Using Quality Improvement to Optimize Pediatric Discharge Efficiency
|
|
|
- Job Rice
- 5 years ago
- Views:
Transcription

1 This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital Cincinnati, Ohio November 2, 2016 James Anderson Center for Health Systems Excellence
2 Objectives Describe strategies for focusing discharge planning processes around medical readiness criteria, regardless of time of day Describe the application of quality improvement principles to improving discharge efficiency Highlight the key high reliability processes used for implementing and sustaining improvement
3 Case At 8am, a 3 year old female admitted with community acquired pneumonia has been stable on room air all night without respiratory distress Afebrile x 24 hours Tolerates her first oral antibiotic dose Drinking well

4 But Why does she stay until 1:00pm? Can we eliminate this waste?
5 Background The Institute of Medicine urges us to provide care that is timely and efficient A 2009 study by Srivastava et al found that nearly 1 in 4 patients experienced a medically unnecessary prolonged hospital stay of at least 1 day Prior studies focused on set discharge time goals such as 11:00 am
6 Background at Cincinnati Children s Hospital Medical Center (CCHMC) In 2012, there were 7000 admissions to our 3 Hospital Medicine units Highest admitting units from Emergency Department and Pediatric Intensive Care Unit Thus, Hospital Medicine discharge delays affect flow throughout the hospital which may lead to Delayed admissions or transfers Canceled or delayed surgeries
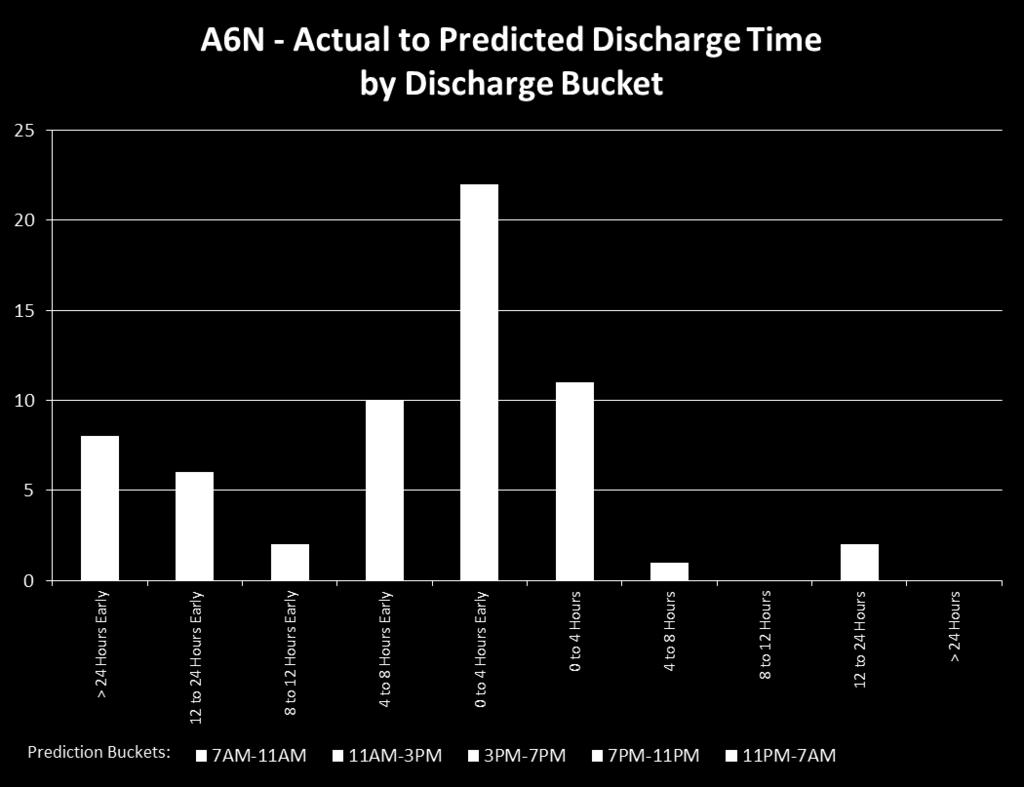
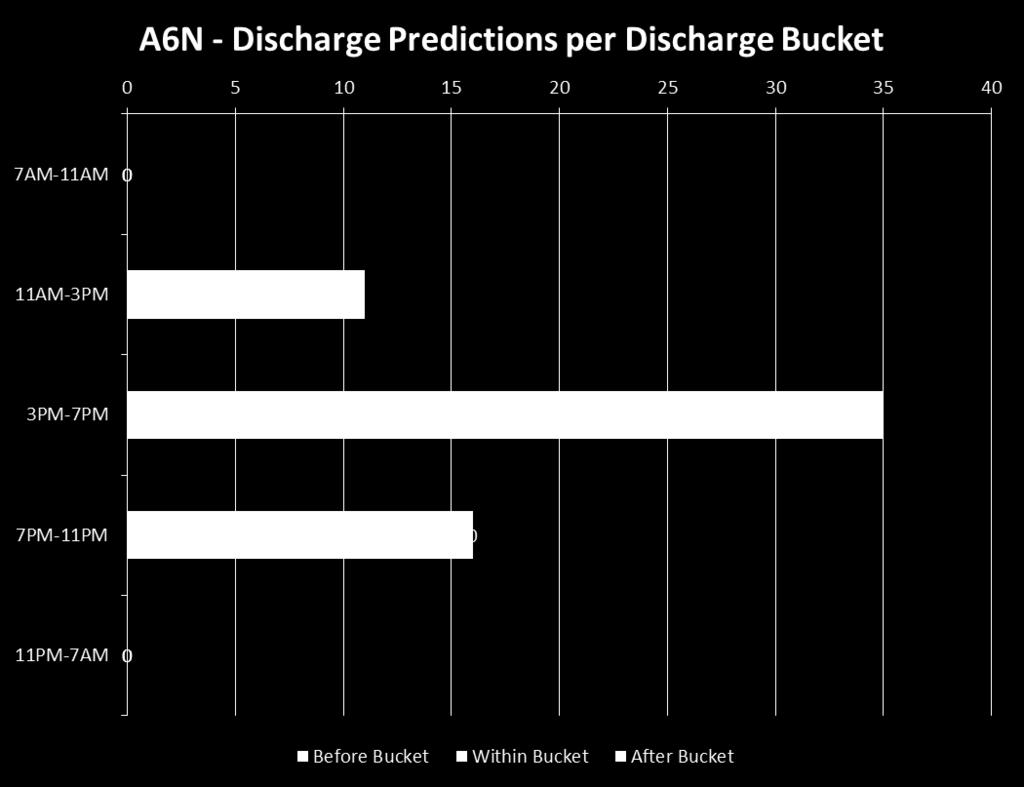
7 Discharge Prediction In 2008, CCHMC began predicting the time of discharges in 4 hour time buckets to Anticipate bed availability Place patients on the appropriately skilled nursing unit These predictions took into account medical, social and system level factors Success defined as patient going home in the predicted bucket or the bucket prior By 2010, discharge predictions had improved but flow hadn t and system delays persisted
8
9
10 Refocusing: Our New Theory We needed to address system issues to improve efficiency: Lack of shared discharge goals for patients Patients with the same diagnoses had goals that varied by physician Goals were not shared with nursing staff or families Discharge planning occurred last minute Shift focus to plan discharge around medical readiness, regardless of time of day
11 AIM To increase the percentage of Hospital Medicine patients admitted to one of three inpatient units with one of 11 common diagnoses discharged within two hours* of meeting medicallyready criteria from 42% to 80% by June 30, 2013 *If criteria were met between 9:00 pm 7:00 am, patients were not expected to leave until 9am.
12 Other Measures Nurse and Physician Process Measures Secondary Measures: Length of stay (LOS) Average daily census Total occupied beds at 8am /number of days in the month

