Results from Contra Costa Regional Medical Center
|
|
|
- Patrick Peters
- 6 years ago
- Views:
Transcription
1 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care
2 High Impact Interventions Sepsis HAPU Ambulatory Care Redesign
3 DSRIP OVERSIGHT COMMITTEE Members include: Chiefs (CEO, COO, CMO, CNO, CMIO, CMQO, Ambulatory Care Medical Director) Director, Safety and Performance Improvement Patient Safety Officer Quality Manager Director, Analytics Behavioral Health Program Chief DSRIP Manager Improvement Specialists
4 Sepsis
5 Sepsis Beginnings Sepsis Team started in 2008 pre-dsrip Integrated Nurse Leadership Program (INLP) began work on one-hour bundle in California Contra Costa chose to continue 1-hour bundle for DSRIP
6 Sepsis Bundle Within 1 hour from time of presentation (i.e., presumed infection and 2 positive SIRS with lactic acid greater than 4 or systolic blood pressure less than 90 or a drop at more than 40 from baseline.) Measure lactic acid level Give 20-30ml/kg fluids (crystalliods) or 2 liters Obtain 2 sets of blood cultures Start broad spectrum antibiotic
7 Value of 1 Hour Sepsis Bundle Allows for early identification of potential organ failure by nursing staff based on objective clinical criteria. Pushed CCRMC to evaluate and streamline workflow to meet 1-hour goal. Standard work allows nursing staff to just do it and do it promptly for the sake of the patient. Nurses do not need permission nor to wait to confer with provider to start care.
8 Sepsis Journey Began in Emergency Department (ED) Bundle education and training by 2008 on one shift and spread slowly Identified physician champion May 2013, ED Nurse Sepsis Protocol order set initiated
9 Sepsis Journey Designated Sepsis nurse assigned every shift to assist with Severe Sepsis cases. Trained Rapid Response Team (RRT) and Emergency Department (ED) nurses to take blood cultures Simplified Sepsis antibiotic order set to two antibiotics Established dedicated sepsis nurse to monitor and train new staff
10 Sepsis Journey Consolidated sepsis treatment order sets from various departments in our Electronic Health Record Spread bundle to the Inpatient setting Created an Inpatient nursing RRT/ICU severe sepsis/septic shock protocol and order set. Small tests of change (PDSA s) were performed on use of the STAT sepsis pager and the RRT Tackle Box to evaluate effectiveness
11 Barriers Overcome Staff uncomfortable with level of fluids given (2 liters) fearing fluid overload. With backing of Cardiology MD, convinced staff that patients are more likely to die from organ failure than fluid overload. Infection Control staff concerned about false positives on blood cultures taken by nurses in ED. With initial education and once per year competency checks, ED and RRT nurses are fully capable of performing accurate blood cultures.
12 Barriers Overcome Organization-wide consolidation of various departmental sepsis treatment standards within EHR. Agreement by interdisciplinary team (Pharmacy, Critical Care, ED) of two antibiotics for bundle set for the initial antibiotic that cover the majority of infection types occurring with sepsis.
13 Strengths Director of sepsis team is a front-line provider Front-line nurses have responsibility for initiating sepsis treatment orders Reduces number staff needed to treat sepsis efficiently Process streamlined from patient s point of view istat average lactate time within 20 minutes Real time feedback to staff with sepsis team members
14 Success Bundle compliance increases: 50% 72% 78.8% Mortality rate decreases: 17% 11% 7.8%
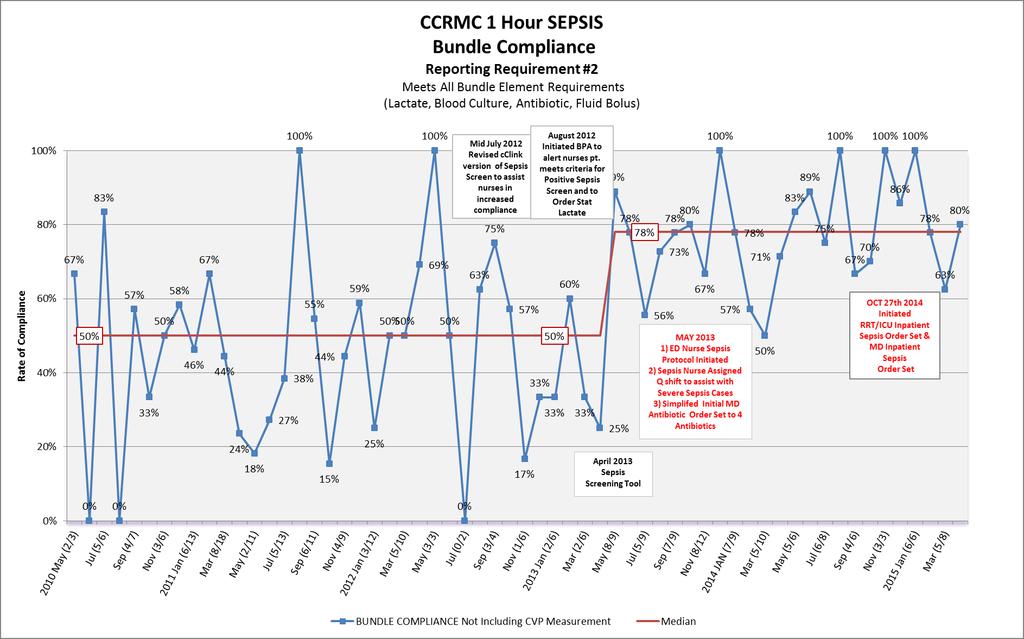
15 BUNDLE COMPLIANCE
16 SEPSIS MORTALITY
17 Hospital Acquired Pressure Ulcers (HAPU)
18 Hospital Acquired Pressure Ulcers Essential factors in promoting healthy skin: Skin assessment Mobility Good nutrition
19 Hospital Acquired Pressure Ulcers Started pre-dsrip with oversight team To meet DSRIP targets, HAPU Prevention Team was restructured in Fall 2011 to be multidisciplinary (nurse leadership, physician champion, unit nurses, quality manager, nurse educators) Goal: Identify and employ a sustainable HAPU prevention bundle that works for our patient population.
20 TESTS OF CHANGE KEY DRIVER DIAGRAM January 18, 2013 PRIMARY DRIVERS SMART AIM To reduce the hospitalwide HAPU rate to 1.75% by June 30, GLOBAL AIM 0% Hospital Acquired Pressure Ulcer Events every month Optimally Implement Prevention Interventions Optimal Assessment Increased Multidisciplinary Involvement and Teamwork Improved Communication Culture shift Appropriate equipment availability (improve bed functionality, availability, surface availability, Early Mobilization Hourly rounding occurs reliably Physical Therapy involvement sooner for high risk patients Dietary consult triggered by Braden Visual cues for staff about Braden score linked interventions (in cclink and on Census Boards) Standardized skin assessment Early identification of risk/timely assessments Documentation that is easy and visible to others Hired advanced level RN focus wound care to consult, educate physicians and staff Increase multidisciplinary involvement at the unit level (discharge rounds,4 eye skin assessment, Braden Scale in ICU/IMCU, 4B, 5D, 4A, ED, PACU,Perinatal. Improve team effort approach in 4C and PES Partnering with patients and families in prevention, intervention and education thereof MCS/NPM/health care team involvement in coordination and optimal utilization/shifting of resources to support staff in meeting patients needs Improve support and development of unit champions Recognition of unit champions and their roles in improvement efforts Education and policy awareness Improve practice through clearly defined policy Improve communication of HAPUs to staff and why they occurred Improve display and communication of data in way to more engage staff and families/patients and increase process owner awareness Improve Culture of safety Awareness- staff and leadership awareness of the last 5 HAPU s and why they occurred. Policy and practice alignment Improve compliance and increase level of best practice sustainability of pressure ulcer prevention and care Standardize audit process Feb 2012Intentional rounding on 5D Nov2012: Braden Score on Census Board-5D Development of automated intervention triggers Standardized Order set s to support HAPU prevention Feb eyes skin assess on 4B4 Eyes Skin Assessment on every transfer or admit to 4A, 4B, 5D'September: Mandatory 15 min. inservice on 4 Eye Skin Assessment on Med/Surg and CCU/IMCU March 2012: Unit Champions 1st 8 hour pressure ulcer training for Unit Champions August: Aug 2012: NAPH kick-0ff; In-service training planning October: 2 hour wound training for unit champions Jan 2012: weekly HAPU Meetings April 2012: Braden < 18 reported to NPM s; safety huddles Braden score on digital whiteboard 4B Communication of patients at risk Staff meetings Standardized messaging 5 minute safety huddles (CN, primary nurse)- standardization between unit 9am daily multidisciplinary discharge rounds CN-CN bedside safety rounds at change of shift Nov2012: Braden Score on Census Board-5B Audit cclink documentation for 4 eyed skin assessments after review of policy Test perinatal storyboard template approach to adapt to Med Surg area Survey (staff) Audits Staff meeting discussions Active Involvement (doing to) Awareness staff and leadership awareness of the last 5 HAPU s and why they occurred. Engagement (doing with) (MD, nursing, MCS, support staff, residents, PT, dietary) CALNOC prevalence survey involvement of team approach Test audit tool Charge Nurse and manager discuss audits and keep log of follow ups
21 First Steps Early 2012 employed intentional hourly rounding Trialed 4-eye skin assessment all patients on one unit, including transfers in and out of unit Unit champions received 8-hr pressure ulcer training 5 minute safety huddles for communication on at-risk patients Braden scores posted on whiteboards for staff Encouraged patient mobility when appropriate
22 Stepping It Up Roll out to all inpatient units: Every admission reviewed for existing pressure ulcers 4-Eye Skin Assessment required every shift, on admission, transfer, postop and upon discharge to a SNF ED nurse protocol: Braden scale/4-eye Assessment required within 2 hours of admission orders Daily monitoring reports and audit tools created
23 Stepping It Up Staff and leadership review of root cause of all HAPUs Treatment guides include stage-specific wound care products Wound care nurse hired to educate and identify areas of improvement
24 Barriers Overcome Education of all inpatient and emergency staff on all shifts on HAPU tools, HAPU stages and Safety event reporting tools Design of assessments into patient care standard workflows Display of real-time patient data to underscore patient care needs and expectations of leadership Identification of physician champion
25 Ongoing Challenges Education of new inpatient and emergency staff on HAPU interventions Continued engagement of front-line staff to assist with problem solving (i.e., patients with co-morbidities, indwelling tubes, etc.) Timely and accurate staging of wounds
26 Strengths Strong, committed multidisciplinary team Skin assessments built into daily standard work Use of proven tools: 4 Eyes Assessment Braden Scale Internal audit reports
27 HAPU Prevalence Rate (Stage 2+) Year Target Rate 2012 N/A 2.40% % 2.04% % 1.06% % 0.13%* * Ten months ending April 2015
28 Hospital Acquired Pressure Ulcers
29 Ambulatory Care Redesign
30 Ambulatory Care DSRIP Projects Increase primary care provider visits Reduce Third Next Available appointment rate Patient experience measurement Establish video interpreting network
31 Ambulatory Care DSRIP Projects Empanel Medi-Cal Health Plan patients Integrate physical and behavioral health care Population health measures (mammography rate, hypertension reduction, CHF 30-day readmission reduction, etc.)
32 Ambulatory DSRIP Results Increase Primary Care Provider visits by 17,000/year Reduced Third Next Available appointments from 13+ days to 6 days Video interpreting access in all 11 clinics
33 Ambulatory DSRIP Results MediCal Health Plan patients empanelled at 99%+ Behavioral health integrated at 3 primary care clinics SBIRT* rate over 75% at pilot clinics and SBIRTs rolled out to all clinics by end of 2015 *Screening, Brief Intervention and Referral to Treatment
34 Ambulatory Care Redesign To ensure ability to meet DSRIP expectations we considered the individual projects part of an organization-wide improvement effort Resources and other interventions were included in the global effort Telephone Consultation Clinic (500 visits/month) Lean education & rapid improvement events IHI collaborative on care access
35 Ambulatory Care Redesign Access to Care Collaborative (IHI) Began with small tests of change at 4 clinic locations with each clinic assigned different project Worked with Nurse Manager Leads and clinical support teams (RNs, LVNs, MAs, clerks) Education provided on improvement work principles and overall goals Teams worked hard on tests of change, meeting regularly with coaches on monthly conference calls and in off-site learning sessions
36 Challenges Small tests of change did not create enough momentum at the individual sites to realize the greater systemic change needed. Adjusted model and employed all patient access interventions tested at the different clinics into one clinic location; provided improvement specialists and other support.
37 Results In first three months, trial clinic shows improvement in: Third next available appointment Patient continuity Appointment disposition (visit frequency) Access model will be rolled out to new clinic locations every three months through early 2016 to hopefully realize the same improvement system-wide for our patients.
38 Ambulatory Care Results Population health measures experiencing movement in right direction overall, i.e., mammography screening, influenza immunization rates, etc. (no set targets) Third next available appointment rate dropped in access pilot clinic from 24 to 8 days Patient care continuity rates at pilot clinics increased by 6-10% Reducing frequency of follow up visits. Percentage of patients asked to return in less than 4 months has dropped by nearly 9 points in 7 months
39 Third Next Available Appointment
40 Patient-Centered Continuity The patient-centric continuity rate increased 6-7% over 7 months in one pilot clinic... and increased by 9 percentage points in a 2 nd pilot clinic since it opened in Spring of 2014.
41 Appointment Disposition, less than 4 months
42 Take Away Without all of our staff pulling together organization leaders, providers and other front line staff - to make the system better for our patients, large systemic change and population health improvement will not be realized.
43 DSRIP Impact The need to meet long-term stretch targets attached to financial incentives ensured our improvement momentum DSRIP leadership and oversight structure created is scalable for oversight of other quality improvement efforts Improvement Academy created to train DSRIP teams first, then mid-level managers on improvement principles
44 DSRIP Impact Lean education provided to management; Kaizen rapid improvement events utilized to create standard work to support the overall improvement efforts on hospital units and in clinics. Non-DSRIP teams now requesting kaizen events and PDSA training and support to improve internal processes
45 DSRIP Impact Dashboards originally created to monitor DSRIP measures have since been created for all clinics, the ED, providers, and quality management. Improvement work started set stage for participation in public and private grants to continue affiliated improvement work. Supports 5 year strategic plan. Sets stage for establishing organizational priorities and supporting key initiatives, including additional capability goals such as Six Sigma training.
46 Questions?
SFGH. Management System. Components. SFGH Management System. Improvement. Time. Strategic Planning True North. Value Streams: Rapid Improvement Events
 SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
HealthONE Sepsis Program
 HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE
 SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE") MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
MEDICAID ACCELERATED EXCHANGE (MAX) SERIES ACCELERATE TRANSFORMATION AND LASTING CHANGE Presented by: Linda Efferen, MD, MBA Medical Director Suffolk Care Collaborative 19 THE MAX SERIES SUPPORTS AN INTERDISCIPLINARY
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
MemorialCare Orange Coast: Using Innovative Technology to Improve Efficacy of Patient Repositioning
 MemorialCare Orange Coast: Using Innovative Technology to Improve Efficacy of Patient Repositioning Presented by: Nika Carlson, MSN, RN, Director of Clinical and Quality Improvement Jennifer Castro, MSN,
MemorialCare Orange Coast: Using Innovative Technology to Improve Efficacy of Patient Repositioning Presented by: Nika Carlson, MSN, RN, Director of Clinical and Quality Improvement Jennifer Castro, MSN,
Bold Goal PI Radar Dashboard
 Bold Goal PI Radar Dashboard Helen Macfie, Pharm.D., FABC Chief Transformation Officer Certified Lean Leader For IHI Patient Safety Executive Development Course, September, 2016 This presenter has nothing
Bold Goal PI Radar Dashboard Helen Macfie, Pharm.D., FABC Chief Transformation Officer Certified Lean Leader For IHI Patient Safety Executive Development Course, September, 2016 This presenter has nothing
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
QUALIS HEALTH HONORS WASHINGTON HEALTHCARE PROVIDERS
 LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
HIMSS Davies Award Enterprise Application. --- Cover Page --- IT Projects and Operations Consultant Submitter s Address: and whenever possible
 HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Passage to Excellence Our Sepsis Journey
 Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
The Davies Award Is: The HIMSS Nicholas E. Davies Award of Excellence. Awarding IT. Improving Healthcare.
 The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
Sepsis Mortality - A Four-Year Improvement Initiative
 Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
ACTION PLANS. OHA Statewide Sepsis Initiative. January 13, 2016
 ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Saving Lives with Best Practices and Improvements in Sepsis Care
 Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Sepsis Quality Improvement Project. October/November 2017
 Sepsis Quality Improvement Project October/November 2017 Stony Brook Medicine includes six Health Sciences schools as well as Stony Brook University Hospital, Stony Brook Southampton Hospital, Stony Brook
Sepsis Quality Improvement Project October/November 2017 Stony Brook Medicine includes six Health Sciences schools as well as Stony Brook University Hospital, Stony Brook Southampton Hospital, Stony Brook
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
Sepsis Interdisciplinary Team Bronx Lebanon Hospital Center
 Sepsis Interdisciplinary Team Bronx Lebanon Hospital Center October/November 2017 Bronx Lebanon Hospital Center Bronx-Lebanon is the largest voluntary, not-for-profit health care system serving the South
Sepsis Interdisciplinary Team Bronx Lebanon Hospital Center October/November 2017 Bronx Lebanon Hospital Center Bronx-Lebanon is the largest voluntary, not-for-profit health care system serving the South
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Quality Improvement Plans (QIP): Progress Report for 2017/18 QIP
: Progress Report for 2017/18 QIP") Quality Improvement Plans (QIP): Progress Report for 20 QIP The Progress Report is a tool that will help organizations make linkages between change ide and improvement, and gain insight into how their
Quality Improvement Plans (QIP): Progress Report for 20 QIP The Progress Report is a tool that will help organizations make linkages between change ide and improvement, and gain insight into how their
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Celebrating our Successes 2014
 Celebrating our Successes 214 Nurse Involvement in Decision Making Groups 5 CODE SEPSIS: Time from Antibiotic Order to Administration 45 4 Time in Minutes from order to administration 35 3 25 2 15 1 5
Celebrating our Successes 214 Nurse Involvement in Decision Making Groups 5 CODE SEPSIS: Time from Antibiotic Order to Administration 45 4 Time in Minutes from order to administration 35 3 25 2 15 1 5
Advancing Accountability for Improving HCAHPS at Ingalls
 iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
The Challenges and Rewards of Patient and Family Centered Care
 The Challenges and Rewards of Patient and Family Centered Care Deborah Baker DNP, ACNP April 30, 2012 1 Patient and Family Centered Care The Institute For Patient and Family- Centered Care defines core
The Challenges and Rewards of Patient and Family Centered Care Deborah Baker DNP, ACNP April 30, 2012 1 Patient and Family Centered Care The Institute For Patient and Family- Centered Care defines core
Indiana Pressure Ulcer Reduction Initiative
 Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
PRESSURE ULCER PREVENTION
 PRESSURE ULCER PREVENTION University of South Alabama Medical Center Mobile, AL Becky Pomrenke, RN, MSN, CNL University of South Alabama Medical Center Academic, Urban Hospital Regional Level I Trauma
PRESSURE ULCER PREVENTION University of South Alabama Medical Center Mobile, AL Becky Pomrenke, RN, MSN, CNL University of South Alabama Medical Center Academic, Urban Hospital Regional Level I Trauma
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Solution Title: Meeting the Challenge of Health Care Change
 Organization: Western Maryland Health System Solution Title: Meeting the Challenge of Health Care Change Program/Project Description, including Goals: What was the problem to be solved? How was it identified?
Organization: Western Maryland Health System Solution Title: Meeting the Challenge of Health Care Change Program/Project Description, including Goals: What was the problem to be solved? How was it identified?
Deeper Dive on Team Roles: Part 2
 Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
Deeper Dive on Team Roles: Part 2 Moderator: Nicole Van Borkulo, MEd, Qualis Health Speakers: Catherine Dower, JD, Associate Director of Research, Susan Chapman, PhD, RN, and Lisel Blash, Senior Research
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound)
") Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Essentia Health. A View on Information Technology. ND HIMS Conference April 12, Tim Sayler, COO Essentia Health - West
 Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Essentia Health A View on Information Technology ND HIMS Conference April 12, 2017 Tim Sayler, COO Essentia Health - West Me Discussing Information Technology Who is Essentia Overview Why: Information
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
An Implementation Framework for Patient Safety in Ambulatory Care. To disseminate key findings from IHI s work on ambulatory safety
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
For audio, join by telephone at , participant code #
 For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
2018 DOM HealthCare Quality Symposium Poster Session
 Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Tina Nelson, MBA, BSN Lisa Stepp, BSN, RN Rebecca Fyffe, BSN, RN Jessica Coughenour, LPN
 Establishing a Conservative Approach to the Prevention of Pressure Ulcers with the Utilization of Data Analytics to Monitor Effectiveness of Quality Efforts and Best Practice Models Tina Nelson, MBA, BSN
Establishing a Conservative Approach to the Prevention of Pressure Ulcers with the Utilization of Data Analytics to Monitor Effectiveness of Quality Efforts and Best Practice Models Tina Nelson, MBA, BSN
Sepsis Management at Russell Medical
 Sepsis Management at Russell Medical Sarah Beth Gettys V.P. Patient Services Russell Medical Dr. Michele Goldhagen MD, CMO, ED Medical Director Russell Medical Oct 3, 2017 1 Objectives List key success
Sepsis Management at Russell Medical Sarah Beth Gettys V.P. Patient Services Russell Medical Dr. Michele Goldhagen MD, CMO, ED Medical Director Russell Medical Oct 3, 2017 1 Objectives List key success
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Columbus Regional Hospital Pressure Ulcer Prevention
 Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
NURSING SPECIAL REPORT
 2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Catheter Associated Urinary Tract Infection Reduction using Daily Management Systems. OHSU Performance Excellence
 Catheter Associated Urinary Tract Infection Reduction using Daily Management Systems OHSU Performance Excellence DATE : April 1 8, 2 0 1 6 PRE SENTE D B Y: Nancy McCully MSN, MBA, RN, CCRN, Marge Willis
Catheter Associated Urinary Tract Infection Reduction using Daily Management Systems OHSU Performance Excellence DATE : April 1 8, 2 0 1 6 PRE SENTE D B Y: Nancy McCully MSN, MBA, RN, CCRN, Marge Willis
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
Transforming Care at the Bedside: Climbing the Clinical Ladder
 Transforming Care at the Bedside: Climbing the Clinical Ladder Rebecca Springer, MSN, RN Chief Nursing Officer, Nurse Executive Temiela Blackman, MA Quality Manager Hendry Regional Medical Center April
Transforming Care at the Bedside: Climbing the Clinical Ladder Rebecca Springer, MSN, RN Chief Nursing Officer, Nurse Executive Temiela Blackman, MA Quality Manager Hendry Regional Medical Center April
Engaging Frontline Staff in Real-Time Improvement
 Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Successfully Using Six Sigma. (6σ) to Improve Nursing Quality. Indictors. Objectives. 1. Describe how Six Sigma can be used to
 to Improve Nursing Quality. Indictors. Objectives. 1. Describe how Six Sigma can be used to") Successfully Using Six Sigma (6σ) to Improve Nursing Quality Indictors Joann Hatton, RN MS, 6σ Black Belt Director of Nursing Professional Practice Heritage Valley Health System Beaver, PA Objectives 1.
Successfully Using Six Sigma (6σ) to Improve Nursing Quality Indictors Joann Hatton, RN MS, 6σ Black Belt Director of Nursing Professional Practice Heritage Valley Health System Beaver, PA Objectives 1.
OhioHealth s Mission: To Improve the Health of Those We Serve
 Enhancing SAFE SKIN Through Computer Utilization OhioHealth s Mission: To Improve the Health of Those We Serve 2 1 3 Grant Medical Center 21,000 patient discharges/year Average daily census of 260 Magnet
Enhancing SAFE SKIN Through Computer Utilization OhioHealth s Mission: To Improve the Health of Those We Serve 2 1 3 Grant Medical Center 21,000 patient discharges/year Average daily census of 260 Magnet
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Strengthen Patient Care by Reducing Hospital Acquired Pressure Ulcers (HAPU)
") Strengthen Patient Care by Reducing Hospital Acquired Pressure Ulcers (HAPU) Nihar Bhatia Head Quality Assurance & Fortis Operating System and Prateem Tamboli, Facility Director, Fortis Escorts Hospital
Strengthen Patient Care by Reducing Hospital Acquired Pressure Ulcers (HAPU) Nihar Bhatia Head Quality Assurance & Fortis Operating System and Prateem Tamboli, Facility Director, Fortis Escorts Hospital
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Make Sure You Are Solving the Right Problem P. 1 Are Electronic Health Records Contributing to Fraud? P. 1 Stress Ulcer Prophylaxis P. 2 Antibiotic Stewardship P. 3 APeX tips for a safe
IN THIS ISSUE: Make Sure You Are Solving the Right Problem P. 1 Are Electronic Health Records Contributing to Fraud? P. 1 Stress Ulcer Prophylaxis P. 2 Antibiotic Stewardship P. 3 APeX tips for a safe
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Presentation Objectives
 ISQua s 31 st International Conference Quality and Safety Along the Health and Social Care Continuum Integrating Performance Measurement into Every Level of Care: What Does it Mean in Your Organization?
ISQua s 31 st International Conference Quality and Safety Along the Health and Social Care Continuum Integrating Performance Measurement into Every Level of Care: What Does it Mean in Your Organization?
An Implementation Framework for Patient Safety in Ambulatory Care
 An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
An Implementation Framework for Patient Safety in Ambulatory Care Jennifer Lenoci-Edwards, RN, MPH, CPPS Director of Patient Safety, IHI Richard Braunstein, MD Executive Director, Manhattan Eye, Ear &
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals
 Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
Quality Measure Indicators +Throughput Metrics + Automated Dashboard = Innovation to Improve Quality Goals DMC Harper- Hutzel Hospital The DMC is an 8 facility academic medical center Harper-Hutzel is
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA. July 26 th, :00 a.m. 12:00 p.m. CDT
 AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management
 Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Our Sepsis Improvement Journey
 A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
A25 Our Sepsis Improvement Journey Driving Value through Collaboration December 6, 2016 9:30 10:45 am #IHIFORUM Session Objectives P2 To describe how our organization reduced sepsis mortality, saved lives
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
TRANSFORMING CARE DELIVERY
 APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
Taming Length of Stay Challenges Through Analytics
 Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
Taming Length of Stay Challenges Through Analytics March 3, 2016 Dr. Michelle Pezzani, Medical Director Utilization Management at El Camino Hospital & Palo Alto Medical Foundation (PAMF) Petrina Griesbach
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Maryland Patient Safety Center s Call for Solutions Submission. Organization: Atlantic General Hospital
 Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Clinical Documentation Improvement (CDI)
") Clinical Documentation Improvement (CDI) Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Jessie Hanks, BS, RHIA, Director HIM Amanda Logue, M.D., Chief Medical Information
Clinical Documentation Improvement (CDI) Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Jessie Hanks, BS, RHIA, Director HIM Amanda Logue, M.D., Chief Medical Information
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE. Early Recognition and Treatment of Severe Sepsis and Septic Shock
 SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence
 PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
PSI-15 Lafayette General Health 2017 Nicholas E. Davies Enterprise Award of Excellence Rachel Brunt, RN, BSN, MBA-HCA, CIC, CPHQ, Director Quality Jessie Hanks, BS, RHIA, Director HIM Lafayette General
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION
 ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
ACCESS LARC INCREASING ACCESS TO IMMEDIATE POSTPARTUM LONG-ACTING REVERSIBLE CONTRACEPTION Chapter One: Building a Successful Initiative General Quality Improvement Tips It takes a multidisciplinary team
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO