Checklists after Gawande
|
|
|
- Grace Simpson
- 5 years ago
- Views:
Transcription
1 Checklists after Gawande John A Windsor University of Auckland Member, WHO Safer Surgery Study Group
2 CAUSE OF DEATH Lack of clean water and basic healthcare for children DEATHS PER DAY 30,000 Smoking 14,000 Iatrogenic harm acute care 10,000 HIV / AIDS 8,000 Road traffic accidents 3,000 Natural disasters 100 Terrorism 20 Runciman et al. Safety and Ethics in Healthcare. 2007


3 BMJ May 2009







4 Where to start? WHO formed the Safer Surgery Study Group

5 50% of avoidable error occurs in the OR
6 Some errors in the OR Risk of Infection Giving antibiotics within one hour before incision can cut the risk of surgical site infection by 50% ¹ Bratzler, The American Journal of Surgery, Classen, New England Journal of Medicine, 1992.
7 Some errors in the OR Wrong site surgery wrong site surgery incidents every year in the United States.¹ 21% of 1050 hand surgeons reported having performed wrong-site surgery at least once during their careers.² ¹ Seiden, Archives of Surgery, ² Joint Commission, Sentinel Event Statistics, 2006.
8 Some errors in the OR Anaesthetic incidents An analysis of 1256 incidents involving general anaesthesia in Australia showed that pulse oximetry on its own would have detected 82% of them.¹ ¹ Webb, Anaesthesia and Intensive Care, 1993.
9 Some errors in the OR Miscommunication Root cause of nearly 70% of the events reported to the Joint Commission from ¹ A preoperative team briefing was associated with enhanced prophylactic antibiotic choice and timing, and appropriate maintenance of intraoperative temperature and glycemia.², ³ ¹ Joint Commission, Sentinel Event Statistics, ² Makary, Joint Commission Journal on Quality and Patient Safety, ³ Altpeter, Journal of the American College of Surgeons, 2007.
10

11
12 Checklists in Healthcare Not novel Google checklist 53,200 hits checklist + operating room 27 hits Checklists are only one strategy to improve quality and institute a safety culture others include: systematic incident monitoring root cause analysis of adverse events training based on objective assessment
13 Functions of checklists Overall to ensure the correct execution of a given procedure or set of tasks Range of functions of checklists Help create and maintain a safety culture A defense strategy to prevent human errors A memory-aid to enhance task performance Standardization of the tasks Facilitate team coordination Support quality control by management Verdaasdonk et al. Surg Endosc 2009

14
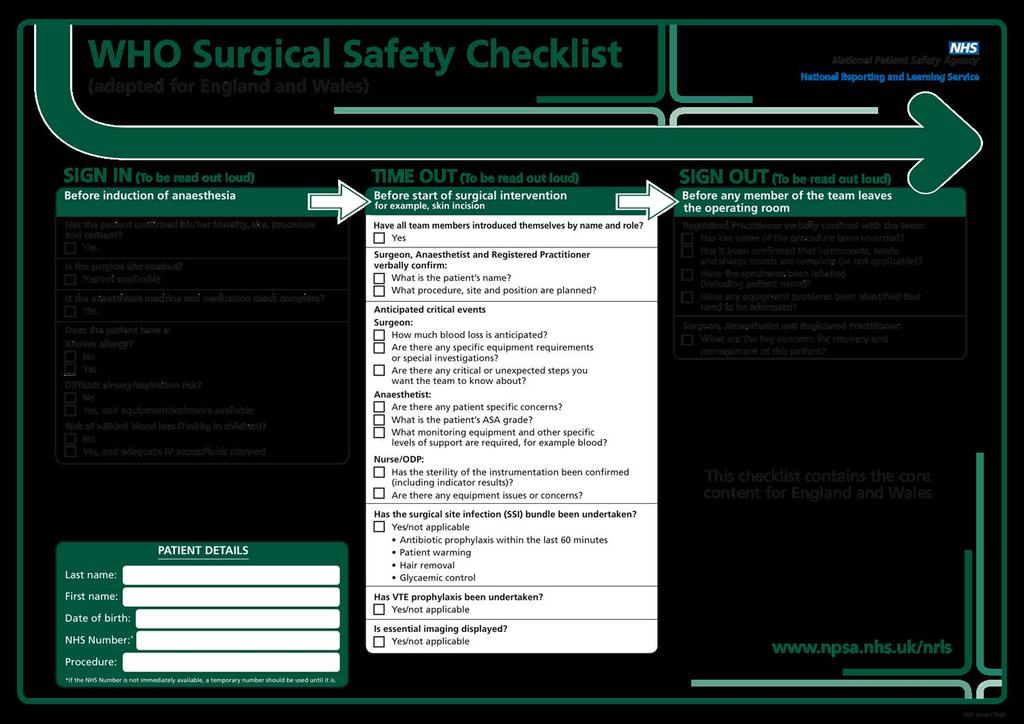
15 Methods Two phase observational study Initial baseline measures (~3 months) Deliberate introduction of checklist Repeat measurements (~3 months) Three phase checklist Sign-in, before induction Time-out, after induction and before incision Sign-out, before patient leaves theatre


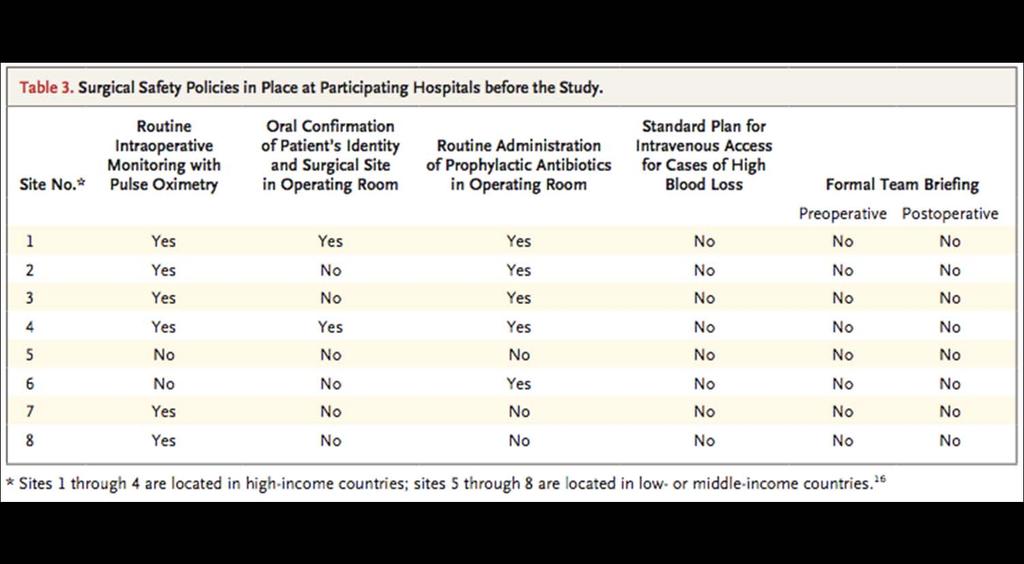
16









17 The Checklist was piloted in 8 cities PAHO I Toronto, Canada EURO London, UK EMRO Amman, Jordan PAHO II Seattle, USA WPRO I Manila, Philippines AFRO Ifakara, Tanzania SEARO New Delhi, India WPRO II Auckland, NZ
18

19
20 Results All Sites Baseline Checklist P value Cases Death 1.5% 0.8% Any Complication 11.0% 7.0% <0.001 SSI 6.2% 3.4% <0.001 Unplanned Reoperation 2.4% 1.8% Haynes et al. A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population. New England Journal of Medicine 360: (2009)
21 Advantages of Surgical Safety Checklist Customizable to local setting and needs Deployable in an incremental fashion Supported by evidence and expert consensus Evaluated in diverse settings around the world Aids adherence to established safety practices Minimal resources required to implement WHO

22 Enthusiastic endorsement

23
24 Global adoption of SSC As of April ,791 hospitals registered in 120 countries 25 countries have a national policy on the Surgical Safety Checklist WHO SSSL Newsletter April 2010


25 Hype Cycle

26 Issues with Surgical Safety Checklist Windsor. ANZ J Surg 2009
27 Issues with Surgical Safety Checklist Design Representation Scope Composition Compliance Counterproductive Cultural resistance
28 Study design Confirmation required Only intended as a pilot study Longitudinal observational design A clustered RCT with random allocation to intervention group or control group (no checklist) should be considered to remove confounders and bias Has NEJM study removed equipoise?
29 Issues with Surgical Safety Checklist Design Representation Scope Composition Compliance Counterproductive Cultural resistance

30 One small hospital One rural hospital No private hospitals One developing, three transitional and three developed nations Note only one district rural hospital
31 Issues with Surgical Safety Checklist Design Representation Scope Composition Compliance Counterproductive Cultural resistance

32 SURPASS checklist
33 Issues with Surgical Safety Checklist Design Representation Scope Composition Compliance Counterproductive Cultural resistance
34 Composition Selection criteria for the 19 items were not given, nor the evidence base, and just agreed to be a committee Authors considered that 6 of the 19 items contributed to effect Was it mainly the Hawthorne effect? What is best composition of checklist?
35 Issues with Surgical Safety Checklist Design Representation Scope Composition Compliance Counterproductive Cultural resistance
36 Adherence markedly differed between centres Site 1 (94% before and after) Site 5 (0% before and after) Site 7 (47% before and 92% after)
37 Issues with Surgical Safety Checklist Design Representation Scope Composition Compliance Counterproductive Cultural resistance
38 Counterproductive if SSC duplicated or replaced existing systems, but did not do them as well.
39 Issues with Surgical Safety Checklist Design Representation Scope Composition Compliance Counterproductive Cultural resistance

40 Leading Indian surgeon this will never work in Indian culture surgeons will not introduce themselves to everyone in the theatre they know who I am there is a subservience culture with unquestioning obedience and real fear of insubordination We need heirarchy, and checklist will undermine authority and autonomy

41 Hell, there are ain t no rules around here, we re trying to accomplish something Thomas Edison

42 we have celebrated cowboys, but what we need is more pit crews

43 Atul Gawande Checklists are often met with hostility, because they challenge doctors cherished notions about status, autonomy and expertise. Good clinicians still need expert audacity, but should be ready to accept the virtues of regimentation and standardisation.

44 Professor Alan Merry, author the introduction of the team by name and role results in the activation phenomenon which allows all members of the team to feel free to speak up and question, to wave a flag if something is not right

45 View of the press Ruth Laugeson, journalist one answer is that the gods of medicine have to submit to a simple and unexpectedly powerful discipline: the humble checklist - the real magic is that it disrupts medical heirarchies and promotes teamwork

46 Surgical Safety Checklist The NEJM study is a landmark and it has rightfully generated significant interest. The question posed, one year on, is whether the SSC is being adopted, adapted and applied as envisaged? Has there been an impact?
47 WHO statement There is no standardized way of measuring the impact of the SSC There is an ongoing challenge to create buy-in There is no clear idea about how to sustain the proper use of it WHO SSSL Newsletter April 2010




48

49 Technology is easy to develop, but changing a culture is the difficult part. People do not like change. Dean Kamen Segway inventor The Economist 2010

50

51 Crossing the chasm Leadership and research
52 Research on Checklist Design elements Elements Simplicity to reduce work and cost Practicality for ease of use Paper vs electronic vs verbal format Strategies To incentivise and change culture To ensure sustainability Impact of checklist on outcome
53 The future of SSC? It has been widely promoted and implemented, but questions remain about whether it will become part of the culture Questions remain about composition, compliance and impact Further research is needed Surgeons have a significant leadership role to play, otherwise...

54

55

56 Hype Cycle

57
58 What contributes to effect? Is there a cause - effect relationship? Or could it be due to the fact that the clinical teams were fully aware of being studied (an unblinded study) the Hawthorne effect, as noted by authors McCambridge et al. NEJM 2009
59 The utility of formal protocols varies with the nature of the activity They can disrupt focus and undermine success They can take away the authority to use own judgement, freedom to be responsible, innovate, and solve problems

60 Minnesota

61
62 Critique of the checklist Composition There are 19 items in the checklist Selection criteria for items not stated Are all items required or useful? Authors speculated that the positive findings were due to only 6 of 19 items Further studies are required to optimise best composition of the checklist
63 Critique of the checklist Consistency between centres Lack of consistency and adherence differed markedly between centres, e.g. Site 1 (94% adherence before and after) Site 5 (0% before and after) Site 7 (47% before and 92% after)
64 Critique of the checklist Confinement to the OR Safety issues can occur from admission to discharge, raising the question whether the checklist should be confined to OR? Half of all deviations occur outside the OR de Vries et al. Lancet 2008 Dutch Study SURPASS, A to D, but has 100 items, and maybe too cumbersome
65 Critique of the checklist Counterproductive Claiming a 30% reduction in mortality on extrapolation maybe misleading NB MR actually increased in one hospital Result not likely in developed countries when checklist implemented as MR already lower than the published result This might adversely affect credibility of approach and long-term compliance. Martin et al. NEJM 2009: 2373

66

67
68 Dismantling Cultural Barriers Deep-seated believe that surgeon autonomy is crucial to quality care, having freedom to lead and make decisions as patient s primary advocate Other cultural barriers include resistance to being measured, resistance to criticizing colleagues resistance to teamwork
69 Are surgeons ready for checklists and vice versa? Checklists, although not optimised, are being widely implemented. There must be a commitment to continuous improvement of this approach by further research. Surgeons are not all ready for checklists, but those not using it are creating a medico-legal risk, because it is now rapidly becoming standard of care

70

71

72
")
73 Dimensions of quality with organizational layers of healthcare Ministry of Health (NZ) 2003

74 Airline Crash Video or Tenerife photograph

75
76

77 Types of checklists

78 Error happens
79 Error in Healthcare Existence recognized since Hippocrates Often caused by the process of healthcare rather than by the underlying disease itself Extent of problem only recognized recently The watershed publication by Institute of Medicine (USA) in 2000: To err is human: building a safer health system
80 Tony Ryall a strong focus on teamwork and communication in the operating room, the main role of the checklist is simply to ensure throughness and consistency, that necessary steps are completed, all the time
81 WHO initiated projected because of Previously underestimated importance of surgery to the overall health of a nation Concern over the on-going problem of iatrogenic harm, particularly in surgery Teamwork identified as the pivotal issue for safer surgery checklist aims for a team conversation It is not just about ticking boxes, but about embracing a culture of teamwork and discipline. 2 minute WHO checklist is just a
82 The hard question, still unaswered, is whether medical culture can seize the opporutnity AG Good clinicians will not be able to dispense with expert audacity, yet we should be ready to accept the virtues of regimentation. The resistance is perhaps and inevitable response
83 Another bestseller?
84 Contribution might be by establishing relationships, forming a team, and instigating three pause points
85 Change in Death and Complications by Income Classification Change in Complications Change in Death High Income 10.3% 7.1%* 0.9% 0.6% Low / Middle Income 11.7% 6.8%* 2.1% 1.0%* Haynes et al. A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population. New England Journal of Medicine 360: (2009) * p<0.05
86
87 Critique of the checklist Cost Authors claimed that the checklist is neither costly nor lengthy No data is provided on either aspect There are additional costs (theatre time, equipment, antibiotics) that have not been accounted for, and maybe prohibitive But WHO has stated that these required for safe surgery Sanders et al. NEJM 2009: 2373
88
89

90
91 Has it? What impact has the SSC had in your hospital? How would you know?
92 ANZ Launch of Checklist Australia launch in Canberra on 19 August 2009 by Hon. Nicola Roxon, Federal Minister for Health and Aging. New Zealand launch in Wellington on 27 August 2009 by Hon Tony Ryall, Minister of Health. An opportunity to undertake a review, after the first year.
93

94


95
96

97 Responsibility of the surgeon

98

99

100 Aviations response to error Mandatory simulation training from 1955

101 Aviations response to error Mandatory simulation training from 1955 Voluntary error reporting from 1977 Anonymous and non-discoverable Non-punitive
102 Aviations response to error Mandatory simulation training from 1955 Voluntary error reporting from 1977 A systems approach to human error system is analyzed to find cause of error operator not named, blamed, shamed
103 Aviations response to error Mandatory simulation training from 1955 Voluntary error reporting from 1977 A systems approach to human error system is analyzed to find cause of error operator not named, blamed, shamed defenses were created to reduce risk of error and adverse outcome one of the defenses is the CHECKLIST

104
105 How should we respond? Acknowledge the significance of the study But recognize that success with a single study is not an enduring reduction in M&M Adopt the checklist philosophy Register your hospital with WHO and participate in ongoing developments Adapt the checklist to India and evaluate with a better designed study in India, possibly a strategic role for IASG
106 Do we need a checklist for the checklist? Great concept in theory Preliminary pilot study evidence insufficient, needs confirmation on a regular basis in each institution (it is not a magic bullet)

107
108 10 OBJECTIVES for Safe Surgery The team will operate on the correct patient at the correct site. The team will use methods known to prevent harm from administration of anaesthetics, while protecting the patient from pain. The team will recognize and effectively prepare for life-threatening loss of airway or respiratory function. The team will recognize and effectively prepare for risk of high blood loss. The team will avoid inducing an allergic or adverse drug reaction for which the patient is known to be at significant risk.
109 10 OBJECTIVES for Safe Surgery The team will consistently use methods known to minimize the risk for surgical site infection. The team will prevent inadvertent retention of instruments or sponges in surgical wounds. The team will secure and accurately identify all surgical specimens. The team will effectively communicate and exchange critical information for the safe conduct of the operation. Hospitals and public health systems will establish routine surveillance of surgical capacity, volume and results.
110 What can you do? Register on the WHO website as a participating hospital Implement the Surgical Safety Checklist in your hospital Measure results such as deaths and complications and give feedback on checklist implementation based on your personal experience
111 Deaths
112 Deaths Complications

113 Deaths Complications Near Misses
114 Support for implementation WHO Guidelines for Safe Surgery Additional resources available online at Web-based community of hospitals, organizations, and clinicians participating in this program Safe Surgery Saves Lives Program Team based in Geneva and Boston
115 Why should you get involved? Save lives and prevent complications Reduce medical costs related to errors Become a part of a supportive international online network of providers and hospitals using the checklist Participate in a program that identifies your hospital as a leader in patient safety
116 Why delayed recognition of the importance of medical error? Semantics innocuous-labelling of the problem sequelae, adverse events, complications Complacency - accepted as inevitable and expected part of operative surgery Fatalism the price to be paid for the great benefits of modern healthcare Rare and dispersed events that has not been systematically measured
117 Surgical safety is a rapidly becoming understood as a critical issue Checklist study has helped to promote this, although it is neither the first nor necessarily the best approach. Major issues exist (list the C s), and further work is required Checklists are not ready for surgeons and I do not think surgeons are ready for checklists
118

119

120
121 Medicines response to error Personal approach to human error

122 Medicine: response to error Personal approach to human error

123

124 Medicine: response to error Emphasis on human error Poor reporting of error (clinical audit)
125 ? Leave this out Fig 1.1 Dimensions of quality and organizational layers of healthcare Safety is just one dimension to consider The focus of this presentation is confined to this area but clearly cannot consider this in isolation.
126 Surgeons and pilots operate in complex environments where teams interact with technology

127
128 Epidemic of error



129
130
131
132
133
134
135
136

137
138
139
140
141 Deaths per year (USA) Number Civil AVIATION 334 National Transportation Safety Board 2007
142 Deaths per year in USA Number Civil AVIATION 334 MEDICINE 323,993
143 Deaths per year in USA due to medical error Number Civil AVIATION 334 MEDICINE 195,000
144 The number of iatrogenic deaths in the USA was equivalent to 2 jumbo jets full of passengers crashing every 3 days. Leape. Error in Medicine. JAMA 1994
145 There is an epidemic of error in healthcare

146

147

148

149

150

151
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
2012 WEBINAR SERIES. ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT.
 2012 WEBINAR SERIES ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT February 23, 2012 Welcome ASC Knowledge Share is a new webinar series
2012 WEBINAR SERIES ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT February 23, 2012 Welcome ASC Knowledge Share is a new webinar series
Expedition: Improving Safety and Reliability for Surgical Procedures
 These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
Washington Patient Safety Coalition & Surgical Public Health:
 Washington Patient Safety Coalition & Surgical Public Health: Surgical Quality in Washington State (SCOAP- Surgical Care and Outcomes Assessment Program), Surgical Safety, and the Introduction of the WHO/SCOAP
Washington Patient Safety Coalition & Surgical Public Health: Surgical Quality in Washington State (SCOAP- Surgical Care and Outcomes Assessment Program), Surgical Safety, and the Introduction of the WHO/SCOAP
Safe Surgery The Checklist Experience
 Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
The Journey To Ariadne Labs. Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist
 The Journey To Ariadne Labs Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist A Little History Flight Controls FREE & CORRECT The Problem The 3 Central Problems in Surgical Safety
The Journey To Ariadne Labs Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist A Little History Flight Controls FREE & CORRECT The Problem The 3 Central Problems in Surgical Safety
Ruth Melville - QLD ACORN Director & Chair Standards Committee NUM ORS Clinical Services NGH
 Perioperative Documentation? Surgical Safety Checklist? Tray Checklists? Count sheets? What are they and how do they fit with current standards/practice? Ruth Melville - QLD ACORN Director & Chair Standards
Perioperative Documentation? Surgical Safety Checklist? Tray Checklists? Count sheets? What are they and how do they fit with current standards/practice? Ruth Melville - QLD ACORN Director & Chair Standards
Teamwork, Communication, Briefing, Checklists, & O.R. Safety
 Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Patient Safety in the Philippines
 Patient Safety in the Philippines Armando C. Crisostomo, MD, MHPEd Professor of Surgery & Associate Dean College of Medicine, UP Manila Chair, Phil. Alliance for Patient Safety Technical Consultant, DOH
Patient Safety in the Philippines Armando C. Crisostomo, MD, MHPEd Professor of Surgery & Associate Dean College of Medicine, UP Manila Chair, Phil. Alliance for Patient Safety Technical Consultant, DOH
Teamwork, Communication, O.R. Safety & SSI Reduction
 2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
WHO PATIENT SAFETY PROGRAMME
 WHO PATIENT SAFETY PROGRAMME Carmen Audera WHO Patient SAFETY Meeting the Challenges Faced by Emerging Countries in the Provision of Quality Primary Health Care Cape Town A 23 year old women in her first
WHO PATIENT SAFETY PROGRAMME Carmen Audera WHO Patient SAFETY Meeting the Challenges Faced by Emerging Countries in the Provision of Quality Primary Health Care Cape Town A 23 year old women in her first
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery
 Plastic Surgery International Volume 2011, Article ID 579579, 5 pages doi:10.1155/2011/579579 Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery Shady Abdel-Rehim,
Plastic Surgery International Volume 2011, Article ID 579579, 5 pages doi:10.1155/2011/579579 Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery Shady Abdel-Rehim,
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Safety: A Key Component of Quality Improvement
 Patient Safety : A Key Issue for Health Systems First, do no harm Dr. Jinpeng Xu, Health Services Development World Health Organization Western Pacific Regional Office (WPRO) 20 July 2009 Training of Trainers
Patient Safety : A Key Issue for Health Systems First, do no harm Dr. Jinpeng Xu, Health Services Development World Health Organization Western Pacific Regional Office (WPRO) 20 July 2009 Training of Trainers
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
Creating and Using a Safe Surgery Checklist
 Creating and Using a Safe Surgery Checklist Michelle George, Vice President of Clinical Services Lisa Sinsel, Group Director of Clinical Services Surgical Care Affiliates 1 Agenda 1 2 3 4 5 6 7 Welcome
Creating and Using a Safe Surgery Checklist Michelle George, Vice President of Clinical Services Lisa Sinsel, Group Director of Clinical Services Surgical Care Affiliates 1 Agenda 1 2 3 4 5 6 7 Welcome
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital.
 An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
Patient Safety in Neurosurgery and Neurology. Andrea Halliday, M.D. Oregon Neurosurgery Specialists
 in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
RESEARCH PROTOCOL M MED (ANAESTHESIOLOGY) DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS)
 DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS)") RESEARCH PROTOCOL M MED (ANAESTHESIOLOGY) DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS) TITLE: AN AUDIT OF PREOPERATIVE EVALUATION OF GENERAL SURGERY PATIENTS AT DR GEORGE MUKHARI
RESEARCH PROTOCOL M MED (ANAESTHESIOLOGY) DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS) TITLE: AN AUDIT OF PREOPERATIVE EVALUATION OF GENERAL SURGERY PATIENTS AT DR GEORGE MUKHARI
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Surgical Safety Checklist:
 Implementing the Surgical Safety Checklist: the journey so far... Introduction This document summarises the experience and reflections of NHS Trusts about their progress in implementing the World Health
Implementing the Surgical Safety Checklist: the journey so far... Introduction This document summarises the experience and reflections of NHS Trusts about their progress in implementing the World Health
Implementation of Surgical Safety Checklist
 Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
Measuring Harm. Objectives and Overview
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3. Measuring Harm
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
National Priorities for Improvement:
 National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
Text-based Document. The Culture of Incident Reporting Among Filipino Nurses. de Guzman, Barbara Michelle. Downloaded 28-Apr :54:41
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital
 Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
TREATMENT OF MEDICAL ERROR ISSUES AT SURGICAL M&M CONFERENCE. Prof. Alberto R. Ferreres, MD, FACS
 TREATMENT OF MEDICAL ERROR ISSUES AT SURGICAL M&M CONFERENCE Prof. Alberto R. Ferreres, MD, FACS MEDICAL ERROR IN M&M CONFERENCE MEDICAL ERROR AT M&M CONFERENCE LA RESPONSABILIDAD MEDICA Y LA PRACTICA
TREATMENT OF MEDICAL ERROR ISSUES AT SURGICAL M&M CONFERENCE Prof. Alberto R. Ferreres, MD, FACS MEDICAL ERROR IN M&M CONFERENCE MEDICAL ERROR AT M&M CONFERENCE LA RESPONSABILIDAD MEDICA Y LA PRACTICA
Identifying Solutions / Implementation
 Patient Safety Research Introductory Course Session 5 Identifying Solutions / Implementation Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Patient Safety Research Introductory Course Session 5 Identifying Solutions / Implementation Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Kupu Taurangi Hauora o Aotearoa
 Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Quality Improvement Committee
 Quality Improvement Committee Serious and Sentinel Events in New Zealand Hospitals 2008/09 Disclaimer This report was prepared by the Quality Improvement Committee. This report does not necessarily represent
Quality Improvement Committee Serious and Sentinel Events in New Zealand Hospitals 2008/09 Disclaimer This report was prepared by the Quality Improvement Committee. This report does not necessarily represent
Safety and Quality Measures: What, Why and How? APHA Congress 2010
 Safety and Quality Measures: What, Why and How? APHA Congress 2010 Chris Baggoley 19 October 2010 Harvard study 17yrs on Although much good work has been carried out there is a sense at the coalface of
Safety and Quality Measures: What, Why and How? APHA Congress 2010 Chris Baggoley 19 October 2010 Harvard study 17yrs on Although much good work has been carried out there is a sense at the coalface of
The World Health Organisation Surgical Safety Checklist
 08 April 2016 No. 08 The World Health Organisation Surgical Safety Checklist SF Zwane Moderator: Y Hookamchand School of Clinical Medicine Discipline of Anaesthesiology and Critical Care CONTENT THE WORLD
08 April 2016 No. 08 The World Health Organisation Surgical Safety Checklist SF Zwane Moderator: Y Hookamchand School of Clinical Medicine Discipline of Anaesthesiology and Critical Care CONTENT THE WORLD
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England
 Report by the Comptroller and Auditor General The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England Ordered by the House of Commons to be printed 14 February 2000 LONDON:
Report by the Comptroller and Auditor General The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England Ordered by the House of Commons to be printed 14 February 2000 LONDON:
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
THE SAFE SURGERY CHECKLIST. MORE THAN JUST A GOOD CATCH
 THE SAFE SURGERY CHECKLIST. MORE THAN JUST A GOOD CATCH April 8, 2016 Welcome! Gina Peck Project Coordinator/Technical Host Carla Williams Patient Safety Improvement Lead Before we get started Please enter
THE SAFE SURGERY CHECKLIST. MORE THAN JUST A GOOD CATCH April 8, 2016 Welcome! Gina Peck Project Coordinator/Technical Host Carla Williams Patient Safety Improvement Lead Before we get started Please enter
Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH. Preparing Graduates for the 21 st Century Health Care System
 Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH Preparing Graduates for the 21 st Century Health Care System Interest in Method and Content: 20 years ago at UCLA -- We observed Students
Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH Preparing Graduates for the 21 st Century Health Care System Interest in Method and Content: 20 years ago at UCLA -- We observed Students
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
PATIENT SAFETY IMPROVEMENT: THE WAY FORWARD
 PATIENT SAFETY IMPROVEMENT: THE WAY FORWARD Hong Kong May 2010 Philip Hassen, President ISQua Former CEO, CPSI Background Canadian population in 2006 was 32.5 million Canadian healthcare spending for 2007
PATIENT SAFETY IMPROVEMENT: THE WAY FORWARD Hong Kong May 2010 Philip Hassen, President ISQua Former CEO, CPSI Background Canadian population in 2006 was 32.5 million Canadian healthcare spending for 2007
HALF YEAR REPORT ON SENTINEL EVENTS
 HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
Zukunftsperspektiven der Qualitatssicherung in Deutschland
 Zukunftsperspektiven der Qualitatssicherung in Deutschland Future of Quality Improvement in Germany Prof. Richard Grol Fragmentation in quality assessment and improvement Integration of initiatives and
Zukunftsperspektiven der Qualitatssicherung in Deutschland Future of Quality Improvement in Germany Prof. Richard Grol Fragmentation in quality assessment and improvement Integration of initiatives and
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers
 Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65
 Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes
 Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Understanding the Causes of Events. Objectives
 Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
Implementation Manual for the World Health Organization Surgical Safety Checklist (First Edition)
") SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Implementation Manual for the World Health Organization Surgical Safety Checklist (First Edition) Author : SAGES
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Implementation Manual for the World Health Organization Surgical Safety Checklist (First Edition) Author : SAGES
The Health Quality & Safety Commission. Research Report. Surgical Culture Safety Survey. Prepared for Health Quality & Safety Commission
 RESEARCH REPORT DECEMBER 2015 The Health Quality & Safety Commission Surgical Culture Safety Survey Research Report Prepared for Health Quality & Safety Commission Prepared by Ltd. 1 1: Executive Summary...
RESEARCH REPORT DECEMBER 2015 The Health Quality & Safety Commission Surgical Culture Safety Survey Research Report Prepared for Health Quality & Safety Commission Prepared by Ltd. 1 1: Executive Summary...
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
1875 Connecticut Ave. NW / Suite 650 / Washington, D.C / / fax /
 Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Testimony of Jane Loewenson Director of Health Policy, National Partnership for Women & Families Before the U.S. House of Representatives Energy & Commerce Subcommittee on Health Hearing on Patient Safety
Patient safety alert 06
 Immediate action Action Update Information request Correct site surgery Surgery performed at the incorrect anatomical site is rare. However, it can be devastating for patients. Correct site surgery (CSS)
Immediate action Action Update Information request Correct site surgery Surgery performed at the incorrect anatomical site is rare. However, it can be devastating for patients. Correct site surgery (CSS)
ORs in facilities that adopted team training had a lower rate of deaths for
 Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
The Regulation and Quality Improvement Authority
 The Regulation and Quality Improvement Authority Review of Theatre Practice in Health and Social Care Trusts in Northern Ireland Overview report June 2014 Assurance, Challenge and Improvement in Health
The Regulation and Quality Improvement Authority Review of Theatre Practice in Health and Social Care Trusts in Northern Ireland Overview report June 2014 Assurance, Challenge and Improvement in Health
8/10/2015. Module 1. A Fundamental Understanding of Quality. Management and its Application to Health Care
 Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Advancing Patient Safety through Accreditation. Triona Fortune Deputy Chief Executive Officer 18 th July 2103
 Advancing Patient Safety through Accreditation Triona Fortune Deputy Chief Executive Officer 18 th July 2103 Society for Quality in Health Care in Nigeria Advancing Patient Safety in Nigeria 2 Overview!
Advancing Patient Safety through Accreditation Triona Fortune Deputy Chief Executive Officer 18 th July 2103 Society for Quality in Health Care in Nigeria Advancing Patient Safety in Nigeria 2 Overview!
Clinical Nurse Specialist - Quality & Research Dept of Anaesthesiology
 Date: June 2017 Job Title : Clinical Nurse Specialist - Quality & Research Clinical Nurse Specialist, Dept of Anaesthesiology & Perioperative Medicine Department : Department of Anaesthesia & Perioperative
Date: June 2017 Job Title : Clinical Nurse Specialist - Quality & Research Clinical Nurse Specialist, Dept of Anaesthesiology & Perioperative Medicine Department : Department of Anaesthesia & Perioperative
Understanding the High Reliability Organization and Why It's Important to Your Lab
 Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Team Resource Management in the OR
 Team Resource Management in the OR What s it all about? A surgeon s perspective Peter Blair March 9, 2010 Surgical Safety Checklist The third phase of the new culture of improved patient safety Team Resource
Team Resource Management in the OR What s it all about? A surgeon s perspective Peter Blair March 9, 2010 Surgical Safety Checklist The third phase of the new culture of improved patient safety Team Resource
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative
 Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population
 special article A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population Alex B. Haynes, M.D., M.P.H., Thomas G. Weiser, M.D., M.P.H., William R. Berry, M.D., M.P.H., Stuart
special article A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population Alex B. Haynes, M.D., M.P.H., Thomas G. Weiser, M.D., M.P.H., William R. Berry, M.D., M.P.H., Stuart
Overcoming Barriers to Error Reporting: Individual, Organizational and Regulatory Issues
 Overcoming Barriers to Error Reporting: Individual, Organizational and Regulatory Issues Jason M. Etchegaray, PhD Krisanne Graves, RN, BSN, CPHQ Debora Simmons, RN, MSN, CCRN, CCNS Institute for Healthcare
Overcoming Barriers to Error Reporting: Individual, Organizational and Regulatory Issues Jason M. Etchegaray, PhD Krisanne Graves, RN, BSN, CPHQ Debora Simmons, RN, MSN, CCRN, CCNS Institute for Healthcare
#104 - Prevention of Medical Errors [1]
![#104 - Prevention of Medical Errors [1]](/thumbs/74/70423609.jpg "#104 - Prevention of Medical Errors [1]") Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm. Kendra Folh, BSN, RNC-OB
 How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
CONSORT guidelines for reporting abstracts of randomized trials. Sally Hopewell
 CONSORT guidelines for reporting abstracts of randomized trials Sally Hopewell EQUATOR Seminar 3 October 2011 Centre for Statistics in Medicine, University of Oxford, UK I recently met a physician from
CONSORT guidelines for reporting abstracts of randomized trials Sally Hopewell EQUATOR Seminar 3 October 2011 Centre for Statistics in Medicine, University of Oxford, UK I recently met a physician from
CPSM STANDARDS POLICIES For Rural Standards Committees
 CPSM STANDARDS POLICIES The Central Standards Committee (CSC) of The College of Physicians and Surgeons of Manitoba (CPSM) is a legislated standing committee of the CPSM and reports directly to the Council.
CPSM STANDARDS POLICIES The Central Standards Committee (CSC) of The College of Physicians and Surgeons of Manitoba (CPSM) is a legislated standing committee of the CPSM and reports directly to the Council.
Teamwork and Communication for Quality & Safety: It s More Than Checklists
 Teamwork and Communication for Quality & Safety: It s More Than Checklists James P. Bagian, MD, PE Director Center for Healthcare Engineering and Patient Safety University of Michigan jbagian@med.umich.edu
Teamwork and Communication for Quality & Safety: It s More Than Checklists James P. Bagian, MD, PE Director Center for Healthcare Engineering and Patient Safety University of Michigan jbagian@med.umich.edu
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
The deteriorating patient recognition and management Dave Story
 The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
Clean Care is Safer Care: a worldwide priority
 Ms # 05-CMT-263 10.03.2006 1 Clean Care is Safer Care: a worldwide priority Didier Pittet 1 and Liam Donaldson 2 1 Lead, Global Patient Safety Challenge, WHO World Alliance for Patient Safety 2 Chair,
Ms # 05-CMT-263 10.03.2006 1 Clean Care is Safer Care: a worldwide priority Didier Pittet 1 and Liam Donaldson 2 1 Lead, Global Patient Safety Challenge, WHO World Alliance for Patient Safety 2 Chair,
The How to Guide for Reducing Surgical Complications
 The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs
 I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs Research Director Boston Children's Hospital Inpatient Pediatrics Service Director, Sleep and Patient Safety Program Brigham and Women's
I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs Research Director Boston Children's Hospital Inpatient Pediatrics Service Director, Sleep and Patient Safety Program Brigham and Women's
High Reliability Organizations The Key to Improving Quality and Safety
 High Reliability Organizations The Key to Improving Quality and Safety William B Munier, MD, MBA Acting Director Center for Quality Improvement and Patient Safety Agency for Healthcare Research and Quality
High Reliability Organizations The Key to Improving Quality and Safety William B Munier, MD, MBA Acting Director Center for Quality Improvement and Patient Safety Agency for Healthcare Research and Quality
Survey on ASA Standards and APSF Recommendations
 Physician-Patient Alliance for Health & Safety Improving Health & Safety Through Innovation and Awareness Survey on ASA Standards and APSF Recommendations Mike Wong Physician-Patient Alliance for Health
Physician-Patient Alliance for Health & Safety Improving Health & Safety Through Innovation and Awareness Survey on ASA Standards and APSF Recommendations Mike Wong Physician-Patient Alliance for Health
TeamSTEPPS TM National Implementation
 TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
Prairie North Regional Health Authority: Hospital-acquired infections
 Prairie North Regional Health Authority: Hospital-acquired infections Main points... 308 Introduction... 309 Background the risk of hospital-acquired infections... 309 Audit objective, scope, criteria,
Prairie North Regional Health Authority: Hospital-acquired infections Main points... 308 Introduction... 309 Background the risk of hospital-acquired infections... 309 Audit objective, scope, criteria,
Promoting Psychological Safety for Physicians
 Doctors of BC Position Promoting Psychological Safety for Physicians Last updated: June 2017 Doctors of BC commits to working with the BC Ministry of Health, health authorities, and other stakeholders
Doctors of BC Position Promoting Psychological Safety for Physicians Last updated: June 2017 Doctors of BC commits to working with the BC Ministry of Health, health authorities, and other stakeholders
Overview. Improving Safety with Health Information Technology. Prioritizing Safety. Question 22/10/2013
 Improving Safety with Health Information Technology ISQua 2013, Edinburgh David Bates, MD, MSc Chief Quality Officer, Chief, Division of General Internal Medicine, Brigham and Women s Hospital Medical
Improving Safety with Health Information Technology ISQua 2013, Edinburgh David Bates, MD, MSc Chief Quality Officer, Chief, Division of General Internal Medicine, Brigham and Women s Hospital Medical
Medical Malpractice Risk Factors: An Economic Perspective of Closed Claims Experience
 Research Article imedpub Journals http://www.imedpub.com/ Journal of Health & Medical Economics DOI: 10.21767/2471-9927.100012 Medical Malpractice Risk Factors: An Economic Perspective of Closed Claims
Research Article imedpub Journals http://www.imedpub.com/ Journal of Health & Medical Economics DOI: 10.21767/2471-9927.100012 Medical Malpractice Risk Factors: An Economic Perspective of Closed Claims
IHI Expedition. Today s Host 9/17/2014
 September 6, 204 Begins at 3:00 PM EST These presenters have nothing to disclose IHI Expedition Expedition: Appropriate Use of Blood Products Session 3: Transfusion Safety Program Infrastructure: Measures
September 6, 204 Begins at 3:00 PM EST These presenters have nothing to disclose IHI Expedition Expedition: Appropriate Use of Blood Products Session 3: Transfusion Safety Program Infrastructure: Measures
IMPLEMENTING THE IDEAL MODEL - CHANGE MANAGEMENT
 IMPLEMENTING THE IDEAL MODEL - CHANGE MANAGEMENT Introducing a changed model of patient care, or making any other change in hospitals, involves all the usual challenges of change management. This is becoming
IMPLEMENTING THE IDEAL MODEL - CHANGE MANAGEMENT Introducing a changed model of patient care, or making any other change in hospitals, involves all the usual challenges of change management. This is becoming
WORLD ALLIANCE FOR PATIENT SAFETY WHO GUIDELINES ON HAND HYGIENE IN HEALTH CARE (ADVANCED DRAFT): A SUMMARY CLEAN HANDS ARE SAFER HANDS
: A SUMMARY CLEAN HANDS ARE SAFER HANDS") WORLD ALLIANCE FOR PATIENT SAFETY WHO GUIDELINES ON HAND HYGIENE IN HEALTH CARE (ADVANCED DRAFT): A SUMMARY CLEAN HANDS ARE SAFER HANDS WHO Guidelines on Hand Hygiene in Health Care (Avanced Draft): A
WORLD ALLIANCE FOR PATIENT SAFETY WHO GUIDELINES ON HAND HYGIENE IN HEALTH CARE (ADVANCED DRAFT): A SUMMARY CLEAN HANDS ARE SAFER HANDS WHO Guidelines on Hand Hygiene in Health Care (Avanced Draft): A
When words and actions matter most: The Case for CANDOR
 January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
What does safe surgery look like? Jonathan Beard Professor of Surgical Education
 What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Executive & Board; Perioperative Education Committee
 OPERATING ROOM NURSES ASSOCIATION OF CANADA RULES & REGULATIONS MANUAL Title Number 405 Source Date Revised January 2011 Date Effective 1998 Perioperative Education Programs Program Review and Approval
OPERATING ROOM NURSES ASSOCIATION OF CANADA RULES & REGULATIONS MANUAL Title Number 405 Source Date Revised January 2011 Date Effective 1998 Perioperative Education Programs Program Review and Approval