13 Balancing Measures 30-day Readmission Rates Family Satisfaction
14 Key Drivers Increase the percentage of Hospital Medicine patients with one of 11 common inpatient diagnoses discharged within two hours of meeting medically ready criteria from 42% to 80% by June 30, 2013 Discharge Criteria Defined Frontline Staff Buy-in and Shared Ownership Discharge Barrier Identification with Mitigation Plans established Team Performance Transparency with Preoccupation with Failure
15 11 Diagnoses Asthma Bronchiolitis Osteomyelitis Hyperbilirubinemia Fever of Uncertain Source Cellulitis Gastroenteritis/Dehydration Urinary Tract Infection Pneumonia Croup Constipation
16 The Process Physicians define criteria in EMR on admission Patient meets medicallyready criteria Nurse places time stamp in EMR If patient does not leave within 2 hours, nurses document reason why
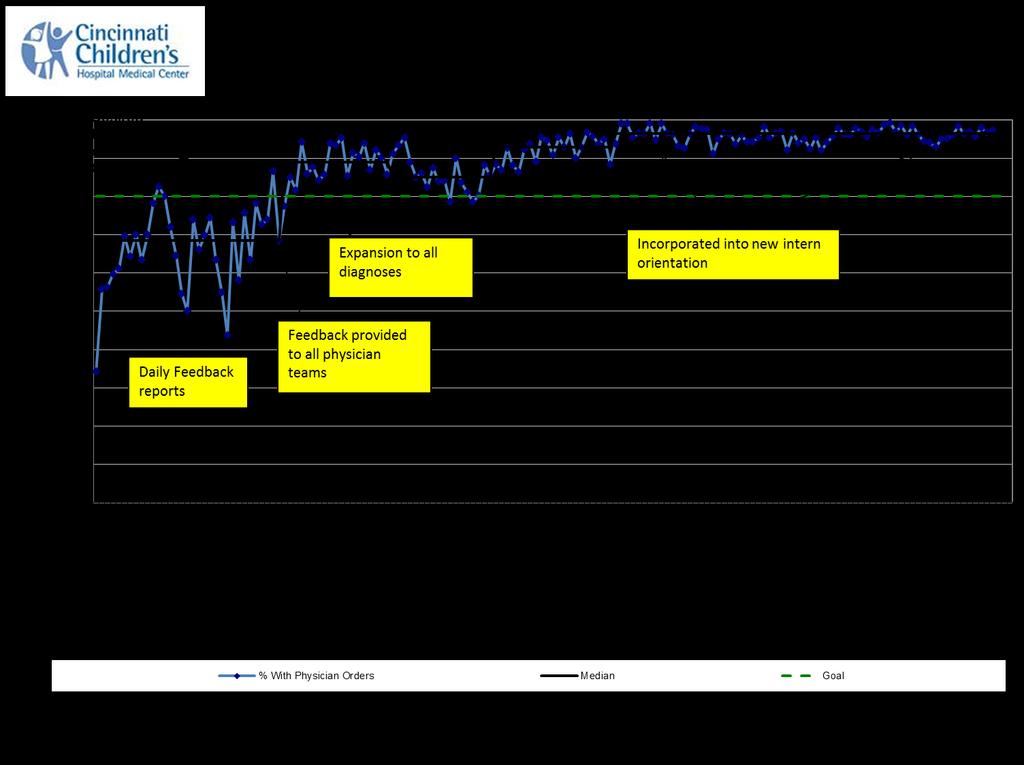
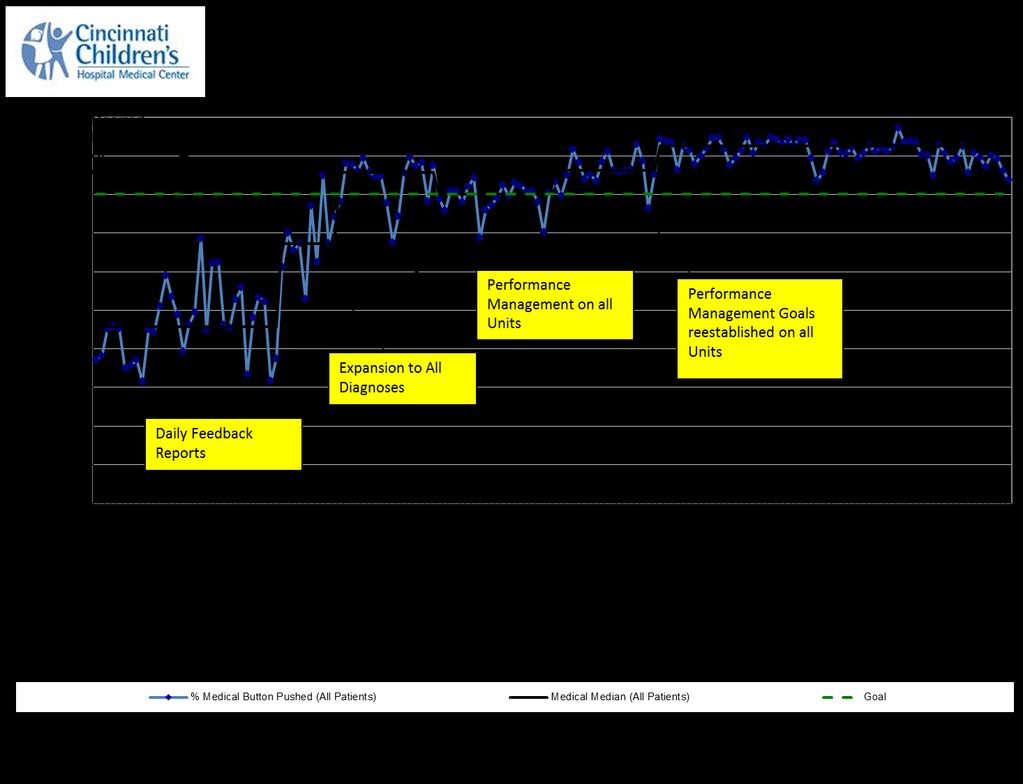
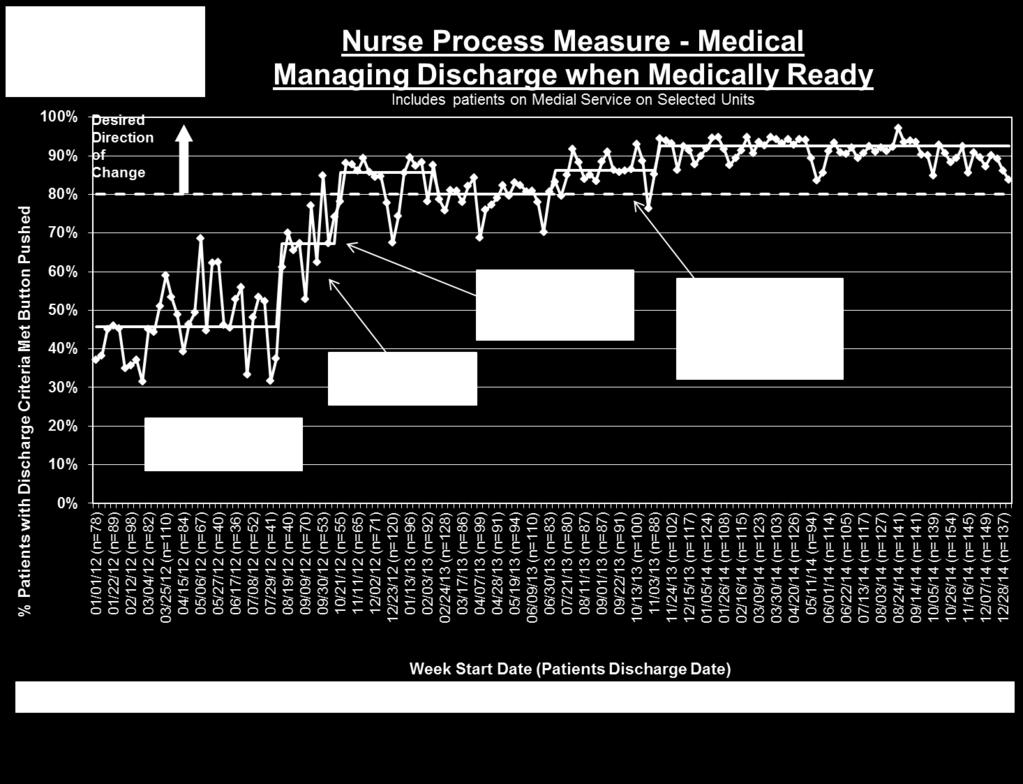
17 Process Measures Physician process measure: the percentage of admitted patients with medically-ready discharge orders Nurse process measure: the percentage of patients with the medically-ready time stamp placed in the electronic medical record (EMR)
18 EMR Discharge Criteria: Physician View 2013 Epic Systems Corporation. Used with permission.

19 EMR Discharge Criteria: Nurse View 2013 Epic Systems Corporation. Used with permission.

20 Time Stamp Documentation 2013 Epic Systems Corporation. Used with permission.

21 Screenshot of button 2013 Epic Systems Corporation. Used with permission.


22 Nurse Documentation of Failure 2013 Epic Systems Corporation. Used with permission.
23 Baseline Failure Reasons
24 Optimizing Discharge Efficiency % Discharged within 2 Hours of Medically Ready
25 Optimizing Discharge Efficiency % Discharged within 2 Hours of Medically Ready Key Intervention Period for General Medical Teams

26 Key stakeholder buy-in and shared ownership 6 Pilot Diagnoses
27 Standardization of Discharge Criteria Based on available evidence and expert consensus Diagnosis-specific goals For example, stable without supplemental oxygen for 6 hours for patients with bronchiolitis Did not include non-medical items For example, medications filled by pharmacy Embedded in physician admission order sets Modifiable
28 EMR Discharge Criteria: Physician View 2013 Epic Systems Corporation. Used with permission.
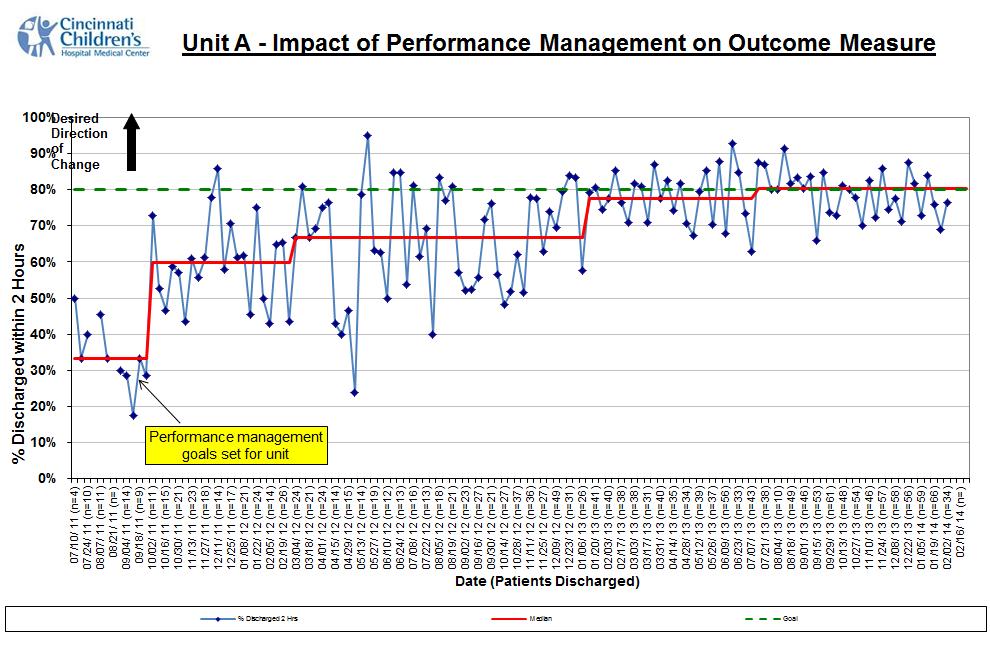
29 Leveraging of Nursing Performance Management System A pay-for performance managerial system to plan, evaluate and reward individual employee performance Goals align with strategic priorities In Oct 2011, one unit included the discharge outcome as the unit s goal That unit s performance improved from 34-60%
30
31
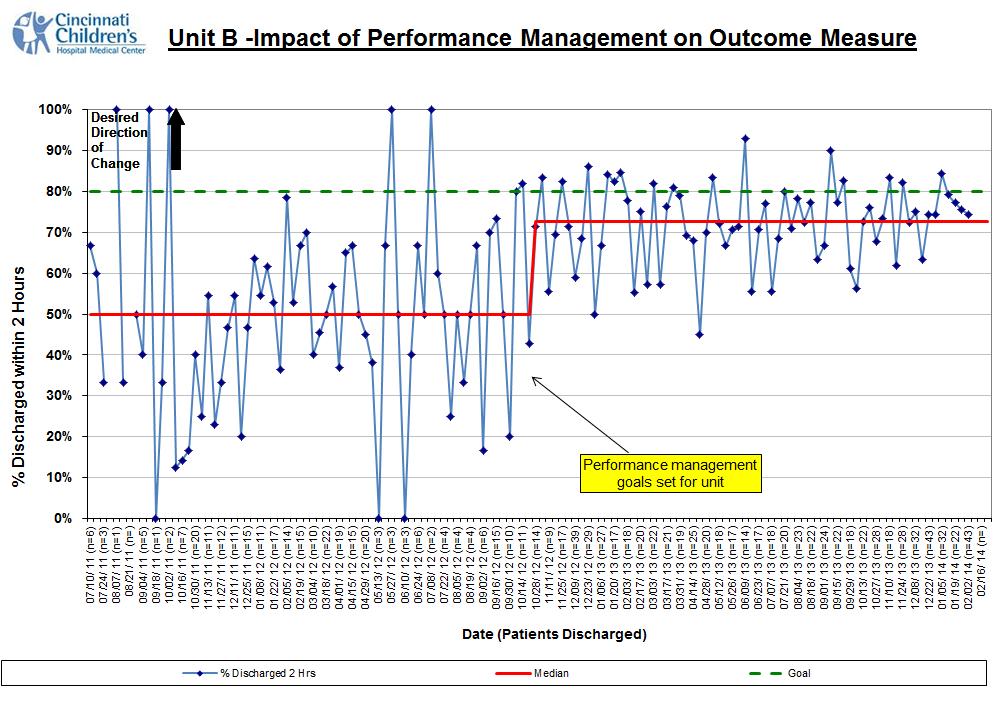
32 Key stakeholder buy-in and shared ownership Second and third unit performance management
33 Discharge Barriers Defined and Mitigation Plans Established Focused on the top 2 failure reasons: Subspecialty Consult timeliness Medication Delays Accounted for 35% of the failures

34 Timeliness of consults Key stakeholder buy-in and shared ownership
35 Subspecialty Consult Timeliness Many patients admitted with asthma exacerbations receive an asthma team consult Staffed by pulmonary medicine or allergy/immunology attendings Help with medication adjustment, diagnostic testing and outpatient follow-up
36 Asthma Team Consult Timeliness Interventions Prioritized consults based on predicted discharge time Instituted a brief consult note with asthma team recommendations
37 Timeliness of consults Pharmacy process optimization Key stakeholder buy-in and shared ownership
38 Pharmacy Process Optimization On admission, nurses documented the families preferred pharmacy in the EMR At CCHMC Pharmacy: Filling prioritization based on predicted discharge time Pharmacist start time shifted to 7 am Delivery of medications Mon-Fri from 8 am to 5 pm

39 Pharmacy Process Optimization Flu shot Order modified to eliminate upon discharge phrase Stocked on the floor
40 Timeliness of consults Pharmacy process optimization Preoccupation With Failure Key stakeholder buy-in and shared ownership
41 Preoccupation with Failure Daily automated reports generated from the EMR: Detailed all the process and outcome failures from the day prior Allowed for: Identification & mitigation of physician process failures Learn about outcome failures

42 Daily Report 42 Numerator for the outcome measure Denominator for the outcome measure Time the patient left the hospital

43 Daily Report Physician process measure: medically ready order place Time the patient MET medically ready criteria Failure reason
44 Timeliness of consults Process Expansion Pharmacy process optimization Preoccupation With Failure Key stakeholder buy-in and shared ownership
45 Expansion to all diagnoses Challenging for frontline providers to remember which patients qualified Shift from work by exclusion model to an all inclusive model In Nov 2012, we applied the processes to ALL HM patients General admission order set

46 General Admission Order Set 2013 Epic Systems Corporation. Used with permission.
47 Timeliness of consults Process Expansion Transparency of Data Pharmacy process optimization Preoccupation With Failure Key stakeholder buy-in and shared ownership
48 Transparency of Data Feedback to physician teams: Weekly s to attendings Poster in resident conference rooms with team compliance Daily s about outcome failures Feedback to nursing units: Run charts posted on the unit Discussions at monthly staff meetings

49 Poster in Resident Conference Room
50 Timeliness of consults Process Expansion Second and third unit performance management Transparency of Data Pharmacy process optimization Preoccupation With Failure Key stakeholder buy-in and shared ownership
51 Discharge Failure Reasons Comparison
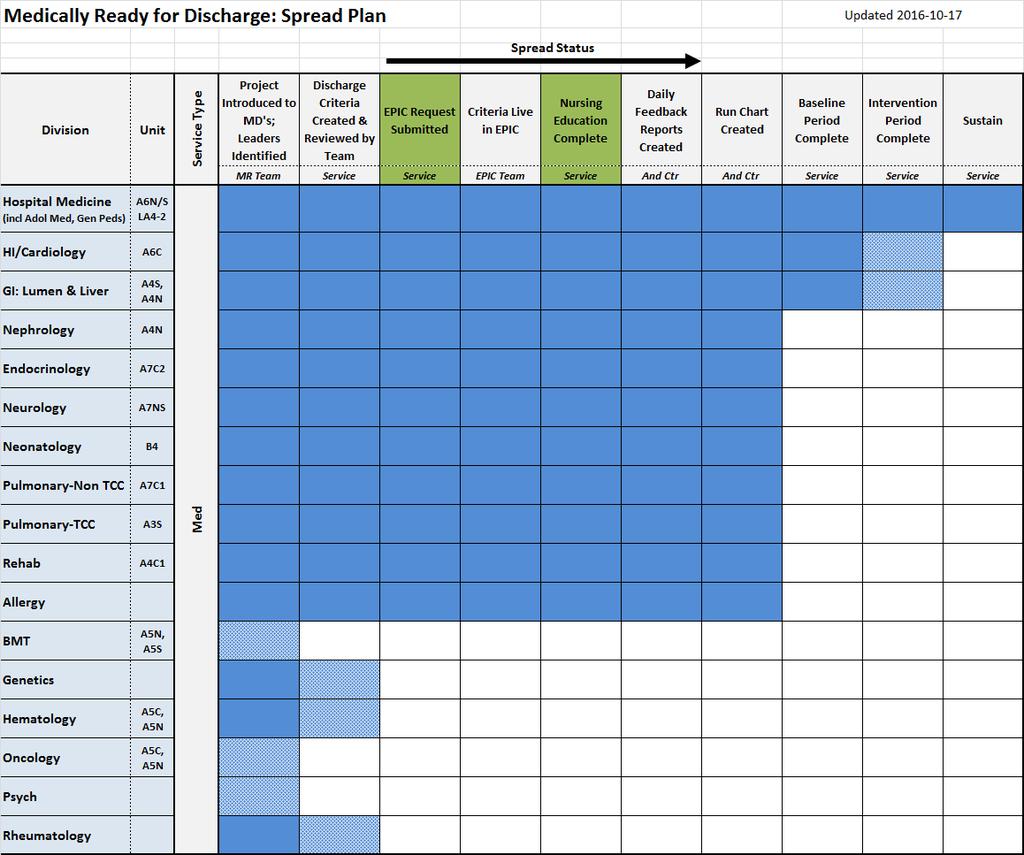
52 07/10/ 11 (n=10) 08/14/ 11 (n=) 09/18/ 11 (n=15) 10/23/ 11 (n=23) 11/27/ 11 (n=30) 01/01/ 12 (n=29) 02/05/ 12 (n=28) 03/11/ 12 (n=37) 04/15/ 12 (n=29) 05/20/ 12 (n=29) 06/24/ 12 (n=19) 07/29/ 12 (n=9) 09/02/ 12 (n=35) 10/07/ 12 (n=47) 11/11/ 12 (n=70) 12/16/ 12 (n=109) 01/20/ 13 (n=75) 02/24/ 13 (n=104) 03/31/ 13 (n=81) 05/05/ 13 (n=80) 06/09/ 13 (n=92) 07/14/ 13 (n=78) 08/18/ 13 (n=90) 09/22/ 13 (n=87) 10/27/ 13 (n=116) 12/01/ 13 (n=115) 01/05/ 14 (n=125) 02/09/ 14 (n=109) 03/16/ 14 (n=120) 04/20/ 14 (n=174) 05/25/ 14 (n=138) 06/29/ 14 (n=133) 08/03/ 14 (n=130) 09/07/ 14 (n=155) 10/12/ 14 (n=153) 11/16/ 14 (n=174) 12/21/ 14 (n=176) 01/25/ 15 (n=219) 03/01/ 15 (n=206) 04/05/ 15 (n=210) 05/10/ 15 (n=198) 06/14/ 15 (n=182) 07/19/ 15 (n=196) 08/23/ 15 (n=173) 09/27/ 15 (n=209) 11/01/ 15 (n=256) 12/06/ 15 (n=209) 01/10/ 16 (n=246) 02/14/ 16 (n=258) 03/20/ 16 (n=) % Discharged within 2 Hours 100% 90% 80% Desired Direction of Change Optimizing Discharge Efficiency % Discharged within 2 Hours of Medically Ready General Medical Teams 70% 60% 50% 40% 30% Increase in Medically Clear Mental Health Patients Admitted to General Medical Teams 20% 10% 0% Week Start Date (Patients Discharged) % Discharged 2 Hrs Centerline Goal Control Limit Control Limit Last Updated 03/02/2016 by S.Neogi, James M. Anderson Center for Health Systems Excellence
53 Other Measures

54
55
56 Secondary Measures Median Length of Stay significantly decreased from 1.57 to 1.44 days (p=0.01) Asthma was the only individual admission diagnosis with a statistically significant improvement in LOS Exclusion of asthma patients still demonstrated a significant decrease in LOS for the remaining compiled diagnoses Average daily census increased from 36.4 to 42.9 (17.5% increase in occupancy)
57 Balancing Measures Readmission rates remained similar for individual diagnoses and overall (4.60% to 4.21%; p=0.24) Family satisfaction remained high
58 Lessons Learned Discharge prediction was the framework for our study but didn t improve flow Decreasing clinical variability in discharge criteria was an essential first step Taking advantage of habits and patterns was necessary Multidisciplinary collaboration was key to our success
59 Where are We Now? Improving discharge efficiency: Focusing Hospital Medicine complex patients with chronic conditions Spread to other services and units Working on consistent modification of the medically ready orders based on clinical course Working on improving the timeliness of the EMR timestamp
60
61 01/01/ 13 (n=130) 02/01/ 13 (n=121) 03/01/ 13 (n=111) 04/01/ 13 (n=117) 05/01/ 13 (n=139) 06/01/ 13 (n=132) 07/01/ 13 (n=144) 08/01/ 13 (n=138) 09/01/ 13 (n=133) 10/01/ 13 (n=157) 11/01/ 13 (n=129) 12/01/ 13 (n=113) 01/01/ 14 (n=117) 02/01/ 14 (n=107) 03/01/ 14 (n=104) 04/01/ 14 (n=141) 05/01/ 14 (n=130) 06/01/ 14 (n=109) 07/01/ 14 (n=118) 08/01/ 14 (n=112) 09/01/ 14 (n=109) 10/01/ 14 (n=90) 11/01/ 14 (n=69) 12/01/ 14 (n=52) 01/01/ 15 (n=66) 02/01/ 15 (n=63) 03/01/ 15 (n=67) 04/01/ 15 (n=81) 05/01/ 15 (n=99) 06/01/ 15 (n=87) 07/01/ 15 (n=106) 08/01/ 15 (n=80) 09/01/ 15 (n=81) 10/01/ 15 (n=103) 11/01/ 15 (n=89) 12/01/ 15 (n=97) 01/01/ 16 (n=102) 02/01/ 16 (n=93) 03/01/ 16 (n=99) 04/01/ 16 (n=84) 05/01/ 16 (n=80) 06/01/ 16 (n=94) 07/01/ 16 (n=96) 08/01/ 16 (n=83) 09/01/ 16 (n=) 10/01/ 16 (n=) % Discharged beofre noon Cardiology: Patients Discharged Before Noon % Discharged before noon A6C 100% 90% 80% Desired Direction of Change Last Updated 09/23/2016 by Smriti Neogi, James M. Anderson Center for Health Systems * due to construction on A6C, April 2015 data is from med ready population 70% 60% 50% 40% I2S2 Project RCIC project 30% 20% Baseline Period 10% 0% Month & Year (Total Patients Discharged) Centerline Control Limit Control Limit
62 Next Steps Shifting focus of interventions to address: Parent/patient concerns Transportation Continue spread to other services, units and hospitals
63 Publications White CM, Statile AM, White DL, Elkeeb D, Tucker K, Herzog D, Warrick SD, Warrick DM, Hausfeld J, Schondelmeyer A, Schoettker PJ, Kiessling P, Farrell M, Kotagal U, Ryckman FC. Using quality improvement to optimise paediatric discharge efficiency. BMJ Qual Saf 2014 Jan; 23(1): 1-9 Statile AM, Schondelmeyer AC, Thomson JE, Brower L, Davis B, Redel J, Hausfeld J, Tucker K, White DL, White CM. Improving Discharge Efficiency in Medically Complex Pediatric Patients. Pediatrics 2016 Aug; 138(2).
64 Thank You to Our Team Angela Statile, MD, MEd Denise L. White, PhD, MBA Amanda Schondelmeyer, MD Dena Elkeeb, MD Karen Tucker, MSN, MBA, RN Stephen D. Warrick, MD Denise M. Warrick, MD Matthew Carroll, MD Paul Yelton, MSCS Shelly Miller, Family Member Julie Hausfeld, BSN, RN Pamela Kiessling, MSN, RN Michael Farrell, MD Uma Kotagal, MBBS, MSc Frederick C. Ryckman, MD David Mayhaus, MS, PharmD Melissa Healy, RPH Karen McDowell, MD Patrick Brady, MD, MSc Laura Brower, MD

65 Questions or Comments?
66 Resources Iantorno S, Fieldston E. Hospitals are not hotels: high-quality discharges occur around the clock. JAMA Pediatr 2013;167(7): Institute of Medicine, Committee on Quality Health Care in America. Crossing the Quality Chasm - A New Health System for the 21st Century. Washington, DC: National Academy Press, 2001 Optimizing Patient Flow: Moving Patients Smoothly Through Acute Care Settings. Secondary Optimizing Patient Flow: Moving Patients Smoothly Through Acute Care Settings IHI innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement. Available at: (accessed 29 May 2013) Srivastava R, Stone B, Patel R, et al. Delays in discharge in a tertiary care pediatric hospital. J Hosp Med 2009;4(8):481-85
Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand
 This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
This presenter has nothing to disclose. Shaping Demand: Managing Elective OR Schedules and Predicting Downstream Demand Flow Symposium Nov. 2016 Frederick C. Ryckman, MD Professor of Surgery / Transplantation
Hospital Flow Case Study: Cincinnati Children s Hospital
 Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Hospital Flow Case Study: Cincinnati Children s Hospital Frederick C. Ryckman, MD Professor of Surgery / Transplantation Sr. Vice President Medical Operations Cincinnati Children s Hospital Cincinnati,
Matching Capacity and Demand:
 We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
We have nothing to disclose Matching Capacity and Demand: Using Advanced Analytics for Improvement and ecasting Denise L. White, PhD MBA Assistant Professor Director Quality & Transformation Analytics
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures. Learning Objectives
 Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
Utilizing a Pharmacist and Outpatient Pharmacy in Transitions of Care to Reduce Readmission Rates. Disclosures Rupal Mansukhani declares grant support from the Foundation for. Rupal Mansukhani, Pharm.D.
abstract QUALITY REPORT
 Improving Discharge Efficiency in Medically Complex Pediatric Patients Angela M. Statile, MD, MEd, a, b Amanda C. Schondelmeyer, MD, MSc, a, b, c Joanna E. Thomson, MD, MPH, a, b, c Laura H. Brower, MD,
Improving Discharge Efficiency in Medically Complex Pediatric Patients Angela M. Statile, MD, MEd, a, b Amanda C. Schondelmeyer, MD, MSc, a, b, c Joanna E. Thomson, MD, MPH, a, b, c Laura H. Brower, MD,
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
4/12/2016. High Reliability and Microsystem Stress. We have no financial, professional or personal conflict of interest to disclose.
 High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service
 Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Redesign the System: Improving Med/Surg Efficiencies and Patient Flow
 These presenters have nothing to disclose. Redesign the System: Improving Med/Surg Efficiencies and Patient Flow Amanda Stefancyk Oberlies, Pat Rutherford and Christine White Hospital Flow Professional
These presenters have nothing to disclose. Redesign the System: Improving Med/Surg Efficiencies and Patient Flow Amanda Stefancyk Oberlies, Pat Rutherford and Christine White Hospital Flow Professional
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: This innovation reduces time to pediatric antibiotic administration by using
IMPROVEMENT IN TIME TO ANTIBIOTICS FOR MGH PEDIATRIC ED PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: This innovation reduces time to pediatric antibiotic administration by using
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
HIMSS Davies Award Enterprise Application. --- Cover Page --- IT Projects and Operations Consultant Submitter s Address: and whenever possible
 HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
Disclosure. SwedishAmerican Hospital A Division of UW Health. Learning Objectives. Medication History. Medication History 2/2/2017
 Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Pay-for-Performance. GNYHA Engineering Quality Improvement
 Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
Pay-for-Performance GNYHA Engineering Quality Improvement The Writing Is On The Wall IOM Report - Rewarding Provider Performance: Aligning Incentives In Medicare 9/21/06 Medicare P4P and quality improvement
OPAT & Paediatric OPAT Standards and Practical Implications for the Hospital and Community. Dr Sanjay Patel & Dr Ann Chapman
 OPAT & Paediatric OPAT Standards and Practical Implications for the Hospital and Community Dr Sanjay Patel & Dr Ann Chapman UK OPAT Good Practice Recommendations - Practical considerations and challenges
OPAT & Paediatric OPAT Standards and Practical Implications for the Hospital and Community Dr Sanjay Patel & Dr Ann Chapman UK OPAT Good Practice Recommendations - Practical considerations and challenges
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Transitions of Care: The need for collaboration across entire care continuum
 H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
H O T T O P I C S I N H E A LT H C A R E, I S S U E # 2 Transitions of Care: The need for collaboration across entire care continuum Safe, quality Transitions Ef f e c t iv e Collaborative Successful The
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Taming Length of Stay Challenges Through Analytics
 Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Decreasing Environmental Services Response Times
 Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Decreasing Environmental Services Response Times Murray J. Côté, Ph.D., Associate Professor, Department of Health Policy & Management, Texas A&M Health Science Center; Zach Robison, M.B.A., Administrative
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
How can we provide the same world class care to patients with psychiatric disorders? 11/27/2016. Dec 2016 Orlando, FL
 The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager A HEALTHIER WORLD THROUGH BOLD INNOVATION
 Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
Krystal M Craddock, RRT-NPS, CCM, COPD Case Manager Department of Respiratory Care UC Davis Medical Center, Sacramento CA UC Davis ROAD Center kmcraddock@ucdavis.edu University of California Davis ROAD
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
Mobile Communications
 Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Priceless Partners: Common Patients, Common Goals
 Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
Priceless Partners: Common Patients, Common Goals Erin Hodson, RN, BSN, ACM Senior Director Case Management Inova Fairfax Hospital Pamela Andrews, RN, MSW, MBA, CCM, ACM Director Medical Management INTotal
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program
 INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
INPATIENT PROGRAM ENVIRONMENT Brain Injury Specialty Program INPATIENT PROGRAM ENVIRONMENT Upon admission, patients and families are oriented to the Rehabilitation Program, and are involved in an evaluation
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
FRIENDS OF EVIDENCE CASE STUDY
 Asthma Improvement Collaborative FRIENDS OF EVIDENCE CASE STUDY This is one of a series of illustrative case studies, under the auspices of the Friends of Evidence, describing powerful approaches to evidence
Asthma Improvement Collaborative FRIENDS OF EVIDENCE CASE STUDY This is one of a series of illustrative case studies, under the auspices of the Friends of Evidence, describing powerful approaches to evidence
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
OMC Strategic Plan Final Draft. Dear Community, Working together to provide excellence in health care.
 Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Dear Community, Working together to provide excellence in health care. This mission statement, established nearly two decades ago, continues to be fulfilled by our employees and medical staff. This mission
Departments to Improve. February Chad Faiella RN, Terri Martin RN. 1 Process Excellence
 Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Coordination of Multiple Departments to Improve ED Throughput February 2011 Chad Faiella RN, Terri Martin RN 1 Agenda OhioHealth information Grant Medical Center facts Bed assignment process Key takeaways
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence
 PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
W e were aware that optimising medication management
 207 QUALITY IMPROVEMENT REPORT Improving medication management for patients: the effect of a pharmacist on post-admission ward rounds M Fertleman, N Barnett, T Patel... See end of article for authors affiliations...
207 QUALITY IMPROVEMENT REPORT Improving medication management for patients: the effect of a pharmacist on post-admission ward rounds M Fertleman, N Barnett, T Patel... See end of article for authors affiliations...
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Quality Improvement in Neonatology. July 27, 2013
 Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
IN EFFORTS to control costs, many. Pediatric Length of Stay Guidelines and Routine Practice. The Case of Milliman and Robertson ARTICLE
 Pediatric Length of Stay Guidelines and Routine Practice The Case of Milliman and Robertson Jeffrey S. Harman, PhD; Kelly J. Kelleher, MD, MPH ARTICLE Background: Guidelines for inpatient length of stay
Pediatric Length of Stay Guidelines and Routine Practice The Case of Milliman and Robertson Jeffrey S. Harman, PhD; Kelly J. Kelleher, MD, MPH ARTICLE Background: Guidelines for inpatient length of stay
Application of QSEN competencies in a practice setting: The case of Cincinnati Children s Hospital Medical Center
 Application of QSEN competencies in a practice setting: The case of Cincinnati Children s Hospital Medical Center Heather L. Tubbs Cooley, PhD, RN Assistant Professor & Nurse Scientist CCHMC Quality Scholar
Application of QSEN competencies in a practice setting: The case of Cincinnati Children s Hospital Medical Center Heather L. Tubbs Cooley, PhD, RN Assistant Professor & Nurse Scientist CCHMC Quality Scholar
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
The Patient Protection and Affordable Care Act of 2010
 INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Mobilisation of Vulnerable Elders in Ontario: MOVE ON. Sharon E. Straus MD MSc FRCPC Tier 1 Canada Research Chair
 Mobilisation of Vulnerable Elders in Ontario: MOVE ON Sharon E. Straus MD MSc FRCPC Tier 1 Canada Research Chair Competing interests I have no relevant financial COI to declare I have intellectual/academic
Mobilisation of Vulnerable Elders in Ontario: MOVE ON Sharon E. Straus MD MSc FRCPC Tier 1 Canada Research Chair Competing interests I have no relevant financial COI to declare I have intellectual/academic
Measuring Medication Harm: Advantages of Using a Trigger Tool. Frank Federico Executive Director
 Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit Henry Ford Hospital Detroit Transition of Care (TOC) Services Introduction to Pharmacy Services Pharmacy Transition
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT)
") Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Impact of an Innovative ADC System on Medication Administration
 Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
Impact of an Innovative ADC System on Medication Administration March 1, 2016 Nilesh Desai, BS, RPh, MBA Administrator Pharmacy and Clinical Operations Hackensack University Medical Center Conflict of
Hospital Flow Professional Development Program
 Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Disclaimer: Consistent with the IHI s policy, faculty for this program are expected to disclose at the beginning of their presentation(s)
Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Disclaimer: Consistent with the IHI s policy, faculty for this program are expected to disclose at the beginning of their presentation(s)
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
Introduction of EPMA in paediatric practice in UK:
 Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Care Management Framework:
 WHITE PAPER Care Management Framework: The Critical Path to Implementing a Care Management Strategy An Encore Point of View Randy Thomas, FHIMSS, Barbara Doyle, MSN, RN, January 2017 Tina Burbine, MBA,
WHITE PAPER Care Management Framework: The Critical Path to Implementing a Care Management Strategy An Encore Point of View Randy Thomas, FHIMSS, Barbara Doyle, MSN, RN, January 2017 Tina Burbine, MBA,
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
PA Education Worldwide
 Physician Assistants: Past and Future Roderick S. Hooker, PhD, MBA, PA October 205 Oregon Society of Physician Assistants PA Education Worldwide Health Workforce North America 204 US Canada Population
Physician Assistants: Past and Future Roderick S. Hooker, PhD, MBA, PA October 205 Oregon Society of Physician Assistants PA Education Worldwide Health Workforce North America 204 US Canada Population
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically