Ruth Melville - QLD ACORN Director & Chair Standards Committee NUM ORS Clinical Services NGH
|
|
|
- Ilene Beasley
- 6 years ago
- Views:
Transcription

1 Perioperative Documentation? Surgical Safety Checklist? Tray Checklists? Count sheets? What are they and how do they fit with current standards/practice? Ruth Melville - QLD ACORN Director & Chair Standards Committee NUM ORS Clinical Services NGH

2 Achieving better patient outcomes Best practice in QH Basically, safer perioperative patient care ACORN standards

3 State-wide Perioperative Patient Form Surgical Safety Checklist (SSC) Impact of the new Perioperative Documentation on CSSD & ORS Strategies/examples of using tray checklists as part of the count process Alignment with ACORN standards

4 Standardised Documentation Why? Reduce risk of staff errors due to a structured standardised approach Ease of transition of staff moving within perioperative settings Consistent information delivered to patients Reduced risk of retained accountable items Therefore improved PATIENT SAFETY
5
6 Swiss Cheese Model No Standard Procedure for pre-operative checks Pressure to do more cases to shorten waiting list No team briefing prior to operation being commenced Lack of surgeon awareness of risk of incorrect surgery Nurse asked Mr Smith to confirm not state his name FAILURES (holes in cheese) Patient Mr. Sims partly deaf answered yes Organisation Workplace DEFENSES (slices of cheese) Team Individual Patient Mr. Sims had wrong operation HARM Adapted from Reason, 1990
 involvement to undertake Project 2007")
7 The Journey? PNAQ Endorsement Strategic Meeting Undertook State-wide analysis of Perioperative documentation Clinical Practice Improvement Centre (CPIC) involvement to undertake Project Completion of project plan by CPIC Clinical Networks endorsement SWAPNET Project management undertaken by CPIC Trial form completed Trial commenced in 47 QH sites Feedback correlated & forms updated Forms now ready to utilise Plan

8 How was the gap identified? During downtime at our facility, a CN was allocated A Comparison across the state of sample documentation and questionnaires 54 Public sent out, 46 received back 45 Private sent out, 35 received back Identified as a priority strategy from State-wide Perioperative safety Forums

9 What did the gap identify? Vast differences in styles of information recorded Inconsistencies in counting procedure of consumables and instrumentation Inconsistences with use of tray checklists for instrument trays. Varying sizes and throughput of HCF s Therefore the need for a consistent generic state-wide approach not a facility approach

10 What support did the project have? PNAQ NUM support Patient Safety Centre Sandy Blake & John Wakefield CPIC support SWAPNET support
 and recommended practices (ACORN) Care plan to follow for work practices (pre-op checklist) Variance")
11 What were the considerations for this document? Consistent language for collection of data Reflect - regulatory requirements (3C s) and recommended practices (ACORN) Care plan to follow for work practices (pre-op checklist) Variance orientated therefore replace pathways Strategic state-wide approach not a facility approach Able to be used for Adult and paediatric facilities



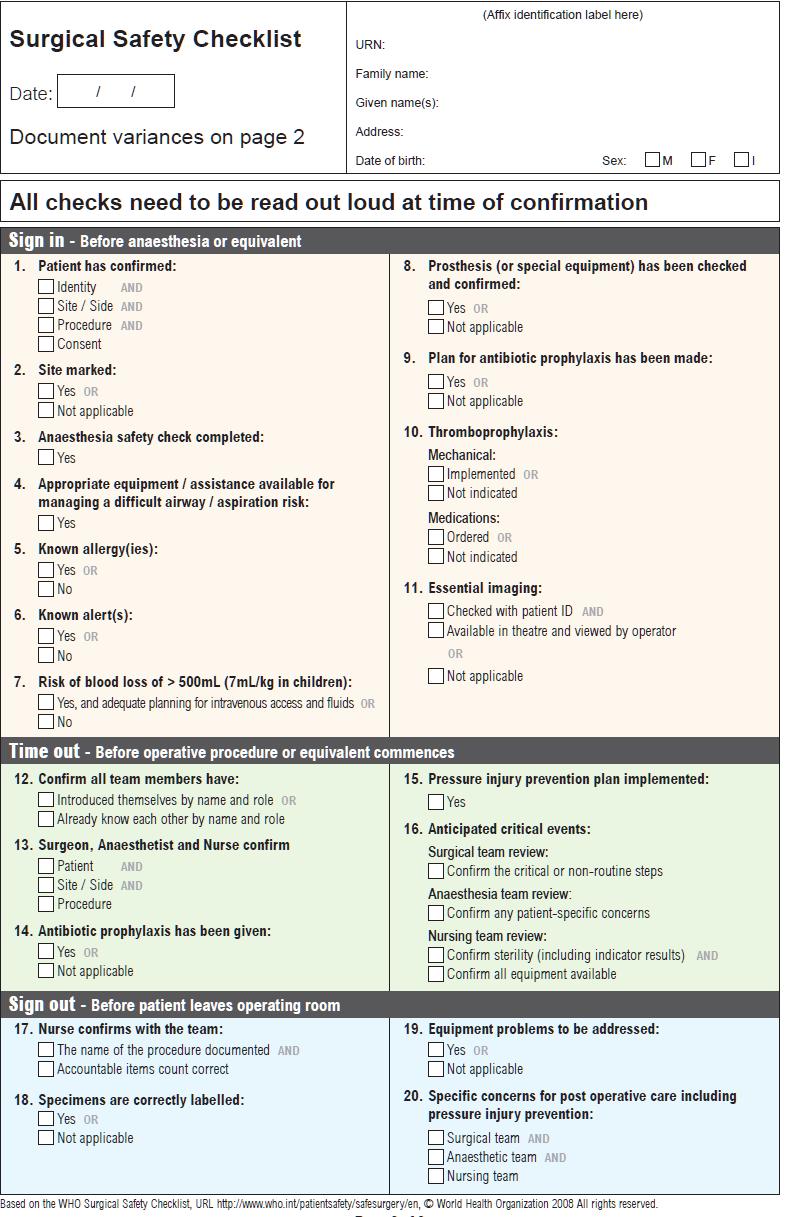
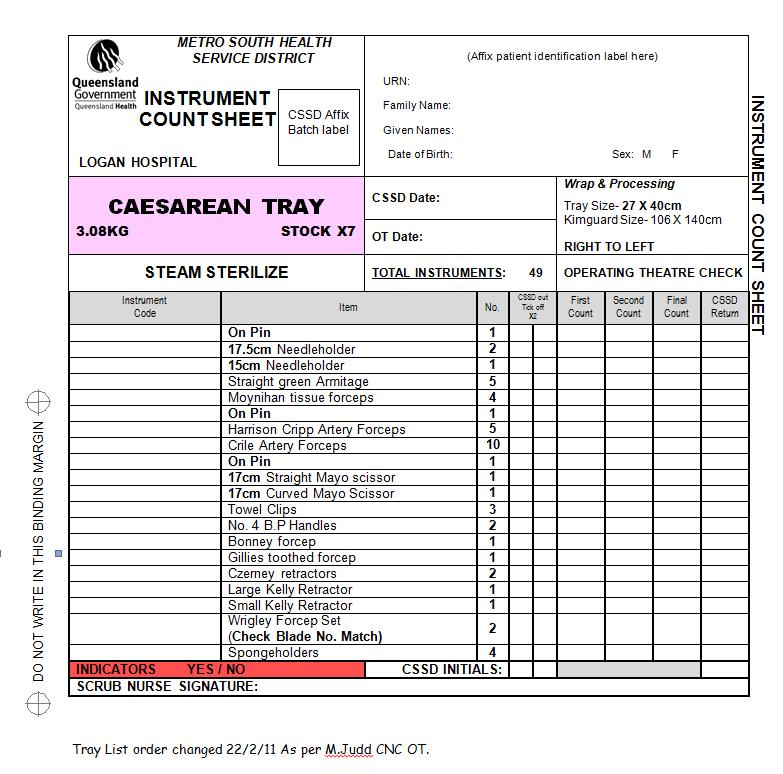
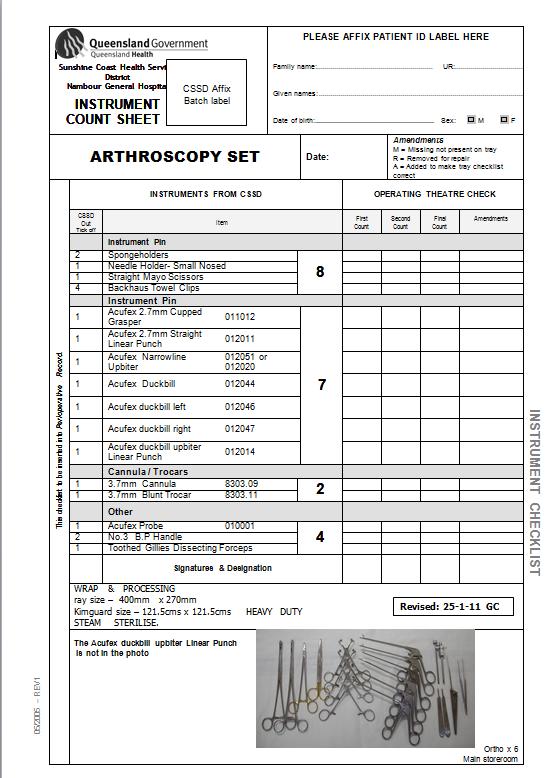
12 What are the components? Perioperative Patient Form A3, 3 page document which includes the Surgical Safety Checklist Count Sheet double sided with intraoperative information included (ORMIS sites) Sterility Validation Tracking and Prosthesis Used form Intraoperative Form (sites without ORMIS)
 by anaesthetic/circulating nurse prior to transfer into Operating Theatre Note: The location of each check may")
13 Preoperative Checks 3 Checks should be undertaken when patient care is passed from one clinician/location to another eg Ward/Unit to Theatre transfer for example:- Prior to Transfer to Operating Suite On arrival to Operating Suite To be undertaken in anaesthetic bay (if available) by anaesthetic/circulating nurse prior to transfer into Operating Theatre Note: The location of each check may vary dependent upon the local facility.


14 Pt states An antibiotic Rash & Hot Pacemaker Left Chest 3/9/ hr Site not yet marked by surgeon,, registrar notified R Melville RN State the allergy and the effect Other implants and prostheses may also include Grommets, peg feeds and portacaths. State the variance and what you have done about it. This information is available to clinicians in the perioperative and post operative environment.
