Survey on ASA Standards and APSF Recommendations
|
|
|
- Rolf Welch
- 5 years ago
- Views:
Transcription
1 Physician-Patient Alliance for Health & Safety Improving Health & Safety Through Innovation and Awareness Survey on ASA Standards and APSF Recommendations Mike Wong Physician-Patient Alliance for Health & Safety url: September 20, 2011
2 The Physician-Patient Alliance for Health & Safety ( PPAHS ) is an advocacy group devoted to improving patient health and safety. 1 With the purpose of growing awareness and furthering discussion of patient health and safety issues, PPAHS conducted a survey on the American Society of Anesthesiologists ( ASA ) Standards of Basic Anesthetic Monitoring ( ASA Standards ) and the Anesthesia Patient Safety Foundation ( APSF ) conclusions and recommendations ( APSF Recommendations ): - The ASA Standards were in October 2010 updated to read: During moderate or deep sedation the adequacy of ventilation shall be evaluated by continual observation of qualitative clinical signs and monitoring of the presence of exhaled carbon dioxide unless precluded or invalidated by the nature of the patient, procedure, or equipment. The ASA Standards were implemented July 1, The Anesthesia Patient Safety Foundation (APSF) recently issued recommendations and conclusions on electronic monitoring strategies to detect drug-induced postoperative respiratory depression. Among other things, the APSF Recommendations provide, Continuous electronic monitoring of oxygenation and ventilation should be available and considered for all patients and would reduce the likelihood of unrecognized clinically significant opioid-induced depression of ventilation in the postoperative period. 2 This report is divided into the following three discussion parts A. Survey Recommendations B. Detailed Survey Analysis C. Respondent Analysis Appendix A contains a summary of the survey results from Survey Monkey. 1 PPAHS is inspired by Howard Snitzer, who survived 96 minutes without a heart beat. Howardʼs resuscitation by volunteer paramedics and Dr Roger White at the Mayo Clinic is a truly remarkable story. For more on Howard Snitzerʼs resuscitation, please see 2 For more on these recommendations, please see /2
3 Survey Recommendations From the results of the survey, two immediate action steps are apparent and recommended: Encourage Monitoring of All Post-Surgical Patients Almost all respondents (90%) believe continuous electronic monitoring of oxygenation and ventilation should be available and considered for all patients. Such monitoring would reduce the likelihood of unrecognized clinically significant opioid-induced depression of ventilation in the postoperative period. As explained by Dr. Daniel Sessler, who is Professor and Chair of the Department of Outcomes Research at the Cleveland Clinic, and Director of the Outcomes Research Consortium which is anesthesiaʼs largest academic research organization: Continuous respiratory monitoring, including the use of both capnography and pulse oximetry, is essential for the safe administration of patientcontrolled analgesics.a patient experiencing respiratory depression, if undetected, can easily progress to respiratory arrest and consequent brain damage or death. Develop and Distribute a Safety Checklist Almost all the respondents (85%) favor the development and use of safety checklists. An example of a checklist is the surgical checklist that was created and is being promoted by the WHO 3 and through the efforts of Dr Atul Gawande 4. As their experience illustrates, focusing on common process failures is where a safety checklist would have great benefit in improving patient health and safety. To support the call for the monitoring of all patients post-surgically, a safety checklist should focus on a common failure with patients after surgery. One such area is patientcontrolled analgesia. According to the study by Dr Thomas McCarter and his colleagues published in America Health & Drug Benefits: 5 Capnographic monitoring and automatic pausing of patient-controlled analgesia improved postoperative outcomes in situations that could have otherwise been fatal. Use of capnography improved clinician confidence that opioid dosing could be safely continued in postoperative patients for more effective pain management Dr Atul Gawande, The Checklist Manifesto (2009) 5 For more details, please see /3
. Respondents answered the Survey over an approximate two week period beginning August 26, 2011.")
4 Detailed Survey Analysis The Survey was sent to doctors, nurses, hospital administrators, other healthcare providers, and advocates (for an analysis of respondents, please see the next section Respondent Analysis ). Respondents answered the Survey over an approximate two week period beginning August 26, The Survey consisted of eight questions: Question 1 asked respondents to self-identify themselves. An analysis of Survey respondents is provided in the next section Respondent Analysis. Six substantive questions (i.e. Questions 2 to 7), which are discussed in detail below. Question 8 asked whether the respondent wanted to receive a copy of this report, as well whether they wanted to be entered into a draw to win a randomly drawn ipad offered by a PPAHS supporter. Question 2 As of July 1, 2011, I would describe the medical practices, of which I am aware, to be in accord with ASA Standards as Completely Mostly Partially 6 Although the survey did remain open for responding to after midnight of September 9, 2011, for the purposes of this Report the cut off date was midnight CT of September 9, /4
5 66.2% of respondents indicated that that the medical practices of which they are aware are completely in accord with ASA Standards. However, 33.8% answered mostly or partially, which would seem to indicate a non-compliance issue. There are two conclusions to be drawn from these results. First, there is need for improvement. Even though this is a subjective question and is reliant upon the personal knowledge and information of the respondent, anything short of 100% responding completely indicates that there is room for improvement in how healthcare facilities adhere to ASA Basic Monitoring Standards. As noted by Dr Richard Dutton (executive director of the Anesthesia Quality Institute): The safety of patients under anesthesia is extremely good, and the majority who believe that ASA Standards have been completely implemented is an indication of this. However, a significant minority clearly see room and areas for improvement, and I would concur with their observations. Quality of anesthesia provision can affect patient safety, quality outcomes, and finances facility. With the goal that no patient shall be harmed from anesthesia, healthcare facilities need to continually locate and deal with those areas. Second, some respondents may have been thinking of the application of ASA Standards outside of the operating room. For example, while there may be complete compliance inside operating rooms, there may not be compliance outside of the operating room. This would seem to be supported by some comments that were received regarding how to improve compliance with ASA Standards that referred to remote locations and the need for more capnography equipment: some remote non OR locations do not allow all ASA monitors (e.g. temp in mri) need to get enough capnometry monitoring to supply our "off-site" locations where we do MAC cases /5

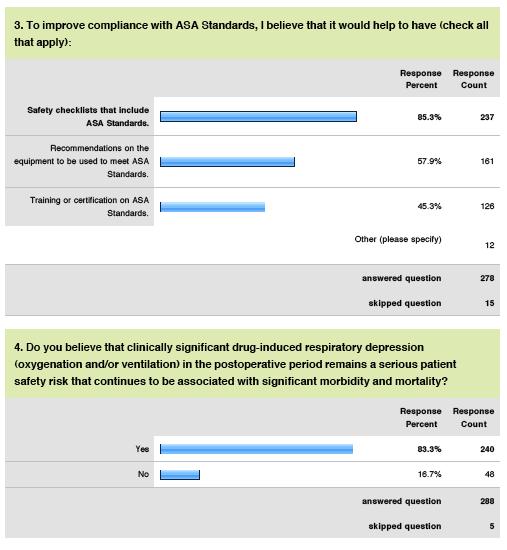
6 Question 3 To improve compliance with ASA Standards, I believe that it would help to have (check all that apply) Safety checklists that include ASA Standards. Recommendations on the equipment to be used to meet ASA Standards. Training or certification on ASA Standards. This three part question first underscores the need for safety checklists. Almost all the respondents (85%) believe that safety checklists would improve compliance with ASA Standards. A surgical safety checklist was created and is now being used thanks to the WHO 7 and the efforts of Dr Atul Gawande 8. So, it is unlikely that respondents were referring to the need for a checklist in the operating room, but one that would address common failure problems post-surgery. As a result, PPAHS is putting together a working group to create a checklist focused on patient-controlled analgesia. From 1999 to 2007, the number of U.S. poisoning deaths involving any opioid analgesic (e.g., oxycodone, methadone, or hydrocodone) more than tripled, from 4,041 to 14,459, or 36% of the 40,059 total poisoning deaths in In 1999, opioid analgesics were involved in 20% of the 19,741 poisoning deaths. During , the number of poisoning deaths involving specified drugs other than opioid analgesics increased from 9,262 to 12,790, and the number involving non-specified drugs increased from 3,608 to 8,947. According to the study by Dr Thomas McCarter and his colleagues published in America Health & Drug Benefits: 9 Capnographic monitoring and automatic pausing of patient-controlled analgesia improved postoperative outcomes in situations that could have otherwise been fatal. Use of capnography improved clinician confidence that opioid dosing could be safely continued in postoperative patients for more effective pain management Dr Atul Gawande, The Checklist Manifesto (2009) 9 For more details, please see /6
7 Moreover, better monitoring of patients using PCA pumps has been shown to improve patient safety and produce a significant return on investment. According to the study Intravenous Infusion Safety Technology: Return on Investment, 10 St. Josephʼs/Candler Health System 11 found out that the costs over a 5-year period of implementing a patient safety initiative was the prevention of at least 471 adverse events, a return on investment of $1.87 million, an internal rate of return of 81%. Second, respondents (58%) saw the need for recommendations on the equipment to be used to meet ASA Standards. While it may seem to be an obvious point, clearly knowing what equipment should best be used to for patients to be ʻevaluated by continual observation of qualitative clinical signs and monitoring of the presence of exhaled carbon dioxide would be helpful. Perhaps what people are asking is whether it would have been so hard to say, for example, use capnography to monitor for the presence of exhaled carbon dioxide? Third, 44% of respondents saw the need for training or certification on ASA Standards. As Dr Philip Lumb (Chair of Anesthesiology, Keck School of Medicine) said, Continuing education should be provided for all individuals taking care of patients who have received procedural anesthesia/sedation. Special emphasis should be given to 'nontraditional' areas outside the purview of normal operating room and perioperative procedures and surveillance. This is increasingly important for office-based practices, interventional suites (GI, Radiology, etc) and ambulatory surgery centers. In summary, the sentiment of a patient advocate should be noted: I believe you can't have too much training or too many checklists and equipment being checked should be a given 10 For more information, please see /7
8 Question 4 Do you believe that clinically significant drug-induced respiratory depression (oxygenation and/or ventilation) in the postoperative period remains a serious patient safety risk that continues to be associated with significant morbidity and mortality? 83.3% of respondents believe that clinically significant drug-induced respiratory depression (oxygenation and/or ventilation) in the postoperative period remains a serious patient safety risk that continues to be associated with significant morbidity and mortality. Because a substantial majority believes that drug-induced respiratory depression continues to be a patient safety issue, this poses interesting questions for the 16.7% who answered no : Have they figured it out? in the sense that in their healthcare facility, drug-induced respiratory depression is no longer an issue; or Are they not recognizing it? As one prominent neuroanesthesiologist ed PPAHS on this question, We should stop the found dead in bed syndrome. An argument for a non-recognition factor is supporter in the response to Question 7 (see below), where 61% believe that caregivers are failing to recognize the true risk of drug-induced depression of ventilation. /8

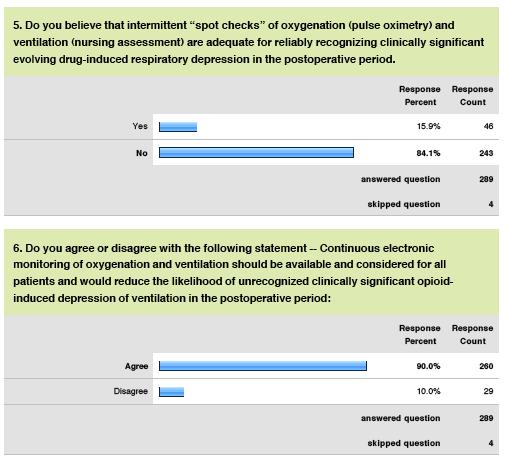
9 Question 5 Do you believe that intermittent spot checks of oxygenation (pulse oximetry) and ventilation (nursing assessment) are adequate for reliably recognizing clinically significant evolving drug-induced respiratory depression in the postoperative period 84.1% of respondents believe that intermittent spot checks are not adequate, which answer is consistent with the 83.3% who believe that drug-induced respiratory depression (oxygenation and/or ventilation) in the postoperative period remains a serious patient safety risk (see Question 4). The answer to this question is interesting, not so much in the fact that 84.1% do not believe that intermittent spot checks are adequate, but that a sizable minority (15.9%) are in disagreement with their fellow practitioners and believe that these spot checks are adequate. /9
10 Question 6 Do you agree or disagree with the following statement -- Continuous electronic monitoring of oxygenation and ventilation should be available and considered for all patients and would reduce the likelihood of unrecognized clinically significant opioid-induced depression of ventilation in the postoperative period Almost all respondents (90%) believe continuous electronic monitoring of oxygenation and ventilation should be available and considered for all patients. Such monitoring would reduce the likelihood of unrecognized clinically significant opioid-induced depression of ventilation in the postoperative period. What is interesting about this response is the 10% who believe that continuous electronic monitoring of oxygenation and ventilation should not be available and considered for all patients. As one medical director for a surgical intensive care unit of a prominent healthcare provider ed, I am quite shocked that the disagree group is that high! In practice, for example, some patients may not be continuously monitored electronically because they may not have been identified as having risks associated with obstructive sleep apnea, obesity, or chronic opioid therapy. Perhaps, as one anesthesiologist ed PPAHS, continuous monitoring is available and being considered, but not applied. However, in such cases, respondents should have more properly answered agree that monitoring is being considered, as the question was not whether monitoring was being applied to all patients. As a medical director for inpatient pain service at a prominent hospital ed: /10
11 Of course these monitors "should be available and considered" but since clinically significant respiratory depression events, ie. hypoxemia or hypercapnia/acidosis requiring naloxone, are rare, I would only encourage routine or mandatory use of the "available" monitors on the highest risk patients. I don't think it's feasible or necessary for "all" patients. However, more importantly, what 90% of respondents seem to be saying is that all patients should be continuously monitored. This was certainly the sentiment in direct Twitter messages and s from healthcare providers and others on this question. As a physician at a well-known childrenʼs hospital ed: All post-operative patients should be monitored. According to the HealthGrades study of patient safety in American hospitals, 12 failure to rescue and postoperative respiratory failure (also known as Code Blue ) are the first and third most common patient safety related adverse events affecting Medicare patients accounting for 113 events per 1,000 at-risk patient admissions. These adverse events which affect both Medicare and non-medicare patients result in death or anoxic brain injury in the majority of cases, observes Dr. Daniel Sessler, who is Professor and Chair of the Department of Outcomes Research at the Cleveland Clinic, and Director of the Outcomes Research Consortium which is anesthesiaʼs largest academic research organization. The Consortium conducts research in anesthesia, critical care, and comprehensive pain management. Continuous respiratory monitoring, including the use of both capnography and pulse oximetry, is essential for the safe administration of patient-controlled analgesics, explains Professor Sessler. A patient experiencing respiratory depression, if undetected, can easily progress to respiratory arrest and consequent brain damage or death HealthGradesPatientSafetyInAmericanHospitalsStudy2011.pdf /11
 the true risk of druginduced depression of ventilation Absence of evidence-based data to support")
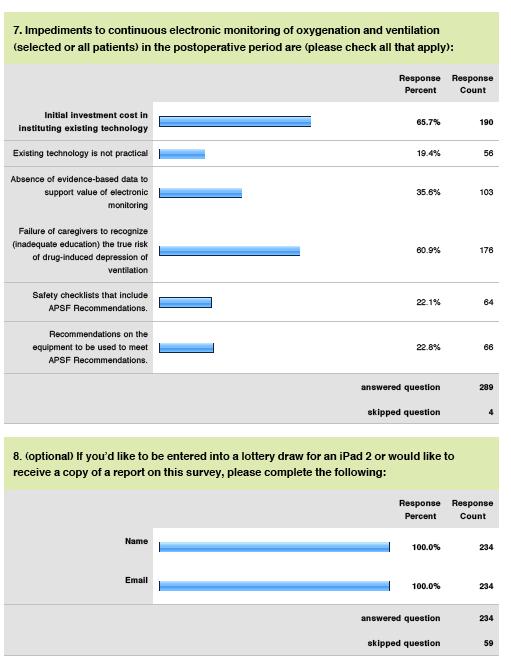
12 Question 7 Impediments to continuous electronic monitoring of oxygenation and ventilation (selected or all patients) in the postoperative period are (please check all that apply) Initial investment cost in instituting existing technology Failure of caregivers to recognize (inadequate education) the true risk of druginduced depression of ventilation Absence of evidence-based data to support value of electronic monitoring (55.6%) Existing technology is not practical Recommendations on the equipment to be used to meet APSF Recommendations Safety checklists that include APSF Recommendations This question explores the impediments to continuous electronic monitoring of oxygenation and ventilation. Answers to this question reveal two main areas of interest or, if you will, concern. The first is on the technology. The majority believe that the technology is practical (80.6%). In other words, from a use point of view, there does not seem to be a concern about existing technology (pulse oximetry or capnography). However, a major impediment to adoption of continuous monitoring is cost (with 65.7% expressing this concern). The second relates to awareness and the belief that caregivers are failing to recognize the true risk of drug-induced depression of ventilation, with 61% expressing this concern (please see chart on next page). It is unlikely that the respondents are saying that caregivers do not know drug-induced respiratory depression when they see it, but they may not be recognizing the risk when it occurs. Continuous electronic monitoring of all patients (as suggested in response to Question 6) would eliminate this risk of nonidentification. /12

13 /13
 are healthcare providers, with about three-quarters of these being doctors and the rest nurses or physician assistants.")
14 Respondent Analysis 293 people responded to the survey. Almost all the respondents (285 or 97.2%) are healthcare providers, with about three-quarters of these being doctors and the rest nurses or physician assistants. The remainder were healthcare administrators, patient advocates, or in some way related to the healthcare system. Moreover, most of the respondents (about 60%) indicated anesthesiology as their medical practice. Other practice areas represented were pediatric/neonatal (22%) and critical care (8%). In addition, other specialities represented constituted about 8% of the respondents indicating such areas as radiology, pulmonology, surgery, and neurology. /14

15 Appendix A /15
16 /16
17 /17
18 /18
Statement on Safe Use of Propofol (Approved by ASA House of Delegates on October 27, 2004);
;") CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
9/8/2014. I have no conflicts of interest to disclose. Conflict of Interest Disclosure. Carrie Brunson: Except
 ENSURING OPIOID SAFETY: DO OUR NURSES POSSESS THE KNOWLEDGE Click to add subtitle TO RESCUE PATIENTS? Carrie Brunson MSN, APRN-BC, ACNS-BC Clinical Nurse Specialist Acute Pain Service September 2014 ASPMN
ENSURING OPIOID SAFETY: DO OUR NURSES POSSESS THE KNOWLEDGE Click to add subtitle TO RESCUE PATIENTS? Carrie Brunson MSN, APRN-BC, ACNS-BC Clinical Nurse Specialist Acute Pain Service September 2014 ASPMN
Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications
 Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications March 14, 2016 AAMI Foundation Vision: To drive the safe
Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications March 14, 2016 AAMI Foundation Vision: To drive the safe
We See You When You're Sleeping
 We See You When You're Sleeping Addressing Patient Safety Risks Surrounding Opioid-Induced Sedation Jeanne J. Venella DNP, MS, CEN, CPEN November 30 th, 2016 1 Objectives Review the current state of opioids
We See You When You're Sleeping Addressing Patient Safety Risks Surrounding Opioid-Induced Sedation Jeanne J. Venella DNP, MS, CEN, CPEN November 30 th, 2016 1 Objectives Review the current state of opioids
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures
 procedures") Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
1. Introduction. 1 CMS section
 1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ANESTHESIA CARE AND INTRAOPERATIVE Job Title of Responsible Owner: EFFECTIVE DATE: REVIEW/REVISED DATE: TYPE: Director of Perioperative
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ANESTHESIA CARE AND INTRAOPERATIVE Job Title of Responsible Owner: EFFECTIVE DATE: REVIEW/REVISED DATE: TYPE: Director of Perioperative
PROCEDURAL SEDATION AND ANALGESIA: HOSPITAL-WIDE POLICY
 CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Anesthesia
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
STATEMENT ON GRANTING PRIVILEGES FOR ADMINISTRATION OF MODERATE SEDATION TO PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS
 NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
Advisory on Granting Privileges for Deep Sedation to Non-Anesthesiologist Physicians
 Advisory on Granting Privileges for Deep Sedation to Non-Anesthesiologist Physicians Committee of Origin: Quality Management and Departmental Administration (Approved by the ASA House of Delegates on October
Advisory on Granting Privileges for Deep Sedation to Non-Anesthesiologist Physicians Committee of Origin: Quality Management and Departmental Administration (Approved by the ASA House of Delegates on October
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER
 APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER We are carrying out a survey to establish the quality of anaesthesia care provided to Obstetric patients in East Africa. We therefore
APPENDIX I QUESTIONNAIRE FOR INTERVIEWING THE ANAESTHESIA PROVIDER We are carrying out a survey to establish the quality of anaesthesia care provided to Obstetric patients in East Africa. We therefore
APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that apply)
: (Check all that apply)") POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
Just this past October, the ASA House of
 Monitoring Exhaled Carbon Dioxide: Understanding the Implications of the Revised ASA Standards By Kenneth Y. Pauker, M.D., President-elect, Associate Editor Just this past October, the ASA House of Delegates
Monitoring Exhaled Carbon Dioxide: Understanding the Implications of the Revised ASA Standards By Kenneth Y. Pauker, M.D., President-elect, Associate Editor Just this past October, the ASA House of Delegates
General OR-Stanford-CA-1 revised: Tuesday, February 02, 2016
 Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Anesthesia Services Policy
 Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
The ASA defines anesthesiology as the practice of medicine dealing with but not limited to:
 1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Opioid Safety & Patient Monitoring Conference Compendium
 Opioid Safety & Patient Monitoring Conference Compendium The National Coalition to Promote Continuous Monitoring of Patients on Opioids November 14, 2014 Chicago, IL Author: Jill Schlabig Williams, JSW
Opioid Safety & Patient Monitoring Conference Compendium The National Coalition to Promote Continuous Monitoring of Patients on Opioids November 14, 2014 Chicago, IL Author: Jill Schlabig Williams, JSW
AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN RECOMMENDATIONS ON MONITORING DURING ANAESTHESIA
 Review PS18 (2008) AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 RECOMMENDATIONS ON MONITORING DURING ANAESTHESIA The terms Anaesthetist, medical practitioner and practitioner
Review PS18 (2008) AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 RECOMMENDATIONS ON MONITORING DURING ANAESTHESIA The terms Anaesthetist, medical practitioner and practitioner
JOHNS HOPKINS HEALTHCARE Physician Guidelines
 Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY. Dr. Paul Vercruysse M.D. Belgium
 ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Policies and Procedures. Title:
 Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
The Digital ICU: Return On Innovation
 The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
Anesthesiology 302 Introduction to Anesthesia Goals and Objectives
 Anesthesiology 302 Introduction to Anesthesia Goals and Objectives I. The student will be able to perform an appropriate preoperative evaluation, including history, physical exam, and appropriate use of
Anesthesiology 302 Introduction to Anesthesia Goals and Objectives I. The student will be able to perform an appropriate preoperative evaluation, including history, physical exam, and appropriate use of
Procedural Sedation and Analgesia
 Procedural Sedation and Analgesia Document Owner: Diana McDowell Version: 8 Effective Date: 10/23/2015 Revision Date: 10/23/2018 Approvers: Smith, Kevin Lee; Calkins, Paul; DelBoccio, Suzanne; Cottrell,
Procedural Sedation and Analgesia Document Owner: Diana McDowell Version: 8 Effective Date: 10/23/2015 Revision Date: 10/23/2018 Approvers: Smith, Kevin Lee; Calkins, Paul; DelBoccio, Suzanne; Cottrell,
Partial Dissent of Independent Assessment Committee Report Orillia Soldiers Memorial Hospital and Ontario Nurses Association
 In my expert opinion, the nursing staffing model in the OSMH Pre-Admission Clinic should be two (2) Registered Nurses. I strongly disagree with the recommendation of my colleagues on the Independent Assessment
In my expert opinion, the nursing staffing model in the OSMH Pre-Admission Clinic should be two (2) Registered Nurses. I strongly disagree with the recommendation of my colleagues on the Independent Assessment
University of Minnesota Anesthesiology Residency Program PEDIATRIC ANESTHESIA ROTATION GOALS AND OBJECTIVES
 University of Minnesota Anesthesiology Residency Program PEDIATRIC ANESTHESIA ROTATION GOALS AND OBJECTIVES Goals: The overall goal of the rotation is to provide an introduction and understanding of the
University of Minnesota Anesthesiology Residency Program PEDIATRIC ANESTHESIA ROTATION GOALS AND OBJECTIVES Goals: The overall goal of the rotation is to provide an introduction and understanding of the
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Highmark Reimbursement Policy Bulletin
 Highmark Reimbursement Policy Bulletin Bulletin Number: Subject: RP-033 Anesthesia Services Effective Date: March 12, 2018 End Date: Issue Date: June 11, 2018 Source: Reimbursement Policy Applicable Commercial
Highmark Reimbursement Policy Bulletin Bulletin Number: Subject: RP-033 Anesthesia Services Effective Date: March 12, 2018 End Date: Issue Date: June 11, 2018 Source: Reimbursement Policy Applicable Commercial
University of Virginia Medical Center Clinical Protocol for Moderate or Deep Sedation/Analgesia in Adult Patients
 A. PURPOSE University of Virginia Medical Center Clinical Protocol for Moderate or Deep Sedation/Analgesia in Adult Patients Sedation and analgesia are used alone or in combination to facilitate the performance
A. PURPOSE University of Virginia Medical Center Clinical Protocol for Moderate or Deep Sedation/Analgesia in Adult Patients Sedation and analgesia are used alone or in combination to facilitate the performance
Summary of Workshop Presentations
 NEWSLETTER www.apsf.org The Official Journal of the Anesthesia Patient Safety Foundation Volume 21, No. 4, 61-88 Circulation 80,350 Winter 2006-2007 Dangers of Postoperative Opioids APSF Workshop and White
NEWSLETTER www.apsf.org The Official Journal of the Anesthesia Patient Safety Foundation Volume 21, No. 4, 61-88 Circulation 80,350 Winter 2006-2007 Dangers of Postoperative Opioids APSF Workshop and White
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
Cost Effectiveness of Physician Anesthesia J.P. Abenstein, M.S.E.E., M.D. Mayo Clinic Rochester, MN
 Mayo Clinic Rochester, MN Introduction The question of whether anesthesiologists are cost-effective providers of anesthesia services remains an open question in the minds of some of our medical colleagues,
Mayo Clinic Rochester, MN Introduction The question of whether anesthesiologists are cost-effective providers of anesthesia services remains an open question in the minds of some of our medical colleagues,
Department of Anesthesiology Anesthesia Curriculum Clinical Base Year
 Anesthesia Curriculum Clinical Base Year Description of Rotation The goal of this month long rotation is to teach the basic skills of anesthesia and to provide a foundation on which to build the initial
Anesthesia Curriculum Clinical Base Year Description of Rotation The goal of this month long rotation is to teach the basic skills of anesthesia and to provide a foundation on which to build the initial
Chinwe Nwosu, GE/NMF Scholar Supervisor: Dr. Stephen Ttendo, Senior Lecturer/ Head of Department of Anesthesia
 Chinwe Nwosu, GE/NMF Scholar Supervisor: Dr. Stephen Ttendo, Senior Lecturer/ Head of Department of Anesthesia According to the Uganda Ministry of Health 2010 Clinical Guidelines Read the notes/ medical
Chinwe Nwosu, GE/NMF Scholar Supervisor: Dr. Stephen Ttendo, Senior Lecturer/ Head of Department of Anesthesia According to the Uganda Ministry of Health 2010 Clinical Guidelines Read the notes/ medical
Client Alert. CMS Clarifies Interpretive Guidelines for Hospitals Providing Anesthesia Services
 Contact Attorneys Regarding This Matter: Mark A. Guza 404.873.8796 - direct 404.873.8797 - fax mark.guza@agg.com Diana Rusk Cohen 404.873.8108 - direct 404.873.8109 - fax diana.cohen@agg.com Client Alert
Contact Attorneys Regarding This Matter: Mark A. Guza 404.873.8796 - direct 404.873.8797 - fax mark.guza@agg.com Diana Rusk Cohen 404.873.8108 - direct 404.873.8109 - fax diana.cohen@agg.com Client Alert
Anesthesia Elective Curriculum Outline
 Department of Internal Medicine Texas Tech University Health Sciences Center Odessa, Texas Anesthesia Elective Curriculum Outline Revision Date: July 10, 2006 Approved by Curriculum Meeting September 19,
Department of Internal Medicine Texas Tech University Health Sciences Center Odessa, Texas Anesthesia Elective Curriculum Outline Revision Date: July 10, 2006 Approved by Curriculum Meeting September 19,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Position Paper on Anesthesia Assistants: An Official Position Paper of the Canadian Anesthesiologists Society
 Can J Anesth/J Can Anesth (2018) Appendix 5 Position Paper on Anesthesia Assistants: An Official Position Paper of the Canadian Anesthesiologists Society Background Medical and surgical care has become
Can J Anesth/J Can Anesth (2018) Appendix 5 Position Paper on Anesthesia Assistants: An Official Position Paper of the Canadian Anesthesiologists Society Background Medical and surgical care has become
ADE Webinar Series. May 7, Patient Stories and Best Practices. Preventing Opioid-Related Adverse Events:
 ADE Webinar Series May 7, 2013 Preventing Opioid-Related Adverse Events: Patient Stories and Best Practices Speakers: L. Alexander, D. Fox, M. Loflin, M. Parmenter, M. Wong Introduction Lenore Alexander,
ADE Webinar Series May 7, 2013 Preventing Opioid-Related Adverse Events: Patient Stories and Best Practices Speakers: L. Alexander, D. Fox, M. Loflin, M. Parmenter, M. Wong Introduction Lenore Alexander,
Session 2 Improving Narcotics and Opiate Management
 Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
A Centralized Monitoring Approach to Pulse Oximetry for Patients on Opioids
 A Centralized Monitoring Approach to Pulse Oximetry for Patients on Opioids Phyllis J. Miller About the Author Phyllis J. Miller, MS, RN, FHCE, is an independent nursing consultant. At the time this article
A Centralized Monitoring Approach to Pulse Oximetry for Patients on Opioids Phyllis J. Miller About the Author Phyllis J. Miller, MS, RN, FHCE, is an independent nursing consultant. At the time this article
Protocol/Procedure XX. Title: Procedural Sedation/Moderate Sedation
 Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
Protocol/Procedure XX Title: Procedural Sedation/Moderate Sedation A. DEFINITION Procedural Moderate Sedation/Analgesia is a drug-induced depression of consciousness during which patients respond purposefully
Continuous Monitoring For Patients on Opioids
 Saving Lives, Saving Families Continuous Monitoring For Patients on Opioids Jill Williams About the Author A National Effort Jill Schlabig Williams is a freelance writer based in Kentucky. E-mail: jill.
Saving Lives, Saving Families Continuous Monitoring For Patients on Opioids Jill Williams About the Author A National Effort Jill Schlabig Williams is a freelance writer based in Kentucky. E-mail: jill.
Complications Associated with Anesthesia for Gynecology: A Prospective Survey in Oran Algeria
 ISPUB.COM The Internet Journal of Health Volume 6 Number 2 Complications Associated with Anesthesia for Gynecology: A Prospective Survey in Oran Algeria M Khdidja Citation M Khdidja. Complications Associated
ISPUB.COM The Internet Journal of Health Volume 6 Number 2 Complications Associated with Anesthesia for Gynecology: A Prospective Survey in Oran Algeria M Khdidja Citation M Khdidja. Complications Associated
APC 20 Procedural Sedation Analgesia by Non-Anesthesia Provider. Assessment & Provision of Care
 APC 20 Procedural Sedation Analgesia by Non-Anesthesia Provider Policy Executive: VP Medical Affairs/CMO Patient Care Policy Assessment & Provision of Care Policy Owner: Director Nursing ATTACHMENTS: 1.
APC 20 Procedural Sedation Analgesia by Non-Anesthesia Provider Policy Executive: VP Medical Affairs/CMO Patient Care Policy Assessment & Provision of Care Policy Owner: Director Nursing ATTACHMENTS: 1.
Production pressures are the overt or covert pressures and incentives
 Keeping Patient Safety First While Responding to Production Pressure Production pressures are the overt or covert pressures and incentives on personnel to place production, not safety, as their primary
Keeping Patient Safety First While Responding to Production Pressure Production pressures are the overt or covert pressures and incentives on personnel to place production, not safety, as their primary
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty
 Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
Perioperative Essentials for Early Discharge and Outpatient Total Joint Arthroplasty R. Michael Meneghini MD Associate Professor of Orthopaedic Surgery Indiana University School of Medicine Indianapolis,
STATEMENT ON THE ANESTHESIA CARE TEAM
 Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
Anesthesia Policy. Approved By 3/08/2017
 REIMBURSEMENT POLICY Anesthesia Policy Policy Number 2018R0032B Annual Approval Date 3/08/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are
REIMBURSEMENT POLICY Anesthesia Policy Policy Number 2018R0032B Annual Approval Date 3/08/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are
The residents will work at WVU Ruby Memorial under the supervision of departmental faculty.
 CA-2 Intermediate Clinical Training (ICT) Curriculum Department of Anesthesiology Description of Rotation The goal of this multi-month rotation is to build upon the essential skills learned in the BCT
CA-2 Intermediate Clinical Training (ICT) Curriculum Department of Anesthesiology Description of Rotation The goal of this multi-month rotation is to build upon the essential skills learned in the BCT
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE
 ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
ROTATION SUMMARY PEDIATRIC ANESTHESIA ELECTIVE Rotation Contacts and Scheduling Details Rotation Director: Kelly Yeh, MD Director of Pediatric Anesthesia Santa Clara Valley Medical Center kelly.yeh@hhs.sccgov.org.,
9/29/2017. Enhanced Recovery After Surgery at the University of Virginia Medical Center. Disclosures. Objectives. None
 Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Anesthesia Policy REIMBURSEMENT POLICY CMS Reimbursement Policy Oversight Committee. Policy Number. Annual Approval Date. Approved By 2018R0032B
 REIMBURSEMENT POLICY CMS-1500 Policy Number 2018R0032B Annual Approval Date Anesthesia Policy 3/14/2018 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
REIMBURSEMENT POLICY CMS-1500 Policy Number 2018R0032B Annual Approval Date Anesthesia Policy 3/14/2018 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
ALARM MANAGEMENT ON AN INPATIENT SURGICAL UNIT. Rhyana Rose Whiteley
 ALARM MANAGEMENT ON AN INPATIENT SURGICAL UNIT by Rhyana Rose Whiteley A professional paper submitted in partial fulfillment of the requirements for the degree of Master of Nursing MONTANA STATE UNIVERSITY
ALARM MANAGEMENT ON AN INPATIENT SURGICAL UNIT by Rhyana Rose Whiteley A professional paper submitted in partial fulfillment of the requirements for the degree of Master of Nursing MONTANA STATE UNIVERSITY
2.5 ANCC/AACN CONTACT HOURS. Shades of BY ANNE B. HALLIDAY, RN, CPAN, BSN. 36 Nursing2006, Volume 36, Number 4
 2.5 ANCC/AACN CONTACT HOURS Shades of BY ANNE B. HALLIDAY, RN, CPAN, BSN 36 Nursing2006, Volume 36, Number 4 www.nursing2006.com sedation Learning about moderate sedation and analgesia Find out about the
2.5 ANCC/AACN CONTACT HOURS Shades of BY ANNE B. HALLIDAY, RN, CPAN, BSN 36 Nursing2006, Volume 36, Number 4 www.nursing2006.com sedation Learning about moderate sedation and analgesia Find out about the
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Procedural Sedation
TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Procedural Sedation
By Yvonne D Arcy, CRNP, CNS, MS
 2.0 ANCC/AACN CONTACT HOURS Keep your patient By Yvonne D Arcy, CRNP, CNS, MS PATIENT-CONTROLLED ANALGESIA (PCA), an attractive short-term option for managing acute postoperative pain, puts the patient
2.0 ANCC/AACN CONTACT HOURS Keep your patient By Yvonne D Arcy, CRNP, CNS, MS PATIENT-CONTROLLED ANALGESIA (PCA), an attractive short-term option for managing acute postoperative pain, puts the patient
Actionable Patient Safety Solution (APSS) #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION
 #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION") Actionable Patient Safety Solution (APSS) #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION Table of Contents Executive Summary Checklist 2 The Performance Gap 3 Leadership Plan
Actionable Patient Safety Solution (APSS) #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION Table of Contents Executive Summary Checklist 2 The Performance Gap 3 Leadership Plan
Opioid Sedation Comparison Study
 Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
COMMITTEE ON QUALITY MANAGEMENT AND DEPARTMENTAL ADMINISTRATION AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIOLOGY DEPARTMENT QUALITY CHECKLIST
 COMMITTEE ON QUALITY MANAGEMENT AND DEPARTMENTAL ADMINISTRATION AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIOLOGY DEPARTMENT QUALITY CHECKLIST The following series of questions has been developed by
COMMITTEE ON QUALITY MANAGEMENT AND DEPARTMENTAL ADMINISTRATION AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIOLOGY DEPARTMENT QUALITY CHECKLIST The following series of questions has been developed by
Your Anesthesiologist, Anesthesia and Pain Control
 You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
DEACONESS HOSPITAL, INC. Evansville, Indiana DEPARTMENT OF ANESTHESIOLOGY RULES & REGULATIONS
 DEACONESS HOSPITAL, INC. Evansville, Indiana DEPARTMENT OF ANESTHESIOLOGY RULES & REGULATIONS I. Department Organization and Direction - The Department of Anesthesiology shall be properly organized, directed
DEACONESS HOSPITAL, INC. Evansville, Indiana DEPARTMENT OF ANESTHESIOLOGY RULES & REGULATIONS I. Department Organization and Direction - The Department of Anesthesiology shall be properly organized, directed
Community Hospital Perspective
 Pediatric Perioperative Environment: Should Hospitals and Anesthesia Practitioners Have Performance-Based Credentialing. The California Experience: Wave of the Future? Introduction. Community Hospital
Pediatric Perioperative Environment: Should Hospitals and Anesthesia Practitioners Have Performance-Based Credentialing. The California Experience: Wave of the Future? Introduction. Community Hospital
Within the Scope of Practice/Role of X APRN X RN LPN CNA ADVISORY OPINION MANAGEMENT OF ANALGESIA BY CATHETER IN THE PREGNANT CLIENT
 Wyoming State Board of Nursing 130 Hobbs Avenue, Suite B Cheyenne, WY 82002 Phone (307) 777-7601 Fax (307) 777-3519 E-Mail: wsbn-info-licensing@wyo.gov Home Page: https://nursing-online.state.wy.us/ OPINION:
Wyoming State Board of Nursing 130 Hobbs Avenue, Suite B Cheyenne, WY 82002 Phone (307) 777-7601 Fax (307) 777-3519 E-Mail: wsbn-info-licensing@wyo.gov Home Page: https://nursing-online.state.wy.us/ OPINION:
Silent Danger. Opioids, PCA Pumps, and the Case for Continuous Monitoring
 Copyright AAMI 2013. Single user license only. Copying, networking, and distribution prohibited. Silent Danger Opioids, PCA Pumps, and the Case for Continuous Monitoring Martha Vockley When 18-year-old
Copyright AAMI 2013. Single user license only. Copying, networking, and distribution prohibited. Silent Danger Opioids, PCA Pumps, and the Case for Continuous Monitoring Martha Vockley When 18-year-old
Malpractice Litigation & Human Errors. National Practitioners Data Bank. Judging Clinical Competence. Judging Physician Competence.
 Judging Clinical Competence Robert S. Lagasse, MD Professor & Vice Chair Quality Management & Regulatory Affairs Department of Anesthesiology Yale School of Medicine New Haven, CT 64 th Annual Postgraduate
Judging Clinical Competence Robert S. Lagasse, MD Professor & Vice Chair Quality Management & Regulatory Affairs Department of Anesthesiology Yale School of Medicine New Haven, CT 64 th Annual Postgraduate
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
SAMPLE Perioperative Self-Assessment Questionnaire
 SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
SAMPLE Perioperative Self-Assessment Questionnaire Hospital Name: Person Completing the Assessment: Date: I. Executive Leadership Yes No 1. Do executive leaders have a defined mode of regular communication
High Risk Operations in Healthcare
 High Risk Operations in Healthcare System Dynamics Modeling and Analytic Strategies MIT Conference on Systems Thinking for Contemporary Challenges October 22-23, 2009 Contributors to This Work Meghan Dierks,
High Risk Operations in Healthcare System Dynamics Modeling and Analytic Strategies MIT Conference on Systems Thinking for Contemporary Challenges October 22-23, 2009 Contributors to This Work Meghan Dierks,
UniCare Professional Reimbursement Policy
 UniCare Professional Reimbursement Policy Subject: Anesthesia Services Policy #: UniCare 0020 Adopted: 02/03/2009 Effective: 02/07/2017 Coverage is subject to the terms, conditions, and limitations of
UniCare Professional Reimbursement Policy Subject: Anesthesia Services Policy #: UniCare 0020 Adopted: 02/03/2009 Effective: 02/07/2017 Coverage is subject to the terms, conditions, and limitations of
Services That Require Prior Authorization
 Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
STATEMENT OF PURPOSE: Emergency Department staff care for observation patients in two main settings: the ED observation unit (EDOU) and ED tower obser
 and ED tower obser") DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
DEPARTMENT OF EMERGENCY MEDICINE POLICY AND PROCEDURE MANUAL EMERGENCY DEPARTMENT OBSERVATION UNITS BRIGHAM AND WOMEN S HOSPITAL 75 FRANCIS STREET BOSTON, MA 02115 Reviewed and Revised: 04/2014 Copyright
Appendix 4 Guidelines, Standards and Other Official Statements Available on the Internet
 Can J Anesth/J Can Anesth (2018) Guidelines to the Practice of Anesthesia* Revised Edition 2018 Appendix 4 Guidelines, Standards and Other Official Statements Available on the Internet The Canadian Anesthesiologists
Can J Anesth/J Can Anesth (2018) Guidelines to the Practice of Anesthesia* Revised Edition 2018 Appendix 4 Guidelines, Standards and Other Official Statements Available on the Internet The Canadian Anesthesiologists
Your Anesthesiologist, Anesthesia and Pain Control
 You should avoid having pain after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in advance.
You should avoid having pain after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in advance.
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
B 2 BOARD OF REGENTS MEETING. Harborview Paramedic Training Program
 BOARD OF REGENTS MEETING B 2 Harborview Paramedic Training Program This will be a fifteen minute oral report for information only. Following the presentation, there will be five minutes allowed for public
BOARD OF REGENTS MEETING B 2 Harborview Paramedic Training Program This will be a fifteen minute oral report for information only. Following the presentation, there will be five minutes allowed for public
Anesthesia Payment & Billing Information
 Anesthesia Payment & Billing Information Time and Points Eligible Anesthesia Procedures Defined Blue Cross and Blue Shield of Texas has determined that certain anesthesia procedures will be reimbursed
Anesthesia Payment & Billing Information Time and Points Eligible Anesthesia Procedures Defined Blue Cross and Blue Shield of Texas has determined that certain anesthesia procedures will be reimbursed
Alabama Trauma Center Designation Criteria
 2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
2 Alabama Trauma Center Designation Criteria Office of Emergency Medical Services Master Checklist Alabama Trauma Center Designation Trauma Center Criteria: APPENDIX A Trauma Rules The following table
Contact Hours (CME version ONLY) Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff
 Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff") 1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
When words and actions matter most: The Case for CANDOR
 January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
January 20, 2017 When words and actions matter most: The Case for CANDOR Timothy B McDonald, MD Director, Center for Open and Honest Communication in Healthcare MedStar Health, Institute for Quality and
Proposed Standards Revisions Related to Pain Assessment and Management
 Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Actionable Patient Safety Solution (APSS) #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION
 #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION") Actionable Patient Safety Solution (APSS) #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION Executive Summary Checklist Opioid induced respiratory depression is a leading cause
Actionable Patient Safety Solution (APSS) #4: FAILURE TO RESCUE: MONITORING FOR OPIOID INDUCED RESPIRATORY DEPRESSION Executive Summary Checklist Opioid induced respiratory depression is a leading cause
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS)
") PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare. Friday October 14, 2016
 Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Anthem Blue Cross and Blue Shield Professional Reimbursement Policy
 Subject: Anesthesia CT Policy: 0020 Effective: 08/01/2014 01/31/2015 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria listed
Subject: Anesthesia CT Policy: 0020 Effective: 08/01/2014 01/31/2015 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria listed
Adult Patient Controlled Analgesia (PCA)
") Contents... 1 Policy... 1 Scope/Audience... 1 Associated Documents... 1 Statement... 2 Criteria... 2 Patient and Whanau Education... 2 Procedural Considerations... 3 Pre Administration... 3 Patient Monitoring...
Contents... 1 Policy... 1 Scope/Audience... 1 Associated Documents... 1 Statement... 2 Criteria... 2 Patient and Whanau Education... 2 Procedural Considerations... 3 Pre Administration... 3 Patient Monitoring...
PATIENT CARE MANUAL PROCEDURE
 PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-10 OFFICE-BASED SURGERY TABLE OF CONTENTS
 Medical Examiners Chapter 540-X-10 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-10 OFFICE-BASED SURGERY TABLE OF CONTENTS 540-X-10-.01 Preamble 540-X-10-.02 Definitions - Levels
Medical Examiners Chapter 540-X-10 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-10 OFFICE-BASED SURGERY TABLE OF CONTENTS 540-X-10-.01 Preamble 540-X-10-.02 Definitions - Levels
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
CA-2 Curriculum for Obstetric Anesthesia Department of Anesthesiology
 CA-2 Curriculum for Obstetric Anesthesia Department of Anesthesiology Description of Rotation or Educational Experience The goal of the CA-2 rotation in obstetric anesthesia is to enhance the knowledge
CA-2 Curriculum for Obstetric Anesthesia Department of Anesthesiology Description of Rotation or Educational Experience The goal of the CA-2 rotation in obstetric anesthesia is to enhance the knowledge
Peri-operative Pain Management - a multi-disciplinary team-based approach
 Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Using Continuous Monitoring for Early Recognition of Patient Deterioration in the Post-op Population It Just Makes Sense.
 Using Continuous Monitoring for Early Recognition of Patient Deterioration in the Post-op Population It Just Makes Sense January 12, 2018 Vision: Health technology enhances healthcare providers abilities
Using Continuous Monitoring for Early Recognition of Patient Deterioration in the Post-op Population It Just Makes Sense January 12, 2018 Vision: Health technology enhances healthcare providers abilities