Use of TeleMedicine to Improve Clinical and Financial Outcomes
|
|
|
- Mervin Leonard
- 5 years ago
- Views:
Transcription
1 Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015
2 Use of TeleMedicine to Improve Clinical and Financial Outcomes Assess your needs and your goals plan your strategy Integrate Tele-Medicine into system-wide strategy Collect accurate data, analyze the data, and share the data to demonstrate successes, drive accountability, and identify opportunities for improvement Listen to your customers (patients and clinicians)
3 Objectives Tele-ICU is a tool to improve quality in the ICU and how it is used depends on the needs of your ICU(s) Tele-ICU is a facilitator of change management as much as an intervention. Identify potential cost savings that can result from successful application of the above tools. It is important to state the goals and define metrics to track whether your use of the tele-icu is delivering added quality Then step back and reassess how you can use tele-icu to further improve the quality of Critical Care at your ICU(s) 3
4 ICU-Telemedicine is care provided to critically ill patients by off-site clinicians using audio, video, and electronic links to leverage technical, informational, and clinical resources. 4
5 Advocate Critical Care 18 ICU s 12 hospitals Five Level 1 Trauma Centers > 6000 physicians > 100 Intensivists 301 Critical Care beds (not including our Outreach programs additional beds) Total = 401 beds emobile carts in the ED Critical Access Unit > 24,000 ICU Admissions in 2014 Ventilator days: 29,706 on 6,419 cases Total direct costs (entire hospital stay) of $367M or 31% Advocate s total direct costs for inpatients in 2014 Total direct costs for days while the patients were treated in the ICU (excluding ED and OR costs) were approximately $200M or 17% of direct costs for inpatients eintensivist and ern coverage 24/7/365 with board-certified critical care physicians Mortality Index (APACHE IV) for 2015= (in 2010 = 0.72) 5
6 IT Culture Strategy 6
7 Target State A patient-focused process enacting evidence-based best practices and standardized protocols provided by one unified critical care team with collaboration at the bedside, among sites, and with the eicu. 7
8 The Goal Improve The Quality of Care We Provide To Our Critical Care Patients and Reduce Costs 8
9 Benefits/ROI/VOI Clinical Reduced mortality LOS Reduce adverse events DVT Sepsis Mortality Ventilator days/vap s CLABSI s Reduce Transfusions Improve nutrition Increase mobility Financial Leapfrog compliant Reduced costs ( avoid harm, fewer complications, VAPs, ADE s, sepsis, cost of 24/7 onsite intensivists.) Reduced LOS Increased Capacity Reduce unnecessary tests, xrays Reduce transfers to higher level facility Other Standardize the delivery of ICU care (workflows and protocols) Leverage scarcity of board-certified intensivists Facilitate Data Reporting Process Flow Variability (Gap) Solutions Avoid sleep deprivation Housestaff training and satisfaction Nurse satisfaction and support of less experienced RN s Patient/family satisfaction Decrease burnout of clinicians Extend Intensivist and critical care nurse career (most experienced) 9
10 Variance in Practice of Tele-ICU Technology Types of ICU s Bedside intensivist staff model Bedside documentation/cpoe availability Remote center staffing patterns Qualifications of providers Hours of Operation Buy-in by bedside clinicians Adherence to best practices Use of quality and safety information Intensivist handover of their patients Community v. Tertiary Facility Teaching v. Non-teaching 10
11 What Does Tele-ICU do to Improve Quality? Disease Management - Acute interventions - Patient surveillance for proactive intervention Population Management Best Practices System Engineering Support Individual Unit Special Needs Process flow variability through gap analysis Education - Resident erounds - Nurse Mentoring 11
12 What Does Tele-ICU do to Improve Quality? Disease Management - Acute interventions - Patient surveillance for proactive intervention Population Management Best Practices System Engineering Support Individual Unit Special Needs Process flow variability through gap analysis Education - Resident erounds - Nurse Mentoring 12
13 What Acute Issues Does Tele-ICU Deal With? First look at all new admissions (seen within 30 minutes) Ventilator issues Arrhythmias, especially atrial fibrillation with rapid ventricular response Hypotension Electrolyte abnormalities X-ray checks requested by residents or nursing MD presence at code, RRT transfer, or before on-site MD arrival Adjustment of sedation Need for GI prophylaxis Ventilator liberation assistance Antibiotic stewardship Glucose management 13
14 Tele ICU Experience Interventions Clinically Significant Intervention Number Percentage Best Practice Adherence % Comprehensive Adm Review % Response to Instability 760 7% Alter Ventilator Settings 723 6% Intervention Prevent Instability 679 6% Alter dx/dx Plan 570 5% Antibiotic Sensitivity Change 556 5% Med Admin 203 2% Direct Life Saving % Lilly J In Care Med 2009
15 What Does Tele-ICU do to Improve Quality? Disease Management - Acute interventions - Patient surveillance for proactive intervention Population Management Best Practices System Engineering Support Individual Unit Special Needs Process flow variability through gap analysis Education - Resident erounds - Nurse Mentoring 15
16 Population Management VAPs prevention DVT prophylaxis CLABSI Prevention Sepsis screen Ventilator liberation Sedation Management CPR Auditing enutrition epharmacy Palliative Care CAUTI Prevention Ventilator Induced Lung Injury (VILI)

17 eicu Report Sheet 17
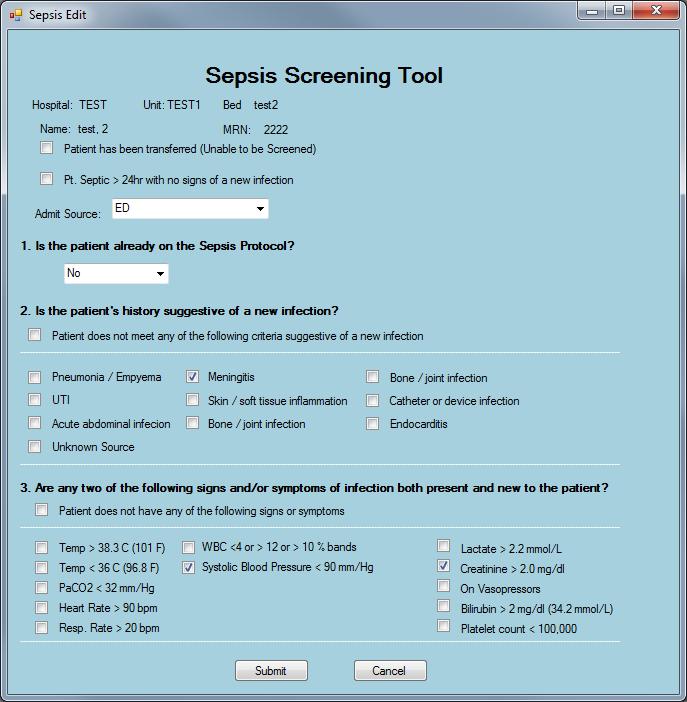
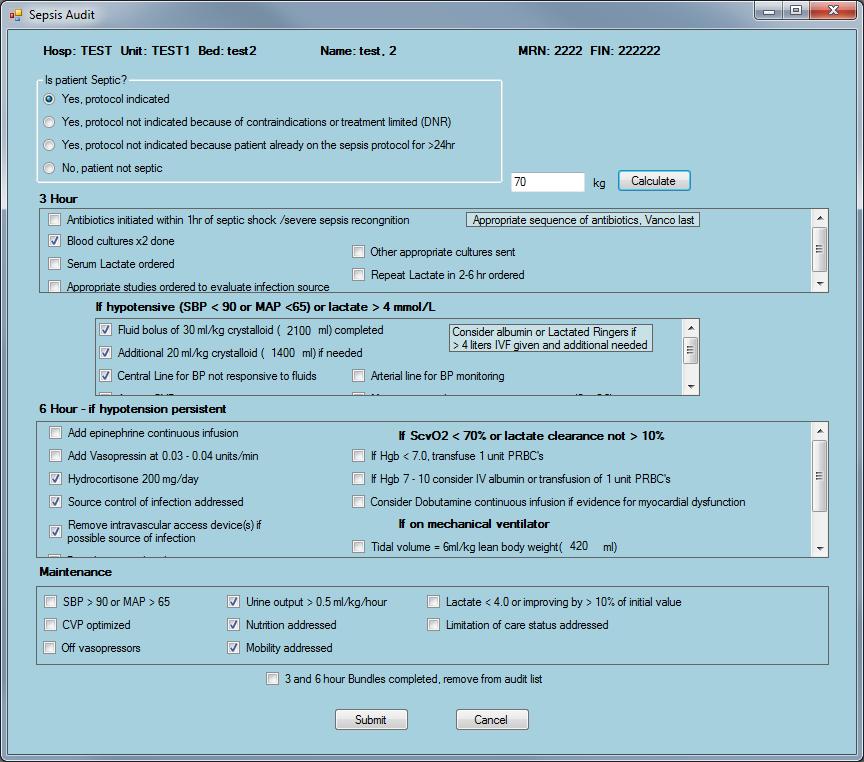
18 18 Ventilator Associated Pneumonia(VAP) Bundle Assessment Screen
19 Proportion Count Percent VAP Compliance CMC MICCU 4Q2011 1Q2012 2Q2012 3Q2012 4Q2012 1Q2013 2Q2013 3Q2013 4Q2013 All ICU Units Vent Days Compliant Vent Bundles % % % % % % % % % Non-Compliant Bundles Non-Compliant for Sedation Vacation Non-Compliant for Assess Extubation Readiness Non-Compliant for GI Bleed Prophylaxis Non-Compliant for DVT Prophylaxis Non-Compliant for HOB30 PM Non-Compliant for HOB30 AM CMC MICCU Vent Days Compliant Vent Bundles 70 96% 74 94% 65 98% 67 93% % % 57 90% % 23 96% Non-Compliant Bundles Non-Compliant for Sedation Vacation Non-Compliant for Assess Extubation Non-Compliant for GI Bleed Prophylaxis Non-Compliant for DVT Prophylaxis Non-Compliant for HOB30 PM Non-Compliant for HOB30 AM VAP compliance (25 months rolling) Components contributing to Non-Compliance in Ventilator Bundle (3 months) 1.0 _ UCL=1 P= LCL= No Non-Compliant items over the last 3 months Sep-09 Nov-09 Jan-10 Mar-10 May-10 Jul-10 4Q 2010 Date 2Q Q Q2012 4Q Q Q Type Sedation Vacation Other Count 1 0 Percent Cum %

20 ICU VAP: Avoided Cost Trend 20 Bethany Hospital excluded from January 2007 forward BroMenn Medical Center included starting in 2010 Sherman Hospital included starting in 2013 Data represents Adult ICU units only
21 DVT Compliance CMC MICCU All ICU Units Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 DVT Days DVT Compliant % % % % % % % % % No prophlaxis Compliant via Contra-indication Type of Prophlaxis Mechanical % % % % % % % % % Pharmicalogical % % % % % % % % % Combined theropy % % % % % % % % % CMC MICCU DVT Days DVT Compliant % % % % % % % % % No prophlaxis Compliant via Contra-indication Type of Prophlaxis Mechanical % % % % % % % % % Pharmacological % % % % % % % % % Combined therapy 46 9% 64 13% 74 14% % 55 10% 55 10% 77 14% 53 11% 42 8% DVT Compliance (25 months rolling) Type of prophlaxis used UCL=1 _ P= LCL= % 90% 80% 70% % 50% 40% 30% 20% Combined therapy Pharmacological Mechanical 0.70 Mar-08 May-08 Jul-08 Sep-08 Nov-08 Jan-09 Mar-09 May-09 Jul-09 Sep-09 Nov-09 Jan-10 Mar-10 10% 0% Dec-09 Jan-10 Feb-10 Mar-10 All ICU Units current month 21
22 22
23 23

24 Sepsis Hospital Mortality Index Target Index not benchmarked by Philips Data reflected is subject to rounding Data Source: APACHE IVa/ 3Q14, 4Q14, 1Q15, 2Q15 Target Index not benchmarked by Philips 2 4
25 What Does Tele-ICU do to Improve Quality? Disease Management - Acute interventions - Patient surveillance for proactive intervention Population Management Best Practices System Engineering Support Individual Unit Special Needs Process flow variability through gap analysis Education - Resident erounds - Nurse Mentoring 25
26 Systems Engineering Define system problems, stakeholders, and goals Prioritize development of a system to meet these goals Use predefined metrics to verify that the completed system is fulfilling stated goals 26
27 Final Target State Guiding Principles Improve Communication/Coordination Achieve System Standardization of Care but with site innovation Creating a Critical Care Team with a strong leader Documentation/Technology Integrate Services (e.g. Pharmacy, PT, Resp Therapy ) Enable the Clinical Staff to care for the patient 27
28 28 Connect the Process to the Outcomes
29 Ventilator Days (Actual/Predicted) System-wide ventilator days were at a ratio of 1.19 to the predicted ventilator days as of 3/31/2012. Achieving a ratio of 1.00 would reduce approx. 4,600 ventilator days. Under the assumption that the excess ventilator days are substituted for a med/surg day, the improvement opportunity saves $3.0 million on an annual basis. Projected savings assume half of opportunity can be achieved in year 1 and the full savings (ratio of 1.00) in year 2. 29
30 KRA Target Overview and Weights 67% Measure Min Target Max Weight ICU Ventilator Days Index Baseline Mid of Min/Max 90th 19.0% CLABSI (ICU) SIR 50th 75th 90th 9.5% CLABSI (non-icu) SIR 50th 75th 90th 9.5% Unassisted Fall Percentile Rank 50th 75th 90th 19.0% 33% Culture of Safety Survey Percentile 50th 75th 90th 10.0% LOS Moderate Mid of Min/Max Well 11.0% CI PHO Score TBD TBD TBD 11.0% Readmissions Rate 50th 63rd 75th 11.0% Lower weight on duplicative measures LOS and readmissions appear in both CI and AdvocateCare index 30
31 Actual/Predicted Mortality Ventilator Day Improvement Summary Health outcomes results: 1938 fewer vent days 3Q13 vs 4Q fewer ICU days 7.4 pts given Sedation Vacation and SBT saves one life Advocate = 828 lives saved Total cost savings: Represents $1.35M* *Savings assumes ICU vent day substituted with Med/Surg Day ICU Mortality APACHE Predicted
32
33

34 ICU CLABSI: Avoided Cost Trend 34 Bethany Hospital excluded from January 2007 forward BroMenn Medical Center included starting in 2010 Sherman Hospital included starting in 2013 Data represents Adult ICU units only
35
36 What Does Tele-ICU do to Improve Quality? Disease Management - Acute interventions - Patient surveillance for proactive intervention Population Management Best Practices System Engineering Support Individual Unit Special Needs Process flow variability through gap analysis Education - Resident erounds - Nurse Mentoring 36
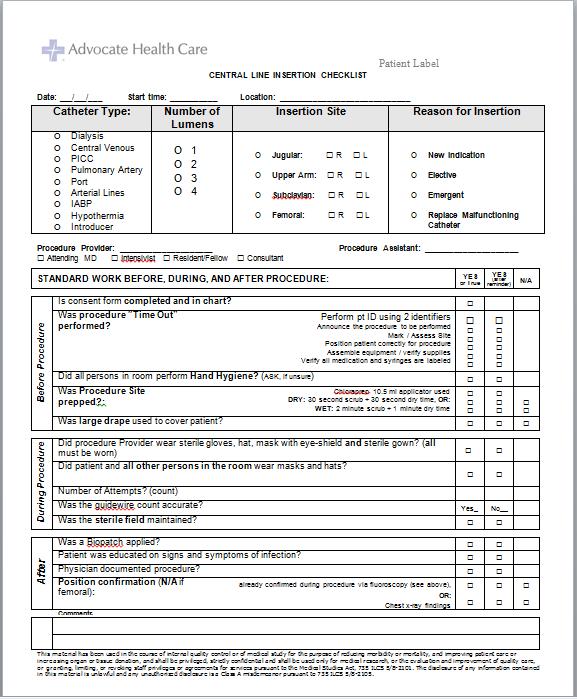
37 Collaboration with Individual Sites on Certain Processes Pneumonia Screening CPR Audit Central Line insertion bundle compliance DVT Intensity of Prophylaxis Tele-Stroke Program Sedation Withdrawal Multidisciplinary Rounds ED Sepsis Management Resident Coverage/Nurse Mentoring enutrition ED Boarders 37
38 Grand Total ED Boarders 2014 Admit to ICU January 6698 February 3130 March April May June July August September October November December Grand Total
39 Patient Safety Story An elderly patient arrived to the ED with severe shortness of breath and O2 sats in the 70 s. She refused intubation and was placed on BiPap. The decision was made to admit the patient and an ICU bed was requested. The ED was informed there were no beds available. While the patient was boarding in the ED, she was not tolerating BiPap and was having runs of V- Tach. The ED physician intubated the patient. The intensivist discussed the case several times with the ED physician, but did not come down to see the patient. Four hours later, the patient was still waiting for an ICU bed. She had continued runs of V-Tach and was given Mag and Amiodarone.
40 Patient Safety Story The patient continued to receive care in the ED, including an EKG. Sixteen hours after the initial bed request, the patient was assigned a bed and report called to the MICCU. A repeat EKG identified a possible STEMI. Serial troponins identified STEMI. Three hours later the patient was taken to the Cath Lab and clinically progressed and was then considered a poor candidate for a CABG. The patient was returned to the ICU. Care was withdrawn and the patient expired.
41 Cause Map e Limited treatment options for cardiac condition Pt admitted to MICCU and holdingin ED No beds available Patients awaiting bed availability to transfer from MICCU. Lack of available beds due to census. Patient Safety Goal Impacted Death Cardiogenic shock Significant myocardial injury Delay in cardiac cath Delay in diagnosing STEMI ED physicians cannot write admit orders Credentials do not allow Patient hemodynamic unstable No admitting orders written on ICU holds in ED. No repeat labs/ekgs ordered No ICU protocols utilized in ED Patient not seen in ED by attending or MICCU docs/residents Intensivist/ Resident from MICCU not involved in patient care in ED MICCU residents work under intensivists who do not see patients before admit to MICCU Too busy with MICCU patients
42 Corrective Action Collaborate with eicu team to identify potential solutions o 4 eicu carts o Create workflow process o Hand off process with ED physician, ED resident, ED RN, Intensivist and eicu MD o First eicu service in an ED with a continuous workflow process
43 ICU patient is ED, ICU bed needed Physician places ICU bed request after Dr. Done ICU Admission Boarding in ED Workflow Patient is admitted as Inpatient status ecare Mobile Cart activated & ealert button pressed by ED RN ED staff enters MRN, Pt Name (Last, First) on monitor eicu Clinician video assesses patient upon notification Hand-over (Follow Communication Workflow) ED Physician or Resident puts in page to initiate 5-way sign-out ED notifies eicu of transfer to MICCU bed by ealert Bed request to Bed Board eicu receives text page from bed board ED notified by bed board that ICU bed not available MICCU bed not available if less than 2 open beds Desk clerk places patient into ICU Virtual Hold Bed ECC5, ECC6, ECC7, ECC8 ED staff notifies eicu of admission Contact info from faxed eicu Assignment Sheet for ED RN 1. Name 2. Patient ID (MRN) 3. Diagnosis 4. Attending Intensivist 5. ED room number 6. Virtual Unit Admit Date/Time eicu HCA admits patient into ecaremanager Verifies lab and trended vital signs Enters height, weight and other data per eicu process eicu Page initiated by resident Call in to Tie-Line for hand-over Intensivist ED Physician RN +/-Attending Resident RN
44 Downgrade, 6 ICU, 20 Downgrade, 8 ICU, 13 Downgrade, 7 ICU, 9 Downgrade, 22 Downgrade, 16 Downgrade, 23 Downgrade, 7 Downgrade, 3 ICU, 7 ICU, 27 ICU, 33 ICU, 31 ICU, 29 Downgrade, 5 Grand Total, 26 Grand Total, 21 Grand Total, 16 Grand Total, 10 ICU, 18 Grand Total, 49 Grand Total, 49 Grand Total, 54 Grand Total, 36 Grand Total, 23 Downgrade, 92 ICU, 169 Grand Total, 261 Monthly emobile Cart Count by Discharge to ICU vs Downgrade /2015 3/2015 4/2015 5/2015 6/2015 7/2015 8/2015 9/ /2015 FEB-OCT

45 Downgrade, 23% Downgrade, 19% Downgrade, 38% Downgrade, 33% Downgrade, 30% Downgrade, 22% Downgrade, 44% Downgrade, 45% Downgrade, 43% Downgrade, 35% ICU, 56% ICU, 55% ICU, 62% ICU, 57% ICU, 67% ICU, 65% ICU, 70% ICU, 77% ICU, 81% ICU, 78% Monthly emobile Cart Percent by Discharge to ICU vs Downgrade 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 2/2015 3/2015 4/2015 5/2015 6/2015 7/2015 8/2015 9/ /2015 FEB-OCT
46 Comparison: 2014 ER to ICU LOS vs 2015 emobile LOS 2014 ER to ICU LOS 2015 emobile LOS Feb Mar Apr May Jun Jul Aug Total 2014 ER to ICU LOS emobile LOS
47 What Does Tele-ICU do to Improve Quality? Disease Management - Acute interventions - Patient surveillance for proactive intervention Population Management Best Practices System Engineering Support Individual Unit Special Needs Process flow variability through gap analysis Education - Resident erounds - Nurse Mentoring 47
48 eicu Associate Satisfaction Trends 100 Percentile Ranking Percentile Ranking Fall 2005 Spring Fall Spring Fall 2007 Spring 2008 Fall 2008 Spring Fall 2009 Spring 2010 Fall 2010 Spring 2011 Fall 2011 Spring 2012 Fall 2012 Spring 2013 Fall
49 Objectives Tele-ICU is a tool to improve quality in the ICU and how it is used depends on the needs of your ICU(s) Tele-ICU is a facilitator of change management as much as an intervention. Identify potential cost savings that can result from successful application of the above tools. It is important to state the goals and define metrics to track whether your use of the tele-icu is delivering added quality Then step back and reassess how you can use tele-icu to further improve the quality of Critical Care at your ICU(s) 49
50 Use of TeleMedicine to Improve Clinical and Financial Outcomes Assess your needs and your goals plan your strategy Integrate Tele-Medicine into system-wide strategy Collect accurate data, analyze the data, and share the data to demonstrate successes, drive accountability, and identify opportunities for improvement Listen to your customers (patients and clinicians)
51 Questions? Thank You! Contact: 51
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Copyright Scottsdale Institute All Rights Reserved.
 Copyright Scottsdale Institute 2018. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s).
Copyright Scottsdale Institute 2018. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s).
Quality Evidence Based Tool: A Multidisciplinary Approach. Monica demariano, RN, MBA JoJo Rapipong, RN
 Quality Evidence Based Tool: A Multidisciplinary Approach Monica demariano, RN, MBA JoJo Rapipong, RN Outline 1) Background 2) Quality Evidence Based Tool (QEBT) 3) Actions/Processes 4) Metrics 5) Data
Quality Evidence Based Tool: A Multidisciplinary Approach Monica demariano, RN, MBA JoJo Rapipong, RN Outline 1) Background 2) Quality Evidence Based Tool (QEBT) 3) Actions/Processes 4) Metrics 5) Data
Wired to Save Lives: A Virtual Hospital Experience
 Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
Wired to Save Lives: A Virtual Hospital Experience Donald J. Kosiak, MD, MBA, FACEP, CPE Vice President for Medical Development Thursday, March 3 rd -- 11:30am Conflict of Interest Donald Kosiak, MD Has
The Digital ICU: Return On Innovation
 The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Two Eyes Are Better Than One
 Two Eyes Are Better Than One Leveraging Telemedicine in the ICU Wendy Deibert, RN, BSN Operations Director, Mercy SafeWatch and Executive Director Telemedicine Services April 18 th, 2012 Agenda Tele-ICU
Two Eyes Are Better Than One Leveraging Telemedicine in the ICU Wendy Deibert, RN, BSN Operations Director, Mercy SafeWatch and Executive Director Telemedicine Services April 18 th, 2012 Agenda Tele-ICU
Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care
 Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care April 29, 2011 Waltham, MA Presented by Lisa Payne Simon, MPH Cheryl H. Dunnington, RN, MS 1 FAST Initiative Overview 2004-2010
Critical Care, Critical Choices: The Case for Tele-ICUs in Intensive Care April 29, 2011 Waltham, MA Presented by Lisa Payne Simon, MPH Cheryl H. Dunnington, RN, MS 1 FAST Initiative Overview 2004-2010
New healthcare delivery models: Interprofessional, regional, international
 New healthcare delivery models: Interprofessional, regional, international Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu Center Timothy G. Buchman PhD, MD, FACS, FCCP, MCCM Founding Director, Emory
New healthcare delivery models: Interprofessional, regional, international Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu Center Timothy G. Buchman PhD, MD, FACS, FCCP, MCCM Founding Director, Emory
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
MUSC Critical Care Outreach Program. Dee W. Ford, MD, MSCR Associate Professor of Medicine
 MUSC Critical Care Outreach Program Dee W. Ford, MD, MSCR Associate Professor of Medicine Disclosures * Funding from the NIH, Department of Defense, and the National Palliative Care Research Center * No
MUSC Critical Care Outreach Program Dee W. Ford, MD, MSCR Associate Professor of Medicine Disclosures * Funding from the NIH, Department of Defense, and the National Palliative Care Research Center * No
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
Celebrating our Successes 2014
 Celebrating our Successes 214 Nurse Involvement in Decision Making Groups 5 CODE SEPSIS: Time from Antibiotic Order to Administration 45 4 Time in Minutes from order to administration 35 3 25 2 15 1 5
Celebrating our Successes 214 Nurse Involvement in Decision Making Groups 5 CODE SEPSIS: Time from Antibiotic Order to Administration 45 4 Time in Minutes from order to administration 35 3 25 2 15 1 5
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Using Telemedicine to Improve Outcomes and Collaboration Within Hospitals and Health Systems
 American Hospital Association Leadership Summit Using Telemedicine to Improve Outcomes and Collaboration Within Hospitals and Health Systems Please note that the views expressed by the conference speakers
American Hospital Association Leadership Summit Using Telemedicine to Improve Outcomes and Collaboration Within Hospitals and Health Systems Please note that the views expressed by the conference speakers
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience. Presented by: Fadwa Jabboury, RN, MSN
 CMC Experience. Presented by: Fadwa Jabboury, RN, MSN") Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
CCU Data Collection with MIDAS+
 May 22 24, 2006 Starr Pass Resort Tucson, Arizona CCU Data Collection with MIDAS+ This session will examine the task of collecting and aggregating CCU data and present the best method for accomplishing
May 22 24, 2006 Starr Pass Resort Tucson, Arizona CCU Data Collection with MIDAS+ This session will examine the task of collecting and aggregating CCU data and present the best method for accomplishing
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Improve the Efficiency and Service of the Emergency Room at North Side Hospital
 Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
Telehealth Integration at Baptist Health South Florida
 Telehealth Integration at Baptist Health South Florida Philip Ludwig, MS, MBA Vice President, Operations Baptist Health South Florida Not-for-profit, community health system 7 acute adult care hospitals
Telehealth Integration at Baptist Health South Florida Philip Ludwig, MS, MBA Vice President, Operations Baptist Health South Florida Not-for-profit, community health system 7 acute adult care hospitals
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT)
") Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Integrating Quality Into Your CDI Program: The Case for All-Payer Review
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Massachusetts ICU Acuity Meeting
 Massachusetts ICU Acuity Meeting Acuity Tool Certification and Reporting Requirements Acuity Tool Certification Template Suggested Guidance Acuity Tool Submission Details Submitting your acuity tool for
Massachusetts ICU Acuity Meeting Acuity Tool Certification and Reporting Requirements Acuity Tool Certification Template Suggested Guidance Acuity Tool Submission Details Submitting your acuity tool for
Key Steps in Creating & Sustaining Excellence
 Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
After reading this learning module, the nurse should be able to:
 After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
Tell Your Story with a Well- Designed Data Plan. Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System
 Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health
 Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
EMR Adoption: Benefits Realization
 EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Catherine Porto, MPA, RHIA, CHP Executive Director HIM. Madelyn Horn Noble 3M HIM Data Analyst
 1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
TeleICU And What It Means To You
 Vanderbilt Department of Anesthesiology TeleICU And What It Means To You Dr. L. Weavind MBBCh Associate Professor Anesthesia and Surgery Director Critical Care Fellowship Vanderbilt University Former Director
Vanderbilt Department of Anesthesiology TeleICU And What It Means To You Dr. L. Weavind MBBCh Associate Professor Anesthesia and Surgery Director Critical Care Fellowship Vanderbilt University Former Director
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
Beyond the Bundle. Improving Ventilator Related Outcomes through Multidisciplinary Collaboration
 Beyond the Bundle Improving Ventilator Related Outcomes through Multidisciplinary Collaboration Definitions VAE Ventilator associated event global term for NHSN reporting criteria VAC: Ventilator Associated
Beyond the Bundle Improving Ventilator Related Outcomes through Multidisciplinary Collaboration Definitions VAE Ventilator associated event global term for NHSN reporting criteria VAC: Ventilator Associated
Our Sepsis Improvement Journey
 A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
The Impact of a Daily Goals Tool in the ICU: More than a Checklist
 S Y S T E M The Impact of a Daily Goals Tool in the ICU: More than a Checklist May 24, 2016 Our Vision To be the Nation's leading public academic health care system. Leading. Teaching. Caring. Acknowledgements
S Y S T E M The Impact of a Daily Goals Tool in the ICU: More than a Checklist May 24, 2016 Our Vision To be the Nation's leading public academic health care system. Leading. Teaching. Caring. Acknowledgements
To Dip or Not To Dip
 To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
To Dip or Not To Dip a patient centred approach to improve the management of UTI in the Care Home environment FIS 30 th November 2017 #ToDipOrNotToDip #FIS17 Elizabeth Beech on behalf of colleagues National
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair
 or Atrial Septal Defect (ASD) Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL
 Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Publication Year: 2008 REASSESSING THE BED COORDINATOR S ROLE SHADY GROVE ADVENTIST HOSPITAL Summary: Creation of Bed Coordinator position to improve patient flow throughout the entire hospital Hospital:
Quality health care in intensive
 Clinical outcomes after telemedicine intensive care unit implementation* Beth Willmitch, RN, BSN; Susan Golembeski, PhD, RN, CHRC; Sandy S. Kim, MA, MEd; Loren D. Nelson, MD, FACS, FCCM; Louis Gidel, MD,
Clinical outcomes after telemedicine intensive care unit implementation* Beth Willmitch, RN, BSN; Susan Golembeski, PhD, RN, CHRC; Sandy S. Kim, MA, MEd; Loren D. Nelson, MD, FACS, FCCM; Louis Gidel, MD,
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Fiscal Year 2014 Final Rule: Updates for LTCHs
 Fiscal Year 2014 Final Rule: Updates for LTCHs Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Mary Dalrymple Managing Director, LTRAX FY14 Final Rule & Impact Objectives Review updates to the FY14
Fiscal Year 2014 Final Rule: Updates for LTCHs Kristen Smith, MHA, PT Senior Consultant, Fleming-AOD Mary Dalrymple Managing Director, LTRAX FY14 Final Rule & Impact Objectives Review updates to the FY14
Healthcare Reform Hospital Perspective
 Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Decreasing Triage to Antibiotic Time for Suspected Sepsis Patients
 Decreasing Triage to Antibiotic Time for Suspected Sepsis Patients Strong Memorial Hospital October/November 2017 Strong Memorial Hospital University of Rochester Medicine Upstate New York Tertiary/quaternary
Decreasing Triage to Antibiotic Time for Suspected Sepsis Patients Strong Memorial Hospital October/November 2017 Strong Memorial Hospital University of Rochester Medicine Upstate New York Tertiary/quaternary
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
CINCINNATI VAMC TELE-ICU PROGRAM MISSION
 VISN 10 Tele- ICU CINCINNATI VAMC TELE-ICU PROGRAM MISSION To care for critically ill Veterans by providing attentive electronic ICU monitoring and consistent uninterrupted management utilizing state of
VISN 10 Tele- ICU CINCINNATI VAMC TELE-ICU PROGRAM MISSION To care for critically ill Veterans by providing attentive electronic ICU monitoring and consistent uninterrupted management utilizing state of
Page 347. Avg. Case. Change Length
 Page 345 EP 8 How nurses use trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery Model(s). The development of operational budgets
Page 345 EP 8 How nurses use trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery Model(s). The development of operational budgets
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
LTCH Lay of the Land: Reporting the LTCH CARE Data Set. July 30, 2012
 LTCH Lay of the Land: Reporting the LTCH CARE Data Set July 30, 2012 Purpose LTCH Quality Reporting Program, specifically the LTCH CARE Data Set CMS guidance, training & transmission Dates & Deadlines
LTCH Lay of the Land: Reporting the LTCH CARE Data Set July 30, 2012 Purpose LTCH Quality Reporting Program, specifically the LTCH CARE Data Set CMS guidance, training & transmission Dates & Deadlines
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals
 Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
SFGH. Management System. Components. SFGH Management System. Improvement. Time. Strategic Planning True North. Value Streams: Rapid Improvement Events
 SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
The Nexus of Quality and Finance
 The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
AirStrip ONE Cardiology
 AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
AirStrip ONE Cardiology A Synchronized View of the Vital Patient Data Needed to Improve Care Heart disease is the leading cause of death in the U.S. The associated costs exceed $100 billion annually. AirStrip
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/11/2016 Contra Costa
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
Seattle Nursing Research Consortium Abstract Style and Reference Guide
 Seattle Nursing Research Consortium Abstract Style and Reference Guide Page 1 SNRC Revised 7/2015 Table of Contents Content Page How to classify your Project. 3 Research Abstract Guidelines 4 Research
Seattle Nursing Research Consortium Abstract Style and Reference Guide Page 1 SNRC Revised 7/2015 Table of Contents Content Page How to classify your Project. 3 Research Abstract Guidelines 4 Research
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY
 MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
MET CALLS IN A METROPOLITAN PRIVATE HOSPITAL: A CROSS SECTIONAL STUDY Joyce Kant, A/Prof Peter Morley, S. Murphy, R. English, L. Umstad Melbourne Private Hospital, University of Melbourne Background /
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Centralizing Multi-Hospital Mortality Reviews
 December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
Countywide Emergency Department Ambulance Patient Transfer of Care Report Performance Report
 Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
Countywide Emergency Department 9-1-1 Ambulance Patient Transfer of Care Report Performance Report Prepared by: Contra Costa Emergency Medical Services Visit us at www.cccems.org 2/28/2017 Patient Transfer
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
1. November RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 12.5%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, December 2013 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. November 2013-2320 RN VACANCY RATE: Overall 2320 RN
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
On the first day of the rotation, please report to the Cardiology Lobby, 5th Floor of the ACC Building, at 8:30 am.
 2018-2019 Catalog Cardiovascular Critical Care - Jacksonville MED E 9J 4th Year Elective Internal Medicine Clinical Science Prerequisites 4th year medical student Course Description This elective involves
2018-2019 Catalog Cardiovascular Critical Care - Jacksonville MED E 9J 4th Year Elective Internal Medicine Clinical Science Prerequisites 4th year medical student Course Description This elective involves
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
The Leapfrog Hospital Survey Scoring Algorithms. Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey
 The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital