Teamwork and Communication for Quality & Safety: It s More Than Checklists
|
|
|
- Lillian Moore
- 6 years ago
- Views:
Transcription
1 Teamwork and Communication for Quality & Safety: It s More Than Checklists James P. Bagian, MD, PE Director Center for Healthcare Engineering and Patient Safety University of Michigan jbagian@med.umich.edu
2 Overview Problem Background Strategy Interventions
3 VA
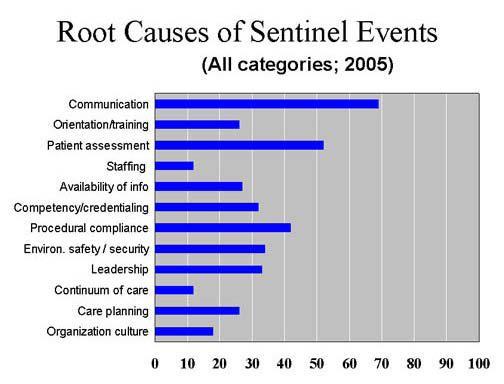
4 Root Cause Analyses (RCA) Database* ~70% to 80% of RCAs cited COMMUNICATION FAILURE as, at least one of the root causes/contributing factors for an adverse event or close call report. *SPOT Database: VA National Center for Patient Safety, April, 2008 Completed RCAs, Number = 8661.
5
6 Assumptions Current OR situation was unacceptable Communication was factor Improvement was possible The risk from intervening was less than the status quo Didn t require absolute evidence base, evaluate on the fly
7 Communication Skills In medical school and nursing school, the focus is on successful communication with the patient.
8 Aviation Safety & Crew Resource Management (CRM)




9 Tenerife March 1977 Pan Am KLM


10 Fatalities - 583
11 Crew Resource Management (CRM)* Origin: NASA workshops examining the role of human error in airline crashes Research into aviation accidents in 1970s Definition: Using all available sources information, equipment, and people to achieve safe and efficient operations. Focus: safety, efficiency, and morale of humans working together LOFT: Line Oriented Flight Training Work in flight simulators and measurement of airline crew performance Briefings and Debriefings * Musson D, Helmreich RL. Team training and resource management in health care: Current issues and future directions. Harvard Health Policy Review. 2004; 5(1):
12 CRM Training* Required by FAA and worldwide the way of doing business Aircrew performance measured by materials, organization, individual, and group variables Expanded aviation training from technical focus to human factors dimensions stress, fatigue, communication, shared awareness, and teamwork Outcomes: efficiency, safety, customer satisfaction Airline crew surveys: CRM relevant, useful, and effective in changing attitudes and behavior to improve safety CRM accepted by industry on face validity * Musson D, Helmreich RL. Team training and resource management in health care: Current issues and future directions. Harvard Health Policy Review. 2004; 5(1):

13 Institute of Medicine establish team training programs for personnel in critical care areas using proven methods such as the crew resource management training techniques employed in aviation. Corrigan J, Kohn LT, Donaldson MS. To Err Is Human. Washington, DC: National Academy Press; 2000.
14 Teamwork
15 What are the characteristics of a TEAM?

16 Characteristics of a Powerful Team Common Purpose Excellent Communications Clear Roles Exceptional Results Solid Relationships Accepted Leadership Effective Processes



17 VHA NCPS Medical Team Training Program Mean = 74 Attendees Per Learning Session Largest One Day Session = 208 (Baltimore, MD Jan 14, 2010) Largest Facility Attendance = 356 (Dallas, TX December 9-11, 2008) 18
18 MTT Plan Identify and guide implementation team at site Months Prior Define responsibilities, goals, and tools (e.g., checklist content) Baseline data e.g., SAQ Weeks/Days Prior OR-wide training on communication, briefings and debriefings Implement Follow-up, measure and assist/advise Months
19 Culture Measurement Survey open to all MDs, RNs, Techs in OR and PACU SAQ (Safety Attitude Questionnaire) Nationally accepted, validated, normed Short (~35 questions) Online Anonymous Shorter and more focused than AHRQ
20 Briefings Dialogue among principals using concise, relevant information to promote clear and effective communication - Real time - Face-to-face - All team members present - All team members participate
21 Why Do a Briefing? Establish a platform for common understanding Gives people permission to be frank & honest Gets everyone on the same page Provides a structure for collaborative planning Creates a shared mental model

22 23
23 Situational Awareness Definition: The continuous perception of self and team in relation to the dynamic environment and the ability to make adjustments. The one most important aid in maintaining Situational Awareness is a common understanding of the briefed plan.
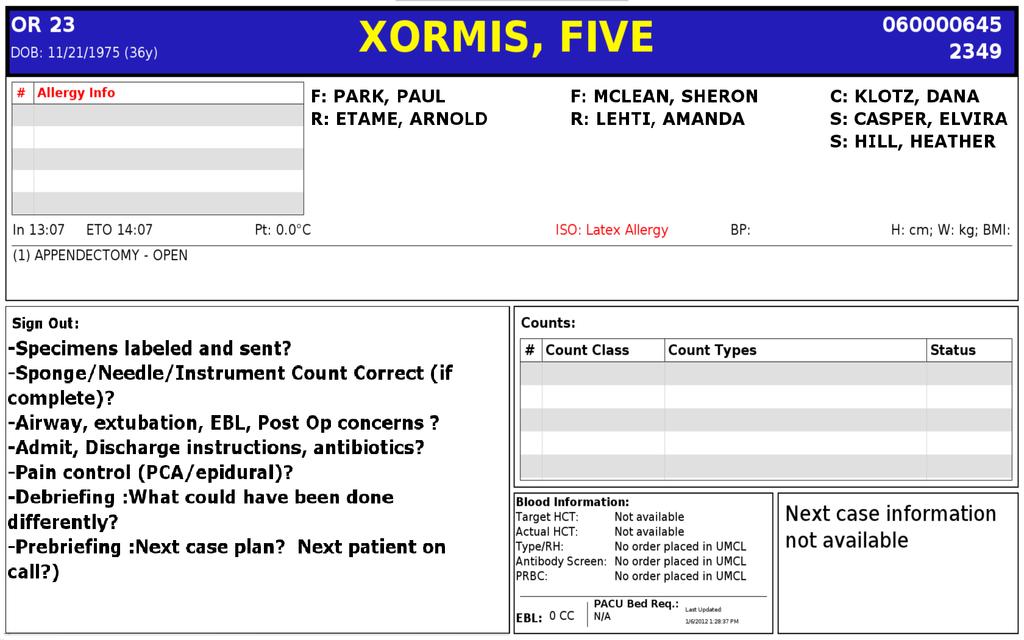
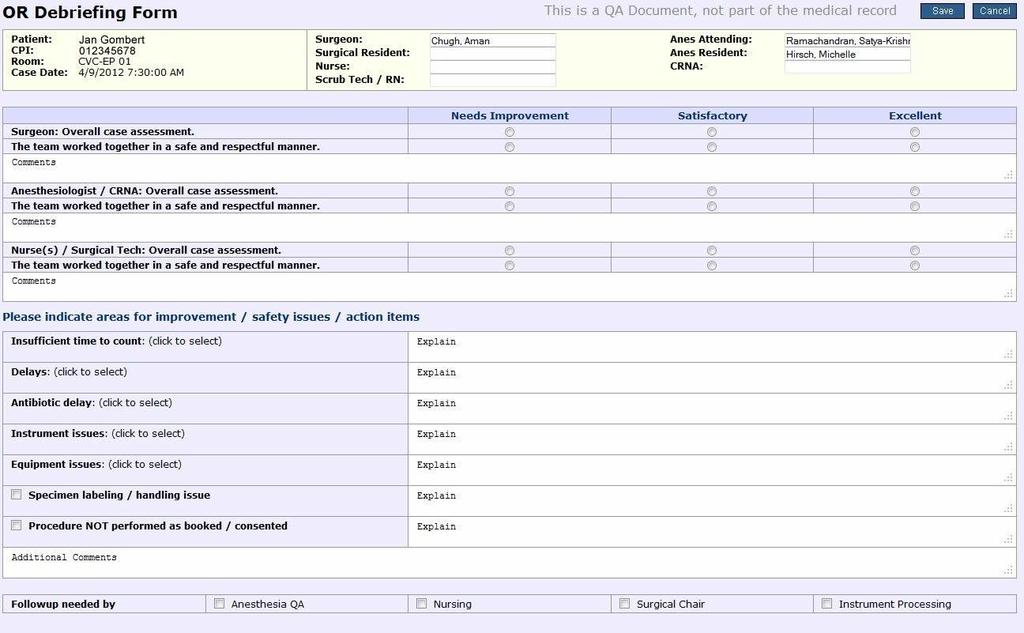
24 Pre-Op Briefing Entire Surgical Team Attending surgeon Anesthesiologist/CRNA Circulator Scrub nurse/tech Resident, PA, perfusionist, others Guided by checklist OR suite prior to anesthetic induction Does not replace pre-op planning Complements the TIMEOUT
25 Supporting Long Term Memory Checklists Put knowledge in the world vs. in the head Recognition is better than recall Tool to Guide and Improve Communication Checklist Philosophy Read and Verify checklists Read and Do checklists

26 Read and Verify
27 Read and Do
 Sharps DISPOSED Site.")
28 Before Insertion IV Insertion Checklist Patient Identification..CONFIRMED Correct Side CONFIRMED Catheter Size..CONFIRMED Equipment AT BEDSIDE Patient..BRIEFED After Insertion Tourniquet REMOVED Line...FLUSHED Pump.SET (with fluids) Sharps DISPOSED Site..LABELED Documentation.COMPLETE

29 Checklist-Driven Preoperative Briefing

30 Checklist-Driven Preoperative Briefing
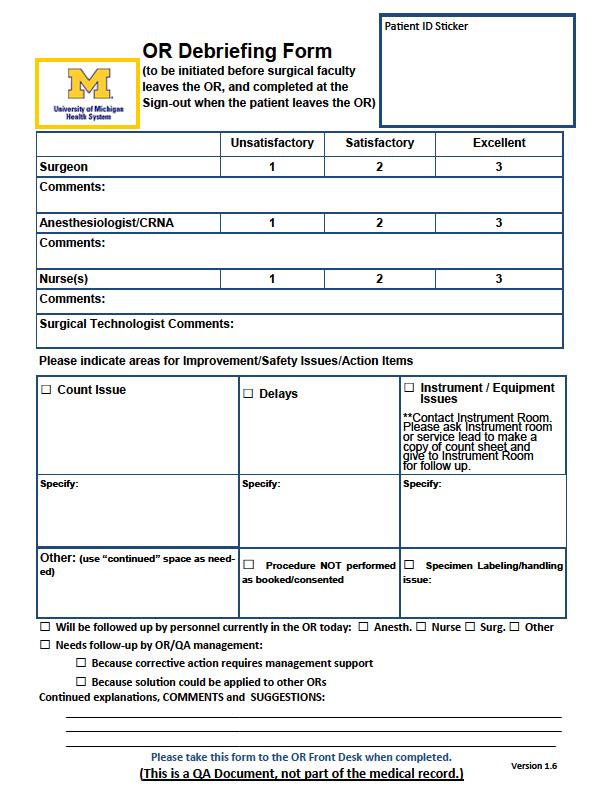
31 Post-op Debriefing Entire Surgical Team Attending surgeon Anesthesiologist/CRNA Circulator Scrub nurse/tech Resident, PA, perfusionist, others Guided by checklist What went well? What did not go well? What can we do to improve our processes? What did we learn? Timing when patient is stable before attending leaves (update prior to patient leaving OR) Method to track debrief items and follow-up: Leadership Group
32
33
34
35 The Checklist is the Tool that Provides the Framework for Communication
36 Communication Techniques Communication techniques Call out/transparent thinking Directed communication Closed-loop communication / Feedback Read back / Repeat back Teamwork, communication protocols Dynamic Skepticism Assertive statements / wording 3 W s, SBAR, 4 steps
37 Dynamic Skepticism Attitude of constantly questioning and evaluating the patient care environment Avoid trusting what appears to be obvious Do not assume! Seek facts Verification is NOT a mistrust of others Questioning and verifying is safe practice
38 Asking the Right Question Any questions? VS What is your biggest concern for today?
39 Clarity Communication should be Specific Direct Concise DO NOT Hint and Hope

40 Hint and Hope Communication Boy that grass is really getting tall out there!


41 Hint and Hope Communication August 2, Fatalities There s Lightning Coming out of that one
42 3 W s 1. What I see 2. What I m concerned about 3. What I want
43 Situation What is the problem? Background Brief background information Assessment SBAR R What is your assessment of the patient? Recommendations What do you recommend? Response Close the loop
44 Assertive Statements Direct and clearly communicated statements that facilitate patient advocacy in decision-making. Not a license to be rude Use I statements, rather than You statements I statements describe your experience rather than another s shortcomings Give people options

45 Assertive Communication Standardized Communication Tools 4 Step Assertive Communication Tool 1. Get Attention - State name/position - Strip away title 2. State concern - Preface with I m uncomfortable 3. Offer Alternative Pose question - to get resolution Assertiveness with Respect

46 When all else fails? Chain of Command



47 STEP BACK Engage Team Use Chain of Command TAKE ACTION 4 Step Assertive Tool 1. Get Attention 2. State Concern I m uncomfortable with 3.Offer Solution 4.Pose Question 3 W s 1. What I see 2. What I m concerned about 3. What I want OR SBARR 1. Specific 2. Direct 3. Concise Avoid Hint and Hope
48 Results


49 ** Are they working in the same OR? Carney, et al, Differences in Nurse and Surgeon Perceptions of Teamwork. AORN J. 2010Jun;91(6):722-9



50 Medical Team Training Safety Attitudes Questionnaire In this clinical area, it is easy to speak up. * * I would feel safe being a patient here. * P < 0.05 paired, Students t-test N = 3138 Questionnaires
51 % Turnover Per Year Nursing Turnover Operating Room 10 P = Pre Post 45 Operating Rooms and 35 Intensive Care Units Pre = 12 Months Prior to Learning Session Post = 12 Months Following Learning Session

52 Leadership Participation Matters
 Team Consensus: Disparity between Physicians and Nurses (Small numbers are be")

53 Diiference between Max and Min response (by role ave.) Team Consensus: Disparity between Physicians and Nurses (Small numbers are be er) disparity 2012 disparity Team Climate Safety Climate Job Sa sfac on Stress Recogni on Percep on of managemnent Working Condi ons SAQ Dimension
54 % consensus Positive Consensus, Before and After MTT 60% 50% 40% 30% PreMTT PostMTT 20% 10% 0% Team Climate Safety Climate Job Satisfaction Stress Recognition Perception of management SAQ Dimension Working Conditions

55 Improved Results after One Year
56 MTT Facility Level Impact 67% High Impact on OR Staff 73% High Impact on OR Patients 69% of OR Teams Improved Teamwork 66% of OR Teams Report Improved Efficiency Eqpt Util (61%), Starts (35%), Duration (19%) Safety Attitudes Questionnaire (SAQ) Significant Improvement (p<0.001): Working Conditions, Perception of Mgmt, Job Satisfaction, Safety Climate, & Teamwork

57 Neily et al. Assoc. Between MTT and Surg Mortality. JAMA. 2010;304(15):
58
59
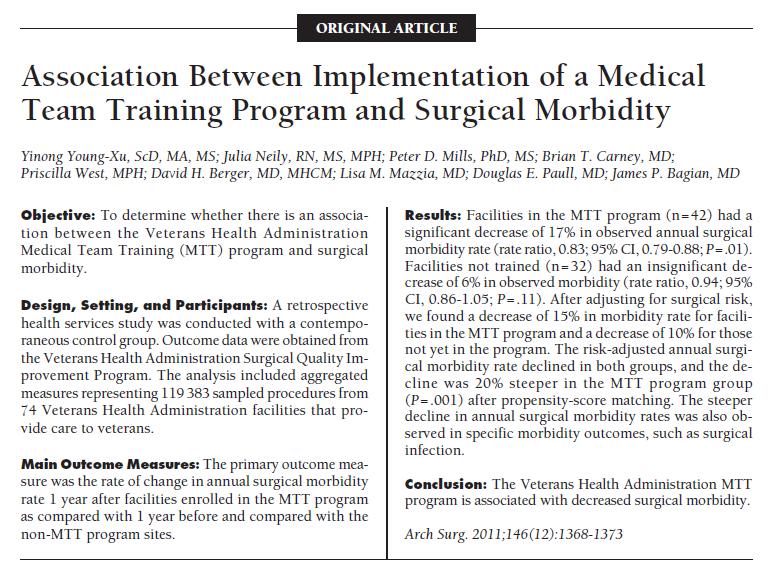
60 MTT Impact - VA N=108; 74 MTT, 34 Control MTT 50% greater decrease in mortality & morbidity than Control, 18% & 17% respectively Dose-response 0.5 deaths/1000 procedures less per quarter p= deaths/1000 procedures per increase in briefing/debriefing p= % reduction in reported OR related harm
61 Debriefings Provide near real-time feedback Must be prepared to handle reports Prioritization Action Feedback must prompt to prevent cynicism The engine for continuous improvement
62
63
64 Obstacles to Performing the Debrief - Summary Transparency and Feedback are the key
65
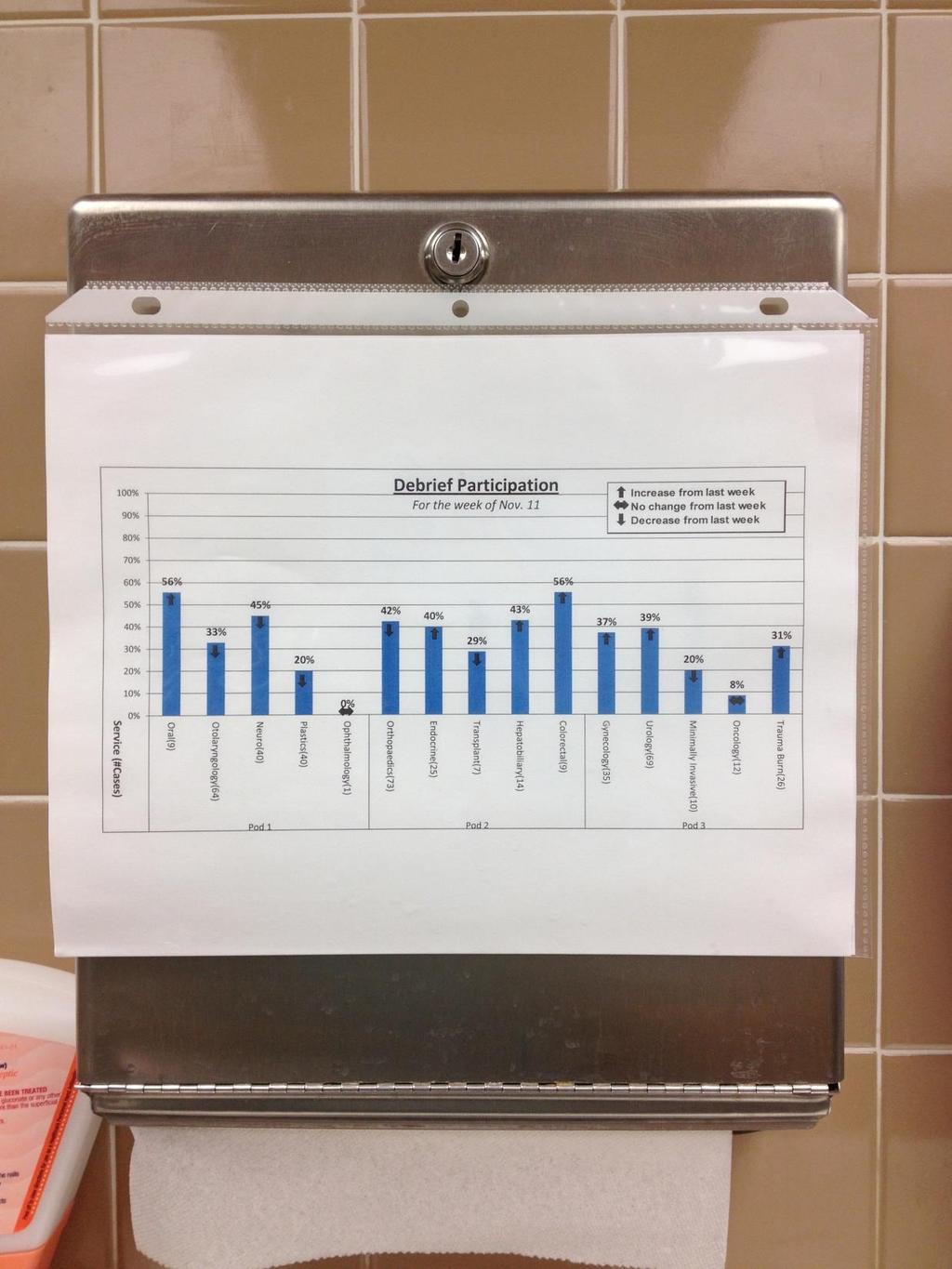
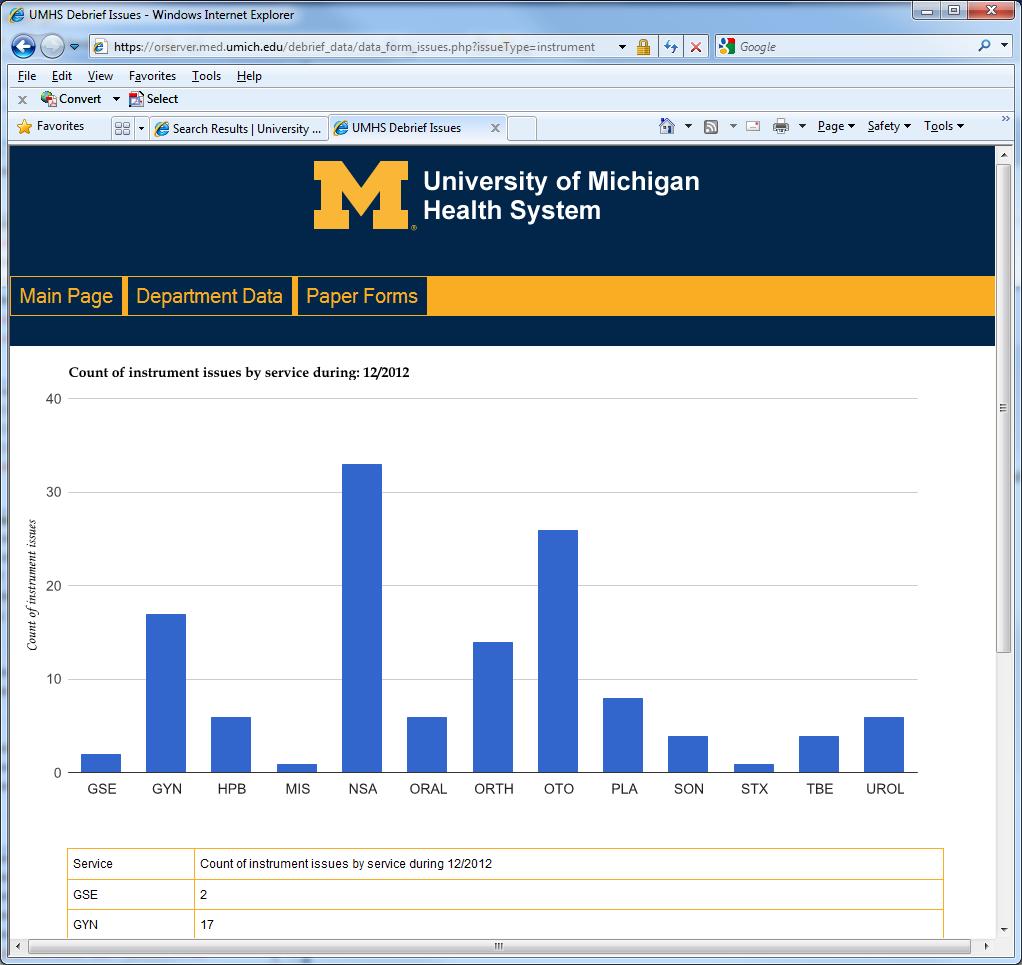
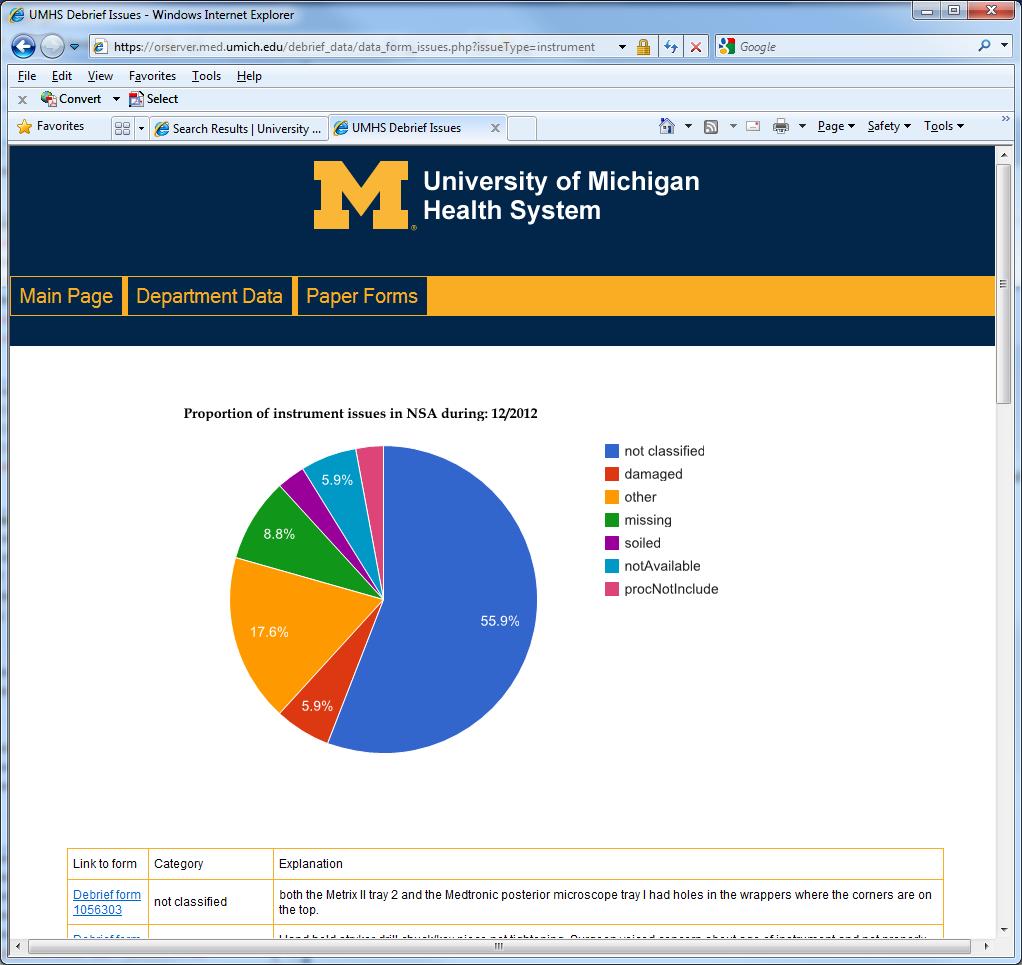
66 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 60% 44% 75% 100% Debrief Participation For the week of Dec % 73% 60% 36% 27% 0% 20% Increase from last week No change from last week Decrease from last week 55% 47% 71% 17% Trauma Burn(12) Oncology(7) Minimally Invasive(15) Urology(11) Gynecology(10) Colorectal(0) Hepatobiliary(5) Transplant(1) Endocrine(11) Orthopaedics(14) Ophthalmology(1) Plastics(26) Neuro(16) Otolaryngology(18) Oral(10) Service (#Cases) Pod 1 Pod 2 Pod 3
67


68

69
70
71
72 Observational Data
73
74
75 MTT Summary Systems Approach Surgical issues must be dealt with in the extended peri-operative period, not solely in the OR Entire System of care must be Examined and Engineered with desired results in mind avoid unintended consequences Team Training start in initial training & sustain More than SBAR Leadership Must Be Involved Checklist-guided briefings and debriefings Can t rely on individuals being careful (vigilant) Compliance Trust But Verify Consequences for Deliberate Non-Compliance
76 Beyond the Operating Room
77

78 Creating a Text here Shared Mental Model Slide Title

79 If patients know what to expect they are more likely to identify and question an unexpected or unplanned event

80 Providers Orders extracted from the electronic medical record Limited to current date Printed for each patient
81 Straightforward Implementation Nurses Review the Daily Plan with patients to: Identify potential errors Explain the day s activity Encourage questions Provide patient education

82 17.6% of the nurses found at least one error as the result of The Daily Plan

83 Improves the patient satisfaction Strengthens communication Provides patient education Facilitates continuity of care
84 Conclusions Need to Provide Recurrent Teamwork Training Not One and Done for OR and Floor Data show that people more likely to be on the on same page post implementation MTT process (Debriefing) highlights issues that need attention Must continue to improve system in place to deal with debrief comments Avoid BLACK HOLE EFFECT Ongoing Process Requires Leadership

85 Resistance Move From: Pro forma Compliance
Addressing Challenges In Pa0ent Safety: Implemen0ng Systems- Based Approaches James P. Bagian, MD, PE
 Addressing Challenges In Pa0ent Safety: Implemen0ng Systems- Based Approaches James P. Bagian, MD, PE Chief Pa)ent Safety and Systems Innova)on Officer Director, Center for Health Engineering & Pa)ent
Addressing Challenges In Pa0ent Safety: Implemen0ng Systems- Based Approaches James P. Bagian, MD, PE Chief Pa)ent Safety and Systems Innova)on Officer Director, Center for Health Engineering & Pa)ent
ORs in facilities that adopted team training had a lower rate of deaths for
 Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Patient safety VA study shows fewer patient deaths after OR team training ORs in facilities that adopted team training had a lower rate of deaths for surgical patients than facilities that had not yet
Teamwork, Communication, Briefing, Checklists, & O.R. Safety
 Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Teamwork, Communication, Briefing, Checklists, & O.R. Safety E. Patchen Dellinger, MD, FACS Professor of Surgery, Chief of General Surgery, Chief of Staff, University of Washington Medical Center (UWMC),
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Crew Resource Management for Trauma Resuscitation. Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation
 Crew Resource Management for Trauma Resuscitation Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation Learning Objectives 1. Review Impact of Errors Aviation Healthcare 2.
Crew Resource Management for Trauma Resuscitation Amy Krichten, MSN, RN, CEN PA Trauma Systems Foundation Director of Accreditation Learning Objectives 1. Review Impact of Errors Aviation Healthcare 2.
ORIGINAL ARTICLE. Incorrect Surgical Procedures Within and Outside of the Operating Room
 ONLINE FIRST ORIGINAL ARTICLE Incorrect Surgical Procedures Within and Outside of the Operating Room A Follow-up Report Julia Neily, RN, MS, MPH; Peter D. Mills, PhD, MS; Noel Eldridge, MS; Brian T. Carney,
ONLINE FIRST ORIGINAL ARTICLE Incorrect Surgical Procedures Within and Outside of the Operating Room A Follow-up Report Julia Neily, RN, MS, MPH; Peter D. Mills, PhD, MS; Noel Eldridge, MS; Brian T. Carney,
Failure Mode and Effects Analysis (FMEA) for the Surgical Patient
 for the Surgical Patient") How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course. Print your Certificate CE s
How to Receive Your CE Credits Read your selected course Completed the quiz at the end of the course with a 70% or greater. Complete the evaluation for your selected course. Print your Certificate CE s
What does safe surgery look like? Jonathan Beard Professor of Surgical Education
 What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
What does safe surgery look like? Jonathan Beard Professor of Surgical Education Incidence of Adverse Events in Healthcare 10-15 % patients* 50% surgical 50% in the operating room 50% preventable Most
Bridging the communication gap in the operating room with medical team training
 The American Journal of Surgery 190 (2005) 770 774 Paper Bridging the communication gap in the operating room with medical team training Samir S. Awad, M.D.*, Shawn P. Fagan, M.D., Charles Bellows, M.D.,
The American Journal of Surgery 190 (2005) 770 774 Paper Bridging the communication gap in the operating room with medical team training Samir S. Awad, M.D.*, Shawn P. Fagan, M.D., Charles Bellows, M.D.,
Development and assessment of a Patient Safety Culture Dr Alice Oborne
 Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Development and assessment of a Patient Safety Culture Dr Alice Oborne Consultant pharmacist safe medication use March 2014 Outline 1.Definitions 2.Concept of a safe culture 3.Assessment of patient safety
Patient Safety in Neurosurgery and Neurology. Andrea Halliday, M.D. Oregon Neurosurgery Specialists
 in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
in Neurosurgery and Neurology Andrea Halliday, M.D. Oregon Neurosurgery Specialists None Disclosures A Routine Operation What human factors contributed to this bad outcome? Halo effect Task fixation Excessive
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Ensuring the Continuum of Interprofessional Education and Collaborative Practice in the Post- Graduate Training Years
 Ensuring the Continuum of Interprofessional Education and Collaborative Practice in the Post- Graduate Training Years Interprofessional Care for the 21 st Century October 11, 2014 Pittsburgh, Pa. Joanne
Ensuring the Continuum of Interprofessional Education and Collaborative Practice in the Post- Graduate Training Years Interprofessional Care for the 21 st Century October 11, 2014 Pittsburgh, Pa. Joanne
3/10/2017. Interprofessional Collaboration, In situ Simulation and TeamSTEPPS : A Practice Improvement Initiative
 Interprofessional Collaboration, In situ Simulation and TeamSTEPPS : A Practice Improvement Initiative Kathleen Poindexter, PhD, RN, CNE; Jennifer Thompson Wood, MSN, RN, ACNS BC; Gayle Lourens, DNP, MS,
Interprofessional Collaboration, In situ Simulation and TeamSTEPPS : A Practice Improvement Initiative Kathleen Poindexter, PhD, RN, CNE; Jennifer Thompson Wood, MSN, RN, ACNS BC; Gayle Lourens, DNP, MS,
Surgery Road Map. General practices. Road map sections
 Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
Surgery Road Map MHA s road maps provide hospitals and health systems with evidence-based recommendations and standards for the development of topic-specific prevention and quality improvement programs,
TeamSTEPPS Introductory Webinar. July 19, 2018
 TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
PATIENT SAFETY IT TAKES A TEAM
 PATIENT SAFETY IT TAKES A TEAM Learning Objectives After studying this learning module I will be able to: Define patient safety. Explain why teamwork is essential to keeping patients safe. Describe tools
PATIENT SAFETY IT TAKES A TEAM Learning Objectives After studying this learning module I will be able to: Define patient safety. Explain why teamwork is essential to keeping patients safe. Describe tools
Unit Based Culture of Safety and Learning. Owensboro Health March, 2017
 Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Unit Based Culture of Safety and Learning Owensboro Health March, 2017 Owensboro Health 477 Bed Regional Hospital 32 Bed ICU 30 Transitional Care Beds Level III Trauma Center Level III NICU Largest employer
Building and Sustaining a Culture of Safety
 Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Assessment of patient safety culture in a rural tertiary health care hospital of Central India
 International Journal of Community Medicine and Public Health Goyal RC et al. Int J Community Med Public Health. 2018 Jul;5(7):2791-2796 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original Research
International Journal of Community Medicine and Public Health Goyal RC et al. Int J Community Med Public Health. 2018 Jul;5(7):2791-2796 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original Research
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Impacting Patient Safety and Patient Satisfaction
 Impacting Patient Safety and Patient Satisfaction Jennifer L. K. Davis, MS, RD Hawaii Dietetic Association May 5, 2011 At the airport.. Objectives Understand HCAHPS and Patient Satisfaction surveys and
Impacting Patient Safety and Patient Satisfaction Jennifer L. K. Davis, MS, RD Hawaii Dietetic Association May 5, 2011 At the airport.. Objectives Understand HCAHPS and Patient Satisfaction surveys and
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment. MEDCOM PS Center
 ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor
 Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Communication and Teamwork for Patient Safety 1.0 Contact Hour Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2008 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
NERC Improving Human Performance
 NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
SURGEONS ATTITUDES TO TEAMWORK AND SAFETY
 SURGEONS ATTITUDES TO TEAMWORK AND SAFETY Steven Yule 1, Rhona Flin 1, Simon Paterson-Brown 2 & Nikki Maran 3 1 Industrial Psychology Research Centre, University of Aberdeen, Aberdeen, Scotland, UK Departments
SURGEONS ATTITUDES TO TEAMWORK AND SAFETY Steven Yule 1, Rhona Flin 1, Simon Paterson-Brown 2 & Nikki Maran 3 1 Industrial Psychology Research Centre, University of Aberdeen, Aberdeen, Scotland, UK Departments
Improving teams in healthcare
 Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery
 Plastic Surgery International Volume 2011, Article ID 579579, 5 pages doi:10.1155/2011/579579 Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery Shady Abdel-Rehim,
Plastic Surgery International Volume 2011, Article ID 579579, 5 pages doi:10.1155/2011/579579 Research Article WHO Surgical Checklist and Its Practical Application in Plastic Surgery Shady Abdel-Rehim,
Using the Just Culture Method. Stacey Thomas, BSN, RNC Risk Analyst
 Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Using the Just Culture Method Stacey Thomas, BSN, RNC Risk Analyst Just Culture A system of Shared Accountability Everyone in the organization is responsible for maintaining a safe and reliable system
Year in Review ro ils RO ILS
 RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
TeamSTEPPS TM. Improving Patient Safety Worldwide Through Teamwork and Communication
 TeamSTEPPS TM Improving Patient Safety Worldwide Through Teamwork and Communication Presenters Susan M Hohenhaus, RN, MA, FAEN President, Hohenhaus & Associates, Inc. Stephen M Powell, MS, Captain, Principal,
TeamSTEPPS TM Improving Patient Safety Worldwide Through Teamwork and Communication Presenters Susan M Hohenhaus, RN, MA, FAEN President, Hohenhaus & Associates, Inc. Stephen M Powell, MS, Captain, Principal,
If you experience any problems, please call Marilyn Nichols at the MOCPS office at , ext 221 or The Basics of CUSP
 Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
EXECUTIVE SUMMARY. The Military Health System. Military Health System Review Final Report August 29, 2014
 EXECUTIVE SUMMARY On May 28, 2014, the Secretary of Defense ordered a comprehensive review of the Military Health System (MHS). The review was directed to assess whether: 1) access to medical care in the
EXECUTIVE SUMMARY On May 28, 2014, the Secretary of Defense ordered a comprehensive review of the Military Health System (MHS). The review was directed to assess whether: 1) access to medical care in the
FACT SHEET. The Launch of the World Alliance For Patient Safety " Please do me no Harm " 27 October 2004 Washington, DC
 FACT SHEET The Launch of the World Alliance For Patient Safety " Please do me no Harm " 27 October 2004 Washington, DC 1. This unique and essential Alliance is set up by the World Health Organization (WHO)
FACT SHEET The Launch of the World Alliance For Patient Safety " Please do me no Harm " 27 October 2004 Washington, DC 1. This unique and essential Alliance is set up by the World Health Organization (WHO)
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Expedition: Improving Safety and Reliability for Surgical Procedures
 These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
These presenters have nothing to disclose Expedition: Improving Safety and Reliability for Surgical Procedures Session 5 William Berry, MD, MPA, MPH, FACS Kathy Duncan, RN January 23, 2014 Expedition Coordinator
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
2. Title Of Initiative Quality Improvement Project
 The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Einstein Medical Center Montgomery 2. Title Of Initiative Quality Improvement Project
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Einstein Medical Center Montgomery 2. Title Of Initiative Quality Improvement Project
Table of Contents. TeamSTEPPS Framework and Competencies Key Principles. Team Structure Multi-Team System For Patient Care
 Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
Table of Contents TeamSTEPPS Framework and Competencies Key Principles Team Structure Multi-Team System For Patient Care Leadership Effective Team Leaders Team Events Brief Checklist Debrief Checklist
TeamSTEPPS TM National Implementation
 TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
Simulation. Turning A Team of EXPERTS Into an EXPERT TEAM! M. Hellen Rodriguez M.D. Jeff Mackenzie R.N.
 Simulation Turning A Team of EXPERTS Into an EXPERT TEAM! M. Hellen Rodriguez M.D. Jeff Mackenzie R.N. Contributors to Maternal M&M from Obstetrical Hemorrhage DELAY IN DIAGNOSIS DELAY IN BLOOD TRANSFUSION
Simulation Turning A Team of EXPERTS Into an EXPERT TEAM! M. Hellen Rodriguez M.D. Jeff Mackenzie R.N. Contributors to Maternal M&M from Obstetrical Hemorrhage DELAY IN DIAGNOSIS DELAY IN BLOOD TRANSFUSION
Effective Perioperative Communication to Enhance Patient Care 1.1
 CONTINUING EDUCATION Effective Perioperative Communication to Enhance Patient Care 1.1 www.aornjournal.org/content/cme J. HUDSON GARRETT, Jr, PhD, MSN, MPH, FNP-BC, CSRN, PLNC, VA-BC, IP-BC, CDONA, FACDONA
CONTINUING EDUCATION Effective Perioperative Communication to Enhance Patient Care 1.1 www.aornjournal.org/content/cme J. HUDSON GARRETT, Jr, PhD, MSN, MPH, FNP-BC, CSRN, PLNC, VA-BC, IP-BC, CDONA, FACDONA
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots
 HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
CRM in USAF Flight and Family Medicine Clinics
 CRM in USAF Flight and Family Medicine Clinics Michael D. Jacobson, DO, MPH Colonel, USAF, MC, SFS USAF School of Aerospace Medicine Wright-Patterson AFB, OH RAM 2013 Distribution A: Approved for public
CRM in USAF Flight and Family Medicine Clinics Michael D. Jacobson, DO, MPH Colonel, USAF, MC, SFS USAF School of Aerospace Medicine Wright-Patterson AFB, OH RAM 2013 Distribution A: Approved for public
Application of Simulation to Improve Clinical Efficiency Systems Integration
 Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES
 A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
A GLOWING RESEMBLANCE A COMPARE AND CONTRAST OF MEDICAL AND NUCLEAR PERFORMANCE IMPROVEMENT INITIATIVES 23 rd Annual HPRCT Conference June 12-15, 2017 Thomas Diller, MD, MMM; Executive Director University
In the middle of the night, a patient arrives with a leaking abdominal aortic
 Clinical management Specialty staff versus generalists: How do ORs strike the balance? In the middle of the night, a patient arrives with a leaking abdominal aortic aneurysm, and the surgeon wants to insert
Clinical management Specialty staff versus generalists: How do ORs strike the balance? In the middle of the night, a patient arrives with a leaking abdominal aortic aneurysm, and the surgeon wants to insert
Creating and Using a Safe Surgery Checklist
 Creating and Using a Safe Surgery Checklist Michelle George, Vice President of Clinical Services Lisa Sinsel, Group Director of Clinical Services Surgical Care Affiliates 1 Agenda 1 2 3 4 5 6 7 Welcome
Creating and Using a Safe Surgery Checklist Michelle George, Vice President of Clinical Services Lisa Sinsel, Group Director of Clinical Services Surgical Care Affiliates 1 Agenda 1 2 3 4 5 6 7 Welcome
The Human Factor: Applying Safety Science in Health Care
 The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
The Human Factor: Applying Safety Science in Health Care Sarah Henrickson Parker, PhD Director of Education and Academic Affairs, Research Scientist National Center for Human Factors Engineering in Healthcare
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers
 Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
Restoring Honesty, Trust and Safety in Healthcare: Educating the Next Generation of Providers Patient Safety and Reducing Your Risk for Malpractice Introductions Timothy McDonald, MD JD Professor, Anesthesiology
The Health Quality & Safety Commission. Research Report. Surgical Culture Safety Survey. Prepared for Health Quality & Safety Commission
 RESEARCH REPORT DECEMBER 2015 The Health Quality & Safety Commission Surgical Culture Safety Survey Research Report Prepared for Health Quality & Safety Commission Prepared by Ltd. 1 1: Executive Summary...
RESEARCH REPORT DECEMBER 2015 The Health Quality & Safety Commission Surgical Culture Safety Survey Research Report Prepared for Health Quality & Safety Commission Prepared by Ltd. 1 1: Executive Summary...
Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians
 Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians Edna Rensing, RN, M.S.H.A., CPHQ This material was prepared by the Virginia Health Quality Center, the Medicare Quality
Staff Perceptions of Patient Safety Appropriate Care To Virginians ACT Virginians Edna Rensing, RN, M.S.H.A., CPHQ This material was prepared by the Virginia Health Quality Center, the Medicare Quality
"Using Simulation to Improve Operating Room Efficiency and Safety"
 "Using Simulation to Improve Operating Room Efficiency and Safety" Phyllis A. Toor RN BSN United States Army Medical Command Nurse Consultant/TeamSTEPPS Program Manager Patient Safety Program 1 Objective
"Using Simulation to Improve Operating Room Efficiency and Safety" Phyllis A. Toor RN BSN United States Army Medical Command Nurse Consultant/TeamSTEPPS Program Manager Patient Safety Program 1 Objective
D espite the awareness that many patients are harmed
 405 ORIGINAL ARTICLE Evaluation of the culture of safety: survey of clinicians and managers in an academic medical center P J Pronovost, B Weast, C G Holzmueller, B J Rosenstein, R P Kidwell, K B Haller,
405 ORIGINAL ARTICLE Evaluation of the culture of safety: survey of clinicians and managers in an academic medical center P J Pronovost, B Weast, C G Holzmueller, B J Rosenstein, R P Kidwell, K B Haller,
Design Principles for Learning and Caring in Patient-Centered Primary Care Homes
 The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
The H.R. Bob Brettell, MD, Memorial Lectureship January 29, 2013 Design Principles for Learning and Caring in Patient-Centered Primary Care Homes Judith L. Bowen, MD, FACP Professor of Medicine Oregon
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A9/B9: Integrating Patient Safety into Your System s DNA
 A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
A9/B9: Integrating Patient Safety into Your System s DNA Doug Bonacum Frank Federico A9 Moderator: Abdulaziz Darwish B9 Moderator: Ibrahim Fawzy Hassan Saturday 26th April A9: 11:00 12:15 B9: 13:30 14:45
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Meeting the Needs of Our Preceptors: Improving Patient Outcomes and Nurse Retention
 Meeting the Needs of Our Preceptors: Improving Patient Outcomes and Nurse Retention Maryland Nurses Association October, 2016 Pamela Shumate, DNP, RN, CCRN, CNE University of Maryland School of Nursing
Meeting the Needs of Our Preceptors: Improving Patient Outcomes and Nurse Retention Maryland Nurses Association October, 2016 Pamela Shumate, DNP, RN, CCRN, CNE University of Maryland School of Nursing
INDEPENDENT ASSESSMENT COMMITTEE REPORT SUMMARY
 INDEPENDENT ASSESSMENT COMMITTEE REPORT SUMMARY Employer: Orillia Soldiers Memorial Hospital, Pre-Admission Clinic and Day Surgery Unit Board: Chair, June Duesburry-Porter; ONA Nominee, Glenda Hubley;
INDEPENDENT ASSESSMENT COMMITTEE REPORT SUMMARY Employer: Orillia Soldiers Memorial Hospital, Pre-Admission Clinic and Day Surgery Unit Board: Chair, June Duesburry-Porter; ONA Nominee, Glenda Hubley;
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Human resources. OR Manager Vol. 29 No. 5 May 2013
 Human resources Second victim rapid-response team helps fellow clinicians recover from trauma One Friday evening at University of Missouri Health System (MUHS) in Columbia, Missouri, Tony*, an RN with
Human resources Second victim rapid-response team helps fellow clinicians recover from trauma One Friday evening at University of Missouri Health System (MUHS) in Columbia, Missouri, Tony*, an RN with
A Study to Assess Patient Safety Culture amongst a Category of Hospital Staff of a Teaching Hospital
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
Communication Among Caregivers
 Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
Communication Among Caregivers October 2015 John E. Sanchez - MS, CPHRM, Pendulum, LLC Amid the incredible advances, discoveries, and technological achievements in healthcare, one element has remained
December 20, Thursday. 7 am. 12 pm. 20 Thursday. December 2012 SuMo TuWe Th Fr Sa 1. January 2013 SuMo TuWe Th Fr Sa
 December 20, 2012 Thursday December 2012 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9101112131415 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 January 2013 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9 10 11 12 13 14
December 20, 2012 Thursday December 2012 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9101112131415 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 January 2013 SuMo TuWe Th Fr Sa 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Patient Safety in Resource Poor Settings
 Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Patient Safety in Resource Poor Settings Global Opportunities (MIT April 8, 2011) Pedro Delgado, Executive Director Institute for Healthcare Improvement www.ihi.org 1 Safe, Timely, Effective, Efficient,
Types of Errors 3/29/12. Approaches of other industries: To err is human, to forgive is divine... Human errors vs. Medical errors vs.
 Medical Errors Management and Early Warning for the Medical Physicist David Hintenlang, Types of Errors Human errors vs. Medical errors vs. Medical events To err is human, to forgive is divine... Approaches
Medical Errors Management and Early Warning for the Medical Physicist David Hintenlang, Types of Errors Human errors vs. Medical errors vs. Medical events To err is human, to forgive is divine... Approaches
Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH. Preparing Graduates for the 21 st Century Health Care System
 Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH Preparing Graduates for the 21 st Century Health Care System Interest in Method and Content: 20 years ago at UCLA -- We observed Students
Osteopathic and Medical Student Education Joseph C. Gambone, DO, MPH Preparing Graduates for the 21 st Century Health Care System Interest in Method and Content: 20 years ago at UCLA -- We observed Students
FLYING WITH DOCTORS: Experiences with the application of 6 techniques from aviation industry in the Rotterdam Eye Hospital
 FLYING WITH DOCTORS: Experiences with the application of 6 techniques from aviation industry in the Rotterdam Eye Hospital Dirk F. de Korne Rotterdam Eye Hospital / Erasmus University Rotterdam PO Box
FLYING WITH DOCTORS: Experiences with the application of 6 techniques from aviation industry in the Rotterdam Eye Hospital Dirk F. de Korne Rotterdam Eye Hospital / Erasmus University Rotterdam PO Box
FY 13 Pillar Goal Update and FY 14 Pillar Goals
 FY 13 Pillar Goal Update and FY 14 Pillar Goals Summer Leadership Assembly C. Wright Pinson, MD, MBA Deputy Vice Chancellor, Health Affairs CEO, Vanderbilt Health System June 19, 2013 Staying Focused on
FY 13 Pillar Goal Update and FY 14 Pillar Goals Summer Leadership Assembly C. Wright Pinson, MD, MBA Deputy Vice Chancellor, Health Affairs CEO, Vanderbilt Health System June 19, 2013 Staying Focused on
How do we know the surgical checklist is making a meaningful. impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010
 How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
How do we know the surgical checklist is making a meaningful impact in surgical care? Virginia Flintoft, MSc, BN Vancouver, BC March 9, 2010 1 Show Me the Evidence You simply have to MEASURE! 2 Why Measure?
Leroy Edozien. Consultants - Obstetrics & Gynaecology St Mary s Hospital, Manchester, UK
 Leroy Edozien Consultants - Obstetrics & Gynaecology St Mary s Hospital, Manchester, UK Introduction Clinicians fundamental principle: first do no harm 1 in every 10 patients suffers a medical accident
Leroy Edozien Consultants - Obstetrics & Gynaecology St Mary s Hospital, Manchester, UK Introduction Clinicians fundamental principle: first do no harm 1 in every 10 patients suffers a medical accident
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Department of Veterans Affairs VHA Directive Washington, DC March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS
 Department of Veterans Affairs VHA Directive 1103 Veterans Health Administration Transmittal Sheet Washington, DC 20420 March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS 1. REASON FOR ISSUE: This Veterans
Department of Veterans Affairs VHA Directive 1103 Veterans Health Administration Transmittal Sheet Washington, DC 20420 March 5, 2016 PREVENTION OF RETAINED SURGICAL ITEMS 1. REASON FOR ISSUE: This Veterans
Submitted by Alexander Kolker, PhD, Outcomes Operations Project Manager, Children s Hospital of Wisconsin
 Using Advanced Process Simulation Methodology to Plan for a Major Facility Renovation of the Surgical Suite at The Children s Hospital of Wisconsin (CHW) Submitted by Alexander Kolker, PhD, Outcomes Operations
Using Advanced Process Simulation Methodology to Plan for a Major Facility Renovation of the Surgical Suite at The Children s Hospital of Wisconsin (CHW) Submitted by Alexander Kolker, PhD, Outcomes Operations
Quality Patient Safety. Quality Patient Safety Lessons from other Industries. Lessons Learned from other Industries
 Lessons from other Industries Or making others best practices yours! Dr. Ken Green Commander, US Navy 202-762-3032 Kenneth.green2@med.navy.mil Personal background: Commander, United States Navy Current
Lessons from other Industries Or making others best practices yours! Dr. Ken Green Commander, US Navy 202-762-3032 Kenneth.green2@med.navy.mil Personal background: Commander, United States Navy Current
From Value to High-Reliability Organization
 From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital
 Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
Associate Professor Jennifer Weller University of Auckland Specialist Anaesthetist, Auckland City Hospital A doctor tends to a mortally ill child in Sir Luke Fildes s 1891 painting The Doctor. The Rise
TASCS 2017 Annual Conference 3/2/2017
 Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
Center for the Future of Surgery
 Center for the Future of Surgery Center for the Future of Surgery 9500 Gilman Drive, La Jolla, CA 92093 858.246.1004 cfs.ucsd.edu Redefining Surgery At UC San Diego Center for the Future of Surgery, our
Center for the Future of Surgery Center for the Future of Surgery 9500 Gilman Drive, La Jolla, CA 92093 858.246.1004 cfs.ucsd.edu Redefining Surgery At UC San Diego Center for the Future of Surgery, our
Overcoming the Culture of Silence
 Overcoming the Culture of Silence Why Your Staff Won't Speak Up, Why You Should Care, and What You Can Do About It Capt. Stephen W. Harden Disclosures of Conflicts of Interest Steve Harden has nothing
Overcoming the Culture of Silence Why Your Staff Won't Speak Up, Why You Should Care, and What You Can Do About It Capt. Stephen W. Harden Disclosures of Conflicts of Interest Steve Harden has nothing
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Understanding the Causes of Events. Objectives
 Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
Introduction to Root Cause Analysis (RCA) Understanding the Causes of Events HSAG Pressure Ulcer Collaborative August 19, 2009 Andrea B. Silvey, PhD, MSN HSAG Chief Quality Improvement Officer 1 Objectives
IHI Expedition. Engaging Frontline Teams to Create a Culture of Safety. March 28 th, Annette Bartley, RN, MS, MPH Tracy Jacobs, BSN, RN
 March 28 th, 2013 These presenters have nothing to disclose IHI Expedition Engaging Frontline Teams to Create a Culture of Safety Annette Bartley, RN, MS, MPH Tracy Jacobs, BSN, RN Today s Host 2 Lizzie
March 28 th, 2013 These presenters have nothing to disclose IHI Expedition Engaging Frontline Teams to Create a Culture of Safety Annette Bartley, RN, MS, MPH Tracy Jacobs, BSN, RN Today s Host 2 Lizzie
The New York Model: Root Cause Analysis Driving Patient Safety Initiative to Ensure Correct Surgical and Invasive Procedures
 The New York Model: Root Cause Analysis Driving Patient Safety Initiative to Ensure Correct Surgical and Invasive Procedures Lawrence L. Faltz, MD, FACP; John N. Morley, MD, FACP; Ellen Flink, MBA; Peg
The New York Model: Root Cause Analysis Driving Patient Safety Initiative to Ensure Correct Surgical and Invasive Procedures Lawrence L. Faltz, MD, FACP; John N. Morley, MD, FACP; Ellen Flink, MBA; Peg
Communication Challenges Overcoming the Barriers to Improve Quality. Presented by: Christy Brinkman LNHA Laura Seleen RN
 Communication Challenges Overcoming the Barriers to Improve Quality Presented by: Christy Brinkman LNHA Laura Seleen RN 6-16-16 Objectives The participant will be able to identify a process to follow to
Communication Challenges Overcoming the Barriers to Improve Quality Presented by: Christy Brinkman LNHA Laura Seleen RN 6-16-16 Objectives The participant will be able to identify a process to follow to
Why Focus on Perioperative Services?
 1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
General OR-Stanford-CA-1 revised: Tuesday, February 02, 2016
 Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Stanford University Anesthesiology Residency Program Rotation specific goals and objectives for residents Core Curriculum for PGY 1 Surgery Residents on the Anesthesia Rotation Description: The General
Doctor in the Cockpit
 Doctor in the Cockpit Diffusion of aviation innovations in hospitals Dirk F. de Korne, PhD MSc Deputy Director, Health Innovation Assistant Professor, Health Services Management & Organisation Singapore
Doctor in the Cockpit Diffusion of aviation innovations in hospitals Dirk F. de Korne, PhD MSc Deputy Director, Health Innovation Assistant Professor, Health Services Management & Organisation Singapore
Re-Engineering Medication Processes to Capitalize on Technology. Jane Englebright, PhD, RN Vice President, Quality HCA
 Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Re-Engineering Medication Processes to Capitalize on Technology Jane Englebright, PhD, RN Vice President, Quality HCA Who is HCA? % % % % U.K. % % % Switzerland % %% % % % % % %% % % % % % % % %% % % %
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety