Right Care Right Place Right Time
|
|
|
- Buck Richardson
- 5 years ago
- Views:
Transcription

1 System Level Measures Right Care Right Place Right Time M15 I have nothing to disclose Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati, Ohio James Anderson Center for IHI 26 th National um December 7, 2015 Health Care Delivery System Transformation Strategic Improvement Priorities and System Level Measures 2 ACCESS FLOW PATIENT SAFETY CLINICAL EXCELLENCE REDUCE HASSLES TEAM WELLBEING FAMILY CENTERED CARE 3 rd Next available appointment % of eligible patients with delays Discharge Prediction and Execution Growth Prediction Adverse drug events (ADE) per 1,000 doses Nosocomial infection rates: Bloodstream infection rate Surgical site infection rate infection rates: VAP Safe Practices Serious Safety Events Codes outside the ICU rate/1000 days Standardized PICU Mortality Ratio Expected/ Actual % use of Evidence- Based Care for eligible patients Functional Health Status Touch Time for Providers Employee Satisfaction Staffing Effectiveness Staff Physician Satisfaction Voluntary staff turnover rate Accident rate for staff with Work days lost Overall Rating: Patient Experience Functional Health Status Risk Adjusted Cost per Discharge 1
 and frequently operating above a system stressing census of 485 (90%")


2 January February March April May June July August September October November December # of Days # of Days Challenges of Growth Operating Above Optimal Occupancy We are increasingly operating above optimal census of 460 (85% occupancy) and frequently operating above a system stressing census of 485 (90% occupancy) * System Census Days between 85-90% Occupancy System Census Days > 90% Occupancy What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver the Correct Therapy / Treatment Outcomes Prevent Complications or Errors in Care Deliver Safe Care regardless of the Inherent Risks Safety Get Me Home, Keep me at Home Respect my needs Give me my Money s Worth Patient / Family Experience Value This is all FLOW management it is essential for SAFETY, PATIENT / FAMILY EXPERIENCE and QUALITY DELIVERY 2
3 Flow is a Safety Initiative Prediction Framework for Safety Getting the Rights Right Right Diagnosis and Treatment Right Patient in Right Bed Location Right Nursing Staff and Staffing Expertise Disease Specific Expertise Equipment Expertise Best Care Model Requires ability to Predict future needs, and manage present capacity control variability Operations Management techniques to understand and manage variability are the key to success Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor 3
4 JUL AUG SEP OCT NOV DEC JAN FEB MAR APR MAY JUN # of Patients with a New Failure Critical Flow Failure Recognition Critical Patient Flow Failures by Month Month of Fiscal Year Last Update: 9/14/2015 by M. Ponti-Zins, for Data Source: MPS 4
5 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, GARDiANS Decrease overutilization of hospital services Optimize patient placement to insure the right care, in the right place, at the right time Increase clinician and staff satisfaction Demonstrate a ROI for the systems moving to bundled payment arrangements Shape or Reduce Demand Match Capacity and Demand Redesign the System IHI Theory on Flow Outcomes Primary Drivers Secondary Drivers Specific Change Ideas Relocate care in ICUs in accordance with patients EOL wishes Relocate care in Med/Surg Units to community-based care settings Relocate low-acuity care in EDs to community-based care settings Decrease demand for hospital beds through delivering appropriate care Decrease demand for hospital beds by reducing hospital acquired conditions Decrease variation in surgical scheduling Oversight system for hospital-wide operations to optimize patient flow Real-time demand and capacity management processes Flex capacity to meet hourly, daily and seasonal variations in demand Early recognition for high census and surge planning Improve efficiencies and throughput in the OR, ED, ICUs and Med/Surg Units Service Line Optimization (frail elders, SNF residents, stroke patients, etc.) Reducing unnecessary variations in care James and managing M. Anderson LOS outliers Center 1. Proactive advanced illness planning 2. Development of palliative care programs (hospital-based and community-based) 3. Reduce readmissions for high risk populations 4. Extended hours in primary care practices 5. Urgent Care and Retail Clinics 6. Enroll patients in community-based mental health services 7. Paramedics & EMTs triaging & treating patients at home 8. Greater use of clinical pathways and evidence-based medicine 9. Care management for vulnerable/high risk patient populations 10. Decrease complications/harm (HAPU, CAUTI, SSI, falls with harm) and subsequent LOS 11. Redesign surgical schedules to create an predictable flow of patients to downstream ICUs and inpatient units 1. Assess seasonal variations and changes in demand patterns and proactively plan for variations 2. Daily flow planning huddles (improve predictions to synchronize admissions, discharges and discharges) 3. Real-time demand and capacity problem-solving (managing constraints and bottlenecks) 4. Planning capacity to meet predicted demand patterns 5. High census protocols to expedite admissions from the ED and manage surgical schedules. 1. Redesign surgical schedules to improve throughput and to improve smooth flow of patients to downstream ICUs and inpatient units 2. Separate scheduled and unscheduled flows in the OR 3. ED efficiency changes to decrease LOS 4. Decrease LOS in ICUs (timely consults, tests and procedures) 5. Decrease LOS on Med/Surg Units (case management for patients with complex medical and social needs) 6. Advance planning for transfers to community-based care settings 7. Cooperative agreements with rehab facilities, SNFs and nursing homes 5
6 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, GARDiANS Evidence Based Care 12 Evidence Based Care Guidelines serve as an interface between rapidly evolving scientific information and busy clinical practices Developed by Inter-disciplinary teams experts Implementation Awareness of recommendation to facilitate change Easy access to the Evidence Feedback on Outcomes Feedback on further improvements Culture of Improvement / Evidence Based Care 6
 52% decrease Chest X Ray 14% Decrease Respiratory Therapies 17% decrease, repeat Tx - 28% decrease")
7 Bronchiolitis 13 Population Infants 1 year or younger with bronchiolitis 3 years control data vs. 3 years post implementation Results Admissions 30% decrease LOS 17% decrease Nasal Washings (RSV) 52% decrease Chest X Ray 14% Decrease Respiratory Therapies 17% decrease, repeat Tx - 28% decrease Net Cost Reduction Total Costs 14% decrease Respiratory care services 72% decrease Re-Admissions No change Perlstein PH et al. Arch Pediatr Adolesc Med 2000; 154: Muething S et al. J Pediatr 2004;144: Cytomegalovirus Prophylaxis 14 75% Decrease in CMV infection liver/intestine transplants Decreased IV-IGG expense Liver - Intestine Danziger-Isakov, Lara et al. CCHMC Integrated Solid Organ Transplant 7





8 Yearly SSI Patients - CCHMC 774 SSI s 9 Years 387 SSI s Prevented 337 SSI s Yearly SSI Patients - CCHMC Case Average 10 days LOS $27, Business Case 3870 days LOS $10.5 million 774 SSI s 9 Years 387 SSI s Prevented 337 SSI s Sparling KW, RyckmanFC, Schoettker PJ et al. Qual Manag Health Care Jul-Sep;16(3): Financial impact of failing to prevent surgical site infection 8


9 Standardization for Outcomes Merging Evidence and Practice Focus on Excellence SSI Spines SSI Accomplishments Baseline rate: 4.4 SSIs/100 procedures, Current Rate: 1.7 SSIs/100 procedures 60% reduction Overall SPS - Estimated 3,699 fewer children harmed Since October $79 million in health care costs saved Toltzis P, O Riordan M, Cunningham DJ, Ryckman FC, Bracke TM, Olivea J, Lyren A. A statewide collaborative to reduce pediatric surgical site infections. Pediatrics :


10 Inflammatory Bowel Disease Remission rate (PGA, Centers >75% registered) 71 Care Centers >19,500 patients >575 physicians >35% of all IBD patients Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, GARDiANS 10

11 Surgical Streams of Care Urgent / Emergent Surgery Predictable and Measurable Natural Variation Possible to Model Can be managed within the System with resource allocation Delay Increased risk and worse outcomes Elective Surgery Unpredictable Whim of Surgical Schedule High variability over time Delay Case specific risk Initial Design around Urgent Needs Goal No urgent cases in Block Time Allocate Block for Urgent Needs Traditional Block Reactive System Urgent Emergent Cases placed within Block Time as needed Elective Case Plan disrupted, prolonged waiting time for elective patients Inefficient (Unsafe) Access for Urgent Cases Push complex Elective Cases into the late hours Overtime Wrong Team in OR Not Ideal 11
12 Scheduling Guidelines A to E Acute Life and Death Emergencies A < 30 Minutes Airway emergency(upper airway obstruction) Cardiac surgery postop bleeding with tamponade Cardiorespiratory decompensation (severe) Liver transplant postoperative emergency Malrotation with volvulus Massive bleeding Mediastinal injury Multiple Trauma-unstable or O.R. resuscitation Neurosurgical condition w/imminent herniation Emergent, but not immediately life threatening B < 2 Hours Acute shunt malfunction Acute spinal cord compression Bladder rupture Bowel perforation, traumatic Cardiac congenital emergencies w/hemodynamic or pulmonary instabilities Compartment syndrome Donor harvest ECMO cannulation Ectopic pregnancy Embolization for acute hemorrhage Esophageal atresia with tracheoesophageal fistula Gastroschisis/omphalocele Heart, heart/lung, lung, liver and intestinal transplants Incarcerated hernias Intestinal obstruction with suspected vascular compromise Intussusception-irreducible Ischemic limb/cold extremity (compromised arterial flow) Liver/Multivisceral/SI Transplant (when organ available) Liver transplant with suspected thrombosis Newborn bowel obstruction Open globe Orbital abscess Pacemaker insertion for complete heart block Replant fingers Replant hand or arm Spontaneous abortion GUIDELINES FOR SURGICAL CASE GROUPING DIAGNOSES/PROCEDURES (guideline only: medical judgment required) Revised Master Urgent C < 4 Hours Abscess with sepsis Airway (non-urgent diagnostic L&B, flex bronch, non-symptomatic foreign body) Appendicitis-with sepsis/rapid progression Biliary obstruction non-drainable Cardiac ventricular assist device placement Cerebral angiogram for intracranial hemorrhage Chest tube placement in patient w/unstable vital signs, increased work of breathing and decreased O2 saturation Contaminated Wounds-Multiple Trauma Diagnostic/therapeutic airway intervention Hepatic angiogram w/suspected vascular thrombus Hip Dislocation Intestinal Obstruction-no suspected vascular compromise Kidney transplant (ORGAN AVAILABLE) Liver laparotomy Massive soft tissue injury Nephrostomy tube placement in patient w/sepsis Obstructed kidney (stones) with sepsis Older child with bowel obstruction PICC placement where patient has no access but needs fluids/medications urgently Progressive shunt malfunction Traumatic dislocation-hip Unstable neurosurgical condition Semi-Urgent D < 8 Hours Abscess drainage Appendicitis-stable/elective Caustic ingestion Chest tube in patient w/stable vital signs Chronic airway foreign bodies Closure abdomen-liver transplant Coarctation repair in newborn Esophageal foreign body without airway symptoms GJ tube/nj tube placement with no other nutrition access Hematuria with clot retention I & D abscess Health without Systems septicemia Excellence Joint aspiration or bone biopsy prior to starting antibiotic therapy Kidney transplant (ORGAN NOT YET AVAILABLE) Add-on case to elective schedule E < 24 Hours Needs to be done that day, but does not require the manipulation of the elective schedule, pyloromyotomy Broviac Closed reduction Eyelid/canalicular lacerations Facial nerve decompression Femoral neck fracture Liver biopsy Mastoidectomy Open fracture grade I/II Open reduction of fracture PICC placement-has other IV access Retinopathy of prematurity treatment Unstable slipped capital femoral epiphysis Options from Simulation # Cases Included # Rooms Average Waiting Times (minutes) Probability 1 Or More Rooms Will Be Available Utilization Rate Recommendations/Considerations 1 A, B, C, D, missing treated as B 1 A: 45 B + missing: 53 C: 72 D: % 40% NOT RECOMMENDED Mean wait for A cases would exceed stated limit 2 A, B, C, missing treated as B 1 A: 21 B + missing: 24 C: 30 76% 24% NOT RECOMMENDED Low utilization rate 3 A, B, C (No missing ) 1 A: 17 B: 19 C: 22 81% 19% NOT RECOMMENDED Low utilization rate Ignores missing cases 4 A E, divided; missing treated as D 2 rooms: 1 room for A- C, 1 room for D,E, & missing A: 18 B: 19 C: 24 D + missing: 70 E: 162 A C room: 80% D E room: 43% A C room: 20% D E room: 57% NOT RECOMMENDED Low utilization rate in A C room Some cases with missing urgency codes may be more urgent than D 5 A E together; missing treated as B 2 rooms that would take any A E case A: 7 B + missing: 8 C + D: 9 E: 17 83% 42%, each room RECOMMENDED Very good waiting times (Wait for A cases would exceed stated limit about 1X/112 weekdays (21.4 weeks )) Treats missing cases conservatively Highest utilization rate Not very sensitive to small increases in case duration or case volume 12

13 Block with Urgent Access Assured Predictive system Urgent Cases in Defined Rooms with Scheduled Teams Resources needed can be modeled Care based on Urgency / Medical Need B-E Case Access - % Successful OR Renovation 1 Add-On Room Closed 13
 1.27 (27%) Medium 304.74 82 (28%) 3.72 (37%) Long 302.56 31 (11%) 9.76 (36%) Grand Total 831.78 290 2.")
14 A Case Access Times Target 30 Minutes ICU Bed Availability ICU Scheduling Category Case Statistics by Category Total PICU Days Case Count ALOS Short (61%) 1.27 (27%) Medium (28%) 3.72 (37%) Long (11%) 9.76 (36%) Grand Total

15 # of Patients with a New Failure 7/16/2008 9/14/ /13/2008 1/12/2009 3/13/2009 5/12/2009 7/11/2009 9/9/ /8/2009 1/7/2010 3/8/2010 5/7/2010 7/6/2010 9/4/ /3/2010 1/2/2011 3/3/2011 5/2/2011 7/1/2011 8/30/ /29/ /28/2011 2/26/2012 4/26/2012 6/25/2012 8/24/ /23/ /22/2012 2/20/2013 4/21/2013 6/20/2013 8/19/ /18/ /17/2013 2/15/2014 4/16/2014 6/15/2014 8/14/ /13/ /12/2014 2/10/2015 4/11/2015 6/10/2015 8/9/2015 '14/1 '14/4 '14/7 '14/10 '15/1 '15/4 '15/7 '15/10 # of Delays 7/16/ /14/2008 1/12/2009 4/12/2009 7/11/ /9/2009 1/7/2010 4/7/2010 7/6/ /4/2010 1/2/2011 4/2/2011 7/1/2011 9/29/ /28/2011 3/27/2012 6/25/2012 9/23/ /22/2012 3/22/2013 6/20/2013 9/18/ /17/2013 3/17/2014 6/15/2014 9/13/ /12/2014 3/12/2015 6/10/2015 9/8/2015 7/16/ /14/2008 1/12/2009 4/12/2009 7/11/ /9/2009 1/7/2010 4/7/2010 7/6/ /4/2010 1/2/2011 4/2/2011 7/1/2011 9/29/ /28/2011 3/27/2012 6/25/2012 9/23/ /22/2012 3/22/2013 6/20/2013 9/18/ /17/2013 3/17/2014 6/15/2014 9/13/ /12/2014 3/12/2015 6/10/2015 9/8/2015 # of Patients with a New Failure # of Patients with a New Failure ICU Admission Model Elective Cases Short Stay Cases Access Cap # Cases on Schedule / Day Long Stay Cases Fixed # Beds Critical Flow Failures 30 Delayed or Canceled Surgery Due to Bed Capacity PICU Bed Not Available for Urgent Use Daily Failures Patients who Utilize an ICU bed b/c an Appropriate Bed is Not 9 Available Daily Failures OR Delays Due to Bed Availability 15
16 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, GARDiANS Discharge Prediction P32 Various approaches to Discharge Management 1980 s Keep it a Secret 1990 s 2000 s Discharge goals Reactive AM before 11 > 30-40% Shift goals 4 hour time block goals with prediction of window Not Patient Centered Prediction Discharge when Medically Ready 16


17 Discharge when Medically Ready Criteria based entirely on completion of necessary treatment plan Discharge criteria are determined on admission by treating physician / service Standardization of criteria for all common treatment protocols All Hospital Medicine Pediatrics Surgery Gen, ENT, Orthopedics, Cardiac Develop mechanism to execute Timeline for DC when Medically Ready Admission to Floor Discharge Criteria Set Treatment Protocol Followed Discharge Criteria Met Nurse Notifies Staff 2 Hrs Discharge Home Re-Adm & LOS Tracked Standardized Criteria Buy-In by Staff Standardized Protocols for most Tx Evaluation Criteria Modify Rounding Clear Discharge Criteria Communication Family Criteria established at admission Nurse at bedside notifies service when Medical discharge criteria are met Discharge from floor in < 2 hours Review Length of Stay and Re-Admissions as balancing measures Not about Speed Now about Efficiency 17

18 Discharge When Medically Ready Karen Tucker, Angela Statile, Diane Herzog, and Christy White Increase percentage of all HM patients who have met* Medically ready criteria who will be discharged within two hours of reaching that goal* on A6S, A6N, LA1W from 75%to 80% by June 30, 2014 Productivity: Optimize use of facilities and staff and improve patient flow to achieve 20% greater utilization of existing assets by June 30, 2015 Criteria for Medically Ready Defined at Admission Shared Ownership/ Accountability and Buy- In Among Physicians and Nurses Communication regarding prediction of discharge and defined goals is ongoing through the hospital stay Potential Barriers to Discharge are Clearly Articulated and Mitigation Plans Established Performance by team is transparent Evidence of Preoccupation with Failure Clear expectations for Parents/ Families Agreement among HM attendings and nursing staff of discharge criteria for order set diagnoses and general admissions (LOR 2) 1) 8 pm Huddle discussion re: early discharges (LOR 2) 2) 0630 notification of patients ready for discharge (LOR 1) Performance Management (LOR 1) Standardized and modifiable order sets (LOR 2) Identify and Mitigate Plans: 1) Transportation- census based (LOR 1) 2) Pharmacy- priority fills (LOR 2), Outpt delivery to patient room (LOR 1) 3) Consults- proactive evaluation (LOR 2) 4) RT- process in PICU (LOR 1) 5) Home Health Care Daily Feedback reports to RNs and MD s with ID and mitigation of process and outcome measure failures (LOR 2) Feedback of data by HM team In conference room and by (LOR 1) Auto notification to resident team that patient has met all criteria (LOR 2) Discharge when Physiologically Ready P36 18


19 Average Length of Stay (Days) Balancing Measures Length of Stay Hospital Medicine Average Length of Stay patients with selected diagnosis Unit 1 Unit 2 Unit 3 All FY11 FY13 Balancing Measures Readmission Rate 19
20 Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, GARDiANS Prediction Model for the Future Static Analytics Performing a ONE TIME analysis of processes with historical data in order to PREDICT what s going to happen under certain circumstances. Critical Care Bed Modeling for Growth Real Time Analytics Performing ONGOING analysis of processes with latest available data in order to continuously PREDICT what s going to happen under certain circumstances. RN Bedside Nurse Staffing Model 20



21 Critical Care Bed Predictions Discrete Event Simulation Variable Input Growth, Length of Stay, Readmissions What if scenarios Sample Output Probability of Full Unit Models future status Allows for Safety Considerations Construct right size units 21

22 ecasted Bed Needs Advantages of Efficiency Estimated number of beds required for given probability of the unit being full. ecast Time Frame Probability of Full Unit PICU Beds CICU Beds ICU Bed Needs Combined ICUs Estimated Savings Year 2 10% % % % Year 5 10% % % % Year7 10% % % % POPULATION: Unscheduled Medical/Surgical, BMT, ENT Airway ICU Elective Cases, Heart Institute Patients Real World Impact of Business Analytics Bed demand predictions facilitate staffing and overflow planning right patient right team ED admit predictions improved from 40% to 70% accuracy resource allocation Encourages staff to more consistently predict and document estimated discharge date, which helps guide care system efficiency Uncovers scheduling issues efficiency and access One-stop source to determine where there is capacity (or lack thereof) to add services (infusions, etc.) efficiency and utilization 22
 Outpatient (Clinical, Testing, Radiology,")

23 Environmental Impact Assessments Predict program demand on current institutional capacity and resources Utilize simulation modeling and data analytics to project future capacity needs in the areas of: Inpatient beds (ICU, Step-down/Floor) Outpatient (Clinical, Testing, Radiology, Therapy, Bronchoscopy) Other (OR resources, pharmacy, blood products, lab) Understanding Capacity Needs & Variability for New/Growth Programs Utilize information from historic data, subject matter experts, market analysis, and outside sources to develop model that predicts future resource demands. 23
24 Quantify Model Results for Analysis & Planning Number of beds needed based on probability of having a full unit (5%, 2%, 1%, 0%) and the growth estimate. 1 Yr Low/Conservative Mid-Range/Most Likely High/Aggressive Growth 3 Yr 5 Yr 7 Yr 10 Yr 1 Yr 3 Yr 5 Yr 7 Yr 10 Yr 1 Yr 3 Yr 5 Yr 5% % % % Outpatient Clinic Needs Clinics/Week Year Year Year Year Year Yr 10 Yr Key Drivers for Capacity Management IHI Drivers CCHMC Initiative Operations Possibilities Shape / Reduce Demand Predictable Care Delivery Management of Variability Evidence Based Best Practices, Analysis of ALOS and outliers, Standardize then Customize, Eliminate unnecessary care Identify Patient Streams Inpatient/Outpatient/OR Manage System Variation D/C Match Optimization of Flow Delivery Capacity Prediction Placement initiatives D:C Matching plans Discharge prediction and planning, Home Care, Parent Initiatives Integration of simulation modeling and planning Environmental Impact Reports for growth programs System Re-Design Capacity Management Flow:Safety Matching Simulation for design and patient placement Environments Impact Planning Flow Failure Analysis, GARDiANS 24


25 Staffing Prediction Proactive Planning Data to Front Line Leaders Updated daily Right Staff for the Right Patients Correct Number and Competency Flexible with Changing Environment Prediction of Needs Be Prepared Be Resilient 25

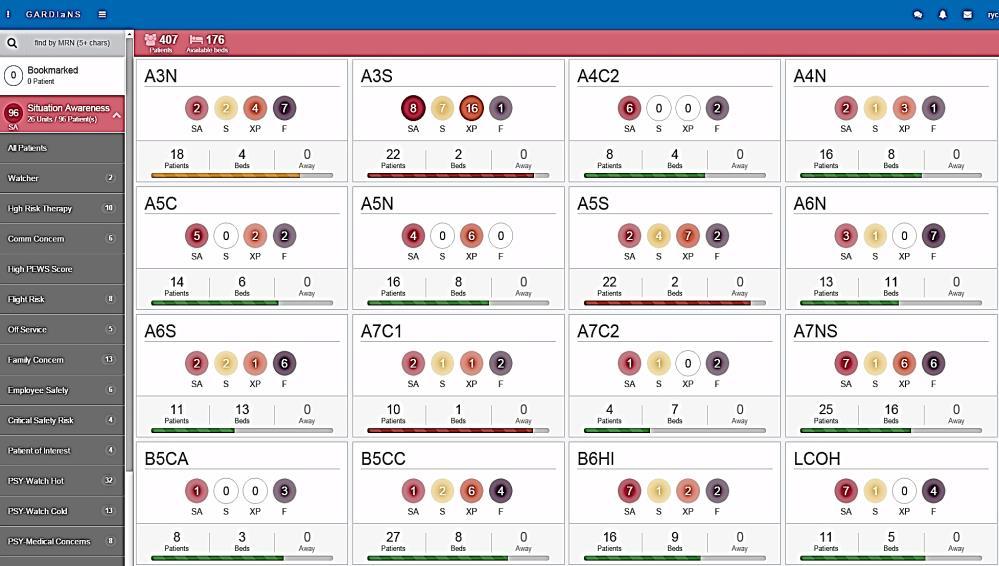
26 GARDiANS GARDiANS 26

27 Hospital Wide System for Safety 3 Times - Every Day Individual Room / Floor / System Predictions Capacity and Safety Floor Huddles PeriOp Huddle Outpt, Home, Psych ED Huddle ICU Huddles Institutional Wide Bed Huddle Capacity Management Pharmacy Pt. Transport Facilities Institutional Daily Operations Brief System Prediction Mitigation Strategy Security Housekeeping P.F.E. Operations and Prediction Meeting (Weekly) COO, RN Leadership, In-Chiefs, Sr. VP s, Safety Director, ED Director Make it Personal Don t let the Data Drown out the Dream Stories not Statistics Names and Faces Accountability is Personal & Group Responsibility Collective Mission/Vision Cincinnati Children s Hospital Medical Center
 35,000 patient per year Great American Ballpark Paul Brown")


28 Patient Satisfaction Only 3-4% of 1 Million outpatient visitors rank our care in the lower half (0-6 of 10 pts) 35,000 patient per year Great American Ballpark Paul Brown Stadium 42,319 65,535 Lessons Learned Building Will to work on Flow is a challenge When it works, it is not on anyone s radar If it works for me, it is not my problem. When I does not work, it is someone else s problem Linkage Safety and Flow Speed vs Efficiency Work Backwards not just ward Embrace Mathematics and Analytics Standardize processes and work flows 28

29 Thanks! 29
Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand
 This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
Hospital Flow Case Study: Cincinnati Children s Hospital
 Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Why Do Flow? The Cincinnati Children s Hospital Journey. December 11, 2017
 December 11, 2017 Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation - Retired Sr. Vice President Medical Operations Cincinnati Children
December 11, 2017 Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation - Retired Sr. Vice President Medical Operations Cincinnati Children
Why Do Flow? The Cincinnati Children s Hospital Journey
 Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation Retired; Sr. Vice President Medical Operations, Cincinnati Children s Hospital, University
Why Do Flow? The Cincinnati Children s Hospital Journey Frederick C. Ryckman, MD Professor of Surgery / Transplantation Retired; Sr. Vice President Medical Operations, Cincinnati Children s Hospital, University
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Matching Capacity and Demand:
 We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
Waits, delays, and cancellations have become so common. Chapter6
 Chapter6 Cincinnati Children s Hospital Medical Center: Redesigning Perioperative Flow Using Operations Management Tools to Improve Access and Safety Frederick C. Ryckman, M.D.; Elena Adler, M.D.; Amy
Chapter6 Cincinnati Children s Hospital Medical Center: Redesigning Perioperative Flow Using Operations Management Tools to Improve Access and Safety Frederick C. Ryckman, M.D.; Elena Adler, M.D.; Amy
Using Quality Improvement to Optimize Pediatric Discharge Efficiency
 This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time
 This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Pat Rutherford Hospital Flow Professional Development
This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Pat Rutherford Hospital Flow Professional Development
4/12/2016. High Reliability and Microsystem Stress. We have no financial, professional or personal conflict of interest to disclose.
 High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time
 This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Hospital Flow Professional Development Program
This presenter has nothing to disclose Strategies to Achieve System- Wide Hospital Flow: Delivering the Right Care, in the Right Place, at the Right Time Hospital Flow Professional Development Program
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core
 Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Relational Coordination: An Imperative Influencing our Capacity to Reach the Core Linda Q. Everett, PhD, RN, NEA-BC, FAAN Executive Vice President & Chief Nurse Executive Indiana University Health 12/7/2012
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Value model in the new healthcare paradigm: Producing value at a single specialty center.
 Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Value model in the new healthcare paradigm: Producing value at a single specialty center. State of Spine Surgery Think Tank June 17, 2017 Catherine MacLean, MD, PhD Chief Value Medical Officer Center for
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo. Session ID: 325
 Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance
 Directorate for Health Workforce and Performance") Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems NPSS Asheville, NC
 Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Optimizing the clinical role of the ACP in Trauma Gena Brawley, ACNP Carolinas Healthcare Systems 2017 NPSS Asheville, NC Objectives Discuss the role of the Critical Care Nurse Practitioner in Trauma Identify
Healthcare Reform Hospital Perspective
 Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
MEASURING POST ACUTE CARE OUTCOMES IN SNFS. David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015
 MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
Trauma Rotation UMASS Memorial University Campus
 Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Trauma Rotation UMASS Memorial University Campus * The following objectives include goals and achievements set forth for successful completion in the acute surgery & trauma rotation such that residents
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
DEPARTMENT OF SURGERY DIVISION OF ACUTE CARE SURGERY ACUTE CARE SURGERY ROTATION (SA1 & SA2)
") DEPARTMENT OF SURGERY DIVISION OF ACUTE CARE SURGERY ACUTE CARE SURGERY ROTATION (SA1 & SA2) University Hospital C.S. Mott Children s Hospital Von Voigtlander Women s Hospital Cardiovascular Center House
DEPARTMENT OF SURGERY DIVISION OF ACUTE CARE SURGERY ACUTE CARE SURGERY ROTATION (SA1 & SA2) University Hospital C.S. Mott Children s Hospital Von Voigtlander Women s Hospital Cardiovascular Center House
ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY)
") July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
July 2011 ROTATION: TRAUMA AND CRITICAL CARE (L AND A SURGERY) ROTATION DIRECTOR: Areti Tillou, M.D. CHIEF OF TRAUMA SURGERY: Henry G. Cryer, M.D. SITE: RRUMC GOALS AND OBJECTIVES: To provide trainees
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Scoring Methodology FALL 2017
 Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
CAMDEN CLARK MEDICAL CENTER:
 INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
CLABSI Prevention Hardwiring Improvement
 CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
EMERGENCY CARE SYSTEMS
 OVERVIEW Emergency and Trauma Care Systems The DCP emergency components of essential packages WHO Emergency Care System Framework Emergency Care System Assessment Tool PREVENTION PREHOSPITAL & TRANSPORT
OVERVIEW Emergency and Trauma Care Systems The DCP emergency components of essential packages WHO Emergency Care System Framework Emergency Care System Assessment Tool PREVENTION PREHOSPITAL & TRANSPORT
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Benchmarking and Key Metrics Utilized by HSCT Administrators. Clint Divine, MBA, MSM Administrative Director, BMT
 Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
Benchmarking and Key Metrics Utilized by HSCT Administrators Clint Divine, MBA, MSM Administrative Director, BMT 1 When you ve seen one HSCT program, you ve seen one HSCT program Although, there are many
Pediatric Surgery Curriculum Clinical Base Year
 Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
Pediatric Surgery Curriculum Clinical Base Year Collaborating Faculty: Cindi Graves, MD Residency Program Director Department of Surgery Purpose and Educational Value The purpose of the Pediatric Surgery
Course: Acute Trauma Care Course Number SUR 1905 (1615)
") Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
Course: Acute Trauma Care Course Number SUR 1905 (1615) Department: Faculty Coordinator: Surgery Dr. Joseph P. Minei Hospital: Periods Offered: Length: Parkland Health & Hospital System All year 4 weeks
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Disclosure of Proprietary Interest
 HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
Pediatric Surgery Elective PL-2 Residents
 PL-2 Residents The is available to senior residents in either a 2 or 4 week block rotation. The experience will include performing inpatient consultations, attending outpatient clinics and observing surgeries
PL-2 Residents The is available to senior residents in either a 2 or 4 week block rotation. The experience will include performing inpatient consultations, attending outpatient clinics and observing surgeries
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Trauma. Level 2. This resident can lead a to recognize common. This resident can. accurately diagnose. team that cares for traumatic conditions and
 Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
Page 1 of 7 Trauma Subject Name Status Employer Program Rotation Evaluation Dates Evaluated by: Evaluator Name Status Employer Program 1 (Trauma) Patient Care: Ward Care This resident is not able lead
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
IX. CINCINNATI CHILDREN S HOSPITAL MEDICAL CENTER (Case study, work in progress) Patricia McGlinchey, Kathleen Kerwin Fuda
 Patricia McGlinchey, Kathleen Kerwin Fuda") 176 IX. CINCINNATI CHILDREN S HOSPITAL MEDICAL CENTER (Case study, work in progress) Patricia McGlinchey, Kathleen Kerwin Fuda Summary: In 2005, the leadership the Cincinnati Children's Hospital Medical
176 IX. CINCINNATI CHILDREN S HOSPITAL MEDICAL CENTER (Case study, work in progress) Patricia McGlinchey, Kathleen Kerwin Fuda Summary: In 2005, the leadership the Cincinnati Children's Hospital Medical
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF GENERAL and PEDIATRIC SURGERY I. The Clinical Mission of the Division of Pediatric Surgery The clinical mission of the Division of Pediatric Surgery at
Sepsis in the NICU and Interventions to Improve Care
 Sepsis in the NICU and Interventions to Improve Care Joseph El Khoury, MD Children s Hospital of Richmond at VCU Virginia Neonatal Perinatal Collaborative Meeting May 12 th, 2017 Significance of Sepsis
Sepsis in the NICU and Interventions to Improve Care Joseph El Khoury, MD Children s Hospital of Richmond at VCU Virginia Neonatal Perinatal Collaborative Meeting May 12 th, 2017 Significance of Sepsis
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Stakeholder input is gathered in several ways. Patients are given the opportunity to provide feedback, the SWOT analysis is based on information from
 Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
Strategic Plan 27 Executive Summary The following is a summary of the information shared in this Operations Review and Plan. This plan highlights operational achievements and challenges, clinical outcomes
Page 347. Avg. Case. Change Length
 Page 345 EP 8 How nurses use trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery Model(s). The development of operational budgets
Page 345 EP 8 How nurses use trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery Model(s). The development of operational budgets
Use of TeleMedicine to Improve Clinical and Financial Outcomes
 Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Select Medical TRANSITIONS OF CARE & CARE COORDINATION
 Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Select Medical TRANSITIONS OF CARE & CARE COORDINATION Agenda Select Medical Overview Transitions of Care Right Patient, Right Level of Care,Right Time Chronic Critical Illness Syndrome Role of Long Term
Hip Today Home Tomorrow:
 Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
Hip Today Home Tomorrow: A Collaborative Effort between an Orthopedic Practice and a Hospital to Create an Innovative Outpatient Total Hip Replacement Program Kimberley Murray RN MS CNS-CNOR Kelly Keenan
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting
 patients from the Acute Care Setting to the Ambulatory Setting") Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting American College of Medical Practice Executives Case Study Submitted by Chantay Lucas,
Transitioning OPAT (Outpatient Antibiotic Therapy) patients from the Acute Care Setting to the Ambulatory Setting American College of Medical Practice Executives Case Study Submitted by Chantay Lucas,
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR.
 Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Duke University Health System Experience of Redesigning Care for Improved Quality and Efficiency CAITLIN DALEY, DR. GEORGE CHEELY, DR. TOM HOPKINS 1 Learning Objectives Describe the Duke University Health
Taming Length of Stay Challenges Through Analytics
 Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs
 Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Medicare P4P -- Medicare Quality Reporting, Incentive and Penalty Programs Presenter: Daniel J. Hettich King & Spalding; Washington, DC dhettich@kslaw.com 1 I. Introduction Evolution of Medicare as a Purchaser
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Penn State Milton S. Hershey Medical Center. Division of Trauma, Acute Care & Critical Care Surgery
 Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Penn State Milton S. Hershey Medical Center Division of Trauma, Acute Care & Critical Care Surgery Residency-Trauma Curriculum The Medical Director for the Penn State Shock Trauma Center is Dr. Heidi Frankel.
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Value Equation for Healthcare
 Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver
Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster.
 Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
Phases of staged response to an increased demand for Paediatric Intensive Care in the event of pandemic or other disaster. Working document The Critical Care Contingency Plan in the event of an emergency
Tell Your Story with a Well- Designed Data Plan. Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System
 Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Integrating Quality Into Your CDI Program: The Case for All-Payer Review
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Pre-operative categorization (triaging) of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency
 of emergency surgical cases. A tool for improving patient care and emergency operating room efficiency") Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
Pre-operative categorization (triaging) of emergency surgical cases A tool for improving patient care and emergency operating room efficiency Introduction No national or provincial guidelines exist for
Mark Stagen Founder/CEO Emerald Health Services
 The Value Proposition of Nurse Staffing September 2011 Mark Stagen Founder/CEO Emerald Health Services Agenda Nurse Staffing Industry Update Improving revenue trends in healthcare staffing 100% Percentage
The Value Proposition of Nurse Staffing September 2011 Mark Stagen Founder/CEO Emerald Health Services Agenda Nurse Staffing Industry Update Improving revenue trends in healthcare staffing 100% Percentage
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
8/31/2015. Session C826 Evidence-Based Staffing Strategies Support Healthy Work-Life Balance Rachael Schweikert, RN Kevin Schwedhelm MSN RN
 Session C826 Evidence-Based Staffing Strategies Support Healthy Work-Life Balance Rachael Schweikert, RN Kevin Schwedhelm MSN RN Nurse Staffing Core vs. Float Staff 30 years ago 20-10 years ago 5 yrs Prior
Session C826 Evidence-Based Staffing Strategies Support Healthy Work-Life Balance Rachael Schweikert, RN Kevin Schwedhelm MSN RN Nurse Staffing Core vs. Float Staff 30 years ago 20-10 years ago 5 yrs Prior
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Diagnostics for Patient Safety and Quality of Care
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve