National Health Regulatory Authority Kingdom of Bahrain
|
|
|
- Joanna Harmon
- 6 years ago
- Views:
Transcription



1 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD BE REPORTED AND THE REPORTING AND MONITORING PROCESSES INVOLVED. VERSION EFFECTIVE: 14 September 2013 THIS GUIDANCE WAS LAST UPDATED IN 14 September 2013 PLEASE ENSURE YOU READ THE MOST UP-TO-DATE GUIDE AVAILABLE ON OUR WEBSITE
2 1 INTRODUCTION 2 PURPOSE The NHRA guidance for Serious Adverse Events Management and Reporting sets out the definitions, requirements and approach to be applied to improve patient safety and quality of care by: Advocating the requirement to develop and implement a management and reporting system in all healthcare facilities for all nonstandard incidents and adverse events; and Identifying the criteria for and means by which to collect, notify and report on serious adverse/ sentinel events defined in the guideline. 3 Scope 3.1 The process is identified for all NHRA licensed healthcare facilities. 3.2 All healthcare facilities are encouraged to follow the guideline and implement processes for the management and reporting of serious adverse / sentinel events to the NHRA. 3.3 All healthcare facilities are encouraged to record and monitor all adverse events, near misses and incidents internally, including those related to all aspects of direct patient care, occupational health and safety, equipment and medications. 4 Definitions 4.1 Safety: Freedom from accidental injuries. 4.2 Error: The failure of a planned action to be completed as intended (i.e. error of execution) or the use of a wrong plan to achieve an aim (i.e. error of planning) Errors may be errors of commission or omission, and usually reflect deficiencies in the systems and processes of care. 4.3 Hazard: Any threat to safety, e.g. unsafe practices, conduct, equipment, labels, names. 4.4 System: A set of interdependent elements (people, processes, equipment) that interact to achieve a common aim. 4.5 Adverse Event an event that causes harm, or has potential to cause harm to a patient. 4.6 Serious Adverse/ Sentinel Event Any unanticipated adverse event or Near Miss event in a healthcare setting resulting in death or serious physical or psychological injury to a patient or patients, not arising from the natural course of the patient's illness, includes events that: Are life threatening Requires in-patient hospitalization or prolongs an existing hospitalization Results in persistent or significant disability or incapacity Is any medically significant event that may put the patient at risk or may require medical or surgical intervention to prevent one of the outcomes listed above 4.7 Near Miss: circumstances or events that had the capacity to cause an adverse event, but which did not reach the patient.
3 4.8 Adverse Event Severity Mild: discomfort noticed but no disruption of normal activity Moderate: discomfort sufficient to reduce or affect normal daily activity Severe: interferes significantly with the subject s normal activity or course of illness. All Serious Adverse Events should be classified as severe. 4.9 Pattern of Events Single event: The event occurred just once, and has ended by the time of reporting Continuous: The event began just once, and is still ongoing at the time of reporting Intermittent: The event has gone through at least one cycle of starting, stopping, and starting again Root cause analysis A process for identifying the basic or causal factors that underlie variation in performance and that may have caused or contributed to an adverse event. It focuses primarily on systems and processes, not on individual performance. It progresses from special causes in clinical processes to common causes in organizational processes and systems and identified potential improvements that would decrease the likelihood of recurrence. 5 Requirements of the Healthcare Facilities 5.1 To develop an adverse events management system in accordance with the NHRA guidance based on the following principles: quality and safety continuous improvement, Transparency Accountability 5.2 A system and process should be identified within the healthcare facility and should: Set out in writing the details of the system in a policy and supporting standard operating procedures and documentation; Establish a governance mechanism to oversee, manage, monitor and report on the effectiveness of this system and any corrective actions; Use the definitions identified by the NHRA in the guidance for the purposes of categorization of all events and actions including corrective actions; and Include delineated roles, responsibilities and accountabilities for staff, and as well as provide appropriate training and orientation plans and materials for all staff.
4 5.2.5 Each licensed healthcare facility should be able to demonstrate that an adverse events management system is implemented and managed in the facility in accordance with NHRA guidance. To do so, a facility should make available to the NHRA, if and when directed to: The adverse events management policy and supporting documents that set out in detail the process and operating procedures and the governance system in place; Documentary evidence of identified and reported adverse events, their causes or suspected causes, trends, actions and improvements planned or implemented to prevent recurrence, as well as training activities undertaken or planned within specified timelines To comply with NHRA directions: The NHRA reserves the right within its role as regulator to investigate any and/or all events and apply sanctions in accordance with its remit under the regulatory legislation that is in force in Bahrain All healthcare facilities and employees should: Comply with all applicable NHRA policies and licensing standards; and Comply with NHRA inspection requirements, and cooperate with the NHRA licensure inspectors Assist the NHRA with its requests for information and/or documentation, and submit requested information within the identified timeframes. 6 Requirements of the NHRA 6.1 The NHRA will set out the definitions and types of serious adverse events/sentinel events to be reported externally and the requirements for reporting. 6.2 Reviews and from time to time revises the list of events that should be reported and investigated in accordance with evidence and reported information to ensure the safety and quality of care for patients is continuously assured and improved. 6.3 The NHRA should share learning from serious adverse events reported, patient safety and quality issues, whilst maintaining confidentiality at all times.
5 6.4 The NHRA should investigate and may commission its own investigations, by independent third party, of certain cases if necessary. 6.5 The NHRA can receive information on serious adverse events via the complaints system and, where necessary, will investigate any complaint in accordance with the NHRA Policies and Standard for Complaints management.(this can be found on the NHRA website) 6.6 Where it finds evidence of noncompliance with the legislation, standards and regulations, NHRA may impose sanctions consistent with its remit and the NHRA Policy on Noncompliance and Sanctions. 6.7 The NHRA will analyze investigations, RCAs and any reports submitted by health care facilities and may direct them to: Provide additional information; Undertake further investigations into cases; Develop/revise action plans to address issues identified. 6.8 Facilities should also be prepared for unannounced visits from the NHRA Licensure inspectors, which can be triggered not only by the serious adverse event reports but also by reports in the media, calls from the patient or family, or calls from concerned health care staff from the affected organization. 7 The Reporting Process Research has shown that focused reporting systems are more valuable for deepening the understanding of particular issues of care. These guidelines focus on reporting systems related to serious adverse events only. The process for reporting to the NHRA is outlined in the flowchart below. Template forms and defined data elements are contained in the appendices to this guide. 7.1 For serious adverse / sentinel events defined in this guide, see appendix 3, Healthcare facilities are requested to: Report occurrence of an identified serious adverse event to the NHRA within 48 hours; Submit an initial SAE report (see appendix 1)of the event within seven days of its occurrence to NHRA with details of the investigation and actions taken including minimizing risk of recurrence; and Submit a full RCA report (see appendix 2) to NHRA with details of the investigation, root cause analysis and action plan to minimize risk of recurrence (within 45 working days).
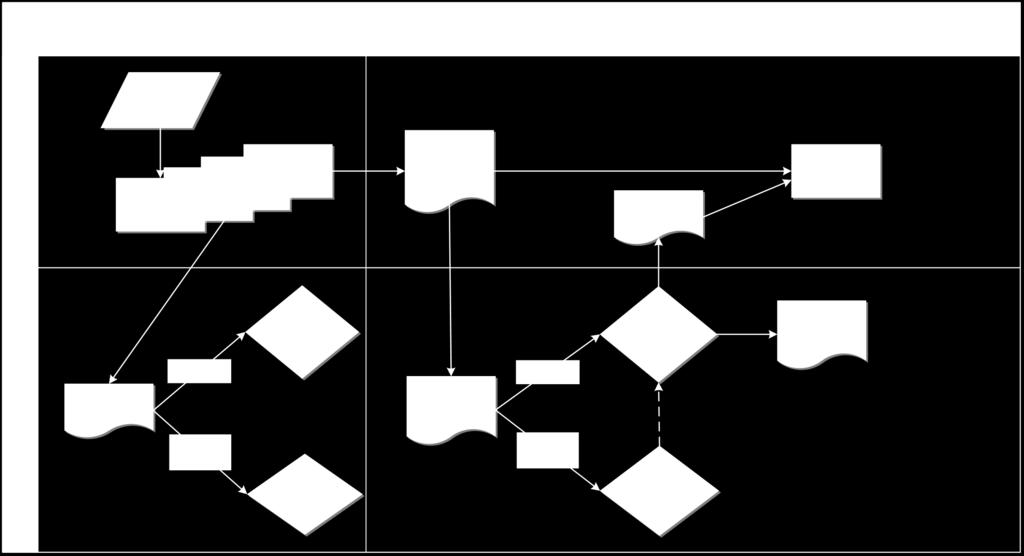
6
7 8 NHRA Reporting Reporting of events is of little value unless the data are analyzed. Regardless of the objective of the system whether to identify new and previously unsuspected hazards, discover trends, prioritize areas for remedial efforts, uncover common contributing factors, or develop strategies to decrease adverse events and patient harm neither the act of reporting nor the collection of data will accomplish that objective unless the data are analyzed and recommendations are made for change. Classification of the event is the first step in the analysis.
8 APPENDIX ONE Licensing & Registration Office National Health Regulatory Authority PO Box Manama Kingdom of Bahrain Report No: (for official use only) REPORT OF SERIOUS ADVERSE EVENT KINGDOM OF BAHRAIN Please complete for any serious adverse event which results in death or loss of a body part, or disability or permanent loss of bodily function. All information is protected under patient confidentiality. Is this a revision of an earlier SAE report to the NHRA Yes No If Yes: provide NHRA report no: 1. GENERAL INFORMATION Facility Name Facility license No: Address: Telephone Nos. (Mobile): (Business): Fax No.: Name of Person Submitting Report:: Title or Position: address: Profession: License No; (if applicable) 2. SERIOUS ADVERSE EVENT Please supply a simple and clear description of the event or situation you are reporting: Incident Date: Time AM PM Date Discovered: Time: AM PM
9 3. HOW WAS EVENT DISCOVERED Report by staff/physician Report by family / visitor Report by patient Assessment by patient after the event Review of chart / record Other 4. PATIENT INFORMATION In Patient Out patient Day Case Medical Record No: Gender: Male Female Patient Name: Address: Date of Birth: Date of Admission: 4. EVENT DETAILS Type of serious adverse event: Care Management Events In a health care facility Patient death / harm due to medication error Patient death / harm due to a haemolytic reaction / incompatible blood or blood products Maternal death / harm due to labour / delivery in a low risk pregnancy Patient death / harm due to hypoglycaemia Stage 3 or 4 pressure ulcer acquired after admission Patient death / harm due to spinal manipulation therapy or spinal tap. Other event causing patient death / harm. CPR No: Date of Discharge: (if applicable) Product or Device Event In a health care facility Patient death / harm due to the use of contaminated drugs/devices/biologics Patient death / harm due to the use of a device which it was not intended Patient death / harm due to intravascular air embolism Patient death / harm due the use of a single use device in which the device is used other than is intended New single use device Reprocessed single use device Other event causing patient death / harm Environmental Events In a health care facility Patient death / harm due to an electric shock Patient death / harm due to oxygen / gas delivery wrong gas delivery / contaminated gas delivery. Patient death / harm due to burn incurred from any source Patient death /harm due to a fall Patient death / harm due to the use of bed / restraint rails Other event causing patient death / harm Surgery Related Events In a health care facility Surgery performed on the wrong patient Surgery performed on the wrong body part Wrong surgical procedure performed on a patient Retention of foreign object in a patient after surgery or other procedure Intraoperative or immediately post operative coma or death. Other event causing patient death / harm
10 6. IF 5A WAS SELECTED, COMPLETE THIS SECTION What type of medication error occurred? (check all that apply) Wrong patient Wrong drug Wrong dose Wrong route Wrong frequency Wrong time Omission Other Brand / Product Name Wrong diluent / concentration /dosage form Generic Name: monitoring error 7. WHERE WAS THE PATIENT WHEN THE EVENT OCCURRED 8. IMMEDIATE CORRECTIVE ACTION TAKEN
11 9. FOR NHRA USE ONLY: Acknowledgement of SAE Report Date Processed: Follow up action Required: Assigned Inspector: RCA completed: Date Inspected: (if required) Inspection Report Completed: Date Issued Learning points identified and shared:
12 APPENDIX TWO Root Cause Analysis Report Template Lead Investigator: Position: Date: 1. THIS REPORT SHOULD BE USED FOR LEARNING PURPOSES ONLY. IT IS NOT TO BE USED TO APPORTION BLAME. 2. DO NOT USE ANY IDENTIFYING INFORMATION, USE DR X NURSE Y E.T.C
13 Root Cause Analysis Report Template 1. Incident Description Use this section to describe the incident and it s consequences, using only the facts. 2. Type of Investigation Undertaken Use this section to describe the methods used during the investigation team interviews, timelines, fishbone diagrams, 5 Whys, barrier analysis etc. Further assistance can be found Findings Use this section to describe the care delivery or service delivery problems and what the contributing factors were found to be. 4. Positive Features and Good Practice Use this section to highlight any positive features, good practice or actions that reduced the severity of the incident. 5. Recommendations and Action Plan Use this section to list the recommendations and the action plan to implement them. Recommendation Action By Whom Due Date The action plan may not be available when the RCA report is written. In this case, the action plan may be sent at a later date so as not to delay the publication of the RCA report s findings.
14 6. Appendices Use this section to record: Lists of documents used Copies of any relevant documents or relevant sections Electronic versions of annotated fishbone diagrams, time lines, barrier analysis tables etc.
15 APPENDIX THREE Serious Adverse events that should be reported to the NHRA Care Management Events in a health care facility Patient death / harm due to medication error Patient death / harm due to a haemolytic reaction / incompatible blood or blood products Maternal death / harm due to labour / delivery in a low risk pregnancy Patient death / harm due to hypoglycaemia Stage 3 or 4 pressure ulcer acquired after admission Patient death / harm due to spinal manipulation therapy or spinal tap. Suicide of an in patient Other event causing patient death / harm. Environmental Events in a health care facility Patient death / harm due to an electric shock Patient death / harm due to oxygen / gas delivery wrong gas delivery / contaminated gas delivery. Patient death / harm due to burn incurred from any source Patient death /harm due to a fall Patient death / harm due to the use of bed / restraint rails Other event causing patient death / harm Product or Device Event in a health care facility Patient death / harm due to the use of contaminated drugs/devices/biologics Patient death / harm due to the use of a device which it was not intended Patient death / harm due to intravascular air embolism Patient death / harm due the use of a single use device in which the device is used other than is intended New single use device Reprocessed single use device Other event causing patient death / harm Surgery Related Events in a health care facility Surgery performed on the wrong patient Surgery performed on the wrong body part Wrong surgical procedure performed on a patient Retention of foreign object in a patient after surgery or other procedure Intraoperative or immediately post-operative coma or death. Other event causing patient death / harm
VERMONT2008 Patient Safety, Surveillance, and Improvement System
 VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
Subject: Hospital-Acquired Conditions (Page 1 of 5)
") Subject: Hospital-Acquired Conditions (Page 1 of 5) Objective: I. To facilitate safe patient care for all Health Share/Tuality Health Alliance (THA) members. II. To encourage and support provider efforts
Subject: Hospital-Acquired Conditions (Page 1 of 5) Objective: I. To facilitate safe patient care for all Health Share/Tuality Health Alliance (THA) members. II. To encourage and support provider efforts
GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH)
") GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH) Effective Date: 02/12 Page No. 1 of 7 I. PURPOSE To comply with mandated reporting requirements of
GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH) Effective Date: 02/12 Page No. 1 of 7 I. PURPOSE To comply with mandated reporting requirements of
POLICY NAME POLICY # Sentinel, Adverse Event and Near Miss. CSP Reporting and Investigation
 Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Purpose To outline a reporting system that promotes client safety by learning from experiences and utilizing the results of investigations and data analysis to prepare and disseminate recommendations for
Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors
 Transparency & Accountability are Critical to Reducing Medical Errors") Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors Tens of thousands of lives are forever changed each year as a result of healthcare errors. There is
Serious Reportable Events (SREs) Transparency & Accountability are Critical to Reducing Medical Errors Tens of thousands of lives are forever changed each year as a result of healthcare errors. There is
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Serious Reportable Events in Healthcare 2011 Update
 Serious Reportable Events in Healthcare 2011 Update July 19, 2011 1 Overview Purpose 2002, 2006, 2011 Facilitate uniform, comparable public reporting Enable systematic learning Ensure currency & appropriateness
Serious Reportable Events in Healthcare 2011 Update July 19, 2011 1 Overview Purpose 2002, 2006, 2011 Facilitate uniform, comparable public reporting Enable systematic learning Ensure currency & appropriateness
Consumers Union/Safe Patient Project Page 1 of 7
 Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
HALF YEAR REPORT ON SENTINEL EVENTS
 HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: September 9, 2013 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL
 UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
UPMC POLICY AND PROCEDURE MANUAL POLICY: INDEX TITLE: HS-PT1200 Patient Safety SUBJECT: Reportable Patient Events DATE: December 4, 2015 I. POLICY It is the policy of UPMC to encourage and promote a philosophy
POLICIES AND PROCEDURE MANUAL
 POLICIES AND PROCEDURE MANUAL Policy: MP209 Section: Medical Benefit Policy Subject: Medical Error Never Events, Hospital Acquired Conditions, and Hospital Readmission Review I. Policy: Medical Error Never
POLICIES AND PROCEDURE MANUAL Policy: MP209 Section: Medical Benefit Policy Subject: Medical Error Never Events, Hospital Acquired Conditions, and Hospital Readmission Review I. Policy: Medical Error Never
Preventing Serious Reportable Events in Health Care
 Preventing Serious Reportable Events in Health Care The National Quality Forum (NQF), a coalition of public and private healthcare sector leaders who are focused on improving healthcare quality and patient
Preventing Serious Reportable Events in Health Care The National Quality Forum (NQF), a coalition of public and private healthcare sector leaders who are focused on improving healthcare quality and patient
ETHICAL CONSIDERATIONS THAT ARISE IN LONG TERM CARE PART 2 REPORTING OBLIGATIONS
 ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
(1) Provides a brief overview of CMS Medicare payment policy for selected HACs;
 Provides a brief overview of CMS Medicare payment policy for selected HACs;") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations SMDL #08-004
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-26-12 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations SMDL #08-004
Serious Reportable Events Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014
 Serious Reportable Events 2011-2013 Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014 1 Overview Background Serious Reportable Events Quality Improvement Initiative Outcomes
Serious Reportable Events 2011-2013 Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014 1 Overview Background Serious Reportable Events Quality Improvement Initiative Outcomes
BAY-ARENAC BEHAVIORAL HEALTH AUTHORITY POLICIES AND PROCEDURES MANUAL
 Page: 1 of 14 Policy It is the policy of Bay-Arenac Behavioral Health Authority (BABHA) that all adverse events, such as unusual events (including risk), critical incidents (including all deaths) and sentinel
Page: 1 of 14 Policy It is the policy of Bay-Arenac Behavioral Health Authority (BABHA) that all adverse events, such as unusual events (including risk), critical incidents (including all deaths) and sentinel
Safety Reporting in Clinical Research Policy Final Version 4.0
 Safety Reporting in Clinical Research Policy Final Version 4.0 Category: Summary: Equality Assessment undertaken: Impact Policy The Medicines for Human Use (Clinical Trials) Regulations 2004 and subsequent
Safety Reporting in Clinical Research Policy Final Version 4.0 Category: Summary: Equality Assessment undertaken: Impact Policy The Medicines for Human Use (Clinical Trials) Regulations 2004 and subsequent
Key California Health Laws: AB 211, SB 541. Overview
 Key California Health Laws: AB 211, SB 541 Shirley P. Morrigan, Esq. Foley & Lardner LLP 555 South Flower, #3500 Los Angeles, CA 90071 tel: (213) 972-4668 fax: (213) 486-0065 cell: (310) 488-8788 email:
Key California Health Laws: AB 211, SB 541 Shirley P. Morrigan, Esq. Foley & Lardner LLP 555 South Flower, #3500 Los Angeles, CA 90071 tel: (213) 972-4668 fax: (213) 486-0065 cell: (310) 488-8788 email:
Sentinel Events and S Patient Patient entinel Event Alerts Safety Act Safety Ac Revised: BW/September 2010
 Sentinel Events Sentinel Events and Sentinel Event Alerts Revised: BW/September 2010 Patient Patient Safety Safety Act Act What is a Sentinel Event? 0 A sentinel event is an unexpected occurrence involving
Sentinel Events Sentinel Events and Sentinel Event Alerts Revised: BW/September 2010 Patient Patient Safety Safety Act Act What is a Sentinel Event? 0 A sentinel event is an unexpected occurrence involving
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA
 Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Walking the Tightrope with a Safety Net Blood Transfusion Process FMEA AnMed Health AnMed Health, located in Anderson, South Carolina, is one of the largest and most technologically advanced health systems
Clinical Interdepartmental Policy and Procedure
 Clinical Interdepartmental Policy and Procedure Policy: Staff Response to Medical Errors/Adverse Events Policy Number: MR-006 Joseph S. Gordy, CEO Signature: Flagler Hospital Originator: President Coordinating
Clinical Interdepartmental Policy and Procedure Policy: Staff Response to Medical Errors/Adverse Events Policy Number: MR-006 Joseph S. Gordy, CEO Signature: Flagler Hospital Originator: President Coordinating
Department of Defense INSTRUCTION. SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP)
 Patient Safety Program (PSP) (MHSPSP)") Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
SAFETY AND QUALITY INDICATORS
 NATIONAL COLLECTION AND REPORTING OF SAFETY AND QUALITY INDICATORS BY PRIVATE HOSPITALS The National Collection and Reporting of Safety & Quality Indicators by Private Hospitals is an independent national
NATIONAL COLLECTION AND REPORTING OF SAFETY AND QUALITY INDICATORS BY PRIVATE HOSPITALS The National Collection and Reporting of Safety & Quality Indicators by Private Hospitals is an independent national
February New Zealand Health and Disability Services National Reportable Events Policy 2012
 February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
CPSM STANDARDS POLICIES For Rural Standards Committees
 CPSM STANDARDS POLICIES The Central Standards Committee (CSC) of The College of Physicians and Surgeons of Manitoba (CPSM) is a legislated standing committee of the CPSM and reports directly to the Council.
CPSM STANDARDS POLICIES The Central Standards Committee (CSC) of The College of Physicians and Surgeons of Manitoba (CPSM) is a legislated standing committee of the CPSM and reports directly to the Council.
Sample Reportable Events
 Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
Sample Reportable Events This list serves as a guideline of event types typically reported through the ERS (Event Reporting System), online event reporting software. These examples come from hospitals
Healthcare Facility Regulation
 Healthcare Facility Regulation October 21, 2016 Presented by Melanie Simon Division Chief 0 Our Mission HFR is committed to protecting Georgia s health care consumers and ensuring the quality of health
Healthcare Facility Regulation October 21, 2016 Presented by Melanie Simon Division Chief 0 Our Mission HFR is committed to protecting Georgia s health care consumers and ensuring the quality of health
Cynthia M. Kirchner, MPH, Director, Quality Improvement. Emmanuel Noggoh, Director, Health Care Quality Assessment
 2010 Summary Report Office of Health Care Quality Assessment Report Preparation Team Cynthia M. Kirchner, MPH, Director, Quality Improvement Emmanuel Noggoh, Director, Health Care Quality Assessment Mary
2010 Summary Report Office of Health Care Quality Assessment Report Preparation Team Cynthia M. Kirchner, MPH, Director, Quality Improvement Emmanuel Noggoh, Director, Health Care Quality Assessment Mary
POLICY/PROCEDURE PLAN GUIDELINE. SECTION: I Administrative
 TITLE: Patient Safety Occurrence Report POLICY PTCADM100.23 SCOPE: Children's Hospital of Pittsburgh ("CHP") Main Children's Hospital of Pittsburgh Satellites Children's Hospital of Pittsburgh Ambulatory
TITLE: Patient Safety Occurrence Report POLICY PTCADM100.23 SCOPE: Children's Hospital of Pittsburgh ("CHP") Main Children's Hospital of Pittsburgh Satellites Children's Hospital of Pittsburgh Ambulatory
ED0028 Adverse event, critical incident, serious issue, and near miss procedure
 ED0028 Adverse event, critical incident, serious issue, and near miss procedure 1. Full description Adverse event, critical incident, serious issue, 2. Preamble Doctors working in Australia have responsibilities
ED0028 Adverse event, critical incident, serious issue, and near miss procedure 1. Full description Adverse event, critical incident, serious issue, 2. Preamble Doctors working in Australia have responsibilities
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager
 Ratchada Prakongsai Senior Manager") Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Quality Improvement and Patient Safety (QPS) Ratchada Prakongsai Senior Manager Overview 2 Comprehensive approach to quality improvement and patient safety that impacts all aspects of the facility s operation.
Post Market Surveillance Requirements. SAMED Regulatory Conference 2 December 2015
 Post Market Surveillance Requirements SAMED Regulatory Conference 2 December 2015 Topics Surveillance & Vigilance Adverse Events Reportable Adverse Events Reporting Adverse Events Time frames Exemptions
Post Market Surveillance Requirements SAMED Regulatory Conference 2 December 2015 Topics Surveillance & Vigilance Adverse Events Reportable Adverse Events Reporting Adverse Events Time frames Exemptions
OSH Incident Reporting & Investigation Procedure
 Contents Document Review and Approval... 2 1. Purpose and Scope... 3 2. Procedure... 3 2.1 Injury, Illness and OSH Incident Classification... 3 2.2 Recordable and Reportable Incidents... 4 2.3 Incident
Contents Document Review and Approval... 2 1. Purpose and Scope... 3 2. Procedure... 3 2.1 Injury, Illness and OSH Incident Classification... 3 2.2 Recordable and Reportable Incidents... 4 2.3 Incident
ADVERSE HEALTH EVENTS IN MINNESOTA
 S E C O N D ANNUAL F EBRUARY 2006 TABLE OF CONTENTS Introduction.................................................. 3 Background................................................... 4 How to use this report.........................................
S E C O N D ANNUAL F EBRUARY 2006 TABLE OF CONTENTS Introduction.................................................. 3 Background................................................... 4 How to use this report.........................................
Overview of Root Cause Analysis
 Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Human Samples in Research
 Human Samples in Research Adverse Event Reporting Document Identifier HTA-11-SOP-Adverse Event Reporting AUTHOR APPROVER EFFECTIVE DATE: Name and role Signature and date Name and role Signature and date
Human Samples in Research Adverse Event Reporting Document Identifier HTA-11-SOP-Adverse Event Reporting AUTHOR APPROVER EFFECTIVE DATE: Name and role Signature and date Name and role Signature and date
INCIDENT POLICY Page 1 of 15 July 2017
 Page 1 of 15 Policy Applies To All Mercy Hospital Staff Credentialed Medical Specialists and Allied Health Personnel are required to indicate understanding of the incident policy via the credentialing
Page 1 of 15 Policy Applies To All Mercy Hospital Staff Credentialed Medical Specialists and Allied Health Personnel are required to indicate understanding of the incident policy via the credentialing
Never Events LISA Matt Provost
 Never Events LISA 2017 Matt Provost mattpro@yelp.com/@hypersupermeta Yelp s Mission Connecting people with great local businesses. History of the NHS World s first universal health care system - June 1948
Never Events LISA 2017 Matt Provost mattpro@yelp.com/@hypersupermeta Yelp s Mission Connecting people with great local businesses. History of the NHS World s first universal health care system - June 1948
Root Cause Analysis LITE (RCA Lite)
") Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Root Cause Analysis LITE (RCA Lite) INTRODUCTION The root cause analysis Lite tool is designed to assist Ottawa Hospital teams to review an adverse event or near miss, identify root causes of the event
Sponsor Responsibilities. Roles and Responsibilities. EU Directives. UK Law
 EU Directives Pharmacovigilance Legislation, SOPs and Reporting Louise Boldy, Governance & Safety Manager David Martin, Pharmacovigilance Monitor EU Legislation 2001/20/EC 2005/28/EC EudraLex Vol 10 UK
EU Directives Pharmacovigilance Legislation, SOPs and Reporting Louise Boldy, Governance & Safety Manager David Martin, Pharmacovigilance Monitor EU Legislation 2001/20/EC 2005/28/EC EudraLex Vol 10 UK
Health and Safety Strategy
 NHS Newcastle Gateshead Clinical Commissioning Group Health and Safety Strategy Document Status Equality Impact Assessment Document Ratified/Approved By Final No impact Quality, Safety and Risk Committee
NHS Newcastle Gateshead Clinical Commissioning Group Health and Safety Strategy Document Status Equality Impact Assessment Document Ratified/Approved By Final No impact Quality, Safety and Risk Committee
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING
 Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
NERC Improving Human Performance
 NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
TITLE: Reporting Adverse Events SOP #: RCO-204 Page: 1 of 5 Effective Date: 01/31/18
 SOP #: RCO-204 Page: 1 of 5 1. POLICY STATEMENT: The research team is responsible for recognizing changes in subject health that may qualify as adverse events, classifying those results as defined in the
SOP #: RCO-204 Page: 1 of 5 1. POLICY STATEMENT: The research team is responsible for recognizing changes in subject health that may qualify as adverse events, classifying those results as defined in the
PROMPTLY REPORTABLE EVENTS
 PROMPTLY REPORTABLE EVENTS PURPOSE AND SCOPE To define the structure and responsibility for reporting unanticipated problems that occurs during the conduct of research. APPLICABLE REGULATIONS Policy II.02
PROMPTLY REPORTABLE EVENTS PURPOSE AND SCOPE To define the structure and responsibility for reporting unanticipated problems that occurs during the conduct of research. APPLICABLE REGULATIONS Policy II.02
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
BY ORDER OF THE COMMANDER 59TH MEDICAL WING 59TH MEDICAL WING INSTRUCTION 44-130 10 JANUARY 2017 Medical PATIENT SAFETY COMPLIANCE WITH THIS PUBLICATION IS MANDATORY ACCESSIBILITY: Publications and forms
7084 MANAGEMENT OF INCIDENTS Facility Management Plan
 6 7084 MANAGEMENT OF INCIDENTS 7084.3 Facility Management Plan Each facility shall have a risk management plan that includes: 1. Explicit assignment of responsibilities for the facility s risk management
6 7084 MANAGEMENT OF INCIDENTS 7084.3 Facility Management Plan Each facility shall have a risk management plan that includes: 1. Explicit assignment of responsibilities for the facility s risk management
I. Scope This policy defines unanticipated problems and adverse events and establishes the reporting process and timeline.
 Human Research Protection Program Policies & Procedures Unanticipated Problems and Adverse Events Version 3.0 Date Effective: 11.9.2012 Research Integrity Office Mail code L106-RI Portland, Oregon 97239-3098
Human Research Protection Program Policies & Procedures Unanticipated Problems and Adverse Events Version 3.0 Date Effective: 11.9.2012 Research Integrity Office Mail code L106-RI Portland, Oregon 97239-3098
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
New Jersey Department of Health Report Preparation Team. Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics
 2012 Summary Report New Jersey Department of Health Report Preparation Team Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics Emmanuel Noggoh, Director Health Care Quality
2012 Summary Report New Jersey Department of Health Report Preparation Team Abate Mammo, PhD, Acting Executive Director Healthcare Quality and Informatics Emmanuel Noggoh, Director Health Care Quality
Patient Care Coordination Variance Reporting
 Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
IDENTIFYING, RECORDING AND REPORTING ADVERSE EVENTS FOR CLINICAL INVESTIGATIONS OF MEDICAL DEVICES
 IDENTIFYING, RECORDING AND REPORTING ADVERSE EVENTS FOR CLINICAL INVESTIGATIONS OF MEDICAL DEVICES DOCUMENT NO.: CR012 v2.0 AUTHOR: Raymond French ISSUE DATE: 18 September 2017 EFFECTIVE DATE: 02 October
IDENTIFYING, RECORDING AND REPORTING ADVERSE EVENTS FOR CLINICAL INVESTIGATIONS OF MEDICAL DEVICES DOCUMENT NO.: CR012 v2.0 AUTHOR: Raymond French ISSUE DATE: 18 September 2017 EFFECTIVE DATE: 02 October
Improving the reporting of medication-related safety incidents
 Rationale Improving the reporting of medication-related safety incidents Research shows that organisations which regularly report more patient safety incidents usually have a stronger learning culture
Rationale Improving the reporting of medication-related safety incidents Research shows that organisations which regularly report more patient safety incidents usually have a stronger learning culture
Go for the Gold. Incorporating Regulatory Issues into the Quality Management Process. June 9 11, 2008 Starr Pass Resort Tucson, Arizona
 Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
Biomedical IRB MS #
 Department for Human Research Protections Institutional Review Boards Biomedical IRB MS # 1035 419-383-6796 IRB.Biomed@utoledo.edu Social, Behavioral and Educational IRB MS # 944 419-530-6167 IRB.SBE@utoledo.edu
Department for Human Research Protections Institutional Review Boards Biomedical IRB MS # 1035 419-383-6796 IRB.Biomed@utoledo.edu Social, Behavioral and Educational IRB MS # 944 419-530-6167 IRB.SBE@utoledo.edu
IS YOUR QAPI COP READY?
 IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
Contact Hours (CME version ONLY) Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff
 Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff") 1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Patient Safety Hazard Risk Assessment FY 2018
 Completed by: Patient Safety Committee Date Completed: Ocber 31, 2017 Methodology: Information utilized complete this Patient Safety Hazard Assessment included availa patterns/trends, high risk, prom prone
Completed by: Patient Safety Committee Date Completed: Ocber 31, 2017 Methodology: Information utilized complete this Patient Safety Hazard Assessment included availa patterns/trends, high risk, prom prone
C H A P T E R HAZARD ANALYSIS
 C H A P T E R 8 HAZARD ANALYSIS 8.1. Safety Inspections All areas and operations of each workplace, including office areas, must be inspected at least once a year. More frequent inspections shall be conducted
C H A P T E R 8 HAZARD ANALYSIS 8.1. Safety Inspections All areas and operations of each workplace, including office areas, must be inspected at least once a year. More frequent inspections shall be conducted
The Patient Safety Act Reporting and RCA Requirements
 The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
Standard Operating Procedure
 Standard Operating Procedure SOP number: SOP full title: SOP-JRO-07-004 Recording, managing and reporting Adverse Events for Clinical Trials of Investigational Medicinal Products and trials of Advanced
Standard Operating Procedure SOP number: SOP full title: SOP-JRO-07-004 Recording, managing and reporting Adverse Events for Clinical Trials of Investigational Medicinal Products and trials of Advanced
Defining incident-based peer review
 CHAPTER 1 Defining incident-based peer review Learning objectives After reading this chapter, the participant will be able to: Identify three external sources imposing higher nursing standards Discuss
CHAPTER 1 Defining incident-based peer review Learning objectives After reading this chapter, the participant will be able to: Identify three external sources imposing higher nursing standards Discuss
Incident Reporting and Investigation Guideline
 Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
Clinical Governance & Risk Management Awareness. Incl. investigation of accidents, complaints and claims. Unit 2
 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
Guideline for the notification of serious breaches of Regulation (EU) No 536/2014 or the clinical trial protocol
 No 536/2014 or the clinical trial protocol") 1 2 31 January 2017 EMA/430909/2016 3 4 5 Guideline for the notification of serious breaches of Regulation (EU) No 536/2014 or Draft Adopted by GCP Inspectors Working Group (GCP IWG) 30 January 2017 Adopted
1 2 31 January 2017 EMA/430909/2016 3 4 5 Guideline for the notification of serious breaches of Regulation (EU) No 536/2014 or Draft Adopted by GCP Inspectors Working Group (GCP IWG) 30 January 2017 Adopted
Guidelines for Disclosure Process. 1) Patient disclosure does not include:
 Patient disclosure does not include:") Disclosing Serious Unanticipated Adverse Events Educational Guidelines for Washington University Physicians Adopted: June 21, 2007 Amended: March 18, 2008 Timely, honest and sustained communication with
Disclosing Serious Unanticipated Adverse Events Educational Guidelines for Washington University Physicians Adopted: June 21, 2007 Amended: March 18, 2008 Timely, honest and sustained communication with
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
CHAPTER 12 -QUALITY MANAGEMENT AND PERFORMANCE IMPROVEMENT
 CHAPTER 12 -QUALITY MANAGEMENT AND PERFORMANCE IMPROVEMENT 12.0 QUALITY MANAGEMENT REQUIREMENTS Health Choice Integrated Care works in partnership with providers to continuously monitor and improve the
CHAPTER 12 -QUALITY MANAGEMENT AND PERFORMANCE IMPROVEMENT 12.0 QUALITY MANAGEMENT REQUIREMENTS Health Choice Integrated Care works in partnership with providers to continuously monitor and improve the
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator
 Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
Blood Sample Labeling Shean Strong, QI Director Lisle Mukai, QI Coordinator Presented at Webex Conferences: July 20, 21, & 22, 2010 Blood Sample Labeling Seminar 6255 West Sunset Blvd Los Angeles, CA Blood
Version Number: 003. On: September 2017 Review Date: September 2020 Distribution: Essential Reading for: Information for: Page 1 of 13
 CONTROLLED DOCUMENT Reporting Research Incidents and Breaches Policy CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the framework and principles for reporting
CONTROLLED DOCUMENT Reporting Research Incidents and Breaches Policy CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the framework and principles for reporting
3/9/2010. Objectives. Pharmacist Role in Medication Safety and Regulatory Compliance
 Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
NEWCASTLE CLINICAL TRIALS UNIT STANDARD OPERATING PROCEDURES
 NEWCASTLE CLINICAL TRIALS UNIT STANDARD OPERATING PROCEDURES SOP details SOP title: Safety Reporting in CTIMPs and ATMPs SOP number: TM-003 SOP category: Trial Management Version number: 04 Version date:
NEWCASTLE CLINICAL TRIALS UNIT STANDARD OPERATING PROCEDURES SOP details SOP title: Safety Reporting in CTIMPs and ATMPs SOP number: TM-003 SOP category: Trial Management Version number: 04 Version date:
Clinical Research Seminar
 Clinical Research Seminar HOW TO DEVELOP A CORRECTIVE AND PREVENTIVE ACTION PLAN (THAT EVEN THE IRB AND FDA WILL LOVE) April 11, 2018 Fiona Rice, MPH Human Research Quality Manager fionar@bu.edu Mary-Tara
Clinical Research Seminar HOW TO DEVELOP A CORRECTIVE AND PREVENTIVE ACTION PLAN (THAT EVEN THE IRB AND FDA WILL LOVE) April 11, 2018 Fiona Rice, MPH Human Research Quality Manager fionar@bu.edu Mary-Tara
Incident Management June 2018
 Incident Management June 2018 Table of Contents 1.0 Purpose... 1 2.0 Scope... 1 3.0 Definitions... 1 4.0 Responsibilities... 2 4.1. Senior Executives, Deans and Directors... 2 4.2. Supervisors... 3 4.3.
Incident Management June 2018 Table of Contents 1.0 Purpose... 1 2.0 Scope... 1 3.0 Definitions... 1 4.0 Responsibilities... 2 4.1. Senior Executives, Deans and Directors... 2 4.2. Supervisors... 3 4.3.
Guide to Incident Reporting for In-vitro Diagnostic Medical Devices
 Guide to Incident Reporting for In-vitro Diagnostic Medical Devices SUR-G0004-4 02 AUGUST 2012 This guide does not purport to be an interpretation of law and/or regulations and is for guidance purposes
Guide to Incident Reporting for In-vitro Diagnostic Medical Devices SUR-G0004-4 02 AUGUST 2012 This guide does not purport to be an interpretation of law and/or regulations and is for guidance purposes
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Practice Guidance: Large Scale Investigations
 Practice Guidance: Large Scale Investigations Version: Version 1: April 2014 Ratified by: Leeds Safeguarding Adults Board Date ratified: April 2014 Author/Originator of title Safeguarding Policy, Protocols
Practice Guidance: Large Scale Investigations Version: Version 1: April 2014 Ratified by: Leeds Safeguarding Adults Board Date ratified: April 2014 Author/Originator of title Safeguarding Policy, Protocols
Policy for the Reporting and Management of Incidents Including Serious Incidents. Version Number: 006
 CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
January Version 2. Accreditation Standards for Medical Centers
 January 2018 Version 2 Accreditation Standards for Medical Centers 0 Forward The National Health Regulatory Authority (NHRA) is dedicated to ensure that health services in the Kingdom of Bahrain meet the
January 2018 Version 2 Accreditation Standards for Medical Centers 0 Forward The National Health Regulatory Authority (NHRA) is dedicated to ensure that health services in the Kingdom of Bahrain meet the
POLICY ON RESEARCH RELATED ADVERSE EVENT REPORTING
 POLICY ON RESEARCH RELATED ADVERSE EVENT REPORTING CLASSIFICATION TRUST POLICY NUMBER APPROVING COMMITTEE R & D Governance Committee RATIFYING COMMITTEE Quality & Risk Committee DATE RATIFIED October 2009
POLICY ON RESEARCH RELATED ADVERSE EVENT REPORTING CLASSIFICATION TRUST POLICY NUMBER APPROVING COMMITTEE R & D Governance Committee RATIFYING COMMITTEE Quality & Risk Committee DATE RATIFIED October 2009
ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS
 JANUARY 2005 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS FIRST ANNUAL PUBLIC REPORT 3 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS MDH 2 0 0 5 TABLE OF CONTENTS 2 HOW TO USE THIS REPORT 3 SELECTED SAFETY
JANUARY 2005 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS FIRST ANNUAL PUBLIC REPORT 3 ADVERSE HEALTH EVENTS IN MINNESOTA HOSPITALS MDH 2 0 0 5 TABLE OF CONTENTS 2 HOW TO USE THIS REPORT 3 SELECTED SAFETY
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS
 I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
Various Views on Adverse Events: a collection of definitions.
 Various Views on Adverse Events: a collection of definitions. April 20, 2008 Werner CEUSTERS a,1, Maria CAPOLUPO b, Georges DE MOOR c, Jos DEVLIES c a New York State Center of Excellence in Bioinformatics
Various Views on Adverse Events: a collection of definitions. April 20, 2008 Werner CEUSTERS a,1, Maria CAPOLUPO b, Georges DE MOOR c, Jos DEVLIES c a New York State Center of Excellence in Bioinformatics
SERIOUS REPORTABLE EVENTS IN HEALTHCARE 2011 UPDATE: A CONSENSUS REPORT
 DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS IN HEALTHCARE 2011 UPDATE: A CONSENSUS REPORT DRAFT REPORT FOR VOTING DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS
DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS IN HEALTHCARE 2011 UPDATE: A CONSENSUS REPORT DRAFT REPORT FOR VOTING DRAFT DRAFT DRAFT NATIONAL QUALITY FORUM SERIOUS REPORTABLE EVENTS
NEWCASTLE CLINICAL TRIALS UNIT STANDARD OPERATING PROCEDURES
 NEWCASTLE CLINICAL TRIALS UNIT STANDARD OPERATING PROCEDURES SOP details SOP title: Safety Reporting in CTIMPs and ATMPs SOP number: TM 003 SOP category: Trial Management Version number: 03 Version date:
NEWCASTLE CLINICAL TRIALS UNIT STANDARD OPERATING PROCEDURES SOP details SOP title: Safety Reporting in CTIMPs and ATMPs SOP number: TM 003 SOP category: Trial Management Version number: 03 Version date:
Sentinel Event Data. Root Causes by Event Type Copyright, The Joint Commission
 Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
Marie-Claire Rickard, RG and GCP Manager Jimena Lovos, Quality Assurance Manager Elizabeth Clough, R&D Governance Operations Manager
 Standard Operating Procedures (SOP) for: Pharmacovigilance processing for the JRMO SOP Number: 26c Version Number: V1 Effective Date: 5/8/16 Review Date: 5/8/17 Author: Reviewer: Reviewer: Authorisation:
Standard Operating Procedures (SOP) for: Pharmacovigilance processing for the JRMO SOP Number: 26c Version Number: V1 Effective Date: 5/8/16 Review Date: 5/8/17 Author: Reviewer: Reviewer: Authorisation:
SAMPLE: Peer Review Referral Policy
 SUBJECT: SCOPE: NUMBER: EFFECTIVE DATE: APPROVED BY: DISTRIBUTION: DATE: I. Purpose Statement To establish a uniform and consistent method of generic screening of clinical indicators, as well as for the
SUBJECT: SCOPE: NUMBER: EFFECTIVE DATE: APPROVED BY: DISTRIBUTION: DATE: I. Purpose Statement To establish a uniform and consistent method of generic screening of clinical indicators, as well as for the
POLICY ON INCIDENT REPORTING AND INCIDENT MANAGEMENT
 POLICY ON INCIDENT REPORTING AND INCIDENT MANAGEMENT It is the policy of ACHIEVA to establish procedures for the prevention and management of incidents in accordance with ODP Incident Management Bulletin
POLICY ON INCIDENT REPORTING AND INCIDENT MANAGEMENT It is the policy of ACHIEVA to establish procedures for the prevention and management of incidents in accordance with ODP Incident Management Bulletin
Thresholds for initiating Adult Safeguarding Referrals or Care Concerns
 September 2012 Thresholds for initiating Adult Safeguarding Referrals or Care Concerns Establishing whether or not abuse of a vulnerable adult has taken place is not always straightforward. In some cases,
September 2012 Thresholds for initiating Adult Safeguarding Referrals or Care Concerns Establishing whether or not abuse of a vulnerable adult has taken place is not always straightforward. In some cases,
SKILLED NURSING HOME RISK MONITOR METRICS
 The Risk Monitor offers three views: FACILITY 1st column, total number year-to-date (calculated by the system, from January and including the current month); 2nd column, actual numbers submitted by your
The Risk Monitor offers three views: FACILITY 1st column, total number year-to-date (calculated by the system, from January and including the current month); 2nd column, actual numbers submitted by your
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM
 Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Patient Safety is Everyone s Responsibility Tammy Brock, MSN RN CPHRM Objectives Know TJC 2016 National Patient Safety Goals Discuss human factors on patient safety What is your role in patient safety?
Incident Management Procedure
 Incident Management Procedure Table of Contents 1 Intent... 3 2 Scope... 3 3 Responsibility... 3 4 Incident Management... 4 4.1 Incident Response And Investigation Flowchart... 4 4.2 Invoke Emergency Response...
Incident Management Procedure Table of Contents 1 Intent... 3 2 Scope... 3 3 Responsibility... 3 4 Incident Management... 4 4.1 Incident Response And Investigation Flowchart... 4 4.2 Invoke Emergency Response...