 on the 14 th June")
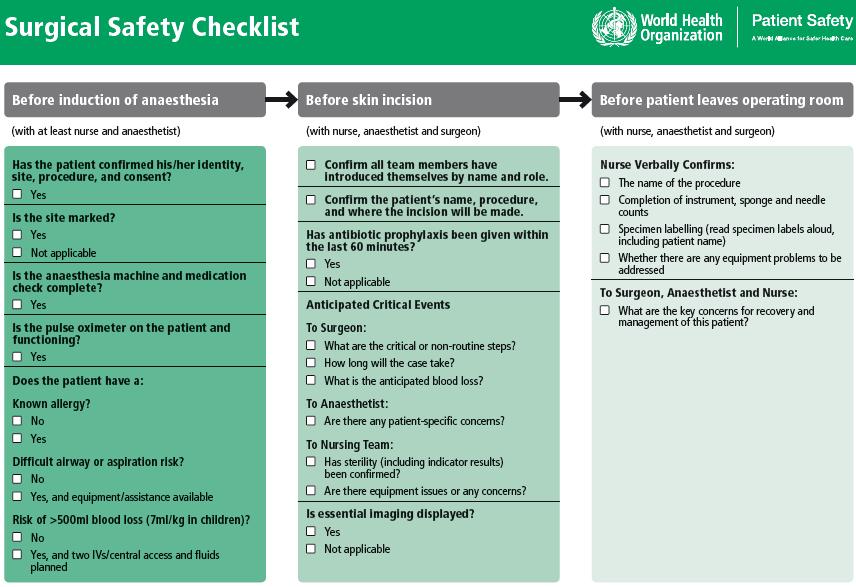
15 Surgical Safety checklist Background Endorsed and launched by both medical and nursing peak bodies (RACS, ACORN, ANZCA, RANZCOG) and Federal Health Minister August 2009 Endorsed by Health Ministers AHMC in November 2009 QH Surgical Safety Checklist Policy, Standard and Manual approved for state-wide implementation by the Patient safety and Quality Executive Committee (PSQEC) on the 14 th June Commitment to implement across Australia by 1 July 2011

16 Why was the checklist developed? (To address the WHO 10 Objectives for Safe Surgery) 1. The team will operate on the correct patient at the correct site. 2. The team will use methods known to prevent harm from the administration of anaesthetics, while protecting the patient from harm. 3. The team will recognise and effectively prepare for life-threatening loss of airway or respiratory function. 4. The team will recognise and effectively prepare for risk of high blood loss. 5. The team will avoid inducing an allergic or adverse drug reaction for which the patient is known to be at significant risk (WHO 2009)

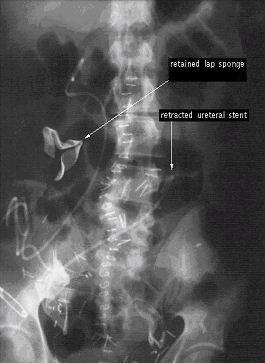
17 Why was the checklist developed? (To address the WHO 10 Objectives for Safe Surgery) 6. The team will consistently use methods known to minimise the risk for surgical site infection. 7. The team will prevent the inadvertent retention of instruments and sponges in surgical wounds. 8. The team will secure and accurately identify all surgical specimens. 9. The team will effectively communicate and exchange critical information for the safe conduct of the operation. 10. Hospitals and public health systems will establish routine surveillance of surgical capacity, volume and results. (WHO 2009)
18

19 Where was the checklist piloted? Toronto, Canada London, UK Amman, Jordan, Jordan Manila, Philippines Seattle, USA Auckland,NZ Ifakara, Tanzania New Delhi, India World Health Organization, 2009
20
21 QH Surgical Safety Checklist The aim of the checklist is to: Reinforce accepted safety practices through better communication and teamwork between individuals (Implementation Manual WHO Surgical Safety Checklist 2009)
22 ACORN(SS2) Standard Statement 2 HCF shall develop a policy, which clearly defines the counting process within their organisation and is used in conjunction with the standard. Rationale ACORN acknowledges that each surgical procedure carries a different risk for instruments, and other items, being retained. Therefore, the risk shall be considered, when determining those instruments, equipment and other items that shall require mandatory documentation. Note: There may be variations within each HCF in relation to the standard and these should be included in the HCF policy. Criteria The multidisciplinary management committee shall develop a policy which: 2.1 clearly defines any additional items to be included in mandatory counts; and, 2.2 ensures the timely annual review of all processes and documentation.
23 ACORN(SS5) Standard Statement 5 The nurse shall utilise a tray list as a risk management and inventory management tool. Rationale The use of tray lists provides a record of instruments received prior to surgery, and those returned for reprocessing. It may also be used by the HCF as a reprocessing quality audit tool. ACORN recommends the tray list be used to check instruments prior to the commencement of the surgical procedure, at the completion of the surgical procedure, and that both these checks are performed by two nurses, one of whom shall be a RN. ACORN recommend a process should be developed by the HCF which accounts for additional separate instruments opened for use during a surgical procedure. Criteria The two (2) nurses shall: 5.1 ensure the contents of each tray are checked; 5.2 utilise the tray list to confirm the presence of all instruments, prior to the commencement of the surgical procedure. This process will establish a baseline record for subsequent checks ensure a list is present on each instrument tray used which has been checked and signed off by the sterilising department technician, or an authorised person, prior to sterilisation prior to the commencement of a procedure if an instrument tray is deemed incorrect, this is noted on the tray list and the HCF APD shall be completed. The tray list shall be retained to aid investigation;
24 ACORN(SS5) Standard Statement utilise the tray list to confirm the presence of all instruments at the completion of the surgical procedure at the completion of the surgical procedure ensure that the identification of the instrument nurse and circulating nurse, the date and the patient s medical record number, in accordance with HCF policy, is recorded on the instrument tray list, and returned with the instrument tray for reprocessing; Note: As a quality check, prior to reprocessing, the instrument tray shall be checked for completeness, by a sterilising department technician, or an authorised person. For audit purposes, the tray list shall be retained, according to HCF policy, until the final processing is correct and complete. 5.4 utilise loan sets in accordance with the patient s surgical requirements when accounting for loan sets refer to ACORN Standard S23 Handling of loan equipment.
25 Use of Tray Checklist as part of count Process Tray checklists need Consistent generic format for counts Process for updating Information for sterile processing Ability for sterility stickers to be adhered to Checklist can be printed on carbonated paper (duplicate) Uses ordinary Laser Printer?jamming problems Paperwork attached with adhesive plastic sleeve to outside of tray after sterilisation. Over 500 tray checklists!! Safety benefits for patients & staff in ORS counting in logical order Not double documentation leading to errors Consistent documentation therefore more educationally comprehensive, easier for beginning practioners
26
27
, 38-40. Gawande, A., Studdert, D., Orav, E., Brennan, T., & Zinner, M. (2003). Risk factors for retained instruments and sponges after surgery.")
