Benefit Best Practice Stricter 990 reporting requirements Impending growth of Medicaid population Limited Primary & Specialty Care provider capacity Falling hospital reimbursement rates Expanding need for cost reduction innovations Increased competition around hospital quality 3
4 Definition Accountable Care Organization A provider-led organization whose mission is to manage the full continuum of care and be accountable for the overall costs and quality of care for a defined population ACO - Multiple forms: Large integrated delivery systems Physician-hospital organizations Multispecialty practice groups Independent practice associations Virtual inter-dependent networks of hospitals, physicians & clinics Reference: Rittenhouse, Shortell, Fisher N.Engl.J.Med 2009; 361:
5 Starting with a vision A Community Care Service Line Conceptual Framework 5
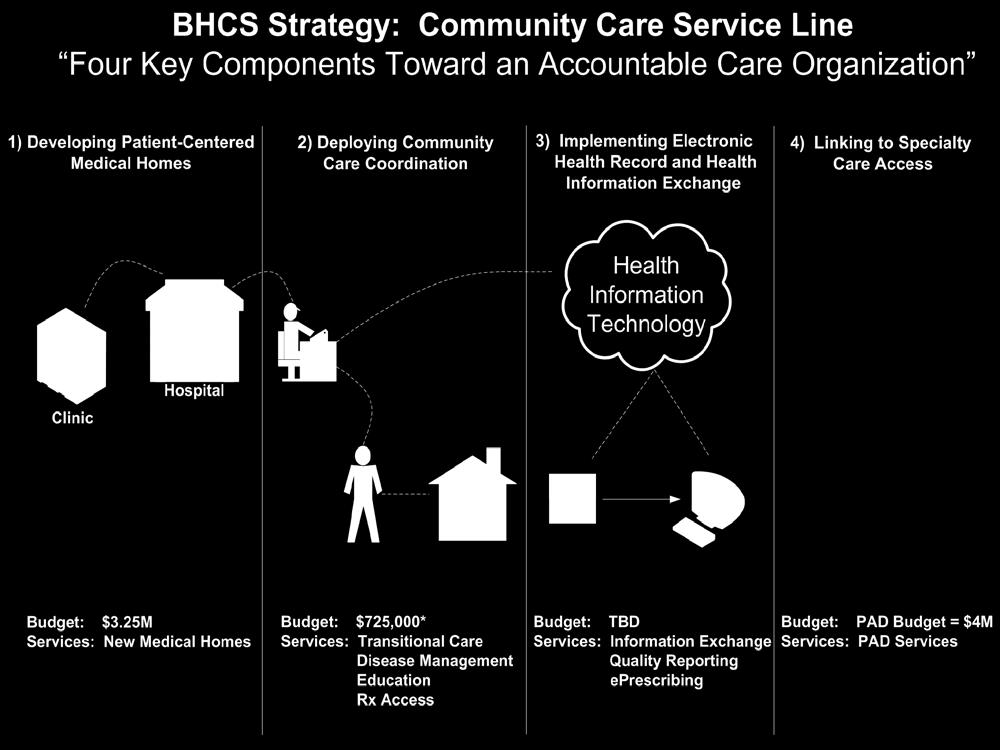

6
7 Building community-based ambulatory care capacity Strategy #1: Developing Patient- Centered Medical Homes 7
8 Community Care s Asset Map Hospital-based residency clinics Hospital-based chronic disease clinics Diabetes, Heart Failure, Asthma Community-based Primary Care FQHCs Charitable Clinics Private Physicians Specialty Care & RX Access Programs Project Access 8

9 What is the Service Area for PAD Health Information Exchange? v 6 Major Health Care Systems: Baylor HCA Methodist Parkland THR UTSWMC v Volunteer physicians v 10 Charity Clinics 9
10 Community Care Service Line Proposed Budget Increase FY11 FY08 FY09 FYTD 10 (thru 1-10) Current Funding FY11 Budget Commitment from BHCS Commitment from Outside Organizations FY-11 Funding Increase Request Difference Baylor Worth Street $0 $983,667 $720,511 $1,750,000 $1,280,000 $0 $470,000 Central Dallas Ministries $837,373 $727,754 $444,466 $1,424,000 $800,000 $624,000 $0 Christ's Family Clinic $0 $0 $0 $127,500 $0 $66,160 $61,340 Hope Clinic of Garland $0 $0 $0 $117,200 $0 $97,500 $19,700 Irving Interfaith Clinic $0 $0 $0 $117,200 $0 $97,500 $19,700 Baylor Diabetes Health & Wellness Institute $0 $0 $0 $600,000 $600,000 $0 $0 TOTAL $837,373 $1,711,421 $1,164,977 $4,135,900 $2,680,000 $885,160 $570,740 Low cost ambulatory health care delivery: ~6,300 patients; ~ $425/patient per year 10
11 Community Care Service Line Patient Capacity FY11 Projected FY10 Visits Projected FY10 Unduplicated Patients Projected FY11 Unduplicated Patients Projected FY11 Visits Patients % Change Baylor Family Med. Worth Street (3.5 FTEs) 4,170 2,370 2,850 9,450 20% ~2,700 Central Dallas Ministries (2.4 FTEs) New 8,564** 1,392 1,728 10,627** 24% Patients Christ's Family Clinic get a (0.2 FTEs) % medical Hope Clinic of Garland*** home in (0.5 FTEs) 2, ,175 3,877 32% FY-11 Irving Interfaith Clinic*** (0.5 FTEs) 1,850 1,640 1,968 6,494 20% Diabetes Health & Wellness Institute (1.5 FTEs) 0 0 1,230 4,059 - TOTAL 17,811 6,364 9,059 34,843 42% *Assumes Patient Panel Size of 1,000 patients per FTE Provider: ACMPE Paper, Determining Provider Panel Size in a Staff-model HMO, ** Central Dallas Ministries has an average of 6.15 visits per patient annually, compared to an HMO benchmark of 3.3 visits per patient ***Both Clinics recruit volunteer providers to expand PCP capacity 11
12 Community Care Service Line: Increased hospital-to-medical home connections Dedicated Project Access Enrollment Coordinators will enroll eligible patients from BHCS hospitals and establish medical homes at partnering charitable clinic. Weekly Hospital Enrollment Capacity Monthly Hospital Enrollment Capacity FY-11 Hospital Enrollment Capacity Worth Street ~1, Central Dallas Ministries 2 8h Unassigned hospitalized 96 Hope Clinic of Garland 6 24 patients get 288 a medical Irving interfaith Clinic 6 24 home in FY- 288 Diabetes Health & Wellness Institute TBD TBD 11 TBD TOTAL ,152 12
13
14 Productivity: Local Charity Clinic 1,000 Community Health Services Corps - CDM Total wrvu's by Month FY '10 - YTD wrvu's CDM 25th% MGMA Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun FTE (Jul. '09 - Aug. '09), 2.16 FTE (Sept. '09 - Current) *Note: Benchmark: 25% MGMA per 1 FTE Physician (w/o OB): 3787 per Year / 316 per Month Nurse Practitioner: 1590 per Year / 132 per Month 14
15 Productivity: Hospital-Owned Clinic 1,000 Community Health Services Corps - Worth St. Total wrvu's by Month FY '10 - YTD 900 wrvu's Worth St 25th% MGMA Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun FTE (Jul. '09 - Sept. '09), 3.0 FTE (Oct. '09 - Dec. '09), 3.25 (Jan. '09 - Current) *Note: Benchmark: 25% MGMA per 1 FTE Physician (w/o OB): 3787 per Year / 316 per Month Nurse Practitioner: 1590 per Year / 132 per Month 15
16 100% Outcomes: Service Excellence Community Health Services Corps Patient Satisfaction - Overall Mean Score Rolling 12 Months: Apr '09 - Mar '10 Overall Mean Score 90% 80% 70% Apr-09 May-09 Jun-09 Jul-09 Aug-09 Sept-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Worth St 89.1% 90.7% 96.4% 83.4% 97.3% 93.5% 91.0% 96.9% 93.3% 91.7% 83.8% 89.2% CDM 83.4% 88.4% 85.8% 96.4% 87.9% 94.8% 90.3% 80.9% 89.2% 94.9% 93.5% 84.8% Christ's Family 76.2% Irving Interfaith Hope Garland 100.0% 98.0% # of Surveys Apr-09 May-09 Jun-09 Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Worth St CDM CFC 1 Irving Hope *Survey Data by Discharge/Service Date
17 Outcomes: Quality Improvement POA 100% 90% 80% 70% 60% 50% 67% 56% Community Health Sercives Corps Adult Preventative Services Percent Opportunity Achieved July '08 - December '09 93% 93% 83% 83% 70% 62% 88% 85% 76% Jul - Dec '08 Jan - Jun '09 Jul - Dec '09 Dr. Berry Dr. Grimson Dr. Robertson Dr. Stephen Dr. Wang HTPN Average *Note: Percent Opportunity Achieved (POA) = The sum of the services provided (or completed, i.e. "done") divided by the total services applicable to the patient 17
18 Clinic Outcomes: Budget Stewardship Community Care Service Line FYTD '10 Total Expense 1 (Thru 2/10) FYTD '10 Budget (Thru 2/10) Variance (+ = over budget) (- = under budget) % Variance (+ = over budget) (- = under budget) CDM $511,621 $509,769 + $1, % Worth St. $833,099 $1,114,575 - $281, % Christ s 2 $38,644 $8,082 + $30, % Family Irving 2 $42,336 $31,964 + $10, % Interfaith Hope 2 $42,336 $31,964 + $10, % Garland *Note: 1 Total Expense from Cash Financials (3380) 18 2 Difference Between Expenses and Income
19 There is a return on investment Impacting Hospital Utilization, Uncompensated Costs & Quality 19
20 BHCS Hospital Utilization Analysis for Worth Street Patients 365 Day Pre and Post Initiation of Care Number of Uncompensated Emergency, Inpatient and Outpatient Services (n=480 patients) # ED Encounters # IP Encounters IP Avg LOS # OP Encounters Total Encounters Before Initiation of Care After Initiation of Care %Change -10.1% -51.3% -38.7% % +13.7% 20
21 BHCS Hospital Utilization Analysis for Worth Street Patients 365 Day Pre and Post Initiation of Care Total Uncompensated Emergency, Inpatient and Outpatient Costs (n=480 patients) ED Total Costs IP Total Costs OP Total Costs Total Costs Before Initiation of Care $128,769 $3,522,420 $247,087 $3,898,276 After Initiation of Care $129,586 $707,199 $398,681 $1,235,466 % Change +0.6% -79.9% +61.4% -68.3% 21
22 Outcomes: Reduced Uncompensated Hospital Care Costs $5,000,000 BHCS Hospital Utilization Analysis for Worth Street Patients 365 Day Pre and Post Initiation of Care Total Emergency, Inpatient, and Outpatient Uncompensated Costs (n=480 patients)* Reducing Hospital Care Costs: ~$5,500/patient Uncompensated Costs $4,000,000 $3,000,000 $2,000,000 $1,000,000 $0 $3,522, % Reduction $707,199 $2.6 million $128,769 $129,586 $247,087 $398, % Increase $3,898,276 ED IP OP Total 365 Day Pre Initiation 365 Day Post Initiation 68.3% Reduction $1,235,466 * At the end of CY-09, Total Patient Panel = 2,300 x $5,547 saved per patient in first year = $12,758,100 in avoided hospital costs *Note: Hospital Utilization data provided my BHCS Decision Support / Revenue Cycle. Analysis includes patients with a 1 st Date of Service at Worth St. on or before 12/21/08 with hospital utilization data through 12/21/09. 22
23 Outcomes: Reduced 30-day Post- Discharge Readmission Rate VPN-CHF Program 30-Day Post-Discharge Readmission Rate from Initial Index Admission (n = 38 total patients) 13.2% BUMC Heart Failure Readmission Rate % Improving 30-day Readmission Rates BHVH Heart Failure Readmission Rate % US National Readmission Rate for Heart Failure Patients % CMS 2004 Heart Failure Readmission Rate 2 25th Percentile 18.8% 50th Percentile 23.1% 75th Percentile 27.3% 1 U.S. Department of Health & Human Services Hospital Quality Compare. 2 Hospital 30-Day Heart Failure Readmission Measure Methodology Submitted by Yale University/Yale-New Haven Hospital Center for Outcomes Research & Evaluation (YNHH-CORE) 23
24 It s not all about the clinics Strategy #2: Developing Community Care Coordination 24
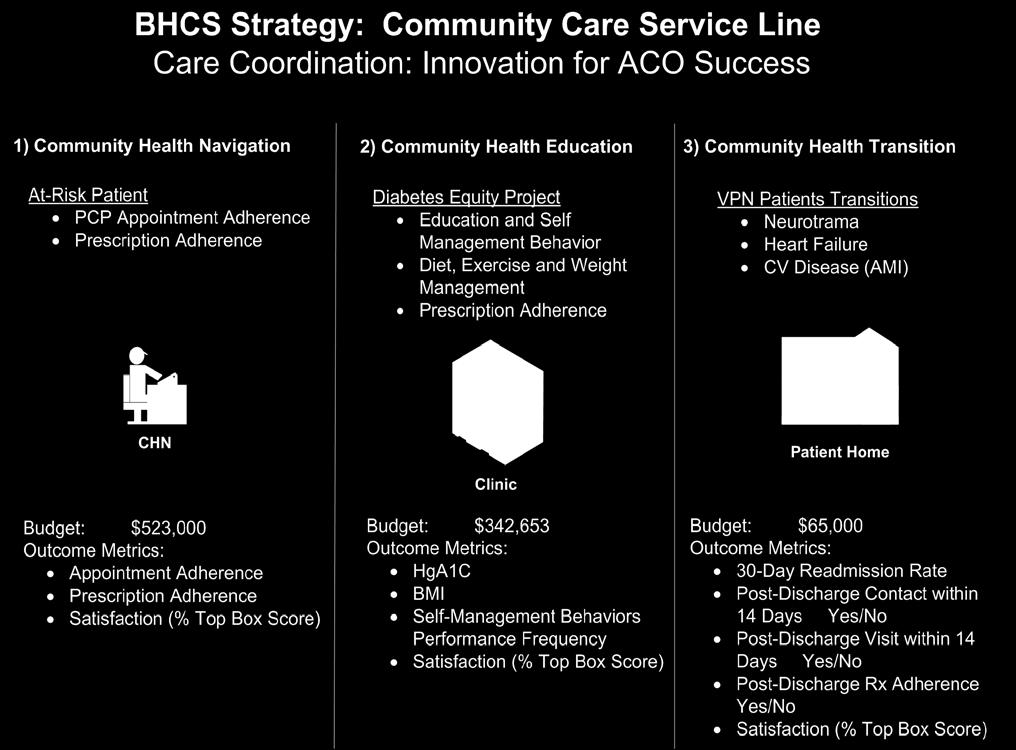
25 25
26 Community Health Navigation 26
27 Adapting Care Coordination: Community Health Navigation Utilizing the Community Health Worker (CHW) skill set Adapting CHWs to Community Health Navigation (CHN) CHNs establish relationships with patients & clinics CHNs use phone calls and visits (home, clinic, hospital, pharmacy, resource center) to coordinate and monitor a patient s successful navigation of 7 key barriers CHNs may provide emergency assistance & then coach their patients on how to better navigate in the future 27
28 How do CHNs Help Patients Navigate Health Care Systems? CHNs assigned to specific charitable clinics and targeted neighborhoods CHNs visits patients homes, clinics, hospitals and pharmacies CHNs use navigation pathways to facilitate effective care coordination CHNs provide patients with bus/light rail passes, emergency funds for prescription co-pays, health information, referrals, emotional support, translation services, etc. CHNs facilitate communication between patients, Project Access clinics and the PAD administrative office 28
29 Community Health Education 29
30 Adapting Care Coordination: Community Health Education Utilizing the Community Health Worker (CHW) skill set Adapting CHWs to Diabetes Health Promotion (DHP) Use of Community Health Workers to provide chronic disease education and self-management training to diabetic patients within charitable health clinics across Dallas County Conducting one-on-one counseling with patients (7 visits/year) DHP is bilingual/bi-cultural Contextualizes diabetes curriculum & messages Advocates for diabetics & families (meds, referrals, etc.) Serving as an additional point-of-contact for patient/families 30
31 Community Health Education Diabetes Control Study Community Diabetes Education Project (CoDE) (p=.53) Hb A1C % (p=.84) (p=.33) 8.00 (p=.03) (p=.043) Control Group (CG) Experimental Group (EG) Baseline 3 Mos 6 Mos 9 Mos 12 Mos N=90 CG, N=90 EG N=89 CG, N=85 EG N=84 CG, N=84 EG N=82 CG, N=77 EG N=78 CG, N=78 EG Experimental Group = Enrolled in CoDE Program Control Group = Standard of Care Not enrolled in CoDE Mean Age at Diabetes Onset: ( SD 10.99) Average Number of Years Since Diagnosis: 4.80 (SD 5.20) 31
 PAD DM Patients Community Care Coordination Refer to: CoDE Program 1 st - Based on Patient s Medical Home 2 nd - Based on Closest")
32 Expanding Success Health Equity Diabetes Program Manager Health Education 1 st Target Program Patient Population Medical Home DFW Charity Clinics Community Health Centers Private Practices 2 nd Target Program Patient Population Project Access Dallas (PAD) PAD DM Patients Community Care Coordination Refer to: CoDE Program 1 st - Based on Patient s Medical Home 2 nd - Based on Closest Location to Patient s Residence Refer to: CoDE Program Non PAD DM Patients DFW Charity Clinics Community Health Centers PAD Volunteer Physicians *Community Diabetes Education Program CoDE* Sites Original Success Site Juanita Craft Clinic (SSHI) Irving Interfaith Clinic CDM Hope Clinic of Garland Healing Hands- Lake Highlands Oversight of Program and CHWs Diabetes Educator (CHW) Diabetes Educator (CHW) Diabetes Educator (CHW) Diabetes Educator (CHW) Diabetes Educator (CHW) Through Grant Funds: Employed by BHCS Certified as Diabetes Educators and CHWs Equipped with Computer, Educational materials and Supplies Diabetes Education CoDE Curriculum See Attached Detailed Intervention Protocol Visit 1: Scheduled ~2 weeks after Enrollment (1 hr. visit) Visit 2: Scheduled 2 weeks after 1 st Visit (1 hr. visit) Visit 3: Scheduled ~3 weeks after 2 nd Visit (1 hr. visit) Quarterly Visits: Scheduled indefinitely after 3 rd Visit (30-60 minute visit) Clinical Support: Physician 5 Community Safety Net Clinics engaged in Community Health Education Demographics, Visits/Utilization, DM Clinical Indicators, Lab Results, DQOL Score, Medications, Foot Complication s Risk Score, Patient Goals Patient s Data Capture: Diabetes Registry Web-Based Output Patient Health Outcome Evaluation (improvement/ setbacks) Patient Reports (Identify DM management priority areas) Physician Reports Program Utilization and Effectiveness Medication Adherence and Utilization Evaluation
33 Community Health Education: Diabetes Equity Project BAYLOR HEALTH CARE SYSTEM DIABETES HEALTH PROMOTION VISIT TWO WAITING AREA o Think about this question Of all the things that could happen during this visit, what would be the most important thing? Your DHP will be asking you this shortly. YOUR VISIT WITH THE DIABETES HEALTH PROMOTER o o o Answer some questions about you and your diabetes Check your Height and weight Blood pressure Blood glucose and A1C Feet Learn about Diabetes Healthy eating tips Questions that you have o You'll be given Information on healthy eating Your diabetes daily reminder sheet Updated information for your wallet card Instructions and appointment for your next visit Patient satisfaction survey to complete today (below) AFTER YOUR VISIT o The DHP will inform your doctor of how you are doing and how we can better assist you How long have you been going to the Diabetes Health Promoter (DHP)? LESS THAN 3 MONTHS AT LEAST 3 MONTHS BUT LESS THAN 1 YEAR MORE THAN 1 YEAR Not at all Most definitely 1. Were you treated with respect today? o o o o 2. During today s visit, did you increase your understanding of diabetes care for yourself? o o o o 3. Do you feel that you could call the DHP to ask questions about the care of your diabetes? o o o o 4. How likely would you be to recommend this program to Not at all likely Very likely one of your friends or family members who has diabetes too? o o o o Comments: 33

34 Diabetes Equity Project The Diabetes Health Promoter Team 34
35 Community Health Transitions 35
36 Adapting Care Coordination: Community Health Transition Utilizing the Community Health Worker (CHW) skill set Adapting CHWs to manage patient care transitions Use of Community Health Workers to provide chronically ill hospitalized patients with effective hospital discharge: Post-discharge follow-up medical home care Access to medication, community health navigation, community health education related to chronic disease self-management Contextualizes discharge instructions & follow-up Serving as an additional point-of-contact ( warm hand-off) for patient/families Support quality goals related to 30-day readmission/mortality reduction 36
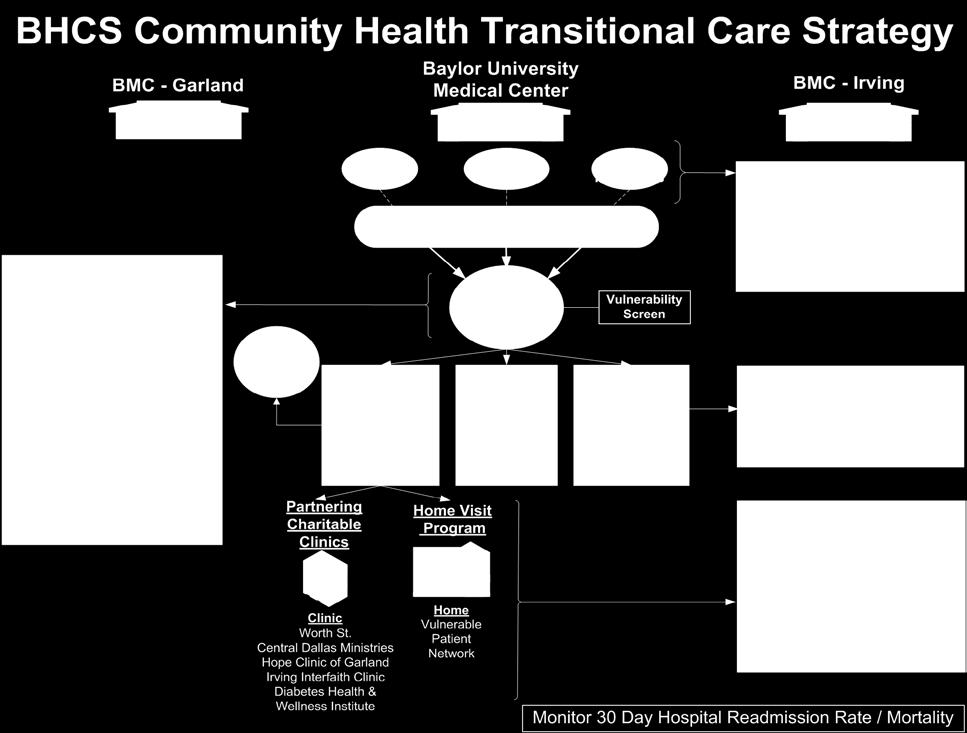
37
38 BHCS Community Care Coordination Community Health Transition Innovation PCP - Clinic Hospital Faith Community HTPN Administration Manager Volunteer Coordinator Clinic Office Manager Scheduling Office Rep Health Transition Enrollment Coordinator Unassigned Chronically Ill Underserved Patients Vulnerability Index Home Visit Community Food Drive VPN Care CHW Traditional Care MA Pt. Discharge Summary + Vulnerability Score Community Health Transitions Food Advocacy Education (Follow-up within 1 Week) Menu (AA) Specific Groceries Menu (Hispanic) Specific Groceries APN Mobile MD APN PCP Appointment Project Access Enrollment Project Access Health Navigation Home Visit Clinic Visit Metrics Community Health Education Community Health Navigation 1) Post-Hospital Clinic Visit Rate within 14 Days 2) Rate of VPN Visit 38
39 Community Health Transitions: Vulnerability Screening Tool ¹This material was prepared by Georgia QIO, the Medicare Quality Improvement Organization for Georgia under contract with the Centers for Medicare & Medicaid Services (CMS), and agency of the US Department of Health and Human Services. The contents presented do not reflect CMS Policy. 39
40 Adapting Care Coordination: Community Health Transitions A unique house-calls program which utilizes a multi-disciplinary team to provide home-based primary care services to underserved patients with complex medical and social conditions Neuro-trauma and Heart Failure Specially-trained CHW supports the care team CHW s have medical assistant training Utilize clinical and social Equity care-path tools Serve as a single point-of-contact for home-bound patients 40
41 300% Community Health Transitions Impact on Hospital Utilization BHCS Hospital Utilization for VPN-CHF Patients Pre to Post VPN-CHF Program Initiaion of Care Percent Change in Number of Encounters Over Time % Change 200% 100% 0% -100% (-) = Reduction in Utilization 90 Days 180 Days 270 Days 365 Days 450 Days (n=40) (n=38) (n=35) (n=25) Pre and Post Initiation of Care Analysis Timeframe ED IP OP Total (n=20) *Note: Hospital Utilization data provided my BHCS Decision Support / Revenue Cycle. Analysis includes patients with hospital utilization data through 12/21/09. 41
42 400% Community Health Transitions Impact on Hospital Utilization BHCS Hospital Utilization for VPN-CHF Patients Pre and Post VPN-CHF Program Initiation of Care Percent Change in Uncompensated Costs Over Time % Change 300% 200% 100% 0% -100% 90 Days 180 Days 270 Days 365 Days 450 Days (n=40) (-) = Reduction in Utilization (n=38) (n=35) (n=25) Pre and Post Initiation of Care Analysis Timeframe ED IP OP Total (n=20) *Note: Hospital Utilization data provided my BHCS Decision Support / Revenue Cycle. Analysis includes patients with hospital utilization data through 12/21/09. 42
43 $400,000 Community Health Transitions Impact on Hospital Utilization BHCS Hospitalization for VPN-CHF Patients 365-Day Pre and Post VPN-CHF Initiation of Care Emergency, Inpatient and Outpatient Uncompensated Cost (n=25 patients) Uncompensated Cost $300,000 $200,000 $100,000 $0 $6,239 $8, % Increase $278, % Reduction $126,513 $13,405 $56, % Increase $297,960 ED IP OP Total 365 Day Pre Initiation 365 Day Post Initiation 35.8% Reduction $191,310 *Note: Hospital Utilization data provided my BHCS Decision Support / Revenue Cycle. Analysis includes patients with a 1 st Date of Service in VPN-CHF program on or before 12/21/08 with hospital utilization data through 12/21/09. 43
44 We need to communicate better Strategy #3: Implementing Health Information Technology 44
45 Health Information Exchange The value for our medically vulnerable The power of a local HIE - leveraging technology: Longitudinal patient record available across organizations Incremental improvement in health care quality (i.e. decreased morbidity & mortality) Reduction in health care cost (i.e. decreased hospital utilization) Increase efficiency in health care delivery across the local safety-net health care systems Enables the development of Patient-centered Medical Homes Improvement in care coordination for patients 45
46 Physicians HIE Hospitals * Diagnosis (ICD-9) * Discharge * Lab * Medication * X Rays *Diagnostics *Discharge Summaries Regional Health Information Exchange Private MDs Not Employed; Solo & Small Groups Project Access Dallas Network Charity Clinics Hospital-Aligned Charity Clinics Non-Aligned Community Care Coordination COPC Parkland Network COPC Care Coordination Clinic COPC Clinic For-profit & Nonprofit Hospitals Clinic Clinic Care Coordination UTSWMC Network Clinic Care Coordination Clinic Private MDs Emplo yed 501(a) Patients Medically Vulnerable (Future: Commercially Insured, Medicaid/SCHIP, Medicare) 46
47 Leveraging Project Access for ACO Development Strategy #4: Linkage to Specialty Care Access 47
 in partnership with hospitals, business, faith and community organizations, and funded through grants and donations to DCMS")
48 Project Access: Our Mission A physician-led, community effort to provide health care for low-income, working but un-insured Dallas County residents. Managed by the Dallas County Medical Society (DCMS) in partnership with hospitals, business, faith and community organizations, and funded through grants and donations to DCMS foundation, the Dallas Academy of Medicine. 48
49 Supporting Physicians, Charity Clinics & Hospitals VOLUNTEER PHYSICIANS PA PARTICIPANTS Clinics DCMS HOSPITAL & ANCILLARY SERVICES PHARMACY SERVICES PAD Enrollees: Earn < 200% fpl Not Eligible for Medicaid Uninsured Dallas County Residents Referred from: Community Clinics Emergency Rooms Hospitals Doctors Clinics screen and enroll patients web-based 49
50 A Role for Pharmacy Services VOLUNTEER PHYSICIANS PA PARTICIPANTS Clinics DCMS HOSPITAL & ANCILLARY SERVICES PHARMACY SERVICES Patients receive RX thru CVS-CareMark PBM generic formulary CVS-CareMark charges costs of medications back to PAD Patient pays a minimal co-pay ($10/Rx) Some Patients obtain mailorder through Welvista Many Rx filled at Walmart s $4 formulary. 50

51 Outcomes Decreased inappropriate ED use and uncompensated hospital care Organized physician community service Increased capacity & efficiency at community health clinics Increased patient co-responsibility in health care, chronic disease management Increased community awareness and investment in community s uninsured problem 51
52 Summary Community Care Service Line emergence A hospital-linked Community Care Service Line for low income & marginalized populations Community Care s model Innovative collaboration for achieving an accountable care organizational vision Market changes provide a need for ACO Community Benefit Best Practice Stricter 990 reporting requirements Impending growth of Medicaid population Limited Primary & Specialty Care capacity for low income patients Falling hospital reimbursement rates Expanding need for cost reduction innovations Increased competition around hospital quality 52
Accountable Care Organizations Creating A Culture Of Engaged Physicians
 Accountable Care Organizations Creating A Culture Of Engaged Physicians Judith Miller, VP Medical Services & CI Advocate Physician Partners August 14, 2014 1 Sites Of Care Advocate Health Care 13 Hospitals
Accountable Care Organizations Creating A Culture Of Engaged Physicians Judith Miller, VP Medical Services & CI Advocate Physician Partners August 14, 2014 1 Sites Of Care Advocate Health Care 13 Hospitals
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
CAMDEN CLARK MEDICAL CENTER:
 INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
4/10/2013. Learning Objective. Quality-Based Payment Models
 Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Creating Best in Class Perioperative Services under Accountable Care and Value- Based Purchasing Becker s Healthcare Jeffry Peters Learning Objective How ACA/VBP changes how we measure surgical services
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Advancing Popula/on Health and Consumerism
 Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
Advancing Popula/on Health and Consumerism 44,954 Senior Enrollees 274,345 Commercial Enrollees 66,070 Commercial ACO Members Popula/on Health Risk Stra/fica/on: Keep Pa/ents Healthy, Happy & at Home Tier
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER
 PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO
 Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO THE MARKET & PHS S POSITION 2 Progressive Health Systems, Inc. (dba Pekin Hospital) Pekin, IL 3 4 5 Nearby
Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO THE MARKET & PHS S POSITION 2 Progressive Health Systems, Inc. (dba Pekin Hospital) Pekin, IL 3 4 5 Nearby
Team Care Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc.
 2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model
 Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Innovative Reimbursement Models Value-Based Insurance Design and the Medical Home En Route to an ACO Model Mary Ellen Benzik,MD PCPCC Conference March 14, 2011 Community Collaboration to Transform Health
Benchmarking and Key Metrics Utilized by HSCT Administrators. Clint Divine, MBA, MSM Administrative Director, BMT
 Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management
 Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management PCPCC June 26, 2014 Karen Jones MD FACP VP, Chief Medical Officer, WMG Laurie Brown BSN, MBA
Transforming Care Delivery: Redesigning Case Management and Primary Care Roles in Population Health Management PCPCC June 26, 2014 Karen Jones MD FACP VP, Chief Medical Officer, WMG Laurie Brown BSN, MBA
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Hypertension. Collaborating to Control Blood Pressure: Knowing Your Numbers is Just the Beginning
 Hypertension Collaborating to Control Blood Pressure: Knowing Your Numbers is Just the Beginning Al Bradley Senior Program Manager Director, High Blood Pressure Collaborative Finger Lakes Health Systems
Hypertension Collaborating to Control Blood Pressure: Knowing Your Numbers is Just the Beginning Al Bradley Senior Program Manager Director, High Blood Pressure Collaborative Finger Lakes Health Systems
Value Based Purchasing
 Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
Using the BaldrigeCriteria to Achieve High Reliability
 Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
Aurora will expand its geographic coverage within Wisconsin to achieve its mission to: Aurora Health Care 1991 Strategic Plan
 Objectives To describe the 20-year evolution of Aurora Medical Group within Aurora Health Care To identify the cultural characteristics necessary to improve patient access from the patient s perspective
Objectives To describe the 20-year evolution of Aurora Medical Group within Aurora Health Care To identify the cultural characteristics necessary to improve patient access from the patient s perspective
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence
 PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2)
") Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Driving the value of health care through integration. Kaiser Permanente All Rights Reserved.
 Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Analysis of Incurred Claims Trend and Provider Payments
 Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Orange County s Health Care Coverage Initiative Network Structure: Interim Findings
 Orange County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The HCCI Demonstration Program in Orange County provides health care to low-income uninsured adults and
Orange County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The HCCI Demonstration Program in Orange County provides health care to low-income uninsured adults and
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Community Health Workers: Supporting Diabetes Prevention in Michigan
 Community Health Workers: Supporting Diabetes Prevention in Michigan MICHIGAN DIABETES PREVENTION NETWORK Katie Mitchell, LMSW Project Director, MiCHWA March 31, 2016 Okemos, Michigan MiCHWA is supported
Community Health Workers: Supporting Diabetes Prevention in Michigan MICHIGAN DIABETES PREVENTION NETWORK Katie Mitchell, LMSW Project Director, MiCHWA March 31, 2016 Okemos, Michigan MiCHWA is supported
Financing of Community Health Workers: Issues and Options for State Health Departments
 Financing of Community Health Workers: Issues and Options for State Health Departments ASTHO Technical Assistance Presentation Terry Mason, PhD Carl Rush, MRP Geoff Wilkinson, MSW This webinar is supported
Financing of Community Health Workers: Issues and Options for State Health Departments ASTHO Technical Assistance Presentation Terry Mason, PhD Carl Rush, MRP Geoff Wilkinson, MSW This webinar is supported
Key Steps in Creating & Sustaining Excellence
 Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
2018 Hospital Pay For Performance (P4P) Program Guide. Contact:
 Program Guide. Contact:") 2018 Hospital Pay For Performance (P4P) Program Guide Contact: QualityPrograms@iehp.org Published: December 1, 2017 Program Overview Inland Empire Health Plan (IEHP) is pleased to announce its Hospital
2018 Hospital Pay For Performance (P4P) Program Guide Contact: QualityPrograms@iehp.org Published: December 1, 2017 Program Overview Inland Empire Health Plan (IEHP) is pleased to announce its Hospital
thequalitypost in this issue Get Out of Your Comfort Zone Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone
 thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
thequalitypost Edward Tufte s Principles for Effective Presentations Get Out of Your Comfort Zone Multidiciplinary Care for COPD Going Above and Beyond Division Incentive Metrics Monthly Quality Improvement
Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral)
") Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Creating A Niche: Medical-Surgical Nurses Role in Succesful Program Development (Oral) Eileen Sacco MSN, RN, CNRN, ONC
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Community Health Improvement Plan
 Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
CHC-A Continuity Dashboard. All Sites Continuity - Asthma. 2nd Qtr-03. 2nd Qtr-04. 2nd Qtr-06. 4th Qtr-03. 4th Qtr-06. 3rd Qtr-04.
 PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
PPC1: ACCESS AND COMMUNICATION Element B: Access and Communication Results Item 1: Visits with assigned PCP Continuity data is reviewed each month at our Office Redesign Committee (ORDC). The data is collected
North Carolina Division of Medical Assistance
 North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
North Carolina Division of Medical Assistance Medicaid Clinical Policy and Programs Update on Medicaid In-Home Personal Care Services (PCS) Presented Larry Nason, Ed.D. Chief, Medicaid Facility by: and
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Creating Data-driven Strategies to Improve Hospital Outcomes
 Annual National Institute October 16, 2014 Creating Data-driven Strategies to Improve Hospital Outcomes A Case Manager s Guide Information Data Knowledge 1 2014 Conifer Health Solutions, LLC. All Rights
Annual National Institute October 16, 2014 Creating Data-driven Strategies to Improve Hospital Outcomes A Case Manager s Guide Information Data Knowledge 1 2014 Conifer Health Solutions, LLC. All Rights
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017
 D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
Combining Nursing Power and Quality Metrics to Influence Policy Development
 Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Combining Nursing Power and Quality Metrics to Influence Policy Development Patricia Nevins, MSN/Ed, RN, FANAI Baylor Scott and White Hospital Patient Advisory Nursing Department Objectives Analyze financial
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment
 Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
The Triple Aim. Productivity: Digging Deep Enough 11/4/2013. quality and satisfaction); Improving the health of populations; and
; Improving the health of populations; and") NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
Transforming Healthcare Delivery, the Challenges for Behavioral Health
 Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
The Memphis Model: Building Webs of Trust at Community Scale
 The Memphis Model: Building Webs of Trust at Community Scale Rev. Bobby Baker: Director of Faith and Community Partnerships & Dr. Teresa Cutts : Director of Research for Innovation The White House Sept.
The Memphis Model: Building Webs of Trust at Community Scale Rev. Bobby Baker: Director of Faith and Community Partnerships & Dr. Teresa Cutts : Director of Research for Innovation The White House Sept.
Shaping Healthy Communities
 Leveraging Community Health Center Status across Central Texas Shaping Healthy Communities Shaping Healthy Communities. Pete Perialas, CEO March 2010 Mission and Model o Every new clinic that opens under
Leveraging Community Health Center Status across Central Texas Shaping Healthy Communities Shaping Healthy Communities. Pete Perialas, CEO March 2010 Mission and Model o Every new clinic that opens under
Technology Fundamentals for Realizing ACO Success
 Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Welcome Providers. Thursday, November 11, Page 1
 Welcome Providers Thursday, November 11, 2010 Page 1 What is a 3 Share Plan? The 3 Share Plan is an affordable health plan for small businesses. Cost is shared among employers, their employees, and one
Welcome Providers Thursday, November 11, 2010 Page 1 What is a 3 Share Plan? The 3 Share Plan is an affordable health plan for small businesses. Cost is shared among employers, their employees, and one
STEEEP Care Summary Report Baylor Scott & White Health Enterprise FY2017 YTD (July September 2016)
") STEEEP Care Summary Report Baylor Scott & White Health Enterprise FY2017 YTD (July 2016 - September 2016) BSWH Targets and Performance FY17 YTD (September 2016) 30-Day Readmission** Combined Hospital Acquired
STEEEP Care Summary Report Baylor Scott & White Health Enterprise FY2017 YTD (July 2016 - September 2016) BSWH Targets and Performance FY17 YTD (September 2016) 30-Day Readmission** Combined Hospital Acquired
Boosting Your Bottom Line
 Boosting Your Bottom Line Making More Money for Clinics Lisa Clark, MBA NYS Office of Mental Health 7/26/16 Partners in CTAC and MCTAC include: Agenda Introduction Review of Revenue Maximization Basics
Boosting Your Bottom Line Making More Money for Clinics Lisa Clark, MBA NYS Office of Mental Health 7/26/16 Partners in CTAC and MCTAC include: Agenda Introduction Review of Revenue Maximization Basics
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
From Implementation to Optimization: Moving Beyond Operations
 From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
CSM Physician Bulletin
 CSM Physician Bulletin September 2015 Volume 5, Issue 7 Quality and Clinical Integration Status of Performance for FY 2016 Goals: July and August Results We continue to be a leader in breast cancer screening
CSM Physician Bulletin September 2015 Volume 5, Issue 7 Quality and Clinical Integration Status of Performance for FY 2016 Goals: July and August Results We continue to be a leader in breast cancer screening
Effects of Patient Navigation on Chronic Disease Self Management
 Effects of Patient Navigation on Chronic Disease Self Management M. Christina R. Esperat, RN, PhD, FAAN, Professor and Associate Dean for Clinical Services, Texas Tech University Health Sciences Center
Effects of Patient Navigation on Chronic Disease Self Management M. Christina R. Esperat, RN, PhD, FAAN, Professor and Associate Dean for Clinical Services, Texas Tech University Health Sciences Center
Virtual Care Solutions Moving Care from the Hospital to the Home
 Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Highline Health Connections: Care Navigation for Vulnerable Populations
 Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
Highline Health Connections: Care Navigation for Vulnerable Populations WSHA Readmissions Safe Table - Feb 14, 2017 Carolyn Bonner, Director Home Health, Health Connections, Cancer Center, Sleep Center
HCAHPS. Presented by: Bill Sexton. Proudly recognized as one of the Nation s Top 100 Critical Access Hospitals - ivantage Health Analytics
 HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
HCAHPS Presented by: Bill Sexton HCAHPS results will impact your organization's reimbursement in the era of health care reform HCAPHS results are a quality metric, not just a patient satisfaction metric
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Improving Patient Care through Remote Patient Monitoring
 Improving Patient Care through Remote Patient Monitoring A Collaborative Approach Between Olmsted Medical Center Rochester, MN and The Evangelical Lutheran Good Samaritan Society LivingWell@Home Sioux
Improving Patient Care through Remote Patient Monitoring A Collaborative Approach Between Olmsted Medical Center Rochester, MN and The Evangelical Lutheran Good Samaritan Society LivingWell@Home Sioux
Quality Management Report 2017 Q2
 Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Quality Management Report 2017 Q2 Quality Management Program CMS STAR Ratings Member Satisfaction (CAHPS & HOS) HEDIS Risk Adjustment DHS Member Incident Reporting Member Satisfaction Surveys Pay for Performance
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
HITECH* Update Meaningful Use Regulations Eligible Professionals
 HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
Medicare & Medicaid EHR Incentive Programs
 Medicare & Medicaid EHR Incentive Programs Puerto Rico Health & Insurance Conference 2012 Economic Transformation in Health Thomas Novak Health Information Technology for Economic & Clinical Health Centers
Medicare & Medicaid EHR Incentive Programs Puerto Rico Health & Insurance Conference 2012 Economic Transformation in Health Thomas Novak Health Information Technology for Economic & Clinical Health Centers
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
RURAL SWING BED MANAGEMENT (RSBM) TRAINING PROGRAM
 TRAINING PROGRAM") RURAL SWING BED MANAGEMENT (RSBM) The Georgia State Office of Rural Health and HOMETOWN HEALTH Present: The Need for Rural Swing Bed Training One of the challenges that rural hospitals face today is a
RURAL SWING BED MANAGEMENT (RSBM) The Georgia State Office of Rural Health and HOMETOWN HEALTH Present: The Need for Rural Swing Bed Training One of the challenges that rural hospitals face today is a
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex