A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
|
|
|
- Alban Lee
- 6 years ago
- Views:
Transcription

 Rey Gonzalez, President of HOPE Consulting LLC; Associate")
1 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University of North Texas Health Science Center Institute for Patient Safety (UNTHSCIPS) Rey Gonzalez, President of HOPE Consulting LLC; Associate Fellow, UNTHSCIPS
2 Our Mission: To innovatively impact the lives of every patient, student, and healthcare professional by creating a ubiquitous culture of patient safety throughout our community. Our Goals: To improve patient safety and reduce preventable patient harm through Education, Research, Consulting and Influence.

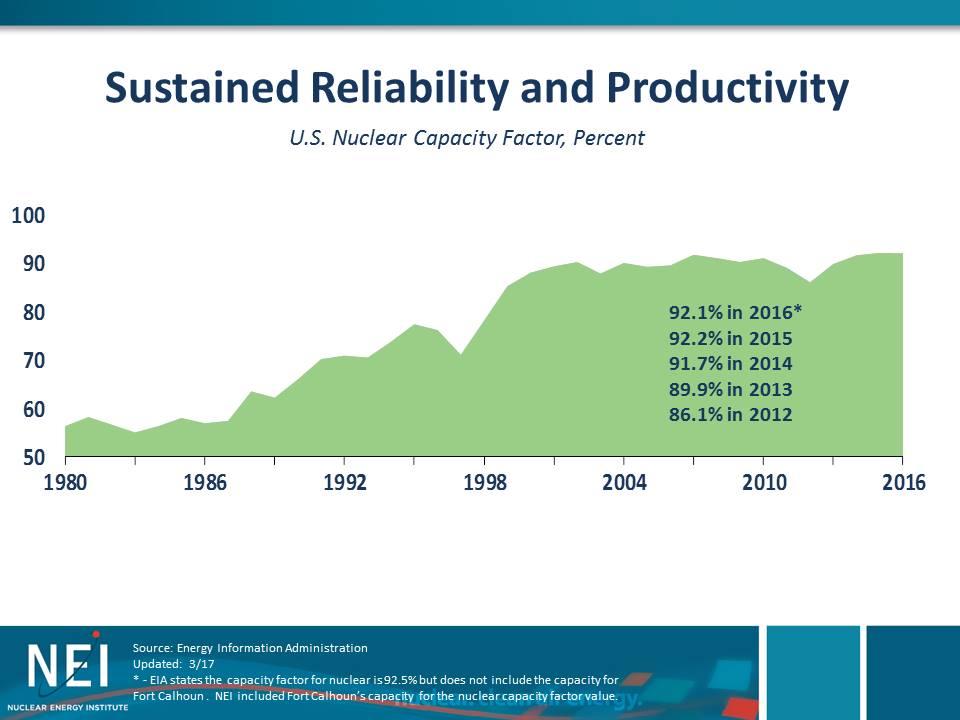
3 US Nuclear Industry


4 International Nuclear Industry Chernobyl Fukushima
5 Nuclear Industry What Was Done to Become an HRO Focus on running the plant as designed* Emphasis on defense-in-depth mindset A cultural focus shift on our #1 priority; Nuclear Safety = Public Safety (Enhancing Nuclear Safety Culture) Enhanced Training and Qualification (including maintenance of the same) A focus on equipment reliability* A focus on human performance Planning for the unexpected

6 The domestic nuclear generation industry has seen benefits from implementation of HPI.
7


8 Institute of Medicine Reports To Err is Human : November 1999 Estimated 44,000 98,000 annual deaths due to medical error Estimated a cost of $17 to $29 billion Errors are caused primarily by faulty systems, processes, and conditions that lead people to make mistakes or fail to prevent them. Crossing the Quality Chasm : March 2001 Laid out a roadmap to improve the nation s healthcare system Six Aims for Improvement Recommended 4 strategies Healthcare must be evidence-based Substantially increase the use of information technology Align payment policies with quality improvement Must prepare healthcare providers and workforce for change
 between 2008 and 2014 8 percent decrease in hospital-onset Clostridium difficile (C.")

9 17 Years After To Err is Human Project-Based Process Measures Outcome Measures Risk-Adjusted Hospital Mortality - HealthGrades: American Hospital Quality Outcomes 2013 Infection Rates 50 percent decrease in central line-associated bloodstream infections (CLABSI) between 2008 and percent decrease in hospital-onset Clostridium difficile (C. difficile) infections between 2011 and percent decrease in hospital-onset methicillinresistant Staphylococcus aureus (MRSA) bacteremia (bloodstream infections) between 2011 and 2014 The Joint Commission: America s Hospitals: Improving Quality and Safety 2016 Annual Report CDC s annual National and State Healthcare-Associated Infections Progress Report (HAI Progress Report) (2014 data, published 2016)

10 Medical Error: The Third Leading Cause of Death in the US Makary and Daniel; British Medical Journal 2016

11 Medical Error: The Third Leading Cause of Death in the US Makary and Daniel; British Medical Journal 2016 Location Deaths / Year Deaths / Day Harm / Day United States ~251,000 ~688 ~12,400 - ~20,630 Texas ~21,600 ~59 ~1,065 - ~1,775 11
12 Current Quality Approach Good Quality is Assumed to Equal Safe Patient Care Quality and Safety are Often NOT the Top Priority of Leadership Quality Improvement is Project Based PI Methods are Inadequate Reactive, rather than Proactive We must transform our culture of safety to a high reliability orientation!!!
13 RESEMBLANCE #1 ROOT CAUSE ANALYSIS Challenges: Reactive response to undesirable events Management culture looking for individual blame Ineffective cause evaluations Good News: We are taking some proactive responses Management learned about the impact of system weaknesses and an understanding of a Just Culture Much better at cause evaluations
14 Traditional Healthcare Root Cause Analysis Heavily focused on TJC Sentinel Events Focused primarily on actual harm, rather than the risk of harm. Facilitates a Culture of Blame Find out Who did What, rather than Why an event occurred. Flawed Investigation Process Inconsistent investigation processes and thus findings. Cases are handled one at a time rather than taking a systematic view of error risk. The Root Causes are Usually High Level and Not Actionable We can t improve poor communication. Corrective Actions Do Not Solve the Problems, which then Recur Find who is at fault and punish them. Change a policy or process with variable outcomes. More education and training. Try Harder!!!

15 RCA 2 Root Cause Analysis and Action Root Cause Analysis An investigation of an adverse event or near miss with the intent of identifying its causes. The goal is to reduce or eliminate the likelihood of a future similar event. Health Care RCA s have not been as effective at preventing future harm as needed. Lack of standardized approach to the RCA. Failure to identify true root causes and prioritize them. Failure to identify systems-based corrective actions. Failure to timely execute the RCA and corrective actions. Failure to ensure follow-through on corrective actions implementation. Failure to measure and reassess the effects of the corrective actions. Failure to engage leadership at all levels of the organization in preventing harm.
16
17 Organizational Influences (96) Inadequate Staffing (21) Inadequate Policies (13) Inadequate Strategic Risk Assessment (13) Inadequate Corporate Procedures (9) HFACS Findings Supervision (69) Failure to Enforce Policies / Procedures (15) Inadequate Mentoring, Coaching (7) Inadequate Oversight (7) Inadequate Training (6) Preconditions for Unsafe Acts (694) Inadequate Comm. Between Providers (82) Failure to Warn/ Disclose Critical Information (58) Inadequate Comm. During Handoff (46) Failure to Use All Available Resources (41) Inadequate Comm. Between Workgroups (41) Lack of Teamwork (32) No or Ineffective Communication Methods (30) Task Overload (26) Confusing / Conflicting Directions (21) Inadequate Comm. - Staff to Patient (21) Perceived Haste (18) No One in Charge (18) Unsafe Acts (852) Routine Violation of Policy / Procedure (76) Inadequate Risk Assessment (75) Critical Thinking Failure (66) Caution / Warning Ignored or Misinterpreted (65) Wrong Response to Urgent Situation (50) Failure to Assess Patient (47) Inadequate Report Provided (44) Misinterpretation of Information (39) Failure to Monitor Patient (34) Inadequate / Untimely Communication (33) Distracting Behavior (26) Selected Incorrect Procedure (23)
18 RESEMBLANCE #2 CHECKLISTS Challenges: Some of the original culture didn t value and therefore didn t start with many checklists, job aids, or procedures Didn t start with any reinforced expectations for use Good News: Checklists, job aids, procedures and standard work documents exist in plenty Reinforced expectations for use by top performers

19 I Have a New Surgical Instrument!!! I will give it to you FREE. Surgical staff find it easy to use and learn. It will take about 3 minutes per case. It s proven to: Cut operative mortality by 50% Cut surgical site infections by 50% Cut any surgical complication by 33% Cut all unplanned returns to the OR by 25% Will you use it???


20 Surgical Safety Checklist NEJM January 29, 2009
21 RESEMBLANCE #3 COMMUNICATION Challenges: Established verbal communication did not close the loop Verbalized organizational communication left un-validated No structure provided on what to communicate Good News: 3-way communication is an effective technique Top performers validate communication flow throughout the organization Several tools; PJBs/Turnovers/SAFER conversations
22 Health Care Communication Improvement Daily Safety Huddles Structured Hand-Offs Face-to-Face with the Patient Use of Checklists Medication Reconciliation SBAR Situation Background Assessment Recommendation Team STEPPS (Crew Resource Management) Read Back Protocols
23 THE HOLY GRAIL SAFETY CULTURE

24 A Call for High Reliability

25 Leadership High Reliability RPI Trust Improve Report Health Care Safety Culture Mark Chassin, MD th International HRO Conference May 21, 2012
26 Health Care Reliability Cannot show reliable and valid safety statistics! Error is too often viewed as a challenge to professionalism and self worth, rather than an opportunity to learn. Ongoing training, simulation and team development is often lacking. Zero harm is often not the primary focus of leadership.
27 Medical Areas for Improvement Transposition errors in patient information (administrative) Non-approved pens for marking ( it washes off ) Not being attentive during the Time-out or Safety Huddle (most prominent) Rushing to keep the OR schedule on track Pre-Op Nurse needs to be able to STOP the line, if necessary (part of the layers of defense)
28 Common Cultural Whole team solutions It takes total dedication to your #1 priority (public safety/ patient health & safety) It takes a release of egos (it s not about competency) It takes courage to speak up (e.g. for patient/nuclear safety) It takes effective communications (are you sure you were understood?)
29 Common Cultural Whole team solutions It takes a relentless pursuit and correction of system weaknesses It takes practice; using effective tools & techniques It takes a dedication to safety over production (managing schedule/time pressure) It takes an entire team commitment

30 QUESTIONS???
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
What is High Reliability and Why Does Healthcare Need it?
 What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement 25th Annual Forum Orlando, FL December
What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement 25th Annual Forum Orlando, FL December
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it?
 M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement
M2 This presenter has nothing to disclose What is High Reliability and Why Does Healthcare Need it? Mark R. Chassin, MD, FACP, MPP, MPH President, The Joint Commission Institute for Healthcare Improvement
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Creating a Highly Reliable Health System: the Leadership Challenge. 6 th Annual Patient Safety Symposium Rick Foster, MD
 Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
TIME OUT! A Patient Safety Strategy. Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service
 TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
TIME OUT! A Patient Safety Strategy Col Doug Risk, Lt Col Kelli Mack USAF Dental Evaluations & Consultation Service Disclosures The opinions expressed in this presentation are those of the authors and
High Reliability and Robust Process Improvement
 High Reliability and Robust Process Improvement Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission July 26, 2016 3000 patients over 6 years 1 2 Current State of Quality Routine
High Reliability and Robust Process Improvement Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission July 26, 2016 3000 patients over 6 years 1 2 Current State of Quality Routine
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
From Value to High-Reliability Organization
 From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication Among Caregivers
 Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
A26/B26: Goal Zero: South Carolina s Commitment to Safety
 A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Preventable Harm: California Fails to Follow Through With Patient Safety Laws
 Preventable Harm: California Fails to Follow Through With Patient Safety Laws March 2010 I. INTRODUCTION More than 10 years after the Institute of Medicine (IOM) first estimated that nearly 100,000 Americans
Preventable Harm: California Fails to Follow Through With Patient Safety Laws March 2010 I. INTRODUCTION More than 10 years after the Institute of Medicine (IOM) first estimated that nearly 100,000 Americans
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Establishing a Culture of Quality and Safety and the Journey to High Reliability
 Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
Leadership and Culture: Building Highly Reliable Systems of Care
 Learning Objectives Leadership and Culture: Building Highly Reliable Systems of Care Michael Batchelor, CEO Baptist Easley Hospital Easley, South Carolina Discuss recent developments in health systems
Learning Objectives Leadership and Culture: Building Highly Reliable Systems of Care Michael Batchelor, CEO Baptist Easley Hospital Easley, South Carolina Discuss recent developments in health systems
Shifting from Blame-&-Shame to a Just-and-Safe Culture
 Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Shifting from Blame-&-Shame to a Just-and-Safe Culture Barb Sproll Medication Safety Pharmacist Winnipeg Regional Health Authority 29 May 2018 Conflict of Interest I have no conflicts to disclose. Objectives:
Hospital Survey on Patient Safety Culture: Debrief and Action Planning
 Hospital Survey on Patient Safety Culture: Debrief and Action Planning August 7, 2018 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association 1 Three
Hospital Survey on Patient Safety Culture: Debrief and Action Planning August 7, 2018 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association 1 Three
Disclosures. assocs.com 2
 May, 2009 Disclosures Courtemanche & Associates Healthcare Synergists is an Approved Provider of continuing nursing education by the North Carolina Nurses Association, an accredited approver by the American
May, 2009 Disclosures Courtemanche & Associates Healthcare Synergists is an Approved Provider of continuing nursing education by the North Carolina Nurses Association, an accredited approver by the American
Targeted Solutions Tools
 TARGETED SOLUTIONS TOOL NOW AVAILABLE FOR OUR INTERNATIONAL CUSTOMERS! Joint Commission Center for Transforming Healthcare Targeted Solutions Tools Hand Hygiene Safe Surgery Hand-off Communications Preventing
TARGETED SOLUTIONS TOOL NOW AVAILABLE FOR OUR INTERNATIONAL CUSTOMERS! Joint Commission Center for Transforming Healthcare Targeted Solutions Tools Hand Hygiene Safe Surgery Hand-off Communications Preventing
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
Patient Safety Overview
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
Paving the Way to High Reliability Healthcare
 Paving the Way to High Reliability Healthcare Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission Ochsner Health System 3 rd Annual Quality and Patient Safety Summit New Orleans,
Paving the Way to High Reliability Healthcare Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission Ochsner Health System 3 rd Annual Quality and Patient Safety Summit New Orleans,
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
High Reliability & Robust Process Improvement
 High Reliability & Robust Process Improvement M. Michael Shabot, MD, FACS, FCCM, FACMI EVP & Chief Clinical Officer, Memorial Hermann Health System Session A16 & B16 The presenters have nothing to disclose
High Reliability & Robust Process Improvement M. Michael Shabot, MD, FACS, FCCM, FACMI EVP & Chief Clinical Officer, Memorial Hermann Health System Session A16 & B16 The presenters have nothing to disclose
ADMINISTRATIVE POLICY & PROCEDURE PATIENT SAFETY PLAN
 PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
COMMON FACTORS CHECKLIST
 COMMON FACTORS CHECKLIST For Identifying Causes and Contributory Factors When attempting to identify potential causes and contributory factors related to an incident or system failure review the following
COMMON FACTORS CHECKLIST For Identifying Causes and Contributory Factors When attempting to identify potential causes and contributory factors related to an incident or system failure review the following
HROs and the Role of Finance South Carolina HFMA Annual Institute
 HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
HROs and the Role of Finance South Carolina HFMA Annual Institute Kari Cornicelli, FHFMA,CPA Vice President/CFO Sharp Metropolitan Medical Campus San Diego, CA 1 Reflection Perfection is not attainable.
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
Designing for Safety
 2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
What is High Reliability, and Why Does Health Care Need It?
 What is High Reliability, and Why Does Health Care Need It? Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission Oklahoma Hospital Association Annual Convention Oklahoma City, OK
What is High Reliability, and Why Does Health Care Need It? Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission Oklahoma Hospital Association Annual Convention Oklahoma City, OK
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
High Reliability Healthcare: A Journey to Zero
 High Reliability Healthcare: A Journey to Zero Arizona Organization of Nurse Executives August 19, 2016 Coleen Smith, RN, MBA, CPHQ, CPPS Objectives Discuss the importance of leaders as agents of change
High Reliability Healthcare: A Journey to Zero Arizona Organization of Nurse Executives August 19, 2016 Coleen Smith, RN, MBA, CPHQ, CPPS Objectives Discuss the importance of leaders as agents of change
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Observations of Implementing the Nuclear Promise for CAP
 Jack Martin Vice President, Consulting BackPacker Jack, Inc.- F-11070 TX Observations of Implementing the Nuclear Promise for CAP A Pendulum Swing in CAP Objectives CAP Regulatory Requirement The evolution
Jack Martin Vice President, Consulting BackPacker Jack, Inc.- F-11070 TX Observations of Implementing the Nuclear Promise for CAP A Pendulum Swing in CAP Objectives CAP Regulatory Requirement The evolution
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Quality Improvement/Systems-based Practice. Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery
 Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
High Reliability Organizations Healing Without Harm by 2014
 Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
Please click your mouse or use the enter button to move onto the next slide High Reliability Organizations Healing Without Harm by 2014 1.1 Stand up if You have suffered harm as a patient at a hospital
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations.
 ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Patient Safety Time for a change in design
 World Congress of Sterilization Milan Italy June 4-7, 2008 Patient Safety Time for a change in design Gina Pugliese, RN, MS Vice President, Premier Safety Institute Associate Faculty University of Illinois
World Congress of Sterilization Milan Italy June 4-7, 2008 Patient Safety Time for a change in design Gina Pugliese, RN, MS Vice President, Premier Safety Institute Associate Faculty University of Illinois
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
These Things (Don t Have to) Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013
 Happen Patient Safety Tami Minnier Chief Quality Officer Friday, April 5, 2013") These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
These Things (Don t Have to) Happen Patient Safety 2013 Tami Minnier Chief Quality Officer Friday, April 5, 2013 Agenda Review the current state of healthcare Define and understand the concept of reliability
Building a Culture That Lasts
 Building a Culture That Lasts Establishing a Leadership Legacy Quality Texas Foundation June 28, 2016 M. Michael Shabot, MD, FACS, FCCM, FACMI Executive Vice President System Chief Clinical Officer V2
Building a Culture That Lasts Establishing a Leadership Legacy Quality Texas Foundation June 28, 2016 M. Michael Shabot, MD, FACS, FCCM, FACMI Executive Vice President System Chief Clinical Officer V2
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
How Should Policy Reflect a Culture of Safety?
 How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
How Should Policy Reflect a Culture of Safety? BETA Healthcare Group BETA HEART Domain I: Culture of Safety All Rights Reserved 2016 Table of Contents How Should Policy Reflect a Culture of Safety?...
Never Events (Including Retained Foreign Objects) The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI
 The Surgeons Point of View. J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI") Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Never Events (Including Retained Foreign Objects) The Surgeons Point of View J.H. Pat Patton, Jr., MD, FACS Henry Ford Hospital, Detroit, MI 1 Disclosures None 2 Learning Objectives Examine the occurrence,
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Translational Safety Through Immersive Learning: Practice What you Preach
 Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
Translational Safety Through Immersive Learning: Practice What you Preach Gregory Botz, MD, FCCM Professor, Department of Critical Care Division of Anesthesiology and Critical Care The University of Texas,
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
Overview of Root Cause Analysis
 Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Checklist: What Can My Organization Do?
 Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Checklist: What Can My Organization Do? 2 Introduction About The Framework This is an evidence and consensus-based framework for successful clinical outcomes in long term and post-acute care. The framework
Accreditation, Quality, Risk & Patient Safety
 Accreditation, Quality, Risk & Patient Safety Accreditation The Joint Commission (TJC) Centers for Medicare & Medicaid Services (CMS) Wyoming Department of Health (DOH) Joint Commission: - Joint Commission
Accreditation, Quality, Risk & Patient Safety Accreditation The Joint Commission (TJC) Centers for Medicare & Medicaid Services (CMS) Wyoming Department of Health (DOH) Joint Commission: - Joint Commission
How Data-Driven Safety Culture Changes Can Lower HAC Rates
 How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
Types of Errors 3/29/12. Approaches of other industries: To err is human, to forgive is divine... Human errors vs. Medical errors vs.
 Medical Errors Management and Early Warning for the Medical Physicist David Hintenlang, Types of Errors Human errors vs. Medical errors vs. Medical events To err is human, to forgive is divine... Approaches
Medical Errors Management and Early Warning for the Medical Physicist David Hintenlang, Types of Errors Human errors vs. Medical errors vs. Medical events To err is human, to forgive is divine... Approaches
LEADERSHIP CHALLENGES IN PATIENT SAFETY
 LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
Yoder-Wise: Leading and Managing in Nursing, 5th Edition
 Yoder-Wise: Leading and Managing in Nursing, 5th Edition Chapter 02: Patient Safety Test Bank MULTIPLE CHOICE 1. In an effort to control costs and maximize revenues, the Rehabilitation Unit at Cross Hospital
Yoder-Wise: Leading and Managing in Nursing, 5th Edition Chapter 02: Patient Safety Test Bank MULTIPLE CHOICE 1. In an effort to control costs and maximize revenues, the Rehabilitation Unit at Cross Hospital
ASM. Common Operations Failure Modes in the Process Industries International Symposium. Dr. Peter Bullemer Human Centered Solutions
 Common Operations Failure Modes in the Process Industries 2009 International Symposium Beyond Regulatory Compliance, Making Safety Second Nature Dr. Peter Bullemer Human Centered Solutions Jason Laberge
Common Operations Failure Modes in the Process Industries 2009 International Symposium Beyond Regulatory Compliance, Making Safety Second Nature Dr. Peter Bullemer Human Centered Solutions Jason Laberge
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Chasing Zero The Journey to Rural Hospital High Reliability
 1 Chasing Zero The Journey to Rural Hospital High Reliability Clint MacKinney, MD, MS Clinical Associate Professor College of Public Health University of Iowa clint-mackinney@uiowa.edu 2 Chasing Zero A
1 Chasing Zero The Journey to Rural Hospital High Reliability Clint MacKinney, MD, MS Clinical Associate Professor College of Public Health University of Iowa clint-mackinney@uiowa.edu 2 Chasing Zero A
NQF. Safe Practices for Better Healthcare SAFE PRACTICES A CONSENSUS REPORT NATIONAL QUALITY FORUM
 THE FOLLOWING SECTIONS ARE IN THIS DOCUMENT Forward......i Table of Contents...iii Executive Summary.v Safe Practices for Better Healthcare-2010 Update: Practice Statement Table...vii Chapter 2: Improving
THE FOLLOWING SECTIONS ARE IN THIS DOCUMENT Forward......i Table of Contents...iii Executive Summary.v Safe Practices for Better Healthcare-2010 Update: Practice Statement Table...vii Chapter 2: Improving
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
TeamSTEPPS Introductory Webinar. July 19, 2018
 TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
Nursing Home Quality Care Collaborative Team Communication. 20 April 2017
 Nursing Home Quality Care Collaborative Team 20 April 2017 Interacting with the Webinar 2 Slides & Recording Registrants were sent a PDF of the slides in advance of the webinar The slides and a recording
Nursing Home Quality Care Collaborative Team 20 April 2017 Interacting with the Webinar 2 Slides & Recording Registrants were sent a PDF of the slides in advance of the webinar The slides and a recording
IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD
 Polskie Towarzystwo Medycyny Ubezpieczeniowej IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD Warsaw, 23.09.2016
Polskie Towarzystwo Medycyny Ubezpieczeniowej IMPORTANCE OF IMPROVING INTERPERSONAL COMMUNICATION SKILLS OF MEDICAL PERSONNEL IN MINIMIZING MEDICAL LIABILITY CLAIMS PIOTR DANILUK, MD Warsaw, 23.09.2016
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Effective Date: January 9, 2017
 Effective Date: January 9, 2017 Overview: The safety and quality of care, treatment, and services depend on many factors, including the following: - A culture that fosters safety as a priority for everyone
Effective Date: January 9, 2017 Overview: The safety and quality of care, treatment, and services depend on many factors, including the following: - A culture that fosters safety as a priority for everyone
Patient Safety in Neurosurgery and Neurology. Andrea Halliday, M.D. Oregon Neurosurgery Specialists
 in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
Sharp HealthCare s HRO Commitment
 Sharp HealthCare s HRO Commitment Daniel L. Gross, DNSc, RN Executive Vice President Amy Adome, MD, MPH Senior Vice President, Clinical Effectiveness November 3, 2016 Perfection is not attainable, but
Sharp HealthCare s HRO Commitment Daniel L. Gross, DNSc, RN Executive Vice President Amy Adome, MD, MPH Senior Vice President, Clinical Effectiveness November 3, 2016 Perfection is not attainable, but
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Centralizing Multi-Hospital Mortality Reviews
 December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
Teaching and Assessing PBL&I and SBP On the Fly. Wisconsin Hospital Visit July 2009
 Teaching and Assessing PBL&I and SBP On the Fly Wisconsin Hospital Visit July 2009 Objectives Demonstrate how to embed the teaching and assessment of PBLI and SBP into daily activity Simple tools Benefits
Teaching and Assessing PBL&I and SBP On the Fly Wisconsin Hospital Visit July 2009 Objectives Demonstrate how to embed the teaching and assessment of PBLI and SBP into daily activity Simple tools Benefits
VA Radiotherapy Incident Reporting and Analysis System (RIRAS)
") VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
Department of Defense Advancement toward High Reliability in Healthcare Awards Program
 Department of Defense Advancement toward High Reliability in Healthcare Awards Program 2018 Application Guidance 1 March 2018 Advancement toward High Reliability in Healthcare Awards Application Guidance
Department of Defense Advancement toward High Reliability in Healthcare Awards Program 2018 Application Guidance 1 March 2018 Advancement toward High Reliability in Healthcare Awards Application Guidance
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
QAPI & Infection Prevention: Putting the Pieces Together
 QAPI & Infection Prevention: Putting the Pieces Together Tammy Baumann, RN, LSSGB Quality Improvement Advisor Great Plains Quality Innovation Network Objectives Identify how QAPI intersects with infection
QAPI & Infection Prevention: Putting the Pieces Together Tammy Baumann, RN, LSSGB Quality Improvement Advisor Great Plains Quality Innovation Network Objectives Identify how QAPI intersects with infection
Guidelines for Managing Pharmacy Systems for Quality and Safety November 2002
 November 2002 Guidelines for Managing Pharmacy Systems for Quality and Safety Background The Australian Council for Safety and Quality in Health Care (ACSQHC) was established by Australian Health Ministers
November 2002 Guidelines for Managing Pharmacy Systems for Quality and Safety Background The Australian Council for Safety and Quality in Health Care (ACSQHC) was established by Australian Health Ministers