28 References Australian College of Operating Room Nurses (ACORN). (2010). Standards, guidelines and policy statements. Adelaide: ACORN. Chiarella, M. (1997). Why are surgeons sued? ACORN Journal, 10 (1), Gawande, A., Studdert, D., Orav, E., Brennan, T., & Zinner, M. (2003). Risk factors for retained instruments and sponges after surgery. New England Journal of Medicine, 348 (3), Gibbs, V. (2003). Retained surgical sponge. Agency for Healthcare Research and Quality, morbidity & mortality rounds on the web. Gibbs, V., & Auerbach, A. (2001). The retained surgical sponge. In K. Shojania, B. Duncan, K. McDonald, & R. Wachter (Eds.), Making healthcare safer: a critical analysis of patient safety practices. Rockville, MD: Agency for Healthcare Research and Quality: , AHRQ publication 01-EO58. Evidence report/technology assessment no. 43 [online]. Hucker, T., Schaeffer, B., Wakeling, H., & Parr, D. (2001). A retained surgical swab Anaesthesia, 56 (11), Queensland Health Patient Safety: From Learning to Action II 2006/7 (2008) Queensland Health Queensland Health Patient Safety: From Learning to Action III 2007/8 (2010) Queensland Health NSW Health (2006). Patient safety and clinical quality program third report on incident management in the public health system, Sydney: Author. Reason, J. (2001). Understanding adverse events: the human factor. In C. Vincent (Ed.), Clinical risk management: enhancing patient safety (pp.9-30). London: BMJ Publishing. Vincent, C., Taylor-Adams, S., & Stanhope, N. (1998). Framework for analysing risk and safety in clinical medicine. British Medical Journal, 316,

29 Summary - Understand the changes with the new Perioperative Patient Form - Recognise the Patient Safety aspects of the utilisation of the Surgical Safety Checklist and use of tray checklist as part of counting procedure - Identify some example's of different uses of tray checklists Thank-you & any questions
2012 WEBINAR SERIES. ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT.
 2012 WEBINAR SERIES ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT February 23, 2012 Welcome ASC Knowledge Share is a new webinar series
2012 WEBINAR SERIES ASC Knowledge Share SAFE SURGERY CHECKLIST: TOOLS TO SUPPORT COMPLIANCE WITH THE NEW CMS REPORTING REQUIREMENT February 23, 2012 Welcome ASC Knowledge Share is a new webinar series
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
The Journey To Ariadne Labs. Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist
 The Journey To Ariadne Labs Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist A Little History Flight Controls FREE & CORRECT The Problem The 3 Central Problems in Surgical Safety
The Journey To Ariadne Labs Bill Berry, MD, MPH Chief Medical Officer Principle Research Scientist A Little History Flight Controls FREE & CORRECT The Problem The 3 Central Problems in Surgical Safety
Implementation of Surgical Safety Checklist
 Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
Implementation of Surgical Safety Checklist The World Health Organisation has identified through consultation with surgeons, anaesthetists and nurses a checklist of critical steps that are common to all
Washington Patient Safety Coalition & Surgical Public Health:
 Washington Patient Safety Coalition & Surgical Public Health: Surgical Quality in Washington State (SCOAP- Surgical Care and Outcomes Assessment Program), Surgical Safety, and the Introduction of the WHO/SCOAP
Washington Patient Safety Coalition & Surgical Public Health: Surgical Quality in Washington State (SCOAP- Surgical Care and Outcomes Assessment Program), Surgical Safety, and the Introduction of the WHO/SCOAP
Expedition: Improving Safety and Reliability for Surgical Procedures
 These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
Checklists after Gawande
 Checklists after Gawande John A Windsor University of Auckland Member, WHO Safer Surgery Study Group CAUSE OF DEATH Lack of clean water and basic healthcare for children DEATHS PER DAY 30,000 Smoking 14,000
Checklists after Gawande John A Windsor University of Auckland Member, WHO Safer Surgery Study Group CAUSE OF DEATH Lack of clean water and basic healthcare for children DEATHS PER DAY 30,000 Smoking 14,000
NSQHS Standard 3: How are we going?
 NSQHS Standard 3: How are we going? Sue Greig RN, MN (Inf Cont) Syd Uni, CICP Adjunct Lecturer, Griffith University Senior Project Officer, National HAI Prevention Program The NSQHS Standards Standard
NSQHS Standard 3: How are we going? Sue Greig RN, MN (Inf Cont) Syd Uni, CICP Adjunct Lecturer, Griffith University Senior Project Officer, National HAI Prevention Program The NSQHS Standards Standard
Safe Surgery The Checklist Experience
 Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
Safe Surgery The Checklist Experience Modificirana prezentacija uz suglasnost Gerald Dziekan, WHO Patient Safety The Surgical burden Estimated 234 million major operations performed worldwide each year
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Teamwork, Communication, Briefing, Checklists, & O.R. Safety
 Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
PATIENT ASSESSMENT POLICY Page 1 of 7
 Page 1 of 7 Policy applies to: All staff and allied health professionals involved in patient care delivery at Mercy Hospital including Manaaki. Related Standards: Health & Disability Services (core) Standards
Page 1 of 7 Policy applies to: All staff and allied health professionals involved in patient care delivery at Mercy Hospital including Manaaki. Related Standards: Health & Disability Services (core) Standards
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Safety and Quality Measures: What, Why and How? APHA Congress 2010
 Safety and Quality Measures: What, Why and How? APHA Congress 2010 Chris Baggoley 19 October 2010 Harvard study 17yrs on Although much good work has been carried out there is a sense at the coalface of
Safety and Quality Measures: What, Why and How? APHA Congress 2010 Chris Baggoley 19 October 2010 Harvard study 17yrs on Although much good work has been carried out there is a sense at the coalface of
The How to Guide for Reducing Surgical Complications
 The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
Advanced Roles and Workforce Planning. Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow
 Advanced Roles and Workforce Planning Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow Confusion of Advanced Roles Clinical Support Worker (CSW) Nurse Practitioner (NP) Physicians Associate
Advanced Roles and Workforce Planning Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow Confusion of Advanced Roles Clinical Support Worker (CSW) Nurse Practitioner (NP) Physicians Associate
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
Legal and Legislative Services Branch 28 January 2016 NSW Ministry of Health Locked Bag 961 NORTH SYDNEY 2059
 Legal and Legislative Services Branch 28 January 2016 NSW Ministry of Health Locked Bag 961 NORTH SYDNEY 2059 Email: legalmail@doh.health.nsw.gov.au RE: Discussion Paper - Cosmetic Surgery and The Private
Legal and Legislative Services Branch 28 January 2016 NSW Ministry of Health Locked Bag 961 NORTH SYDNEY 2059 Email: legalmail@doh.health.nsw.gov.au RE: Discussion Paper - Cosmetic Surgery and The Private
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital.
 An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
Patient safety alert 06
 Immediate action Action Update Information request Correct site surgery Surgery performed at the incorrect anatomical site is rare. However, it can be devastating for patients. Correct site surgery (CSS)
Immediate action Action Update Information request Correct site surgery Surgery performed at the incorrect anatomical site is rare. However, it can be devastating for patients. Correct site surgery (CSS)
SFHPCS14 - SQA Code HC7X 04 Prepare surgical instrumentation and supplementary items for the surgical team
 Prepare surgical instrumentation and supplementary items for the Overview This standard covers the preparation of surgical instrumentation and supplementary items for the. This includes the preparation
Prepare surgical instrumentation and supplementary items for the Overview This standard covers the preparation of surgical instrumentation and supplementary items for the. This includes the preparation
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM
 CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
CHALLENGES TO IMPROVE PATIENT SAFETY IN THE OPERATING ROOM Rouba Rassi El-Khoury, Pharm.D, M.Sc, MBA HM Quality Director, Hôtel-Dieu de France University Medical center President of the LSQSH The 9th Congress
POLICY. The purpose of this policy is to establish Saskatoon Health Region s (SHR s) communication requirements for all surgical patients.
 communication requirements for all surgical patients.") POLICY Number: 7311-60-026 Title: Surgical Safety Checklist Authorization [ ] President and CEO [ X] Vice President, Finance and Corporate Services Source: Chair(s), Surgical Operations Committee Cross
POLICY Number: 7311-60-026 Title: Surgical Safety Checklist Authorization [ ] President and CEO [ X] Vice President, Finance and Corporate Services Source: Chair(s), Surgical Operations Committee Cross
Safe Care and Support
 SPECIALIST PALLIATIVE CARE May 2014 Safe Care and Support Supporting services to deliver quality healthcare 1 Introduction Welcome to the Quality Assessment and Improvement Workbook. This workbook will
SPECIALIST PALLIATIVE CARE May 2014 Safe Care and Support Supporting services to deliver quality healthcare 1 Introduction Welcome to the Quality Assessment and Improvement Workbook. This workbook will
Aneurin Bevan Health Board. Improving Theatre Performance
 Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
Anaesthesia Fellow. Position Description. Department : Department of Anaesthesia & Perioperative Medicine
 Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Benefits Measurement from the Use of an Automated Anaesthetic Record Keeping System (AARK)
") electronic Journal of Health Informatics http://www.ejhi.net 2011; Vol 6(1): e6 Benefits Measurement from the Use of an Automated Anaesthetic Record Keeping System (AARK) Sue McLellan 1, Mary Galvin 2,
electronic Journal of Health Informatics http://www.ejhi.net 2011; Vol 6(1): e6 Benefits Measurement from the Use of an Automated Anaesthetic Record Keeping System (AARK) Sue McLellan 1, Mary Galvin 2,
Australian and New Zealand College of Anaesthetists (ANZCA)
") PS08 2016 Australian and New Zealand College of Anaesthetists (ANZCA) Statement on the Assistant for the Anaesthetist 1. PURPOSE The purpose of this document is to recognise the importance of and to promote
PS08 2016 Australian and New Zealand College of Anaesthetists (ANZCA) Statement on the Assistant for the Anaesthetist 1. PURPOSE The purpose of this document is to recognise the importance of and to promote
Sheffield Teaching Hospitals NHS Foundation Trust
 Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Enhancing Patient Safety through Team Work and Communication Strategies
 Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Enhancing Patient Safety through Team Work and Communication Strategies St. Joseph Medical Center- Towson Maryland Program/Project Description. In July 2009, Catholic Health Initiatives, of which St Joseph
Offsite theatre sterile surgical units a clinical risk?
 Offsite theatre sterile surgical units a clinical risk? R. Madhu, R. Kotnis, C.S. Galasko, K. Willett. Rachala Madhu MRCS Rohit Kotnis MRCS Professor Charles Galasko FRCS Professor Keith Willett FRCS Research
Offsite theatre sterile surgical units a clinical risk? R. Madhu, R. Kotnis, C.S. Galasko, K. Willett. Rachala Madhu MRCS Rohit Kotnis MRCS Professor Charles Galasko FRCS Professor Keith Willett FRCS Research
Standard 1: Governance for Safety and Quality in Health Service Organisations
 Standard 1: Governance for Safety and Quality in Health Service Organisations riterion: Governance and quality improvement system There are integrated systems of governance to actively manage patient safety
Standard 1: Governance for Safety and Quality in Health Service Organisations riterion: Governance and quality improvement system There are integrated systems of governance to actively manage patient safety
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Teamwork, Communication, O.R. Safety & SSI Reduction
 2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
2011 Infection Prevention Leadership Teamwork, Communication, O.R. Safety & SSI Reduction Teamwork, Communication, O.R. Safety & SSI Reduction 2 Presented by: E. Patchen Dellinger, MD, FACS Professor of
Wrong site interventions
 Publication Ref: I2017/004/1 Wrong site interventions 27 November 2017 This interim bulletin contains facts which have been determined up to the time of issue. It is published to inform the NHS and the
Publication Ref: I2017/004/1 Wrong site interventions 27 November 2017 This interim bulletin contains facts which have been determined up to the time of issue. It is published to inform the NHS and the
NES Patient Safety Programme. Human Factors in Healthcare. NES Educational Developments and Resources
 NES Patient Safety Programme Human Factors in Healthcare NES Educational Developments and Resources Introduction The three Quality Ambitions articulated in the Healthcare Quality Strategy include a focus
NES Patient Safety Programme Human Factors in Healthcare NES Educational Developments and Resources Introduction The three Quality Ambitions articulated in the Healthcare Quality Strategy include a focus
Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65
 Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
The Regulation and Quality Improvement Authority
 The Regulation and Quality Improvement Authority Review of Theatre Practice in Health and Social Care Trusts in Northern Ireland Overview report June 2014 Assurance, Challenge and Improvement in Health
The Regulation and Quality Improvement Authority Review of Theatre Practice in Health and Social Care Trusts in Northern Ireland Overview report June 2014 Assurance, Challenge and Improvement in Health
Labor recognises RACS and its executive for their important and continued advocacy on behalf of our State s surgical professionals.
 David Walters Chair of SA Regional Committee Royal Australasian College of Surgeons PO Box 44 NORTH ADELAIDE SA 5006 Dear Mr Walters Thank you for your letter dated 23 January, in which the Royal Australasian
David Walters Chair of SA Regional Committee Royal Australasian College of Surgeons PO Box 44 NORTH ADELAIDE SA 5006 Dear Mr Walters Thank you for your letter dated 23 January, in which the Royal Australasian
PLANNED CARE THEATRE OPERATIONAL POLICY
 PLANNED CARE THEATRE OPERATIONAL POLICY Review date: April 2021 Mr U Khan : Clinical Director Mr M Brown :Associate Director Planned Care Mr M Cawley : Theatre Manager Theatre Operational Policy V4.1 Policy
PLANNED CARE THEATRE OPERATIONAL POLICY Review date: April 2021 Mr U Khan : Clinical Director Mr M Brown :Associate Director Planned Care Mr M Cawley : Theatre Manager Theatre Operational Policy V4.1 Policy
Patient Safety in the Philippines
 Patient Safety in the Philippines Armando C. Crisostomo, MD, MHPEd Professor of Surgery & Associate Dean College of Medicine, UP Manila Chair, Phil. Alliance for Patient Safety Technical Consultant, DOH
Patient Safety in the Philippines Armando C. Crisostomo, MD, MHPEd Professor of Surgery & Associate Dean College of Medicine, UP Manila Chair, Phil. Alliance for Patient Safety Technical Consultant, DOH
QUESTIONS PERTINENT TO PRODUCT SELECTION:
 QUESTIONS PERTINENT TO PRODUCT SELECTION: Impact on patient outcomes Impact on patient/staff safety Economic considerations Use the following pages to help facilitate discussion with vendors, write your
QUESTIONS PERTINENT TO PRODUCT SELECTION: Impact on patient outcomes Impact on patient/staff safety Economic considerations Use the following pages to help facilitate discussion with vendors, write your
O1 Readiness. O2 Implementation. O3 Success A FRAMEWORK TO EVALUATE MUSCULOSKELETAL MODELS OF CARE
 FOR MUSCULOSKELETAL HEALTH O1 Readiness O2 Implementation O3 Success A FRAMEWORK TO EVALUATE MUSCULOSKELETAL MODELS OF CARE GLOBAL ALLIANCE SUPPORTING ORGANISATIONS The following organisations publicly
FOR MUSCULOSKELETAL HEALTH O1 Readiness O2 Implementation O3 Success A FRAMEWORK TO EVALUATE MUSCULOSKELETAL MODELS OF CARE GLOBAL ALLIANCE SUPPORTING ORGANISATIONS The following organisations publicly
Prepare surgical instrumentation and supplementary items for the surgical team
 About this Unit This standard covers the preparation of surgical instrumentation and supplementary. This includes the preparation of the sterile trolley, surgical instruments and supplementary equipment.
About this Unit This standard covers the preparation of surgical instrumentation and supplementary. This includes the preparation of the sterile trolley, surgical instruments and supplementary equipment.
Improving the safety of remote site emergency airway management
 BMJ Quality Improvement Reports 2014; u202785.w1275 doi: 10.1136/bmjquality.u202785.w1275 Improving the safety of remote site emergency airway management Julian Wijesuriya, Jonathan Brand Darlington Memorial
BMJ Quality Improvement Reports 2014; u202785.w1275 doi: 10.1136/bmjquality.u202785.w1275 Improving the safety of remote site emergency airway management Julian Wijesuriya, Jonathan Brand Darlington Memorial
Executive & Board; Perioperative Education Committee
 OPERATING ROOM NURSES ASSOCIATION OF CANADA RULES & REGULATIONS MANUAL Title Number 405 Source Date Revised January 2011 Date Effective 1998 Perioperative Education Programs Program Review and Approval
OPERATING ROOM NURSES ASSOCIATION OF CANADA RULES & REGULATIONS MANUAL Title Number 405 Source Date Revised January 2011 Date Effective 1998 Perioperative Education Programs Program Review and Approval
POINT OF CARE TESTING POLICY Page 1 of 6 Reviewed: October 2017
 Page 1 of 6 Policy Applies to: All clinical staff involved in using Point of Care Testing (POCT) equipment. Related Standards: Health & Disability Standard 4.2.3 Amenities, fixtures, equipment and furniture
Page 1 of 6 Policy Applies to: All clinical staff involved in using Point of Care Testing (POCT) equipment. Related Standards: Health & Disability Standard 4.2.3 Amenities, fixtures, equipment and furniture
Z: Perioperative Nursing Specialty
 Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
Z: Perioperative Nursing Specialty Alberta Licensed Practical Nurses Competency Profile 263 Major Competency Area: Z Perioperative Nursing Specialty Priority: One Competency: Z-1 HPA Authorizations and
ASA Standards of Practice for Injection of Local Anesthetics
 ASA Standards of Practice for Injection of Local Anesthetics Adopted by BOD March 2014 Introduction The following Standards of Practice were researched and authored by the ASA Education and Professional
ASA Standards of Practice for Injection of Local Anesthetics Adopted by BOD March 2014 Introduction The following Standards of Practice were researched and authored by the ASA Education and Professional
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Medication Management Policy and Procedures
 POLICY STATEMENT This policy establishes guidelines for ensuring safe and correct management of client medications in accordance with legislative and regulatory requirements and professional practice competency
POLICY STATEMENT This policy establishes guidelines for ensuring safe and correct management of client medications in accordance with legislative and regulatory requirements and professional practice competency
Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery
 Plastic Surgery International Volume 2011, Article ID 579579, 5 pages doi:10.1155/2011/579579 Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery Shady Abdel-Rehim,
Plastic Surgery International Volume 2011, Article ID 579579, 5 pages doi:10.1155/2011/579579 Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery Shady Abdel-Rehim,
RACMA GUIDE TO PRACTICAL CREDENTIALING AND SCOPE OF CLINICAL PRACTICE PROCESSES
 DINO DEFAZIO 1 Contents 1. Introduction... 2 2. Definitions... 3 3. Roles of RACMA members... 3 4. Guiding Principles... 4 3.1 General... 4 3.2 Principles underpinning credentialing processes... 4 3.3
DINO DEFAZIO 1 Contents 1. Introduction... 2 2. Definitions... 3 3. Roles of RACMA members... 3 4. Guiding Principles... 4 3.1 General... 4 3.2 Principles underpinning credentialing processes... 4 3.3
Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy The MERU, HSE (2013)
 and in Radiotherapy The MERU, HSE (2013)") Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy 2010-2012 The MERU, HSE (2013) CONTENT Executive summary.. 2 Introduction 3 Incidents reported in
Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy 2010-2012 The MERU, HSE (2013) CONTENT Executive summary.. 2 Introduction 3 Incidents reported in
Clinical Governance Framework
 Clinical Governance Framework Introduction Whanganui District Health Board (WDHB) is committed to continuously improving the safety and quality of services provided to patients and their families. This
Clinical Governance Framework Introduction Whanganui District Health Board (WDHB) is committed to continuously improving the safety and quality of services provided to patients and their families. This
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition
 Nursing Competency Workbook 6th Edition") Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
Chapter 3M Specialty Nursing Competencies Perioperative (Recovery) Nursing Competency Workbook 6th Edition The Royal Children's Hospital (RCH) Nursing Competency Workbook is a dynamic document that will
Policy for Patient Identification. Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead:
 CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
CONTROLLED DOCUMENT Policy for Patient Identification CATEGORY: CLASSIFICATION: PURPOSE Controlled Document Number: Version Number: 3 Controlled Document Sponsor: Controlled Document Lead: Approved By:
Introduction National reviews Sterilising Technology Certificate III & Certificate IV 2012 Commonwealth of Australia Vocational Education Training ref
 The National Health Training Package The Australian Way Elinor V. Radke QEII Hospital, Brisbane, Australia, Nurse Unit Manager, CSSD. Introduction National reviews Sterilising Technology Certificate III
The National Health Training Package The Australian Way Elinor V. Radke QEII Hospital, Brisbane, Australia, Nurse Unit Manager, CSSD. Introduction National reviews Sterilising Technology Certificate III
SOUTH CENTRAL NEONATAL NETWORK
 SOUTH CENTRAL NEONATAL NETWORK Audit of the current provision of education and training within the Neonatal South Central Network 1.0 Background The driving principles for the reform of the NHS education
SOUTH CENTRAL NEONATAL NETWORK Audit of the current provision of education and training within the Neonatal South Central Network 1.0 Background The driving principles for the reform of the NHS education
Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36
 Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
The non-medical surgical assistant in Australia: who should contribute to governance?
 The non-medical surgical assistant in Australia: who should contribute to governance? AUTHORS Toni Hains RN, MClinSc (PNSA), MNPractSt, PhD Scholar The University of Queensland, School of Nursing, Midwifery
The non-medical surgical assistant in Australia: who should contribute to governance? AUTHORS Toni Hains RN, MClinSc (PNSA), MNPractSt, PhD Scholar The University of Queensland, School of Nursing, Midwifery
APPENDIX ONE. ICAT: Integrated Clinical Assessment Tool
 APPENDIX ONE ICAT: Integrated Clinical Assessment Tool Contents Background...25 ICAT learning objectives...25 Participant information...258 Explanation of scoring of the ICAT...25 Participant responsibilities...25
APPENDIX ONE ICAT: Integrated Clinical Assessment Tool Contents Background...25 ICAT learning objectives...25 Participant information...258 Explanation of scoring of the ICAT...25 Participant responsibilities...25
RESEARCH PROTOCOL M MED (ANAESTHESIOLOGY) DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS)
 DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS)") RESEARCH PROTOCOL M MED (ANAESTHESIOLOGY) DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS) TITLE: AN AUDIT OF PREOPERATIVE EVALUATION OF GENERAL SURGERY PATIENTS AT DR GEORGE MUKHARI
RESEARCH PROTOCOL M MED (ANAESTHESIOLOGY) DEPARTMENT OF ANAESTHESIOLOGY, UNIVERSITY OF LIMPOPO (MEDUNSA CAMPUS) TITLE: AN AUDIT OF PREOPERATIVE EVALUATION OF GENERAL SURGERY PATIENTS AT DR GEORGE MUKHARI
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
NON-MEDICAL PRESCRIBING POLICY
 NON-MEDICAL PRESCRIBING POLICY To be read in conjunction with the Medicines Policy, Controlled Drug Policy and the FP10 Prescribing Forms Policy Version: 5 Date of issue: August 2017 Review date: August
NON-MEDICAL PRESCRIBING POLICY To be read in conjunction with the Medicines Policy, Controlled Drug Policy and the FP10 Prescribing Forms Policy Version: 5 Date of issue: August 2017 Review date: August
TRUST BOARD SEPTEMBER Surgical Services Reconfiguration
 def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
Introduction to Gynaecology & Obstetrics Theatres St Marys Hospital
 Introduction to Gynaecology & Obstetrics Theatres St Marys Hospital Name: Start Date:. Mentor:. Introduction My name is Helen McCallum; I am the Clinical Skills Facilitator for St Marys Theatres. I would
Introduction to Gynaecology & Obstetrics Theatres St Marys Hospital Name: Start Date:. Mentor:. Introduction My name is Helen McCallum; I am the Clinical Skills Facilitator for St Marys Theatres. I would
Bariatric Surgery Registry Outlier Policy
 Bariatric Surgery Registry Outlier Policy 1 Revision History Version Date Author Reason for version change 1.0 10/07/2014 Wendy Brown First release 1.1 01/09/2014 Wendy Brown Review after steering committee
Bariatric Surgery Registry Outlier Policy 1 Revision History Version Date Author Reason for version change 1.0 10/07/2014 Wendy Brown First release 1.1 01/09/2014 Wendy Brown Review after steering committee
What does safe surgery look like? Jonathan Beard Professor of Surgical Education
 What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital
 Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Welcome to Townsville We hope you are enjoying the sunshine and for what will be for some of you very warm weather for this time of year.
 Welcome to Townsville We hope you are enjoying the sunshine and for what will be for some of you very warm weather for this time of year. This is the first SRACA Queensland Conference to be held in Townsville
Welcome to Townsville We hope you are enjoying the sunshine and for what will be for some of you very warm weather for this time of year. This is the first SRACA Queensland Conference to be held in Townsville
Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives
 NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect
NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Agored Cymru Level 3 Diploma in Perioperative Support (QCF) - (600/1799/5) Qualification Guide
 - (600/1799/5) Qualification Guide") 1 Agored Cymru Level 3 Diploma in Perioperative Support (QCF) - (600/1799/5) Operational start date: 01-May-2011 Review date: 31-Dec-2016 Offices South North 3 Purbeck House 3-4 Ash Court Cardiff Business
1 Agored Cymru Level 3 Diploma in Perioperative Support (QCF) - (600/1799/5) Operational start date: 01-May-2011 Review date: 31-Dec-2016 Offices South North 3 Purbeck House 3-4 Ash Court Cardiff Business
Surgery Road Map. General practices. Road map sections
 Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Clinical governance for Primary Health Networks
 no: 22 date: 21/04/2017 title Clinical governance for Primary Health Networks authors Amanda Jones Manager, Deeble Institute for Health Policy Research Australian Healthcare and Hospitals Association Email:
no: 22 date: 21/04/2017 title Clinical governance for Primary Health Networks authors Amanda Jones Manager, Deeble Institute for Health Policy Research Australian Healthcare and Hospitals Association Email:
What we have learned:
 What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.
What we have learned: Perception Nursing Process Observations Nurses place undue reliance and trust in the count. Each individual nurse is sure that his/her count is correct yet there are retained sponges.
JOB DESCRIPTION. Psychiatrist REPORTING TO: CLINICAL DIRECTOR - FOR ALL CLINICAL MATTERS SERVICE MANAGER FOR ALL ADMIN MATTERS DATE: APRIL 2017
 JOB DESCRIPTION Psychiatrist SECTION ONE DESIGNATION: CONSULTANT PSYCHIATRIST MEDICAL OFFICER PSYCHIATRY NATURE OF APPOINTMENT: FULL TIME/10/10THS FTE LOCATION: WEEKLY TIMETABLE: INDICATIVE ONLY REPORTING
JOB DESCRIPTION Psychiatrist SECTION ONE DESIGNATION: CONSULTANT PSYCHIATRIST MEDICAL OFFICER PSYCHIATRY NATURE OF APPOINTMENT: FULL TIME/10/10THS FTE LOCATION: WEEKLY TIMETABLE: INDICATIVE ONLY REPORTING
Neurosurgery. Themes. Referral
 06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
Chapter 13. Documenting Clinical Activities
 Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
ORs in facilities that adopted team training had a lower rate of deaths for
 Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Accreditation Program: Office-Based Surgery
 ccreditation Program: Office-Based Surgery National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Office-Based Surgery National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
New Waves of Evidence Changing the Tides of ACORN Standards: A Case Exemplar
 New Waves of Evidence Changing the Tides of ACORN Standards: A Case Exemplar Dr Sonya Osborne ACORN Standards Editor Natural History of Asepsis 1847 1850 Ignaz SemMelweiss HANDWASHING 1800 1830 1850 1900
New Waves of Evidence Changing the Tides of ACORN Standards: A Case Exemplar Dr Sonya Osborne ACORN Standards Editor Natural History of Asepsis 1847 1850 Ignaz SemMelweiss HANDWASHING 1800 1830 1850 1900
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
OR staffing supports the provision of safe perioperative patient care and promotes a safe perioperative environment
 ACCREDITATION STANDA RDS INTRAOPERATIVE CARE OR staffing supports the provision of safe perioperative patient care and promotes a safe perioperative environment A minimum of two perioperative nurses are
ACCREDITATION STANDA RDS INTRAOPERATIVE CARE OR staffing supports the provision of safe perioperative patient care and promotes a safe perioperative environment A minimum of two perioperative nurses are
Delivering surgical services: options for maximising resources
 Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Job Description. Clinical Nurse Coordinator Perioperative Department Acute Theatres
 Job Description Clinical Nurse Coordinator Perioperative Department Acute Theatres Report To: Liaise with: Clinical Nurse Manager Perioperative Department Perioperative Associate Clinical Nurse Managers
Job Description Clinical Nurse Coordinator Perioperative Department Acute Theatres Report To: Liaise with: Clinical Nurse Manager Perioperative Department Perioperative Associate Clinical Nurse Managers
The Care Values Framework
 The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
PROFESSIONAL STANDARDS OF PRACTICE
 PROFESSIONAL STANDARDS OF PRACTICE Index Page Introduction.. 3 Definition.. 4 Standard One... 5 Standard Two.. 6 Standard Three... 7 Standard Four... 8-9 Appendix A: Standards on Infection Control.. 10-13
PROFESSIONAL STANDARDS OF PRACTICE Index Page Introduction.. 3 Definition.. 4 Standard One... 5 Standard Two.. 6 Standard Three... 7 Standard Four... 8-9 Appendix A: Standards on Infection Control.. 10-13
If you can t measure it, you can t manage it!
 LINICAL NDICATOR ROGRAM If you can t measure it, you can t manage it! THE AUSTRALIAN COUNCIL ON HEALTHCARE STANDARDS LINICAL NDICATOR ROGRAM The ACHS Clinical Indicator Program (CIP) was established in
LINICAL NDICATOR ROGRAM If you can t measure it, you can t manage it! THE AUSTRALIAN COUNCIL ON HEALTHCARE STANDARDS LINICAL NDICATOR ROGRAM The ACHS Clinical Indicator Program (CIP) was established in
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY
 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
Surgical Paediatric Ambulatory Care Pathway Division of Surgery and Perioperative Medicine in partnership with Women's and Children's Division
 Southern Adelaide Local Health Network Surgical Paediatric Ambulatory Care Pathway Division of Surgery and Perioperative Medicine in partnership with Women's and Children's Division Lydia Belet SALHN Perioperative
Southern Adelaide Local Health Network Surgical Paediatric Ambulatory Care Pathway Division of Surgery and Perioperative Medicine in partnership with Women's and Children's Division Lydia Belet SALHN Perioperative
Consensus Reports and Recommendations to Prevent Retained Surgical Items
 Consensus Reports and Recommendations to Prevent Retained Surgical Items Summary by the Institute for Population Health Improvement, UC Davis Health System Category Items included in surgical count When
Consensus Reports and Recommendations to Prevent Retained Surgical Items Summary by the Institute for Population Health Improvement, UC Davis Health System Category Items included in surgical count When
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation